
Abstract
Objectives. We explored the effect of a culturally targeted calorie label intervention on food purchasing behavior of elementary school students. Method. We used a quasi-experimental design with two intervention schools and one control school to assess food purchases of third through fifth graders at standardized school food sales before and after the intervention (immediate and delayed) in schools. The intervention comprised three 1-hour assembly-style hip-hop–themed multimedia classes. Results. A mean total of 225 children participated in two baseline preintervention sales with and without calorie labels; 149 children participated in immediate postintervention food sales, while 133 children participated in the delayed sales. No significant change in purchased calories was observed in response to labels alone before the intervention. However, a mean decline in purchased calories of 20% (p < .01) and unhealthy foods (p < .01) was seen in immediately following the intervention compared to baseline purchases, and this persisted without significant decay after 7 days and 12 days. Conclusion. A 3-hour culturally targeted calorie label intervention may improve food-purchasing behavior of children.
Keywords
One third of the total calories of food consumed by Americans are from food prepared outside of the home in a variety of food outlets (Guthrie, Lin, Okrent, & Volpe, 2013). The menu label legislation contained in Section 4205 of the Affordable Care Act mandating calorie postings in chain restaurants with 20 or more outlets is an attempt to help Americans make better food choices when eating away from home. Some studies have shown that restaurant patrons purchase fewer calories in response to posted point-of-purchase calories (Krieger et al., 2013), while other studies have shown no effect on purchasing behavior (Black, 2014). Regarding young children and low-income individuals, data on menu-labeling effects are limited, with reports showing negligible influence on the food-purchasing habits of these groups (Elbel, Kersh, Brescoll, & Dixon, 2009; Tandon et al., 2011). Theoretically, menu labeling could have powerful behavioral effects on reducing weight gain and diet-related diseases; indeed the Food and Drug Administration has estimated that if 0.6 percent of the adult obese population limit caloric consumption by 100 calories the desired benefits of menu label legislation could be realized (U.S. Department of Health and Human Services, Food and Drug Administration, 2014).
The gap between menu label policy and practice is largest among low-income groups and the youth (Elbel et al., 2009; Tandon et al., 2011), and little is known about the type of consumer education required to increase the use of menu labels among these groups. Children, the focus of this study, are playing a greater role in family food-purchasing decisions (Holsten, Deatrick, Kumanyika, Pinto-Martin, & Compher, 2012; O’Dougherty, Story, & Lytle, 2006) and typically choose their own meals when visiting restaurants with their parents (Tandon et al., 2011). With this background, we developed an educational intervention designed to motivate children to use point-of-purchase calorie postings in dietary decisions. The intervention is modeled on a previously developed culturally targeted multimedia intervention for stroke-related behaviors called Hip Hop Stroke (Williams, DeSorbo, Noble, & Gerin, 2012; Williams, DeSorbo, Noble, Shaffer, & Gerin, 2012; Williams & Noble, 2008), which we have now adapted for a contextual menu label intervention that targets energy balance behaviors of children called Hip Hop HEALS (Healthy Eating And Living in Schools; HHH). Cultural targeting was designed to increase identification, interest, and realism of our intervention to low-income minority schoolchildren using elements of hip-hop culture and age-appropriate media. In a prior report we showed that our intervention increases children’s menu label literacy, which we define as knowledge of major chain restaurant menu board terminology, abbreviations, and calorie ranges posted, along with basic numeracy required for calculating caloric content of meals (Williams, Sawyer, & DeSorbo, 2011); we now explore its effect on food purchasing behavior.
Method
We used a quasi-experimental design with intervention and control arms to assess food-purchasing behavior change of third through fifth graders (ages 8-11) recruited as targeted classes using standardized snack food sales during lunch recess in schools. Three New York City schools from low-income neighborhoods matched by Peer Index (PI) were randomly assigned to no intervention (School A) or intervention (Schools B and C) arms. PI is the percentage of the students who are eligible for free lunch × 30 + percentage of students with disabilities × 30 + percentage of Black/Hispanic students × 30 + percentage of English language learners × 10. For elementary schools, a higher PI indicates a higher need population. PI scores for school A, B, and C were 55, 46, and 50 respectively, which are considered high-need. In the intervention Schools B and C, we conducted the HHH intervention in school auditoriums to whole grades. Small kiosks were set up in high student traffic locations (near the cafeteria) where standardized food sales were conducted, and the food-purchasing behavior of children was measured. Only children from targeted classes were permitted to participate in the food sales. Children’s food purchases were then analyzed for caloric content and nutrient value at baseline and immediately (the next day) following the intervention. Additionally, delayed food sales were conducted 7 days after the intervention (School B) and 12 days after the intervention (School C). In School A where no intervention (HHH program) occurred, food sales were conducted at similar intervals as the intervention schools. To assess the independent effect of calorie labels on food purchases, we conducted two baseline food sales in all three schools. The first sale was performed without calorie labels on food items, and the second preintervention sale was performed with calorie labels on food items. All snack food items sold at food sales were selected based on availability in neighborhood bodegas, chosen via a focus group of representative students, and approved by a nutritionist (Vallance, Murray, Johnson, & Elavsky, 2011). All student snack purchases were anonymous, and sale staff collected only information on the child’s class/grade as this was required to participate in the sale, and signage was posted to reflect this by each kiosk. An important aspect of the intervention was that the children were not aware that their food purchases were being monitored, and to facilitate this, a separate team, not involved in the delivery of the intervention, conducted the food sales. All snacks were priced at $0.50, and only one snack was permitted per child at each sale. Parents from targeted classes were sent a letter from the school principal the day before each sale to alert them of the sale and ask them to give their child 50 cents. Although all children in the targeted classes of intervention schools participated in the HHH intervention, only those with 50 cents were permitted to participate in the food sales. All proceeds from the food sales were donated to the school.
The Intervention
The goal of HHH is to help children engage in an informed cost–benefit analysis that will keep unhealthy eating to a minimum and promote energy balance behaviors. HHH teaches children how to make an informed decision regarding a food purchase based on posted calories (menu label literacy) and nutrient density using a traffic light model (Savoie, Harvey, Ann Binnie, & Pasut, 2013). The target age-group for the HHH intervention is third through fifth graders because students below third grade may lack the basic math skills required to make the necessary computations when interpreting calorie postings on menu boards (Cohn, Larson, Araujo, Sawyer, & Williams, 2012). Specifically, the intervention uses animated musical cartoons as a motivating tool, along with video games, songs, and comic books (Figure 1) to teach child consumers the following: (1) what calories are and why they are important, (2) how many calories they need to consume on a given day based on individual caloric needs, (3) how to distinguish between healthy and unhealthy foods using a traffic light model, and (4) the general meaning of calorie ranges posted for food items, which may include sides and drinks, toppings and fillers, different flavors, condiments, or types of bread and crust. The cartoons and music are incorporated into digital PowerPoint-based program modules, and the video games are components of homework activities that are accessed online and played at home. Children were also given hard copies of comic books within which are contained interactive pages for parental participation and that can also be viewed and/or downloaded online. The intervention, which occurs in the school auditorium as an assembly-style program, is conducted as a “loading dose” in three 1-hour sessions (Table 1) on 3 consecutive days and “maintenance doses,” which our group has since integrated into a fourth-grade math curriculum and which was not part of the current study. The 3-hour loading dose was selected based on our pilot experience regarding the time required to complete intervention components and satisfy our desired exposure frequency to our media. This exposure frequency or number exposures to the cartoons was selected based on theories governing “effective frequency” from marketing studies. “Effective frequency” is defined as the number of exposures to an advertising message required for achieving effective communication and influencing consumer purchasing behavior. It is generally accepted that a single exposure, if relevant to the recipient’s concerns, may achieve effective communication; however, the marketing literature suggests that repeated exposure will be more effective and that a minimum of three exposures may be required (Krugman, 1972). We then decided to deliver our loading dose over 3 days in three 1-hour sessions due to logistical constraints in schools and the need to optimize student attention spans. To ensure age appropriateness and cultural targeting, each HHH module and media tool, were developed iteratively, through focus groups with target children and a process of real-world trial-and-error implementation that involved more than 12,000 Black and Hispanic fourth to sixth graders in high-need New York City public schools over an 18-month period. This process was guided by a transdisciplinary team that included a nutritionist, an exercise physiologist, two public health researchers, two physicians, one behavioral scientist, one schoolteacher, a team of hip-hop artists, a children’s television writer/producer (formerly of Sesame Street), and a 16-member fifth-grade student advisory board from high-need public schools located in minority neighborhoods. Hip-hop music was the final vehicle of choice on which educational modules and media tools were built, and each storyboard and artistic concept included cultural themes, cues, and nuances derived from our developmental process.
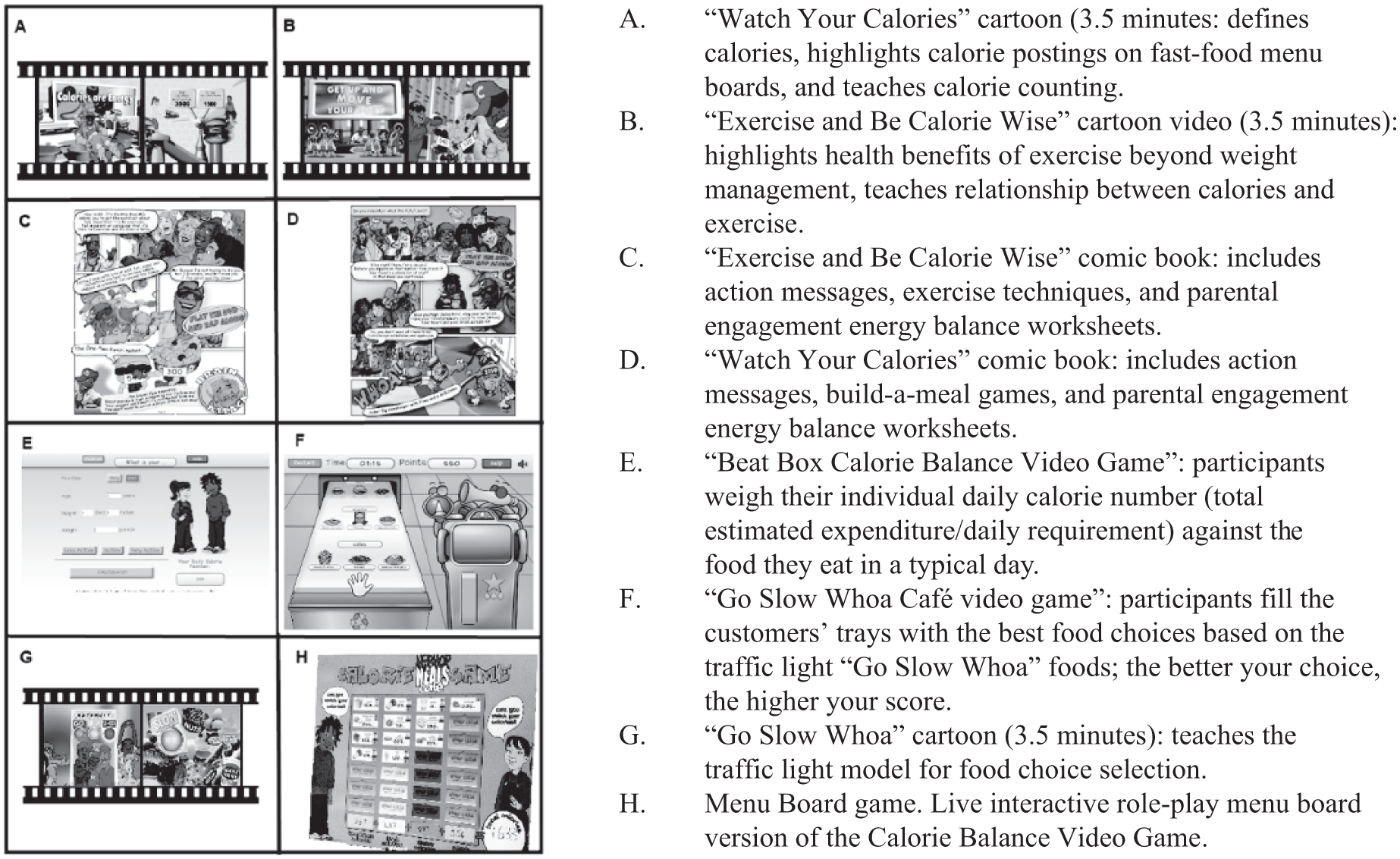
Hip Hop HEALS multimedia tools.
Hip Hop HEALS “Loading Dose” Multimedia Curriculum.

Theoretical Underpinnings of the Intervention
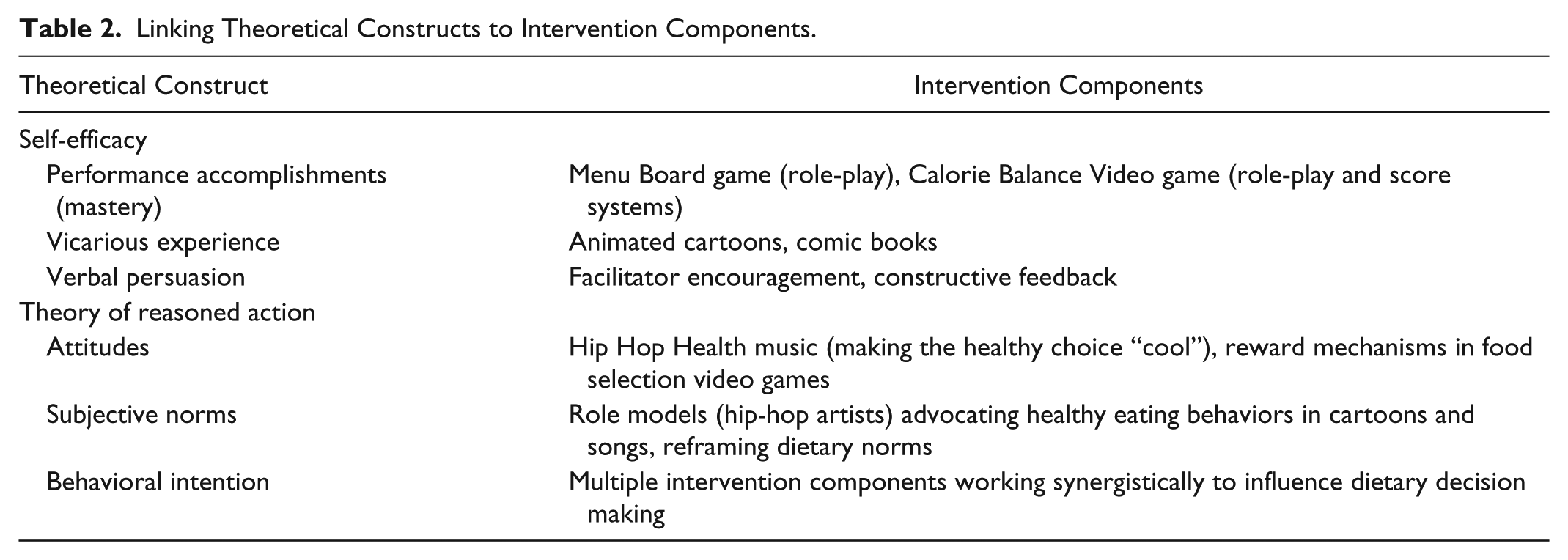
Three constructs have been shown to be key to fostering risk-related behavior change. (1) Theory of reasoned action (Gittelsohn et al., 2006) addresses the decision-making process for the children who are the primary targets of the intervention (Fishbein, 2008). (2) Social cognitive theory (SCT) posits that control over one’s outcomes produces a sense of mastery, or self-efficacy for those behaviors, and that increased self-efficacy leads to increased motivation to engage in the desired behavior (Parcel et al., 2009). (3) A positive feedback loop occurs, in which the provision of the number of calories in reference to the child’s daily caloric requirement serves to reinforce food-purchasing behavior goals; to the extent that the child begins to successfully engage in the desired behavior–ingesting fewer calories from healthier sources—self-efficacy is built up, which is known to motivate adherence. These constructs are built into the intervention (Table 2) to foster behavior change in children, including their role as part of the health management family structure; this is a means for increasing the children’s self-perception as agents of change and establishing this as a desired behavior.
Linking Theoretical Constructs to Intervention Components.
Descriptive and Comparative Statistics
Descriptive statistics were prepared for all measures using frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Comparisons between intervention groups or time points were made using chi-square tests or Fisher’s exact tests for categorical measures and analysis of variance for continuous measures. When overall testing was significant, pairwise comparisons were conducted. All hypothesis testing was two-sided, and p values less than .05 were considered statistically significant. All analyses were conducted using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). This study was approved by the institutional review boards at Columbia University Medical Center and at the New York City Department of Education.
Results
A mean total of 225 third- through fifth-grade students (aged 8-11 years) participated in the two baseline sales. Two hundred students participated in the first baseline food sale without labels, including 73(out of 95) students at our control school and 127 (out of 176) at our two intervention schools, while 251 (out of 271) students participated in the second baseline food sales with calorie labels across all schools. Overall, calorie labeling alone was not associated with any significant differences in food purchasing for any single food item or Nutrient Density group (p > .05; Table 3). No significant changes in food-purchasing behavior were observed across three sales in the control school (p > .05; Table 3). One hundred and forty-nine students participated in immediate postintervention food sales, while 133 students participated in the delayed postintervention food sales (at 7 and 12 days) in both intervention schools (Table 4). At baseline in the intervention schools, no significant change in caloric content or nutrient value was observed with and without calorie labels (179 calories with labels, 175 calories without labels; p >0.05; Table 3). Immediately following the intervention, the mean number of calories per snack for the intervention schools declined significantly in intervention schools (179 calories at baseline vs. 144 calories immediate post intervention—a 20% reduction; p < .01; Table 3). Additionally, significant improvement occurred in the percentage of students purchasing “Go” foods immediately following the intervention (8% at baseline vs. 36% immediately postintervention, p < .01), and we observed a significant reduction in the number of students purchasing “Whoa” foods immediately following the intervention (51% vs. 36%; p < .01). Overall, most of these improvements in food-purchasing behavior persisted without significant decay at seven days postintervention in School B and at 12 days postintervention in School C although students in both of these intervention schools showed trends towards increased caloric content in food choices during the delayed food sales (Table 4).
Food-Purchasing Behavior Across the Program Sequence, From Baseline Through Immediate Postintervention.
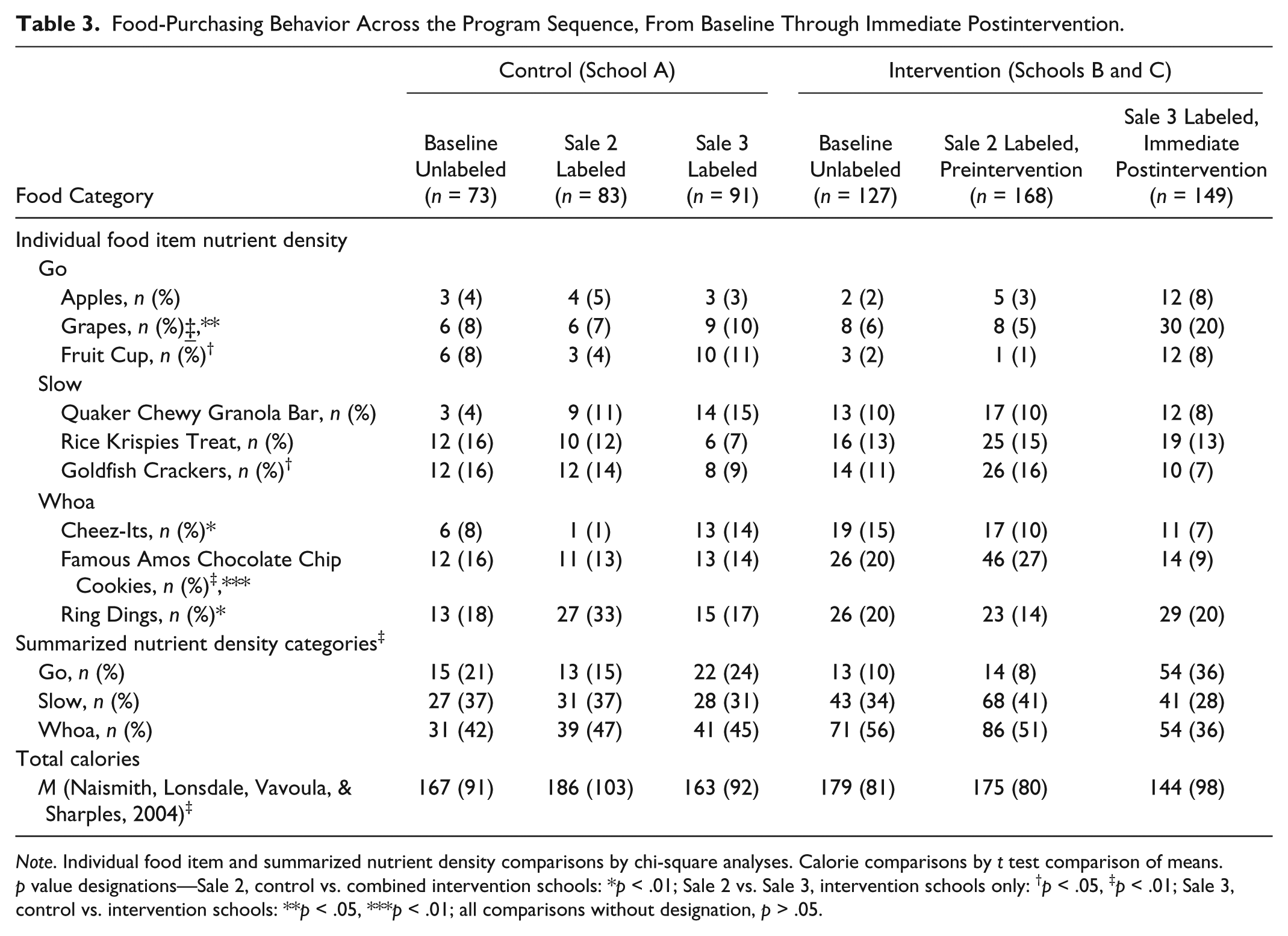
Note. Individual food item and summarized nutrient density comparisons by chi-square analyses. Calorie comparisons by t test comparison of means. p value designations—Sale 2, control vs. combined intervention schools: *p < .01; Sale 2 vs. Sale 3, intervention schools only: †p < .05, ‡p < .01; Sale 3, control vs. intervention schools: **p < .05, ***p < .01; all comparisons without designation, p > .05.
Food-Purchasing Behavior Comparisons of Immediate Postintervention Versus Delayed Postintervention Behaviors.
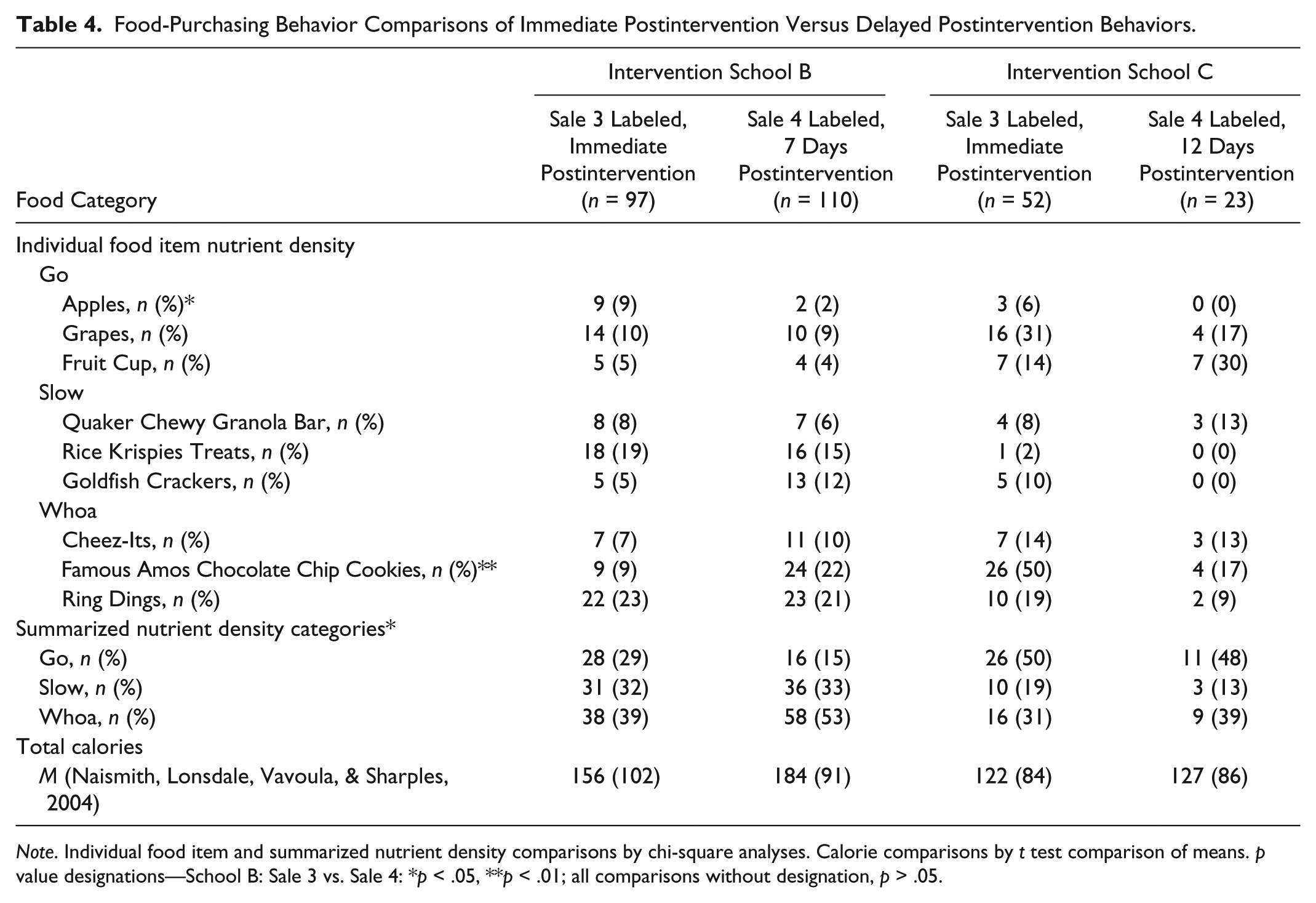
Note. Individual food item and summarized nutrient density comparisons by chi-square analyses. Calorie comparisons by t test comparison of means. p value designations—School B: Sale 3 vs. Sale 4: *p < .05, **p < .01; all comparisons without designation, p > .05.
Discussion
Our findings suggest that (1) calorie labels, by themselves, do not affect food-purchasing behavior of children and (2) a brief 3-hour calorie label intervention may improve food-purchasing behavior both in terms of caloric content (a 20% mean decline in purchased calories) and nutrient value (a significant increase in “Go” foods) of children for up to 12 days following the intervention. While the effect observed is encouraging, it does not infer sustainability but supports our initial hypothesis that a “loading” (3-hour) dose, though sufficient to influence food-purchasing behavior of young children, is insufficient by itself to sustain behavior change. As with many behavioral interventions, it is unreasonable to expect that a single dose of an intervention will continue to affect behavior, especially with regard to food choices of children, who are also influenced by family, environment, and societal factors. Indeed, the goal of our loading dose was to inculcate behavior change in response to the intervention, promote cognitive processes such as self-efficacy, and then catalyze the internalization of the behavior so that they can become habit through a longer term dosing of the intervention such as by integrating HHH modules into school curricula.
The prominent role of media in our curriculum simplifies reproducibility and implementation fidelity given the use of fixed media elements and less reliance on individual teachers. Each cartoon, video game, and song, collectively or individually, is designed to serve as a contemporary, culturally- and age-appropriate mechanism for engaging the youth around nutrition and the use of calorie labels in a fun manner. We suggest that it is these elements driven by our theoretical underpinnings (Table 2) that enhanced student receptivity and motivation to engage in the desired food choice behavior.
Our study has several limitations. We did not track individual children across the food-purchasing sequence and instead performed group-level analyses. Regarding child ages, we did not collect child ages for this study and thus have not explored such analyses. We did not compare menu label literacy of children to food-purchasing behavior. We conducted the study with a convenience sample of three schools and did not perform intraclass correlations or control for baseline differences beyond PI scores. Variable dropout of participants within and between study arms may have introduced bias and further threats to validity, although we did ascertain that, except for School C, dropouts at food sales were mostly due to children not having the 50 cents required to make a purchase at any given time, which was a limitation of our study. Regarding School C, an entire class was barred from participating in follow-up food sales for disciplinary reasons beyond our control and unrelated to the study. The real-world effects of cost and parental influence were not accounted for by our study, which was designed to evaluate efficacy and not effectiveness by standardizing the costs of food items. Finally, the front-loaded nature of the capital expense of developing our multimedia intervention tools requires cost-effective analyses, which was beyond the scope of this pilot study.
Menu labeling with calories provides a viable target for influencing dietary decision making of children. In our study, the average baseline caloric content per snack food item purchased by children was 175 calories and these calories were derived mostly from energy-dense snacks. Consistent with prior reports, we found that calorie labeling had no impact on food selection of children (Dodds et al., 2014); however, supplementation of calorie labeling with HHH led, on average, to a 20% decline in the amount of calories consumed per food item and an increase in the amount of nutrients consumed per food item. Our results demonstrate the feasibility of improving point-of-purchase behaviors of young children and highlight the need to test similar interventions targeting consumer socialization of young children around menu labeling to improve their food-purchasing behaviors. Further studies are needed to confirm our findings and assess the long-term benefit of HHH in a dose–response design.
Footnotes
Acknowledgements
The authors would like to acknowledge our health educators, Adrian Harris, Tiffany Newton, and Saima Huq, as well as Ian Ellis Black and Doug E. Fresh, and Arthur Lloyd, the creative team behind the Hip Hop HEALS musical cartoons.
Authors’ Note
This study was approved by the Columbia University Medical Center and New York City Department of Education Institutional Review Board.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Hip Hop HEALS (Healthy Eating And Living in Schools) program is funded by the New York City Council Office of Inez Dickens. William Gerin was paid as a consultant for the grant that funded this project, out of Columbia University.