
Abstract
Introduction. Based on internal and external assets, the positive youth development approach aims to increase the capacity among adolescents to overcome challenges as they transition to adulthood. Developmental assets have been found to be positively associated with academic achievement, a variety of health promoting behaviors, and improved physical and mental health. The purpose of this exploratory study was to assess the long-term association between positive youth developmental assets with health risk and promoting behaviors. Method. A continuous scale of developmental assets was created using 30 items from Wave I of the National Longitudinal Study of Adolescent to Adult Health, when participants were in 7th to 12th grades. Health behavior outcomes including cigarette use, substance use, fast food consumption, and physical activity were measured at both Wave III (age 18-26) and Wave IV (age 24-32). Path analysis was employed to assess the relationship between these observed measures. Results. The well-fitted path model revealed associations between developmental assets with each health behavior at Wave III. Developmental assets indirectly influenced each health behavior and direct associations were observed between assets with substance use and physical activity at Wave IV. Conclusion. Findings provide additional support for the developmental assets approach to adolescent health. Implications include Healthy People 2020 objectives related to tobacco and alcohol use and nutrition and physical activity.
Keywords
Adolescence has historically been considered a time of chaos and crisis from which negative or risky health behaviors develop (Bowers et al., 2010) and is, as a result, traditionally addressed through deficit-based approaches (Bowers et al., 2010; Lerner, Almerigi, Theokas, & Lerner, 2005). As a result of a recent paradigm shift, the positive youth development model recognizes the complexity of youth and views adolescence as a period of psychological, emotional, social, and intellectual growth (Bowers et al., 2010; Lerner et al., 2005). Accordingly, instead of the traditional view of youth “as problems to be managed” with “deficits,” the positive youth development paradigm regards youth as “resources to be developed” (Roth & Brooks-Gunn, 2003a). As a result, the goal of positive youth development is to develop internal and external assets to increase the capacity among adolescents to overcome challenges through the development of skills and resources as they transition from adolescence to adulthood (Geldhof, Bowers, & Lerner, 2013; Lewin-Bizan, Bowers, & Lerner, 2010).
An asset-building paradigm comprises a systems approach to developing intrapersonal, within-home, and outside-home assets (Atkiss, Moyer, Desai, & Roland, 2011; Catalano, Berglund, Ryan, Lonczak, & Hawkins, 2004; Roth & Brooks-Gunn, 2003a, 2003b). Developed by the Search Institute, the Developmental Assets Framework proposes 40 assets grouped into two categories, internal and external, which serve as the building block of healthy development (Search Institute, 2007). Internal assets described as beliefs, values, and skills needed to engage with others and function in society include (a) commitment to learning, (b) positive values, (c) social competence, and (d) positive identity (Search Institute, 2007). Equally, external assets are described as the external relationships, activities, and structures that create positive environments including (a) positive support, (b) empowerment, (c) boundaries and expectations, and (d) constructive use of time (Search Institute, 2007).
Alignment of internal and external developmental assets have been found to predict school success, leadership, helping others, maintenance of physical health, delayed gratification, valuation of diversity, and overcoming adversity (Scales, Benson, Leffert, & Blyth, 2000). Likewise, developmental asset-based youth development has been shown to affect positive body image (Fenton, Brooks, Spencer, & Morgan, 2010) and a variety of health behaviors including sex health, substance abuse, nutrition, and exercise behaviors (Catalano, Berglund, Ryan, Lonczak, & Hawkins, 2002; Fenton et al., 2010; Glover, Catalano, & Bowes, 2006; Hawkins, Kosterman, Catalano, Hill, & Abbott, 2005; Hoyt, Chase-Lansdale, McDade, & Adam, 2012; Lonczak, Abbott, Hawkins, Kosterman, & Catalano, 2002).
Previous literature regarding the determinants of adolescent health provides support for an asset-building paradigm mobilized through positive youth development programs (Viner et al., 2012). These programs are built on the hypothesis that the more developmental assets attained during adolescence, the greater the likelihood of enhanced health and quality of life over the life course (i.e., accumulative assets principle). A variety of positive youth development programs have been implemented with the goal of improving long-term health via reduction of health endangering behaviors and promotion of health enhancing behaviors during adolescents (Catalano et al., 2002). While many positive youth development programs have been successful at reducing negative health behavior, the majority of evaluations have been cross-sectional in nature, used short-term following (i.e., 6-months postintervention), or focused on just one type of health behavior (Catalano et al., 2002). Although it is still unclear if positive youth development programming in adolescence affects health behaviors in adulthood, a few studies have observed long-term effects. For example, Hoyt et al. (2012) found that positive well-being in adolescence was significantly associated with better perceived general health and decreased risky behaviors including low physical activity, fast food consumption, binge drinking, cigarette smoking, marijuana use, and other illicit drug use in adulthood (Hoyt et al., 2012). Additionally, a longitudinal evaluation of the Seattle Social Development Project revealed fewer mental health disorders and sexually transmitted infections among adults exposed to the intervention 15 years prior (Hawkins, Kosterman, Catalano, Hill, & Abbott, 2008). Further investigation is needed to determine the association between positive youth development and health behaviors in mid and later adulthood.
The current article aims to add to the existing literature regarding positive youth development by exploring the “accumulation of assets” principle. This principle suggests that there is an additive impact of developmental assets whereby having accumulated more assets would generalize into both prevention of high-risk behavior and adoption of health enhancing behaviors. Thus, the current article explores the association between developmental assets in youth with health risk and promoting behaviors measured at two time points in adulthood in a large longitudinal sample. It is hypothesized that greater developmental assets will be associated with reduction of negative health behaviors including cigarette use, substance use, and fast food consumption, and increases of positive health behavior including physical activity, both in young adulthood (age 18-26) and adulthood (age 24-32).
Method
The current study comprises a secondary analysis of the National Longitudinal Study of Adolescent to Adult Health (Add Health). Add Health is a longitudinal study that investigates social, behavioral, and biological factors across the life course. The study began in 1994 with adolescents in 7th through 12th grades. At Wave I a total of 20,745 adolescents were interviewed. There have been four subsequent waves of interviews with the most recent, Wave IV, in 2008 (Harris, 2011; Harris, Halpern, Whitsel, Hussey, & Tabor, 2009). For further information regarding sampling and questionnaire design, see http://www.cpc.unc.edu/projects/addhealth. The current study utilized data from Wave I (Grades 7-12), Wave III (age 18-26), and Wave IV (age 24-32).
Measures
Developmental Assets Scale
Based on the Developmental Assets Framework (Leffert et al., 1998; Search Institute, 2007), a continuous scale of internal and external developmental assets was constructed using items from Wave I that were selected to align with the 40 developmental assets. An initial pool of 113 items was selected from Wave I of the Add Health questionnaire. Some of the original 40 developmental assets were not represented (e.g., cultural competence, equality and social justice, reading for pleasure). In total, 32 of the original 40 were represented in the initial item pool.
In the first phase of scale development, a positive youth development expert assessed the initial item pool. Based on the expert’s assessment, the pool was reduced to 69 items that were then included in a series of exploratory factor analyses. Several external assets focus on family and parents; thus, participants that reported no resident or biological parent were excluded (n = 100). This represented adolescents with no relationship with their biological parents who were living with a non-mother and/or non-father figure. This left a sample size of 20,645 participants included in exploratory factor analyses.
To determine the underlying factor structure of the selected pool of items, as well as to confirm that the scale aligned with the 40 developmental assets, principal axis factoring was performed with a promax rotation. A cutoff of an eigenvalue of one or greater prior to rotation was selected for factor extraction, and a visual inspection of the scree plot was used to confirm the number of selected variables. Items were retained if they loaded significantly (>0.4) on one and only one of the rotated factors.
The result of the Kaiser–Meyer–Olkin measure of sampling adequacy suggested adequate sample size (.751), and Bartlett’s test of sphericity was significant (χ2 = 80127.102, p < .001, df = 406). Item reduction resulted in a solution of 10 factors consisting of 30 items, shown in Table 1. The eigenvalues for the 10 extracted factors ranged from 1.15 to 4.30 and accounted for 62.2% of the total variance. The results of the scree plot also supported the 10-factor solution. The 10 factors aligned with the developmental assets described by the Search Institute (Search Institute, 2007), and were grouped into five external asset factors and five internal asset factors accordingly. While the resulting factor solution did not represent all the developmental assets, it provided a significant range of both external and internal assets. External asset factors included family support, parent involvement in school, caring neighborhood, family encouragement, and high expectations. Internal asset factors consisted of self-esteem, positive view of personal future, sense of purpose, interpersonal competence, and bonding to school.
Principal Axis Factoring Results of Developmental Assets Scale.
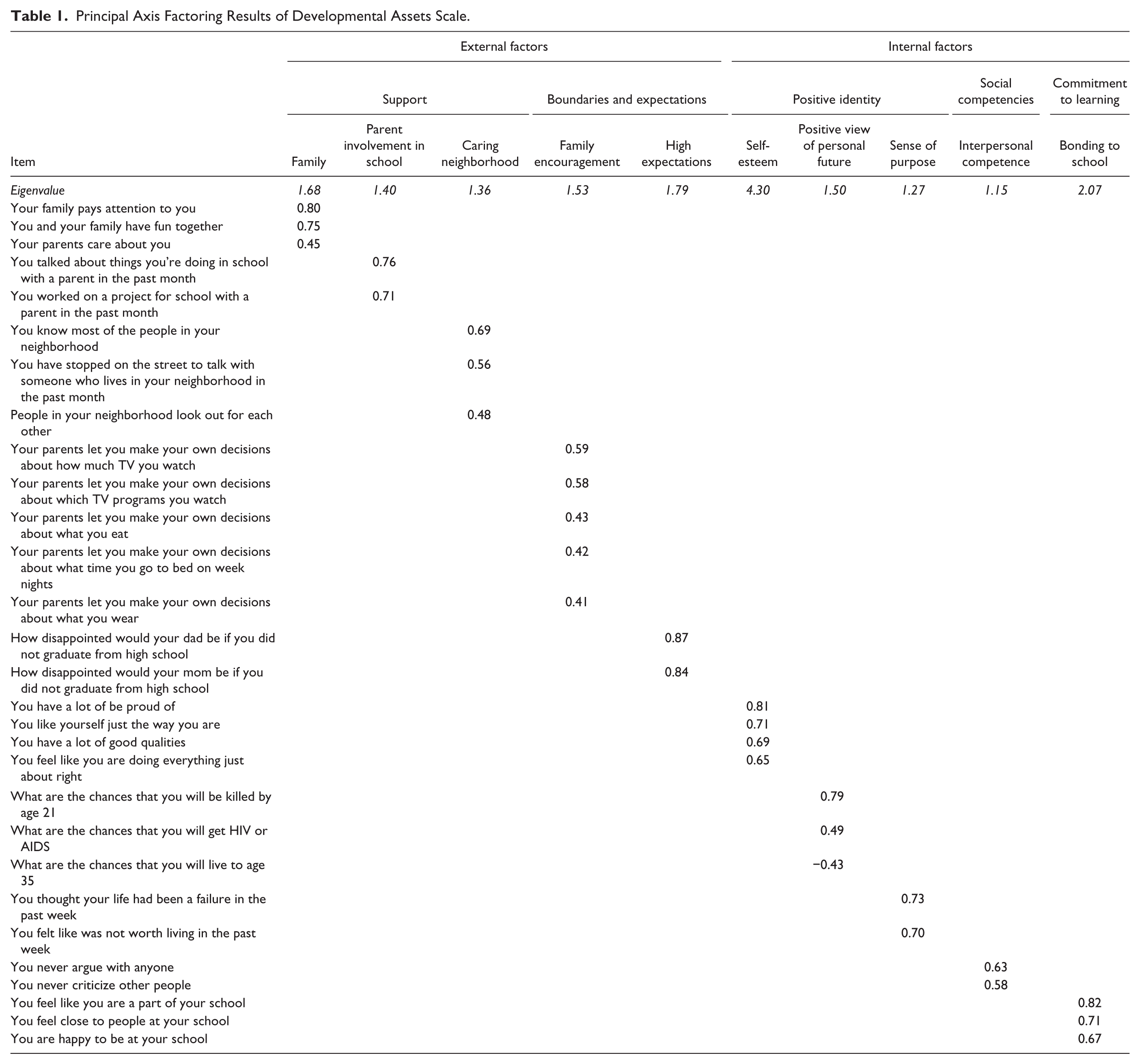
Of the selected items, 17 were scored on a 5-point Likert-type scale, 4 were scored on a 4-point Likert-type scale, and 10 were scored as yes (1)/no (0). Based on the research questions associated with the current study as well as structure of the 40 developmental assets framework, two continuous scales, one of external assets and one of internal assets, were constructed. A sum score was calculated per factor. Then each factor was dichotomized with a cutoff at the 50% percentile. There was one exception in that the family expectation score was not calculated as a sum score but rather the maximum score between the two items; accounting for the fact that many adolescents came from single-parent households. The two scales were calculated as the sum of the binary factors within each scale (external and internal); thus, scores for each scale ranged from zero to five. One continuous scale of development assets was calculated as the sum of the two scales.
Health Behavior Outcomes
Behavioral outcomes, specifically cigarette use, substance use, fast food consumption, and physical activity, were measured via binary indicators at both Wave III and Wave IV. Participants were considered to use cigarettes if they reported any cigarette smoking in the past 30 days. Participants were considered to have reported substance use if they reported any use of marijuana or any other illegal drugs, including cocaine, crystal meth, and injected drugs in the past year. As an indicator of nutrition, fast food consumption was measured as having consumed fast food on two or more days (Wave III) or two or more times (Wave IV) in the past week. Lastly, physical activity was measured via six items at each wave. Participants were considered to be physically active if they reported doing any combination of the following activities five or more times in the past week: bicycle, skateboard, dance, hike, hunt, or yard work; roller blade, roller skate, downhill ski, snow board, play racquet sports, or aerobics; participate in strenuous team sports such as football, soccer, basketball, lacrosse, rugby, field hockey, or ice hockey; participate in individual sports such as running, wrestling, swimming, cross-country skiing, cycle racing, or martial arts; participate in gymnastics, weight lifting, or strength training; or play golf, go fishing or bowling, or play softball or baseball; or walk for exercise (Gordon-Larsen, McMurray, & Popkin, 2000; Gordon-Larsen, Nelson, & Popkin, 2004).
Participants
A total of 13,034 of the original 20,745 participants completed interviews at all three waves. Of the respondents that completed all waves, those that were missing data on the assets scale or any of the behavioral health outcomes were excluded from analysis. Moreover, based on the school and family specific assets, participants that reported not being in school or not living with and not having a relationship with a parent were also excluded. This left a final sample size of 11,719 participants included in the current analysis. There were no differences between those included and those excluded with regard to demographic factors, developmental asset, and health behaviors.
Statistical Analysis
Structural equation modeling techniques were used to explore the hypothesized relationship between developmental assets in adolescence with behavioral health outcomes at two time points in adulthood. In MPlus, weighted least squares means and variance adjusted (WLSMV) was used to estimate the path model. WLSMV was used to account for the binary or categorical nature of the health behaviors outcomes (Proitsi et al., 2011). Several fit indices were used to evaluate model fit, including chi-square test of model fit, comparative fit index (CFI), root mean square error of approximation (RMSEA), and weighted root mean square residual (WRMR). Indicators of good model fit are as follows: chi-square test of model fit (p > .05), CFI (>.95), RMSEA (<.06), and WRMR (<1.0; Schreiber, Nora, Stage, Barlow, & King, 2006; Yu, 2002). The path model included an investigation of the mediating effects of each health behavior at Wave III on the relationship between developmental assets and the given health behavior at Wave IV.
Results
Participants
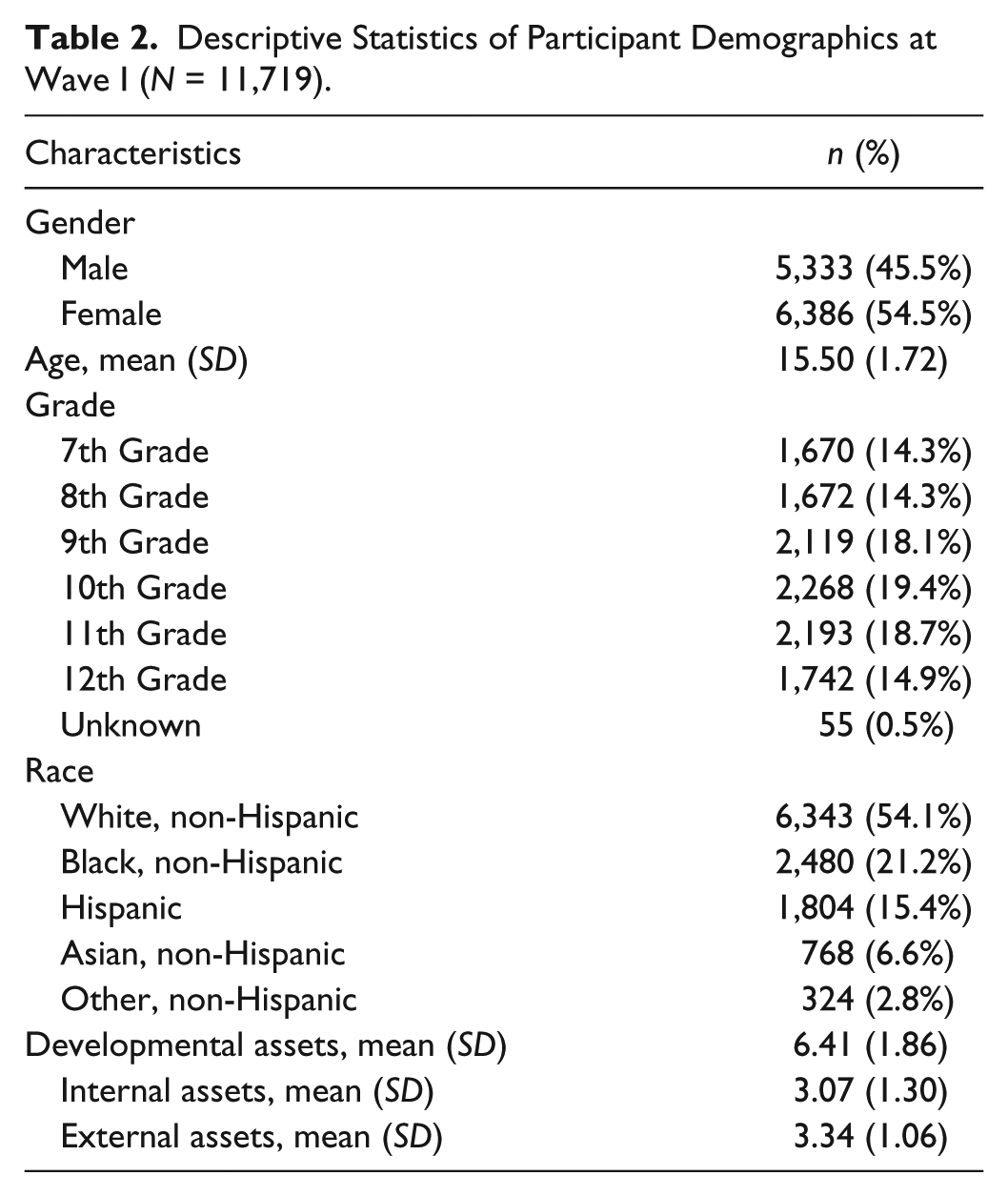
Table 2 displays demographic information for the 11,719 participants included in the analysis. The majority of the sample was female (n = 6,386; 54.5%) and White (n = 6,343, 54.1%), with a mean age at Wave I of 15.50 years (SD = 1.72). On average respondents reported 6.41 (SD = 1.86) developmental assets (out of 10 possible assets); more specifically, 3.07 (SD = 1.30) internal assets (out of five possible assets) and 3.34 external assets (out of five possible assets).
Descriptive Statistics of Participant Demographics at Wave I (N = 11,719).
Prevalence of Health Behavior
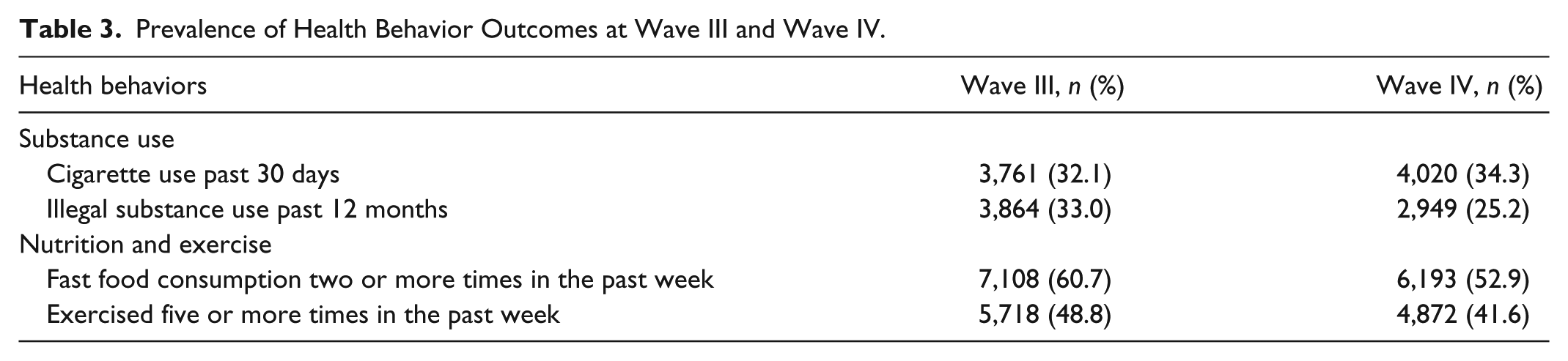
Table 3 displays the prevalence of each health behavior outcome at Wave III (age 18-26) and Wave IV (age 24-32). At Wave III, 32.1% of participants (n = 3,761) reported cigarette use in the past 30 days. In comparison, 34.3% (n = 4,020) of participants reported past month cigarette use at Wave IV. A total of 33.0% (n = 3,864) of participants at Wave III reported illegal substance use in the previous year; this rate dropped to 25.2% (n = 2,949) at Wave IV. In terms of nutrition and exercise, 60.7% of participants (n = 7,108) reported eating fast food two or more times in the previous week, which dropped to 52.9% (n = 6,193) at Wave IV. Last, 48.8% (n = 5,718) of participants reported exercising five or more times in the previous week, as well nutrition, this also slightly dropped at Wave IV to 41.6% (n = 4,872). At both waves, these four health behaviors were correlated with each other. As can be seen in Table 4, at Wave III all health behaviors were correlated with one another (p < .001), with the exception of fast food consumption and substance use. Similarly, the majority of health behaviors were correlated at Wave IV (see Table 4; p < .001) with the following exceptions: there was no correlation between physical activity and cigarette use, or physical activity and substance abuse, and the correlation between fast food consumption and substance use was significant at the p < .05 level.
Prevalence of Health Behavior Outcomes at Wave III and Wave IV.
Correlation Matrix of Health Behavior Outcomes at Wave III.

p < .05. **p < .01. ***p < .001.
Long-Term Effects of Developmental Assets
The resulting path analysis model is displayed in Figure 1. In an effort to simplify the model, only paths related to the main outcomes are shown. Correlations, which can be found in Tables 3 and 4, are not displayed in the model. The model fit the data well with the following fit indices: χ2(df = 12) = 56.96, p < .001, RMSEA = .02, CFI = .998, and WRMR = .981. All indices indicate good fit with the exception of the chi-square statistics. However, as the chi-square statistic is very sensitive to sample size it cannot be accessed alone. Moreover, in the given analysis, it can be assumed that the chi-square statistic was affected by the sample size (n = 11,719), as the statistic is often significant (i.e., poor fit) with samples over 400 observations. In addition, the residual output indicates no residuals over 2.0, further suggesting that the model fits the data.
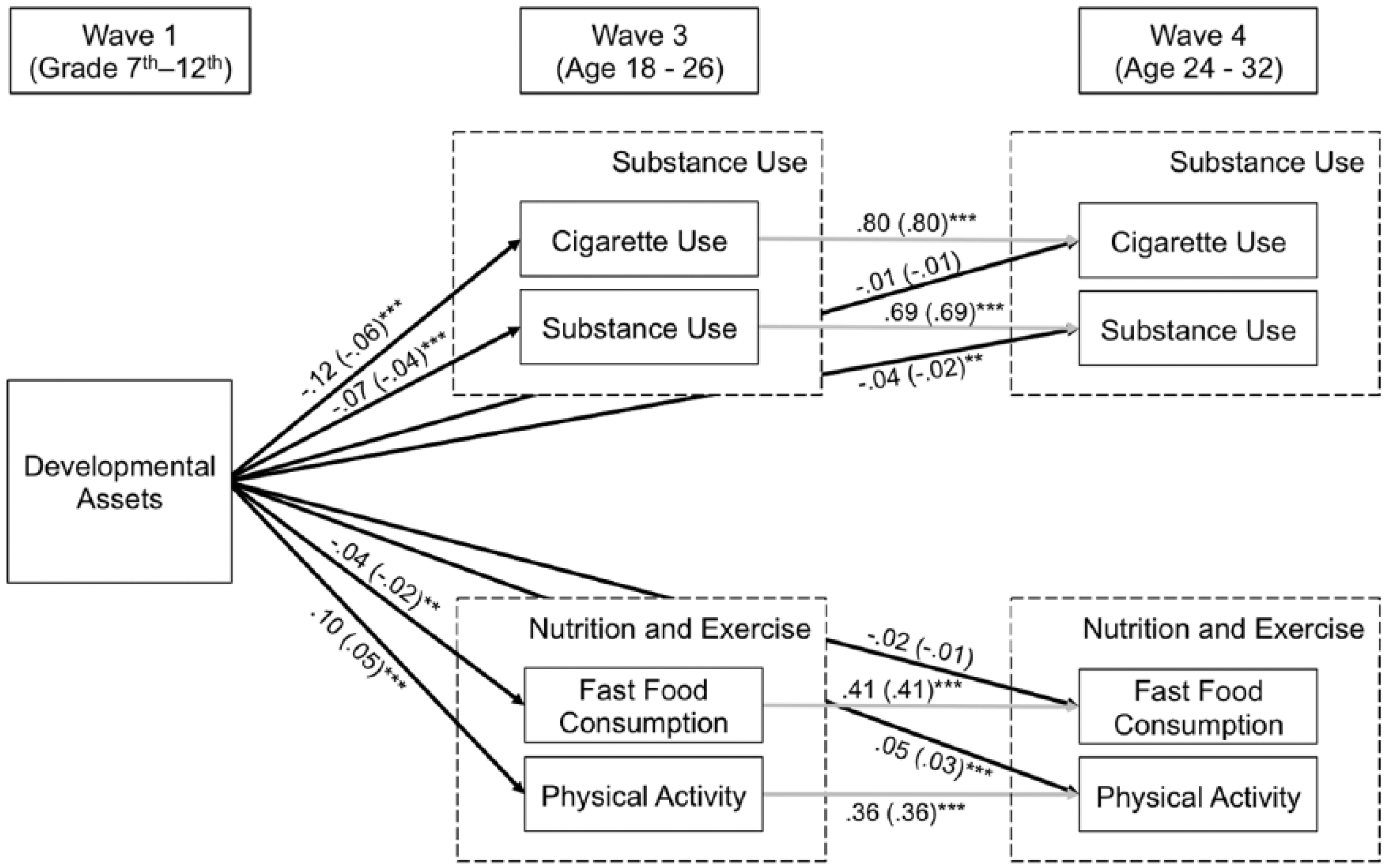
Path model of the relationship between developmental assets in adolescence and health behaviors at two points in adulthood.
As can be seen in the path analysis, the number of developmental assets reported significantly predicted the four health behavior indicators at Wave III; however, the magnitudes of these relationships were generally small. Specifically, greater developmental assets were associated with less cigarette smoking, substance use, and fast food consumption, and more physical activity. There were only two significant direct effects of developmental assets with health behavior outcomes. Greater developmental assets were directly associated with increased physical activity and decreased substance use at Wave IV. There were no direct effects from developmental assets in adolescence to either fast food consumption or cigarette use at Wave IV.
While there were only two direct effects, there were several mediating pathways. Each health behavior at Wave III was positively associated with the same health behavior at Wave IV, thus serving as mediators between developmental assets and Wave IV outcomes. For example, although the number of developmental assets did not directly predict cigarette use at Wave IV, the greater number of developmental assets was associated with less cigarette use at Wave III, which then influenced cigarette use at Wave IV.
Discussion
This exploratory study provides support for the association between developmental assets in adolescence and engaging in health risk and promoting behaviors in adulthood. Specifically, the hypothesis is supported in that developmental assets observed during grades 7th to 12th were associated with each health behavior outcome at age 18 to 26. However, mixed findings were obtained in regard to the relationship with health behaviors later in adulthood. While developmental assets were indirectly associated with each health behavior at age 24 to 32, only two direct associations were observed. Developmental assets in adolescence were significantly and directly associated with the odds of substance use and physical activity at age 24 to 32. Although exploratory in nature, these findings provide additional support for asset-based positive youth development programming.
Findings from the current study demonstrate a relationship between developmental assets and health behaviors at age 18 to 26, which is consistent with previous findings (Hoyt et al., 2012). However, although novel, findings regarding the association at the second time interval, age 24 to 32, provide mixed results, and call for further investigation of these associations. Direct effects of development assets were observed in regard to physical activity and substance use, thus suggesting that increasing positive youth development during adolescence may have lifelong implications for these behaviors. However, developmental assets only indirectly influenced cigarette use and fast food consumption through the mediating effects of the behavior at a younger age. For example, increased development assets were associated with decreased odds of cigarette use. In turn, cigarette use between age 18 and 26 was highly predictive of cigarette use between age 24 and 32. Thus, via this indirect pathway developmental assets have an impact on long-term health behavior outcomes. However, the lack of direct association of developmental assets with cigarette use and fast food consumption calls for other approaches to influence health promotion in adulthood. These findings may suggest that the mechanisms that influence these behaviors differ throughout the life course. Even with the positive impacts of increased developmental assets, additional interventions may be needed in young adulthood to maintain the avoidance of these risky health behaviors. As this is the first investigation of the influence of positive youth development in adolescence on health behaviors in the 24- to 32-year-old age range, additional investigations and evidence is needed to support these findings. It should be noted that while significant associations were found, the magnitude of the resulting associations were very small. More information is needed from future studies to both verify these findings and to determine the practical significance of these associations. Additionally, the current study did not explore differences of the implications of positive youth development between gender, racial, and age groups. Future model replications are needed with tests for the moderating effects of these demographic factors on the model.
Although the longitudinal approach to the current exploratory study is novel, several limitations must be considered in interpretation of results. First, all data were self-report and although longitudinal in nature, the data were analyzed using cross-sectional techniques. Second, the model is also missing several key adolescent behavioral health factors such as alcohol abuse and sexual health. Initial analyses included indictors of binge drinking, problematic drinking, number of sexual partners, and age of sexual initiation; however, due to limitations with these measures and an overall lack of model fit to the data, these behaviors were excluded from the model presented in the current study. Future analysis is needed to investigate the impact of developmental assets on these and other health behaviors. Lastly, based on the inclusion of family- and school-related assets, several participants were dropped because they reported not being in school or having no relationship with a biological or residential parent. This group may be empirically different from those included in analysis and may represent an at-risk subset of adolescents. Although the current study provides novel information regarding the long-term impacts of positive youth development, many positive youth development programs target this at-risk group. Future studies are needed to determine the long-term impacts of positive youth development programs on adolescents that are not in school and/ or do not have parental relationships.
Despite limitations, the current study provides support for the expansion of positive youth development programs aimed at improving overall health. More specifically, programs that focus on developing internal and external developmental assets may decrease the likelihood that youth engage in unhealthy behaviors such as tobacco and other substance use and increase the likelihood of engaging in healthy eating and physical activity behaviors. The importance of adolescent health is demonstrated by its inclusion as a new topic area in the Healthy People 2020 report of national health objectives (U.S. Department of Health and Human Services, 2012). Healthy People 2020 states that adolescence is a time in life when public health and social problems begin, specifically mental health issues, substance abuse, smoking, sexually transmitted infections, and unplanned pregnancies (U.S. Department of Health and Human Services, 2012). In a description of the Healthy People 2020 adolescent health topic area, it states that adolescents are affected either negatively or positively by contextual or environmental factors such as family and peer support, school, and neighborhood (i.e., external supports; U.S. Department of Health and Human Services, 2012). Based on the influence of contextual factors, positive youth development interventions are cited as an area for further investigation for addressing adolescent health issues (U.S. Department of Health and Human Services, 2012). Findings from the current study suggest that a developmental assets approach could influence both adolescent health as well as several adult Healthy People 2020 objectives related to tobacco and alcohol use and nutrition and physical activity. Likewise, by influencing these health behaviors, positive youth development programs may indirectly affect rates of diabetes, cancer, and heart disease, all of which are addressed among the Healthy People 2020 objectives and additionally are considered major public health concerns (U.S. Department of Health and Human Services, 2012). Continuing investigation is needed to determine the long-term effects of positive youth development on health via exploration of additional behavioral health issues as well as health outcomes later in life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.