
Abstract
Introduction. The adult population is increasingly experiencing one or more chronic illnesses and living with such conditions longer. The Chronic Disease Self-Management Program (CDSMP) helps participants cope with chronic disease-related symptomatology and improve their health-related quality of life. Nevertheless, the long-term effectiveness of this evidence-based program on older adults as compared to the middle-aged populations has not been examined in a large-scale, national rollout. Method. We identified baseline characteristics of CDSMP participants aged 65 years or older (n = 687, M = 74.8 years) in the National Study of CDSMP from 2010 to 2012. Comparisons were made to middle-aged participants aged 50 to 64 (n = 325, M = 58.3 years). Assessments were conducted at baseline and 12-month follow-up. Linear and generalized linear mixed models were performed to assess changes in primary and secondary outcomes, controlling the key sociodemographics and number of chronic conditions. Results. All primary outcomes (i.e., social/role activities limitation, depression, communication with doctors) significantly improved in both the older and middle-aged cohorts. Although improvements in illness symptomatology (e.g., fatigue, pain, shortness of breath, and sleep problems) were similar across both cohorts, only the middle-aged cohort benefitted significantly in terms of overall quality of life and unhealthy mental health days. Effect sizes were larger among the middle-aged population who were also more likely to enter the program in poorer health and be from minority backgrounds. Conclusions. The current study documented improved health outcomes but more so among the middle-aged population. Findings suggest the importance of examining how age and interacting life circumstances may affect chronic disease self-management.
The prevalence and costs of chronic conditions among Americans are well documented (Centers for Disease Control and Prevention, 2013). Americans 65 years and older are disproportionately affected by chronic conditions, with more than 90% of older adults having at least one chronic condition, and over 70% having at least two chronic conditions (Anderson, 2010). Data show that as an individual’s number of chronic conditions increases, there is a corresponding escalation in adverse outcomes including poor functional status, unnecessary hospitalizations, adverse drug events, duplicative tests, and conflicting medical advice (Federal Interagency Forum on Aging-Related Statistics, 2010; U.S. Department of Health and Human Services, 2011). Each of these negative impacts leads to higher health costs and greater outlays for programs like Medicare and Medicaid (Kaiser Family Foundation, 2012).
This recent attention given to the negative impacts of multiple chronic conditions has been accompanied by national initiatives to reduce the burden of preventable diseases (Interagency Workgroup on Multiple Chronic Conditions, 2010; U.S. Department of Health and Human Services, 2011). Acknowledging the multiple determinants of health (U.S. Department of Health and Human Services, 2012), a systems approach to improve the quality of life for all Americans has been proposed (National Prevention Council, 2011). Such a systems approach is recommended for developing intervention strategies directed toward building healthy communities, improving clinical and community preventive services, supporting people to make healthy choices, and eliminating health disparities (National Prevention Council, 2011).
Self-management is seen as a key pillar of the National Prevention Strategy for empowering Americans to achieve better health and wellness (National Prevention Council, 2011). Empowering people to make important health decisions can help foster engagement and independence among community-dwelling adults (Montross et al., 2006). The Chronic Disease Self-Management Program (CDSMP; Lorig et al., 2012) is among the most widely disseminated and evaluated evidence-based self-management programs for helping participants living in a community cope with chronic disease-related symptomatology and improve their health-related quality of life (Ory, Smith, & Resnick, 2012). Recent data from a large community-based study confirmed the continued positive impacts of CDSMP on meeting the Health Care Reform Triple Aims of better health, better care, and better value for adults 18 and older (Ory, Ahn, Jiang, Smith, et al., 2013).
Implementation science is just beginning to focus on whom evidence-based programs for chronic disease self-management are attracting when disseminated through multiple clinical and community delivery channels (Smith, Ory, Belza, & Altpeter, 2012). Less is known about the nature and potency of intervention effects among different age cohorts (e.g., a middle-aged cohort where chronic diseases are characteristically just emerging vs. an older cohort where chronic conditions have been accumulating over time; Ory et al., 2012).
Thus, it is difficult, a priori, to predict differences in outcome measures across these two cohorts. It may be that the middle-aged cohort will benefit more from the intervention because group-based problem-solving activities may be more familiar to a younger cohort. Conversely, it may be that the older group will benefit more because they have higher motivation/necessity to manage their chronic conditions due to more serious impacts on their daily lives. However, it may also be that the underlying self-management skills being taught (e.g., goal setting, problem solving, action planning) are universal, and there may be similar effects across the two age cohorts. Or it is highly likely that the patterns will be inconsistent, with variable age effects observed for different outcome domains.
No studies have investigated the long-term effectiveness of CDSMP across age cohorts representing nearly 50 years of adulthood, examining characteristics of those who enroll in the program as well as outcomes for older adults compared to the adjacent cohort of near-elderly adults. Thus, the objectives of this research are to (a) describe characteristics of middle-aged (aged 50-64 years) and older adults (65 years and older) who enrolled in the program; (b) examine primary outcome changes from baseline to 12-month assessment in terms of the medical, emotional, and social role management demands of chronic conditions by age cohort; and (c) investigate secondary outcomes reflecting impacts on health status and quality of life by age cohort. Such research will enable us to document similarities and differences in beneficial effects among older adults relative to middle-aged adults, who represent the next cohort of older adults, for the purposes of better understanding optimal points of intervention.
Method
Data Source and Study Population
Data used in these analyses were collected at baseline and 12 months after enrollment as part of the National Study of the CDSMP. As described elsewhere in fuller detail (Ory, Ahn, Jiang, Lorig, et al., 2013; Ory, Ahn, Jiang, Smith, 2013), this study used a pre–post longitudinal design to examine intervention effects of CDSMP for middle-aged and older adults who enrolled in workshops delivered nationwide. Study participants (n = 1,170) enrolled in workshops between August 2010 and April 2011, which were delivered by 22 licensed sites in 17 states across the nation. Approximately 77% (n = 903) and 71% (n = 825) of the 1,170 participants completed the 6-month and 12-month assessments, respectively. After excluding respondents who were <50 years old (n = 158), the final analytic sample size was 1,012.
CDSMP delivery sites recruited participants using referrals from aging network organizations, health care facilities, and social service organizations as well as self-referrals from a variety of recruitment activities including community flyers, brochures, and health fairs. Participant eligibility criteria included a) having at least one self-reported chronic disease, (b) having not previously taken CDSMP, (c) enrolling in a CDSMP workshop delivered in either English or Spanish, (d) attending at least one of the first two class sessions, (e) completing a baseline survey, and (f) consenting to being in this study. Institutional review board approval was obtained at Stanford University and Texas A&M University.
Intervention
Drawing on well-known evidence-based behavior change principles (Bandura, 1991; Ory, Jordan, & Bazzarre, 2002), CDSMP stresses concepts such as goal setting, problem solving, and action planning. Using a small group workshop format, sessions are facilitated by two trained leaders, one or both of whom are non–health professionals and have at least one chronic disease. Workshops consist of six highly participative sessions held for 2½ hours each, once a week, for 6 consecutive weeks. Subjects covered during CDSMP workshops include (a) techniques to deal with problems such as frustration, fatigue, pain, and isolation; (b) appropriate exercise for maintaining and improving strength, flexibility, and endurance; (c) appropriate use of medications; (d) effective communication with family, friends, and health professionals; (e) nutrition; and (f) how to evaluate a new treatment (Lorig et al., 2012).
Measures
Primary Outcomes
Three broad categories of primary outcomes were included to reflect basic self-management tasks addressed during CDSMP skill-building activities: (a) role management, (b) emotional management, and (c) medical management. These concepts were operationalized by the three standardized scales described below. Each of these scales has been used in previous CDSMP research and psychometric properties have been described (Lorig et al., 2001; Lorig et al., 1999; Stanford Patient Education Research Center, 2012).
Social/role activities limitations
Study participants were asked how much their health has interfered with their social/role activities (i.e., normal activities, recreational activities, household chores, and errands) during the past week. Scores for these items were summed and divided by 4 to create an average value of their social/role activities limitations. Higher scores indicate greater activity limitations.
Depression
Participants’ depression was measured by using the eight-item Patient Health Questionnaire–Depression Scale. Scores range from 0 to 24. Higher scores indicate more severe depression.
Communication with physicians
Communication with a physician was measured using a three-item scale, which asked participants if they did the following things when visiting a physician: prepare a list of questions, ask questions about things they want to know or do not understand, and discuss personal problems. Scores for these items were summed and divided by 3 to create an average value. Higher score represent better communication with a physician or health care provider.
Secondary Outcomes
Several secondary outcomes were selected based on outcomes previously examined in outcomes research (Ory, Ahn, Jiang, Lorig, et al., 2013; Ory et al., 2010). The Healthy Days measures (Centers for Disease Control and Prevention, 2000) were used to gauge self-assessed health status, including estimates of the number of days when physical and mental health was not good during the past 30 days, as well as the number of days the participant was restricted from usual activities. An analogue scale for each illness symptom ranging from 0 to 10 was employed to assess symptoms associated with chronic disease, including fatigue, pain, shortness of breath, and sleep problems as well as overall quality of life (anchored by “very poor” quality to “excellent” quality; Stanford Patient Education Research Center, 2012).
Study covariates
Several personal characteristics served as covariates. This included standard demographic variables such as gender, race/ethnicity, and highest level of education received. For the purposes of this study, age was treated continuously but also dichotomized into two cohorts (i.e., 50-64 years representing a middle-aged adult cohort and 65+ years representing an older adult cohort). Health status was also assessed by the number of chronic conditions. This was measured by a series of items that asked respondents to self-report information about the number and type of chronic conditions in which they had been diagnosed (e.g., diabetes, heart disease, asthma and other lung-related diseases, cancer, arthritis).
Analyses
Baseline characteristics were compared between the two age cohorts using χ2 tests for categorical variables and two-sample t tests for continuous variables. Varying analyses were performed to examine changes from baseline to the 12-month follow-up assessment for primary and secondary outcomes. Linear mixed models (using Stata xtmixed procedure) with participant-level random intercepts were fitted for continuous outcome variables controlling for age, gender, race, education, and number of chronic conditions. Generalized linear mixed models with Poisson distribution and participant-level random intercepts (using Stata xtpoisson procedure), controlling for the same covariates, were used to assess changes in count outcome measures (e.g., number of unhealthy physical days in the past 30 days). These two types of mixed effects models are likelihood-based approaches that used all available data in model estimation and provided unbiased estimates of the intervention effects under the assumption of missing at random. An effect size (d = [posttest M – pretest M]/pretest SD) using estimates of changes from the mixed effects models was computed for each outcome except the zero-inflated variables. Effect sizes of d = 0.2 were considered small, d = 0.5 medium, and d = 0.8, large (Cohen, 1988).
Results
Sample Characteristics
In total, 1,170 participants were recruited into the CDSMP program and completed the baseline assessment. As shown in Table 1, the average age of these participants was approximately 65 years old. More than half of participants were 65 years or older (N = 687, 59%), while 325 (28%) were between 50 and 64 years. Compared with older participants, those in the middle-aged cohort were more likely to be Blacks or Latino/Hispanics. They also had significantly more comorbidities than the older participants (3.3 vs. 2.9, p = .006). Hypertension was the most prevalent condition in both age groups (64.0% of total sample, 58.5% for younger cohort, and 66.7% for older cohort). Arthritis was the next most prevalent condition with 57.9% in the total sample and 51.1 % for younger cohort and 61.1% for older cohort. Type 2 diabetes was the third most reported condition in the total sample (32.3%), with a rate of 36.9% for younger cohort and a rate of 30.1% for the older cohort. Depression was the fourth most reported condition (25.3%), with expected age differentials (42.2% in the younger cohort and 17.3 in the older cohort). Furthermore, the middle-aged participants scored significantly lower on social role function and higher on depression compared to those who were age 65 years or older (1.7 vs. 1.2, p < .001; 8.0 vs. 5.3, p < .001, respectively).
Baseline Characteristics of CDSMP Participants by Age Cohort.

p value for chi-square test comparing the participants in two age-groups. bp value for two-sample t test comparing the participants in two age-groups.
Primary Outcomes
The results in Table 2 show that all three primary outcomes (i.e., social role function, communication with doctors and depression) improved significantly from baseline to 12-month assessment in both age cohorts. The effect sizes of the adjusted changes ranged from 0.20 to 0.33 in the middle-aged cohort and ranged from 0.10 to 0.21 in the older group.
Adjusted a Changes Between Posttest and Pretest Means and Effect Sizes for the Primary Outcomes.

All changes and p-values are adjusted for gender, age, race/ethnicity, education, and number of chronic conditions. bRaw means and standard deviations at each of the assessments. cAdjusted changes between 12-month and baseline from linear mixed regression models.
Secondary Outcomes
As shown in Table 3, most of the secondary outcome variables also improved significantly in both age cohorts. Among middle-aged participants, significant improvements were observed for all secondary outcomes. In the older adult cohort, overall quality of life and unhealthy mental days did not change significantly from baseline to 12-month assessment. The intervention had the greatest effects on self-assessed health status and overall quality of life in the middle-aged cohort (d = 0.35 and 0.39, respectively). In the older adult cohort, the intervention had the greatest effect on sleep problems (d = 0.24). Overall, the magnitude of the effect sizes was generally larger in the middle-aged cohort than that in the older adult cohort. For example, the number of unhealthy physical days was reduced by 24% from baseline to 12-month assessment among middle-aged participants (mean ratio = 0.76, p < .001), whereas it was only reduced by 9% among older adult participants (mean ratio = 0.91, p < .001).
Adjusted a Changes or Ratios Between Posttest and Pretest Means and Effect Sizes for the Secondary Outcomes.
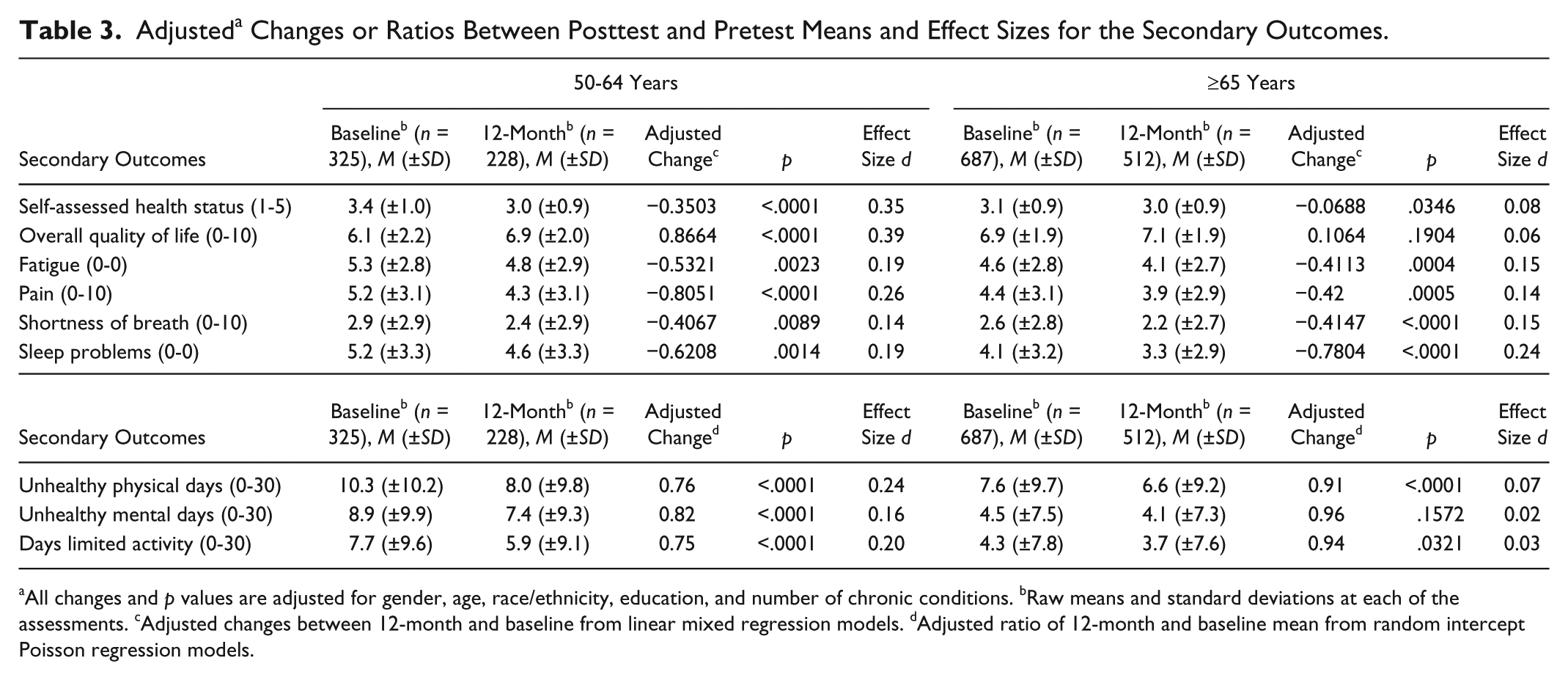
All changes and p values are adjusted for gender, age, race/ethnicity, education, and number of chronic conditions. bRaw means and standard deviations at each of the assessments. cAdjusted changes between 12-month and baseline from linear mixed regression models. dAdjusted ratio of 12-month and baseline mean from random intercept Poisson regression models.
Discussion
As recent findings demonstrate (Ory, Ahn, Jiang, Lorig, et al., 2013; Ory, Ahn, Jiang, Smith, et al., 2013), participation in CDSMP workshops is associated with many positive outcomes (i.e., health and quality of life) that promote healthy aging. Such findings were confirmed by changes in the three primary study outcomes in the current study. As an example, improvement in social role functioning can be seen as an indicator of less interference with normal social activities with family, friends, and neighbors, as well as more engagement in normal tasks, recreational activity, and chores.
Better communication with health care providers may reflect a more motivated and independent patient who prepares questions for the doctor and asks questions about topics of concern. Reductions in depressed symptomatology are viewed as important for attaining interest or pleasure in doing things and feeling joy in interaction with others. In terms of secondary outcomes, decreases in days of limited activity may be considered another strong indicator of the benefit of CDSMP to improve engagement and independence.
This article extends prior literature by examining outcomes in two specific age cohorts. Although positive benefits were reported in both cohorts, the benefits appeared to be stronger in the middle-aged cohort (i.e., 50-64 years) in terms of the number of significant health-related outcomes as well as the strength of the intervention effect. These findings are notable for the following reasons. Although the program was primarily marketed to “older adults,” as part of a national rollout of evidence-based programs sponsored by the Administration on Aging (Ory, Smith, et al., 2013), the current study reveals that the middle-aged or near-elderly cohort were also attracted to this program. The positive outcomes experienced by participants in the 50 to 64 age cohort confirms that middle-age is a time when individuals who are already experiencing multiple chronic conditions can benefit from learning self-management skills, and reinforces the value of a chronic disease self-management at different life stages. This perspective identifies what is unique about the health status, health behaviors, and social roles of each age cohort that would help guide program implementation and dissemination (Ory et al., 2014). For example middle-aged cohorts might have competing role demands that make self-management activities challenging (e.g., balancing work and caregiving responsibilities).
In our study, the middle-aged cohort, although younger, tended to be sicker and from more diverse racial and ethnic backgrounds. The relative success of evidence-based programs (including CDSMP) with lower resourced populations has been previously documented (Smith, Ahn, Mier, Jiang, & Ory, 2012; Smith, Cho, Salazar, & Ory, 2013), and partially attributed to these participants entering the program with poorer health and quality of life indicators that are amenable to change through goal setting and action planning to improve lifestyle behaviors.
Several plausible theoretical explanations can be posited for the weaker intervention effect among the older cohort. Ageist beliefs and stereotypes may still operate in subtle ways (Nelson, 2002). One interpretation may be that older participants hold the traditional belief that it is the doctor’s job to “fix” them, not their own responsibility (Adelman, Greene, & Ory, 2000). Another interpretation may be that older adults have less motivation to improve because they do not believe it is worth the trouble to change their lifestyle this “late in the game”(Ory, Hoffman, Hawkins, Sanner, & Mockenhaupt, 2003). Furthermore, older adults may have underestimated their self-reported baseline scores because they do not view themselves as that sick/limited/impaired considering their age (compared to younger patients with multiple chronic conditions who seem much sicker than most of their peers; Ory & Cox, 1994). This perception may be because these participants already received some form of disease management advice (formally or informally) before entering the program.
Some older adults, especially those 80 years and older, may have reduced cognitive ability. Therefore, the skills taught in workshops may not have been as easily grasped. Alternatively, in exploratory analyses not reported here due to small sample sizes, participants 80 years and older continue to benefit significantly from CDSMP in terms of improved communication with their physicians and some illness symptomatology such as pain and sleep that are prevalent problems among older populations. In fact, the intervention effect size for communication with doctors was largest in the 80+ group (0.28) versus adults aged 65 to 79 (0.11) and 50 to 64 (0.20). These findings indicate that CDSMP workshops can positively affect doctor–patient interactions, even among very old participants.
Although the literature on who benefits most from evidence-based interventions is often mixed due to different intervention modalities, populations, and settings being investigated, our study confirms previous findings that younger participants may benefit most (Reeves et al., 2008). Additionally, our current study supports prior research indicating that participants entering the program in poorer health (e.g., more depression and lower quality of life) benefit more than their healthier counterparts (Harrison et al., 2012). Two explanations are plausible. Those entering CDSMP with more deficits (e.g., depressive symptomology) may be especially responsive to highly interactive and supportive group-based interactions, and hence their improved mental health enables them to engage more fully in self-management activities. Alternatively, findings may reflect a methodological artifact whereby those with lower entry scores have more opportunities for improvement relative to those entering the program with better health. In other words, the different intervention effects between two age cohorts maybe an example of the famous “regression toward the mean” phenomenon. However, in the current study it is impossible to disentangle the impact of age cohort from the particular life circumstances experienced by our younger cohort (e.g., the younger cohort being sicker with greater distress and poorer social role limitations). Future studies comparing age cohorts with similar baseline health status are needed to fully elucidate the underlying mechanism for the differential intervention effectiveness between younger and older participants.
Future studies are needed that examine the relative benefits experienced by CDSMP participants based on their health and social indicators on entry to the program. In addition to controlling for sociodemographics, such studies could perform analyses only among individuals with more baseline deficits (e.g., depressive symptomology) to identify received benefits without findings being attenuated by the inclusion of participants without such baseline deficits.
This study demonstrates the importance of a community-based delivery system that has ability to reach racially, ethnically, and geographically diverse populations who become sicker earlier but may not otherwise have access to health promotion programs (Ory, Smith, et al., 2013). This is especially important because those near-elderly with a greater number of chronic conditions tend to have even higher health care costs when Medicare eligible (Lubell, 2012). From a policy perspective, the near-elderly traditionally have had more difficulty than seniors in accessing and affording health care (Ziliak & Gundersen, 2011), a challenge that should be abated with passage of the Patient Protection and Affordable Care Act of 2010, but that can also be partially addressed through the widespread dissemination of self-management programs.
Although the older cohort did not benefit as much as their younger counterparts, on average, there were significant improvements on most outcomes. This indicates the importance of and need for continued program marketing to older adults. One exception was the ability of CDSMP to more positively affect sleep problems for the older adult cohort. This is important given the prevalence of sleep problems among an aging population (Foley, Ancoli-Israel, Britz, & Walsh, 2004). However, it should be noted that the middle-aged cohort reported more concerns with sleeping, despite a larger effect size seen among older adult participants.
Limitations
As with any study, there are limitations that must be acknowledged. First, this study compared only two age cohorts (i.e., the near-elderly and older adults) due to limited sample size in the oldest old population. Thus, additional research on a broader range of age cohorts is needed to enable researchers to identify more definitively how different age cohorts would benefit from evidence-based CDSMPs. Second, there was no control group in this study design, which may be considered a threat to internal validity. However, the large diverse population being studied enabled the researchers to address threats to external validity, a major concern in translational research (Glasgow, Klesges, Dzewaltowski, Bull, & Estabrooks, 2004). Although significant changes were observed in the predicted direction, the effect sizes tended to be smaller than in the original studies, reflecting greater variability in community-based delivery than in tightly controlled research studies. Although there is some study attrition, the retention rate in this study is excellent for community-based intervention studies (Jiang et al., 2014; Waters, Galichet, Owen, & Eakin, 2011).
Third, many of the measures were single items. This reflects the movement toward a more pragmatic parsimonious set of measures to reduce the data collection burdens in real world settings (Krist et al., 2013). Furthermore, all outcome variables were self-reported, which may have led to under- or overestimation of participant responses.
It is also unknown in the current study whether age or underlying baseline health and social characteristics accounted for observed age cohort differentials. Similarly, it was not possible to examine any potential confounding impacts of health care systems on the health care outcomes in the current study, since such organizational variables were not included in the current database. No information was available about the type or amount of health care that participants were receiving or the linkages between their community and clinical care. As such, it is impossible for us to know whether improvements were partially attributed to other health care interventions.
Finally, due to the small sample size of participants attending Spanish-led workshops, we were not able to differentiate between the CDSMP English language version and the Tomando version for Spanish speakers. However, we did control for race/ethnicity in the multivariate analyses, which should help negate any differential impacts. Furthermore, we performed sensitivity analyses to compare trends by workshop language. The results of these sensitivity analyses were virtually identical between Tomando participants and those from the larger group of CDSMP participants. CDSMP workshops use social and family supports as critical change agents; however, the current study was not designed to assess the specific impact of such external supports
Conclusion
CDSMPs are important for teaching behavioral skills that can enhance engagement and independence of community-dwelling adults with chronic conditions. Demonstrated benefits for both middle-aged and older cohorts reinforce our belief that it is important to consider age-based differences when delivering and evaluating public health interventions, noting that chronic diseases manifest themselves at different time points in different populations. Prior CDSMP studies have projected substantial potential net savings of $364 per participant and national savings of $3.3 billion if only 5% of adults with one or more chronic conditions were reached (Ahn et al., 2013). Program planners and policy makers should consider middle-aged adults an appropriate target for disease prevention and self-management interventions to encourage healthful aging before reaching older adulthood. Additionally, delaying the aging process is important and can save as much as 7 trillion dollars over the next five decades (Goldman et al., 2013). However, given the widespread benefits seen in both age cohorts in the current study, the public health mantra should be “It is never too early or late to intervene for healthy aging!” This can best be accomplished through a comprehensive public health approach of encouraging healthy lifestyles while building supportive environments that “make it easy to do the right thing” for health promotion and disease prevention.
Footnotes
Acknowledgements
We thank the 22 delivery sites and the participants who enrolled in the National Study of Chronic Disease Self-Management Program from 2010-2011. Diana Laurent, Audrey Alonis, Maurice Green, Eileen Bradley, and Angela Devlin from Stanford Patient Education Research Center assisted in the data collection and management. Jairus Pulczinski from Texas A&M assisted in the manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Council on Aging (NCOA) through contracts to Texas A&M Health Science Center (Principal Investigator: Marcia G. Ory) and Stanford University (Principal Investigator: Kate Lorig). Nancy Whitelaw served as the NCOA Principal Investigator. Additionally, we recognize grant support from the Administration on Aging through American Recovery and Reinvestment Act funding for the Chronic Disease Self-Management Program. Also recognized is support from the Healthy Aging Research Network members who provided general consultation on the National Study. Kate Lorig receives royalties from the book used by participants in the Chronic Disease Self-Management Program.
Supplement Issue Note
This article is part of an open access supplement “Fostering Engagement and Independence: Opportunities and Challenges for an Aging Society,” published in SOPHE’s Health Education & Behavior. This supplement was supported by funding provided by the Centers for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and Health Promotion, Healthy Aging Program (Cooperative Agreement #U38HM000454) via the Association of State and Territorial Health Officials, and from a grant provided by the Retirement Research Foundation. Views presented herein do not represent the official views of the CDC.