
Abstract
Although the New York City Chinese population aged ≥65 years increased by 50% between 2000 and 2010, the health needs of this population are poorly understood. Approximately 3,001 Chinese individuals from high-density Asian American New York City areas were included in the REACH U.S. Risk Factor Survey; 805 (26.8%) were aged ≥65 years and foreign-born. Four health-related quality of life and three behavioral risk factor outcome variables were examined. Descriptive statistics were conducted by gender, and logistic regression models assessed sociodemographic and health factors associated with each outcome. Few women were current smokers (1.3% vs. 14.8% of men), 19% of respondents ate fruits and vegetables more than or equal to five times daily, and one-third of individuals received sufficient weekly physical activity. Days of poor health were similar to the national population aged ≥65 years, while self-reported fair or poor health was much greater among our Chinese sample; over 60% of respondents rated their health as fair or poor. Lower education and lower obesity were significantly associated with cigarette smoking among men, and older age was significantly associated with insufficient physical activity overall. Female gender was significantly associated with all poor health days; older age was significantly associated with poor days of physical health, and lower income was significantly associated with poor days of physical health and fair or poor self-reported health. This study provides important health-related information on a rapidly growing older population and highlights future research areas to inform culturally appropriate health promotion and disease prevention strategies and policies within community-based settings.
Keywords
Chinese Americans are the largest Asian American subgroup, representing nearly one quarter (22.8%) of the Asian population in the United States and almost half (47.0%) of the Asian population in New York City (NYC; U.S. Census Bureau, 2010). Chinese Americans aged ≥65 years make up approximately 11.8% of the NYC Chinese population and experienced a 49.8% growth between 2000 and 2010; conversely, the overall population aged ≥65 years in NYC increased 5.9% during this same period (U.S. Census Bureau, 2000, 2010). European-born older populations are more likely to have entered the United States prior to 1970, whereas Asian-born older populations began entering following the Immigration Act of 1965, with an influx in the 1970s (He & U.S. Census Bureau, 2002; Trinh-Shevrin, Islam, & Rey, 2009).
Older Chinese Americans in NYC have been overlooked by health providers and policy makers, as data on this rapidly increasing subgroup are often aggregated with other Asian groups, masking possible differences in health. Research suggests that older Asian Americans are a heterogeneous group exhibiting different characteristics from the general aging population (Trinh-Shevrin et al., 2009). For example, older NYC Chinese individuals live in larger households, have lower incomes, and experience more English language limitations than other groups (Asian American Federation of New York, 2003). Local and national surveys of Asian Americans have included few Asian languages, provide limited geographic coverage, and are based on small sample sizes (Islam et al., 2010). Limited research exists on the health of older Chinese Americans, especially in NYC (G. Kim, Chiriboga, et al., 2010; Parikh, Fahs, Shelley, & Yerneni, 2009; Wong, Dixon, Gilbride, Kwan, & Stein, 2013). Although data from the NYC Community Health Survey exist, information is generally aggregated across Asian Americans, Native Hawaiians, and Pacific Islanders and results limited by small sample size (New York City Department of Health and Mental Hygiene, 2012).
Studies focusing on older Chinese Americans reveal this group is at risk for various health conditions, including chronic diseases and poor mental health, which increase with age (Hwang, Chun, Takeuchi, Myers, & Siddarth, 2005; Lau et al., 2005; Rajpathak & Wylie-Rosett, 2011; Shah et al., 2010). Modifiable behavioral risk factors, including inadequate levels of physical activity (PA), smoking, and poor nutrition have an adverse effect on health (Danaei et al., 2009; Mozaffarian et al., 2012), as well as on chronic diseases associated with the leading cause
Good physical and mental health is important for older adults (Drewnowski & Evans, 2001; McGuire, Strine, Okoro, Ahluwalia, & Ford, 2007). PA helps reduce risk of falls and fractures, as well as the risk of depression (Gregg, Pereira, & Caspersen, 2000; Strawbridge, Deleger, Roberts, & Kaplan, 2002). According to the 1998 to 2008 National Health Interview Survey, one third of people aged ≥65 years reported sufficient weekly PA (Carlson, Fulton, Schoenborn, & Loustalot, 2010). Risk of poor mental health varies among different subgroups of Asian Americans. Filipino American women are shown to have better self-reported health than Chinese and Vietnamese American women (Appel, Huang, Ai, & Lin, 2011), while rates of depression have been found to be high among Chinese Americans, and lower among Filipinos and Vietnamese (Takeuchi et al., 2007; Yeung et al., 2004). Mental health issues, however, are often underrecognized and undertreated among these Asian subgroups (Alegria et al., 2008; G. Kim, Jang, Chiriboga, Ma, & Schonfeld, 2010; Yeung, Yu, Fung, Vorono, & Fava, 2006).
Data for this study were obtained from the Racial and Ethnic Approaches to Community Health across the U.S. (REACH U.S.) Risk Factor Survey. The objectives of the current study were to (a) describe the demographic and health characteristics of foreign-born, Chinese Americans aged ≥65 years living in NYC; (b) examine health related quality of life (HRQOL) and health behaviors (i.e., PA, fruit and vegetable intake [F&V intake], and smoking); and (c) examine the factors associated with HRQOL and health behaviors. This study fills an important gap in the knowledgebase about the health of this growing population of older Chinese individuals in the United States, and specifically in NYC.
Method
Study Setting
REACH U.S., supported by the Centers for Disease Control and Prevention (CDC), is designed to mobilize local communities to implement and evaluate community-based strategies to eliminate health disparities within racial and ethnic populations. Surveys were conducted annually in 28 grantee communities as part of evaluation activities. This study used 4 years of aggregated data (2009-2012) from the B Free CEED: National Center of Excellence in the Elimination of Hepatitis B Disparities program site (Pollack et al., 2011; Trinh-Shevrin et al., 2011) that oversampled Asian Americans in NYC.
Study Design and Sample
The survey used an address-based sampling design with geographical information systems technology to target Census tracts with a large density of Asian Americans and was conducted using self-administered questionnaires (60%), telephone interviews (39%), and in-person interviews (1%, 2009). Chinese respondents completed the survey in Mandarin, Cantonese, or English. Household eligibility screening was performed for telephone and in-person interviews. The median response rate over 4 years of surveys was 21% based on Equation #3, the American Association for Public Opinion (2011). A complete description of survey methods can be found elsewhere (Liao et al., 2011). A total of 3,001 respondents self-identified as Chinese American. Of those, 827 were aged ≥65 years. These analyses were limited to foreign-born respondents (n = 805).
Study Measures
Survey items were adapted from the Behavioral Risk Factor Surveillance System (BRFSS) interview, a previously validated survey (Nelson, Holtzman, Bolen, Stanwyck, & Mack, 2001).
Dependent Variables
Health-Related Quality of Life
HRQOL is a health-focused quality of life measure of self-reported physical health, mental health, and social functioning (CDC, 2000) used to understand the health status of a population (Brown et al., 2003). The Healthy People 2020 national health initiative includes health-related quality of life and well-being as one of its four overarching goals for all persons in the United States (U.S. Department of Health and Human Services, 2012). Four previously validated core HRQOL measures (CDC, 2000; Moriarty, Kobau, Zack, & Zahran, 2005; Moriarty, Zack, & Kobau, 2003) were used, including self-reported general health, days of poor physical health in the past month, days of poor mental health in the past month, and days of limited activities due to poor physical or mental health in the past month. General health was categorized as excellent/very good/good and fair/poor, while days of poor physical and mental health and limited activity days were categorized as ≥14 days and <14 days in the past month.
Behavioral Risk Factors
Physical Activity
PA levels were based on the 2008 Physical Activity Guidelines for Americans, which recommends that all adults should perform ≥150 minutes of moderate intensity or ≥75 minutes of vigorous intensity PA weekly (U.S. Department of Health and Human Services, 2008). Respondents were classified as sufficiently active (≥150 minutes/week of moderate PA, ≥75 minutes/week of vigorous PA, or an equivalent combination) or insufficiently active (less than sufficient or no PA).
Cigarette Smoking
Cigarette smoking status was determined using (a) “Have you smoked at least 100 cigarettes in your entire life” and (b) “Do you now smoke cigarettes every day, some days, or not at all?” Those responding “yes” to the first question and “every day” or “some days” to the second question were current smokers. Those responding “no” to the first question were characterized as never smoked, and those responding “yes” to the first question and “not at all” to the second question were former smokers.
Fruit and Vegetable Intake
F&V intake was determined using a six-item food frequency screener. Respondents reported consumption of (a) fruit juice, (b) fruit, (c) green salad, (d) potatoes (not counting fried potatoes or potato chips), (e) carrots, and (f) other vegetables. Healthy People 2010 objectives include consumption of ≥3 daily servings of vegetables and ≥2 daily servings of fruit (U.S. Department of Health and Human Services, 2000). For this analysis, frequencies were combined and adjusted to number of times per day and were dichotomized to ≥5 times per day versus <5 times per day.
Independent Variables
Sociodemographic variables included gender, age, education, and English language spoken at home. Body mass index (BMI) was calculated from self-reported height and weight. World Health Organization (WHO) recommended guidelines for Asians were adopted rather than the standard BMI definition, as a substantial proportion of Asian individuals with a high risk of type 2 diabetes have been found at lower BMI levels than the existing WHO cutoff point of ≥25 for overweight (WHO Expert Consultation, 2004). Asian BMI is defined as <23 (underweight/normal weight), 23 to 27.49 (overweight), and >27.5 (obese).
Additional variables included annual household income, health insurance, recent routine check-up, unable to see a doctor in the past year because of cost, diabetes diagnosis, high blood pressure diagnosis, leisure time PA, flu shot in the past year, and pneumonia vaccine in lifetime. English reading fluency was assessed in Year 4.
Statistical Analyses
Descriptive statistics were performed for all independent variables and stratified by gender. Percentages and standard errors (SEs) are presented. Chi-square tests were run for categorical variables, and t tests were run for continuous variables across gender.
Logistic regression models were run to identify the effects of gender, age, education, home language, and BMI on each outcome variable. Diagnoses of disease, variables with little variation such as health insurance, and variables found to be nonsignificant in bivariate analyses were not included in regression models. Income was excluded due to the large amount of missing responses. Adjusted odds ratios (ORs), 95% confidence intervals (CIs), and p values were reported for all variables in each model. Two-sided p values <.05 were considered statistically significant. Hosmer and Lemeshow goodness-of-fit tests were conducted to test model fit.
SAS-callable SUDAAN 11.0 accounted for the complex sample design; each sample was weighted to reflect the probability of selection, the number of eligible family members, and the age-gender population size of the surveyed population.
Results
Table 1 presents the sociodemographic and health characteristics of the sample, overall and by gender. Significant differences were found by gender. Women were more likely to have health insurance, have had a routine check-up in the past year, have been diagnosed with high blood pressure, and report more days of poor physical health, mental health, and limited activity. Men were more likely to have higher education, higher income, report better English reading fluency (Year 4 only), smoke cigarettes, and perform recommended weekly PA.
Sociodemographics and Health-Related Characteristics of Foreign-Born Chinese Individuals Aged ≥65 Years in New York City by Gender and Percentage (SE).
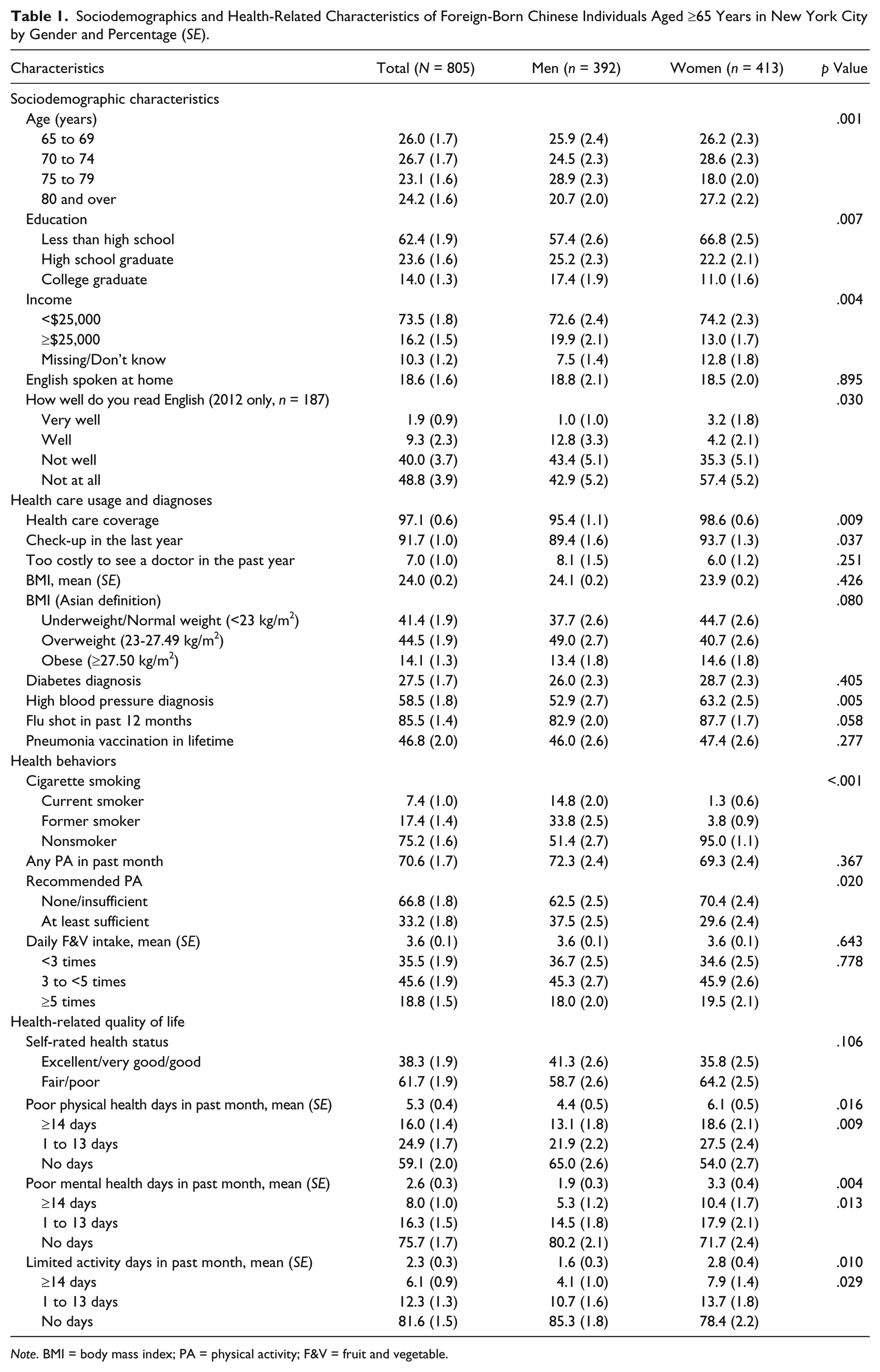
Note. BMI = body mass index; PA = physical activity; F&V = fruit and vegetable.
Significant differences by gender were seen for all HRQOL measures; women self-reported worse health, in addition to a greater number of poor mental health, poor physical health, and limited activity days, when compared with men.
Overall, 66.8% of respondents reported insufficient levels of PA, 7.4% were current smokers, and 81.2% of respondents consumed F&V <5 times per day. Women were significantly more likely to receive insufficient PA and to be current nonsmokers compared with men.
HRQOL Measures
Results from a series of multivariable logistic regressions on HRQOL measures are presented in Table 2. For mental health, women were 2.07 times more likely than men to report ≥14 days of poor mental health in the past month. For physical health, women were 1.65 times more likely than men to report ≥14 days of poor physical health and older age was significantly associated with ≥14 days of poor physical health. For limited activity days, women were 2.06 times more likely than men to report ≥14 days of limited activities and older age was significantly associated with ≥14 days of limited activities. Compared with respondents who completed college, those with less than a high school education or some college education were significantly more likely to report fair or poor health (1.68 and 1.72, respectively). Finally, respondents with a BMI ≥27.5 were 1.80 times more likely than those with a BMI <23 to report fair or poor health.
Predictors of Health-Related Quality of Life Measures Among Foreign-Born Chinese Individuals Aged ≥65 Years, Adjusted Logistic Regression Models.
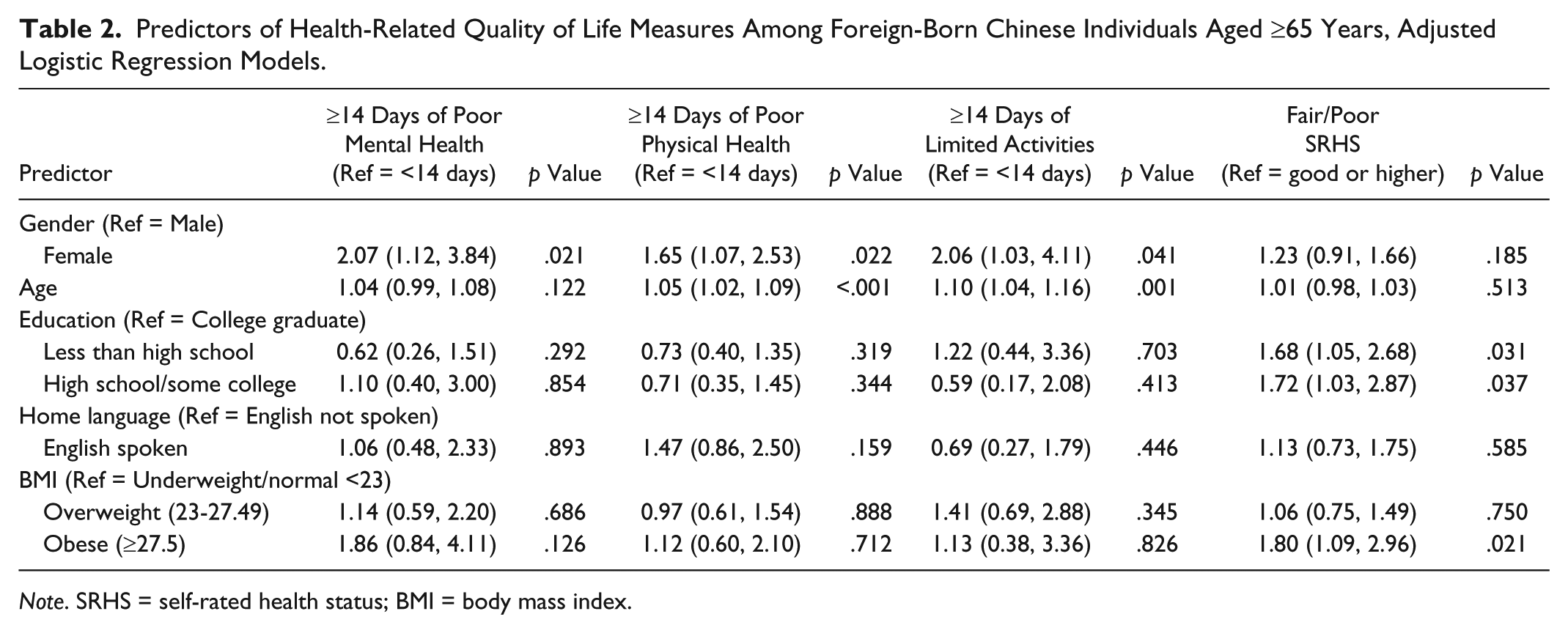
Note. SRHS = self-rated health status; BMI = body mass index.
Behavioral Risk Factors
Results from a series of multivariable logistic regression on behavioral risk factors are presented in Table 3. Few demographic characteristics were significantly associated with the behavioral risk factors. Older age was significantly associated with insufficient PA. Due to the small smoking prevalence among women, adjusted analyses for smoking was only run for men. Men with less than a high school education were 6.13 times more likely than men with a college education to be current smokers and respondents with a BMI ≥23 were less likely than those with a BMI <23 to smoke.
Predictors of Behavioral Risk Factors Among Foreign-Born Chinese Individuals Aged ≥65 Years, Adjusted Logistic Regression Models.
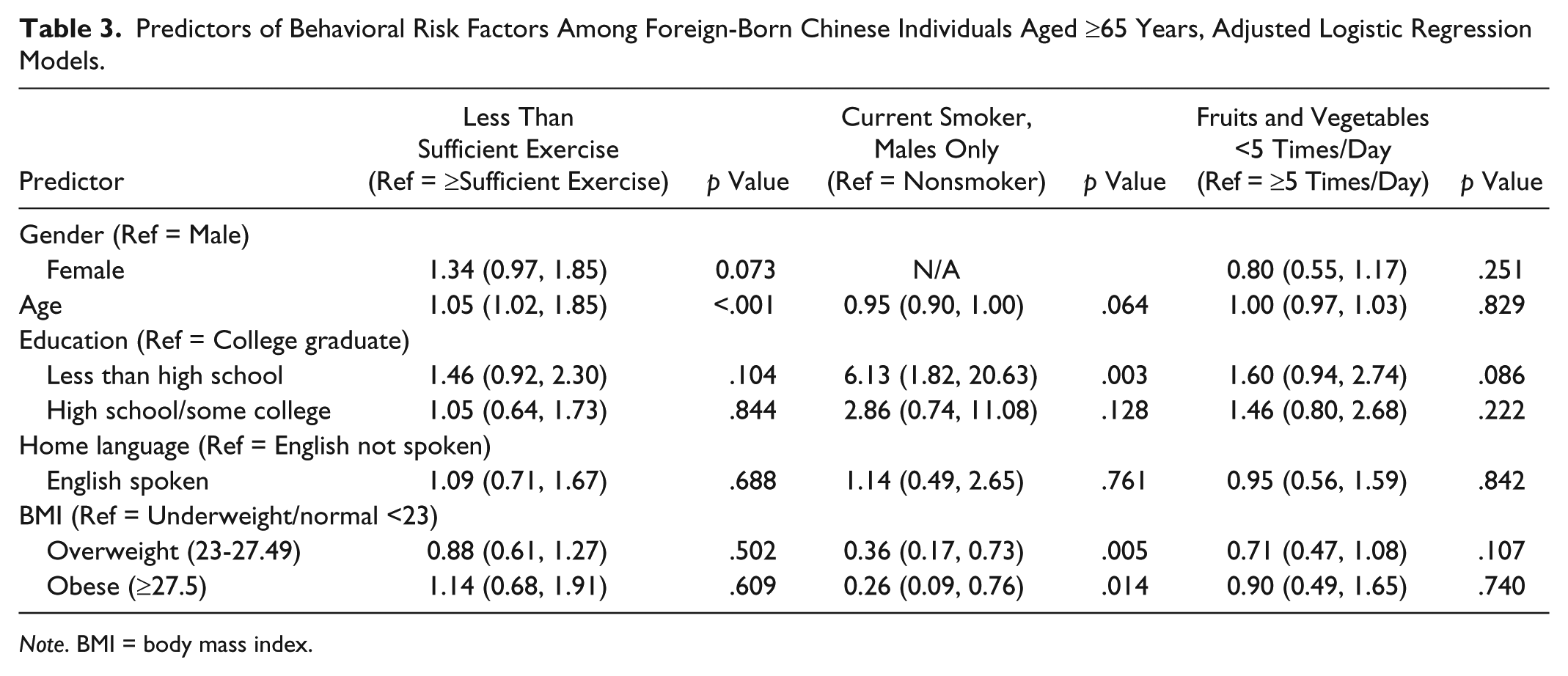
Note. BMI = body mass index.
Discussion
To our knowledge, this is the first study to use a population-based data set to oversample Asian Americans in NYC, providing important descriptive information on health behaviors and HRQOL among a large sample of older, foreign-born Chinese Americans. Men were significantly more likely than women to be current and former smokers. Only a third engaged in sufficient weekly PA, and men were significantly more likely than women to engage in sufficient PA. Among older Chinese respondents, HRQOL measures were generally low; the majority reported fair or poor health and days of poor health were high. Women were more likely to report poor mental health, poor physical health, and limited activity days than men.
Smoking prevalence (7.4%) was similar to overall smoking rates among older respondents in NYC (8.2%) (New York City Department of Health and Mental Hygiene, 2012); however, 14.8% of men and 1.3% of women were current smokers, and 33.8% of men and 3.8% of women were former smokers, similar to previous studies (Li, Kwon, Weerasinghe, Rey, & Trinh-Shevrin, 2013; Maxwell, Bernaards, & McCarthy, 2005; Yu, Chen, Kim, & Abdulrahim, 2002). As shown previously, lower educational attainment is associated with current smoking among men (Parikh et al., 2009). The finding that lower BMI is associated with cigarette smoking has been reported in a study among adults in China (Hou et al., 2008; Xu, Yin, & Wang, 2007), and studies have found that smokers often have lower body weight than nonsmokers (Chiolero, Faeh, Paccaud, & Cornuz, 2008; Flegal, Troiano, Pamuk, Kuczmarski, & Campbell, 1995). While this association is not completely understood, it may be related to an increase in energy expenditure among smokers (Hofstetter, Schutz, Jequier, & Wahren, 1986).
Findings from national BRFSS data report that about half of adults aged ≥65 years perform sufficient PA (CDC, 2011). NYC 2012 data found that 38% of adults aged ≥65 years performed sufficient PA and men are more likely than women to perform sufficient PA (New York City Department of Health and Mental Hygiene, 2012). A California study similarly reported that Asian Americans are less likely than non-Asians to meet recommended PA guidelines (August & Sorkin, 2011). As expected, older age was significantly associated with sedentary behaviors and receiving insufficient PA (DiPietro, 2001). Limitations to the PA measure do not allow us to determine reasons for lower PA rates in our sample. Potential areas for future research include the role of neighborhood factors such as perceptions of safety which have been found to influence PA engagement in older adults (Tucker-Seeley, Subramanian, Li, & Sorensen, 2009), as well as access to parks and walkability of neighborhoods (Wen, Kandula, & Lauderdale, 2007).
While recommended daily F&V intake was low, reported rates among NYC older adults and older Asian adults were lower (11.1% and 13.8%, respectively; New York City Department of Health and Mental Hygiene, 2012). Research in California has shown low F&V intake among all adults; college-educated native- and foreign-born Asians had fewer servings of F&Vs than their less-educated counterparts (Bostean et al., 2013). Due to the limitations of the measures, reasons for low F&V intake among our sample are unclear.
In general, Asian Americans are less likely to report poorer HRQOL when compared with Whites and other groups (Chowdhury, Balluz, & Strine, 2008; Zahran et al., 2005). Prior studies using 1993 to 2001 BRFSS data reported that about one third of adults aged ≥65 years self-reported fair or poor health (Zahran et al., 2005), whereas in our sample two thirds of older adults self-reported fair or poor health. Women in our sample reported more days of poor physical and mental health than men, and similar findings have been shown among overall adults (McGuire et al., 2007; Zahran et al., 2005). Few studies have examined HRQOL specifically among older Asian populations; future studies should examine differences that may exist by ethnic subgroups.
These findings also underscore important study population characteristics. Approximately 62% reported having less than a high school education, similar to previous research on older NYC Chinese Americans (Parikh et al., 2009; Wong et al., 2013). In comparison, 26.9% of Chinese Americans aged ≥60 years in California had less than a high school education (G. Kim, Chiriboga, et al., 2010). However, 89% of the older Chinese Americans from the California data set were foreign-born and 56% had limited English proficiency (G. Kim, Chiriboga, et al., 2010). In contrast, our sample was all foreign-born, and in Year 4, 89% of individuals reported reading English not well or not at all. Our findings are similar to NYC data, which reported that 88% of Chinese age ≥65 years spoke English less than very well (Asian American Federation, 2013).
Study Limitations
These findings have several limitations. The BRFSS F&V intake scale is less valid than other instruments; it may overestimate or underestimate daily intake (D. J. Kim & Holowaty, 2003). Second, key variables of interest, such as time in the United States and English reading fluency, are missing or not included for all years. Research has found correlations between immigration age and health status (Lum & Vanderaa, 2010). Additionally, while health insurance was assessed, type of health insurance was not collected (e.g., private or public). Fourth, some predictor variables had high prevalence and could not be used in logistic regression, such as routine check-up and health insurance. Variables representing access to the health care system specific to older populations would be informative for these analyses.
Implications for Practice
Findings suggest that this population differs from other groups of older adults, underscoring the need for further study. To address modifiable lifestyle behavioral risk factors and HRQOL among older Chinese Americans, strategies and policies should be culturally and linguistically tailored to ensure relevancy and successful uptake. Qualitative interviews among older Asians in NYC suggest the need to enhance access to social supports to improve the quality of life among older Asians coping with immigration-related stressors such as acculturation and language barriers and normal stresses of aging (Asian American Federation of New York, 2003). Yang and Kagawa-Singer (2007) propose that community-based, ethnic subgroup-specific health care organizations with bicultural and bilingual staff are needed to provide appropriate care to subgroups such as aging Chinese. Better understanding of cultural, generational, and linguistic challenges to mental health service utilization is critical in tailoring appropriate mental health and social service programs for this population (Asian American Federation of New York, 2003).
Health promotion programs should incorporate traditional cultures and health beliefs related to diet, as older adults may continue dietary patterns from their home country (Satia-Abouta, Patterson, Kristal, Teh, & Tu, 2002). Nutrition programs have focused on older adults with chronic diseases (Lyons, 2013); high rates of diabetes are shown among NYC Asian subgroups (Gupta, Wu, Young, & Perlman, 2011; Islam, Wyatt, et al., 2013), and several community-based, in-language, nutrition and chronic disease interventions have reportedly decreased chronic disease risk factors among targeted Chinese and other Asian Americans (Chesla et al., 2013; Islam, Zanowiak, et al., 2013; M. T. Kim et al., 2009; Lv & Brown, 2011). Culturally relevant activities such as tai chi are also an effective way to promote PA and improve mental health (Adler & Roberts, 2006; Taylor-Piliae, Haskell, Stotts, & Froelicher, 2006; Wang, Collet, & Lau, 2004; Yeung et al., 2012). Community-based programs and system-level policies tailored to the social and cultural context of aging ethnic subpopulations are necessary to provide appropriate care and services to address chronic disease-related risk factors.
Important gender differences were noted and highlight the need for gender-specific, culturally tailored interventions. While community-based and culturally tailored interventions among Chinese American smokers in NYC and Pennsylvania have shown positive results in improved self-efficacy and smoking cessation (Burton et al., 2010; Fang et al., 2006; Shelley et al., 2010; Wu et al., 2009), additional emphasis should be placed on older Chinese men. Furthermore, primary care–based interventions are needed to improve early detection of mental health concerns, especially among older Chinese women (Appel et al., 2011). Previous research found a significant association between income and poor mental health (Chung et al., 2003; Lubetkin, Jia, & Gold, 2003); the majority of our sample reported income earned less than $25,000 annually, potentially placing them at greater risk. Studies have been proposed to address depression among Asian Americans (Trinh et al., 2011; Yeung, Hails, Chang, Trinh, & Fava, 2011), and a lifestyle intervention among older Chinese immigrants saw positive changes in mental health (Lu et al., 2014). Community-based, culturally tailored interventions and policies that address factors associated with health-related behaviors and outcomes are key to providing services to the aging Chinese community as well as other aging racial and ethnic minority communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The NYU Center for the Study of Asian American Health is supported by the NIH/NIMHD cooperative agreement number 2P60MD000538; the NYU Health Promotion and Prevention Research Center is supported by the Centers for Disease Control and Prevention cooperative agreement number 1U48DP001904 and 1U48DP005008-01.
Supplement Issue Note
This article is part of an open access supplement “Fostering Engagement and Independence: Opportunities and Challenges for an Aging Society,” published in SOPHE’s Health Education & Behavior. This supplement was supported by funding provided by the Centers for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and Health Promotion, Healthy Aging Program (Cooperative Agreement #U38HM000454) via the Association of State and Territorial Health Officials, and from a grant provided by the Retirement Research Foundation. Views presented herein do not represent the official views of the CDC.