
Abstract
Background. A substantial proportion of adolescents, particularly girls and minority youth, fail to meet daily physical activity (PA) recommendations. Social support contributes to adolescent PA, but studies examining this relationship have yielded inconsistent results and rarely focus on diverse, urban populations. Aims. This study examines the correlates of support for PA from family and friends and its relationship with PA outcomes among young adolescents. Methods. Data were collected in a cross-sectional survey of 4,773 middle school students. Social support from family and friends was separately measured using the Sallis Support for Exercise Scales. Hierarchical logistic regression models were used to assess correlates of high support and the relationship between support and self-reported PA. Results. Approximately one quarter of students reported being active for at least an hour each day. 31.7% of students reported high family support for PA, while 17.8% reported high friend support. Differences in perceptions of support by gender, ethnicity, and language emerged. Support from family and friends were both consistently strong predictors of all three PA outcomes measured. Discussion. Findings highlight the need for multilevel interventions targeting both psychosocial influences on behavior in addition to addressing the physical environment. Given low rates of friend support for PA, there appears to be an opportunity to increase PA levels through promotion of supportive behaviors among peers. Conclusion. Support for PA from family and friends is a key contributor to increased PA among adolescents. Further research is needed to further understand the mechanisms by which these factors influence PA.
Regular physical activity (PA) supports healthy development (Strong et al., 2005; U.S. Department of Health and Human Services [DHHS], 1996), but a substantial proportion of youth fail to meet the recommended hour of daily PA (Carlson, Densmore, Fulton, Yore, & Kohl, 2009; Centers for Disease Control and Prevention [CDC] & National Center for Health Statistics [NCHS], 2013; UCLA Center for Health Policy Research, 2013). In California, 84.6% of early adolescents do not engage in 60 minutes of daily PA (UCLA Center for Health Policy Research, 2013). Nationally, only 20.4% of 12- to 15-year-olds report being active outside school (CDC & NCHS, 2013). Activity levels drop as children grow older (Aarts, Paulussen, & Schaalma, 1997), which contributes to overweight and obesity and increases risk for chronic disease and comorbidities over the life course (Trudeau, Laurencelle, & Shephard, 2004; U.S. DHHS, 1996).
While PA declines overall during adolescence, vulnerable groups exhibit disproportionately lower rates of PA. For example, middle school girls are usually less active than boys (Prochaska, Rodgers, & Sallis, 2002). Children from lower socioeconomic status families also tend to be less active than higher income peers (Sallis et al., 1992). Furthermore, minority and low-income youth generally have fewer opportunities to engage in PA due to limited access to safe spaces for out-of-school recreation (Gordon-Larsen, 2006; Richmond, 2006; Whitt-Glover et al., 2009). A better understanding of correlates of PA can help promote PA among these groups.
Theories of health behavior suggest that both social and environmental factors play a role in shaping PA practices. The interpersonal domain, including family and peer influence on development and behaviors during adolescence, appears to be particularly important. Social cognitive theory (SCT) explains how relationships affect behavior through the reciprocal influence between cognitive, behavioral, and environmental factors (Bandura, 1977). According to SCT, social support processes are a major mechanism through which these factors influence youth PA behaviors (Welk, Wood, & Morss, 2003).
Social support for PA, particularly parent and peer support, has been identified as a determinant of PA (Duncan, Duncan, & Strycker, 2005; Prochaska et al., 2002; Sallis, Prochaska, & Taylor, 2000). Parents and other family members may serve as PA role models and provide emotional and logistical support, such as encouragement, praise, or transportation (Anderssen & Wold, 1992; Duncan et al., 2005; Prochaska et al., 2002). Peers become more influential in adolescence (Prochaska et al., 2002), and support for PA from peers is a consistent predictor of PA across gender and age groups (Beets, Vogel, Forlaw, Pitetti, & Cardinal, 2006; Duncan et al., 2005; Frenn et al., 2005; Prochaska et al., 2002; Robbins, Stommel, & Hamel, 2008; Voorhees et al., 2005). Peers may provide companionship during PA and influence behavior choices through social reinforcement (Voorhees et al., 2005).
Despite theoretical backing and extensive research examining the relationship between social support for PA and participation in PA, inconsistencies have emerged. One study found no association between monitored PA and support for PA from parents or friends among middle schoolers (Prochaska et al., 2002). Some studies found boys report more support (Trost et al., 2003; Welk et al., 2003), while others found less (Higgins, Gaul, Gibbons, & Van Gyn, 2003; Wu, Pender, & Noureddine, 2003) or no gender difference (Garcia et al., 1995). Similarly, studies inconsistently report on the association between perceptions of support for PA and weight status among youth (Beets et al., 2006; De Bourdeaudhuiji et al., 2005; Ward et al., 2006; Zabinski, Saelens, Stein, Hayden-Wade, & Wilfley, 2003). Many of these inconsistencies are due to differences in measures of PA, including self-reported and monitored measures, and differences in measures of social support for PA across studies. In addition, studies including a wide age range of children and adolescents may obscure potential differences in the influence of social support for PA across different developmental stages.
Interpreting research findings on the association between social support and PA must take into account the social context. Studies examining social support and PA rarely focus on large, urban, multiethnic populations, which is important given inconsistencies in results of studies examining racial/ethnic differences in social support (Felton et al., 2002; Grieser et al., 2008). Few studies have explored the role of psychosocial factors in influencing PA among Latino youth (Belcher et al., 2010; Byrd-Williams, Kelly, Davis, Spruijt-Metz, & Goran, 2007; Foran, Cermak, & Spruijt-Metz, 2013), which is of public health concern given the high rates of overweight and obesity among Latinos (Ogden, Carroll, Fryar, & Flegal, 2015). This study aims to fill these gaps by examining correlates of family and friend social support for PA and the relationship with PA among a large sample of middle school youth from a diverse, urban school district with a large proportion of Latino students.
Methods
Participants and Survey Administration
Data were collected in a cross-sectional survey of 4,773 seventh-grade students recruited from 16 middle schools in a large district in Los Angeles, California. The district has a total of 190 schools that include Grades 6 to 8. Schools were identified by their willingness to participate in a physical education intervention study and level of enrollment in the National School Lunch and Breakfast Programs. Across all schools, an average of 73.8% of students participated in these programs, which is similar to the district-wide participation rate of 75.6%. Seventh-grade students at all study schools were offered the opportunity to participate in the survey during their physical education class prior to any intervention activities during the fall of 2014. Of the 6,201 seventh-grade students at all 16 schools, 5,529 students were enrolled in participating teachers’ classes (89.2%), and 4,773 students completed the survey (77.0%).
This study was approved by the University Institutional Review Board and the school district. Parents were informed through an information sheet distributed to students by the research team. Parents were able to opt their children out of the survey, and students provided verbal assent to participate. Prior to data collection, members of the research team explained the study to students and informed them that participation was voluntary and had no effect on academic grades. The research team remained in the room to answer questions during survey administration.
Instrument and Measures
The survey instrument included items developed by the research team and items adapted and adopted from existing youth surveys (CDC, n.d.; Sallis, 2002). The instrument was pretested with a group of sixth-grade students, followed by revisions to ensure appropriate reading level. The revised survey was again pretested with a group of seventh-grade students.
Social Support
Perceived family and friend support for PA was measured using the family and friend participation subscales of the Sallis Support for Exercise Scales (Sallis, Grossman, Pinski, Patterson, & Nader, 1987). Students responded to 10 items related to support provided by family or members of the household and 10 items concerning support from friends or classmates. Family support items asked about encouragement (e.g., “My family or a member of my household gave me helpful reminders to exercise”), involvement (e.g., “My family or a member of my household exercised with me”), and facilitation (e.g., “My family or a member of my household changed their schedule so we could exercise together”). The friend support scale had similar items related to friends and classmates. All items referred to the previous 3 months and response options were never, rarely, a few times, often, or very often.” These responses were scored 0 to 4, respectively, and summed to create two scale scores (0-40), one for family and one for friends. Similar to another study using these scales (Leslie et al., 1999), family and friend support scales were dichotomized into high support (21-40) for students who tended to report “often” or “very often” and low support (0-20) for students who tended to report “never,” “rarely,” or “a few times.” This dichotomization was performed due to nonnormality of the responses and for better interpretability of the results. This scale has demonstrated evidence of criterion-related and construct validity (Sallis et al., 1987), and previous studies have demonstrated reliability of the scale (Prochaska et al., 2002; Sallis et al., 1987). Internal consistency for these continuous scales in this study was α = .90 for family and α = .91 for friend support, indicating high reliability.
Physical Activity
PA was assessed through three items. Students reported the number of days during the previous week they (1) were physically active for 60 minutes or more per day and (2) did exercises to strengthen or tone muscles. Students also reported the number of sports teams they played on in the past 12 months. These three outcomes were dichotomized to reflect PA recommendations for middle school-age youth (60 minutes or more of PA every day and toning muscles 3 days a week; U.S. DHHS, 2008) and to reflect higher PA (playing on at least one sports team).
Demographics
Gender, age, and ethnicity (Latino or non-Latino) were reported by the students. Students also reported the main language they spoke at home and with friends (English, Spanish, English and Spanish, or other).
Attitudes, Perceptions, and Beliefs
PA attitudes were assessed through four items regarding respondents’ feelings toward PA (e.g., “I would rather watch TV than play sports or be active”). Responses were summed and dichotomized to reflect negative and positive attitudes toward PA (National Institutes of Health, 2001). Perceived access to equipment or space for PA was assessed with two items (e.g., “There are playgrounds, parks, or gyms close to my home or that I can get to easily”). Response options were strongly disagree, somewhat disagree, do not disagree or agree, somewhat agree, and strongly agree. Responses were scored 0 to 4, respectively, and dichotomized to low (0-4) and high (5-8) access. Perceived neighborhood safety was similarly measured with two items (e.g., “It is safe to walk or jog alone in my neighborhood during the day”). Response options were the same as the perceived access questions, and first item was scored the same way. The second item was reverse coded to reflect positive feelings of safety. These two items were summed together and dichotomized into unsafe (0-4) and safe (5-8) neighborhood conditions. Students were also asked about intentions to change weight: “Which of the following are you trying to do about your weight?” Response options were “lose weight,” “gain weight,” “stay the same weight,” and “I am not trying to do anything about my weight.” This item was dichotomized into students who were attempting to lose weight and those who were not.
Anthropometrics
Height and weight data were obtained from FITNESSGRAM (Meredith, Welk, & Cooper Institute, 2010) testing conducted by physical education teachers approximately 3 months after survey data collection. Students’ height and weight were used to calculate body mass index (BMI), and gender- and age-specific percentiles were calculated using the 2000 CDC Growth Charts for ages 2 to <20 years (Kuczmarski et al., 2000). Using CDC guidelines, underweight was defined as a percentile <5, healthy weight as a percentile <85, overweight as a percentile ≥85 and <95, and obese was defined as >95th percentile (Kuczmarski et al., 2000).
Statistical Analyses
All analyses were completed using Stata Version 14.1, and all variables were tabulated using the sample with FITNESSGRAM data. Differences in level of family support and friend support by demographic characteristics were tested using hierarchical logistic regression models to account for clustering within school, as were differences in demographic characteristics between students with and without FITNESSGRAM data. Internal consistency in the continuous social support scales was measured using Cronbach’s alpha.
Hierarchical logistic regression models were used to assess the relationships between the outcomes high family support and high friend support and the independent variables gender, ethnicity, language spoken, weight status, intent to lose weight, access to PA equipment and space, neighborhood safety, and PA attitudes. First, we fit an intercept-only model with a random effect for school to determine if a hierarchical model was appropriate. A second model included the covariates. Interactions between intent to lose weight and weight status and between gender and weight status were tested individually using likelihood ratio tests. The final model included all covariates and significant interactions.
Similarly, hierarchical logistic regression models were used to assess the relationship between the three dichotomized PA outcomes and social support, controlling for PA attitudes, gender, ethnicity, language spoken at home, weight status, intent to lose weight, access to equipment and exercise space, and neighborhood safety. An intercept-only model was used to determine if the hierarchical model was appropriate. A second model included only family and friend social support, and a third model added all other covariates. Interactions between all covariates and the two social support variables were tested individually using likelihood ratio tests. The final model included all covariates and significant interactions.
The two social support scales were only scored when all 10 items had been answered, which resulted in a reduced sample size for the complete case analysis. As a sensitivity analysis, we used multiple imputation using chained equations to impute missing individual scale–level items and repeated the hierarchical logistic regression analyses, a technique recommended for use in large survey data with multiple scales (Plumpton, Morris, Hughes, & White, 2016). We decided to use 25 imputed data sets based on previous research, power considerations, and missingness of data (Enders, 2010; Graham, Olchowski, & Gilreath, 2007; Plumpton et al., 2016).
Results
Of the 4,773 students surveyed, 3,859 (80.9%) had FITNESSGRAM data. Descriptive statistics of this restricted sample are presented in Table 1. Comparing students with FITNESSGRAM data with those without, significant differences were detected in high friend support, high access to equipment and exercise space, gender, and participating in at least one sports team (not shown).
Characteristics of the Sample in Total and by Family and Friend Social Support for Physical Activity.
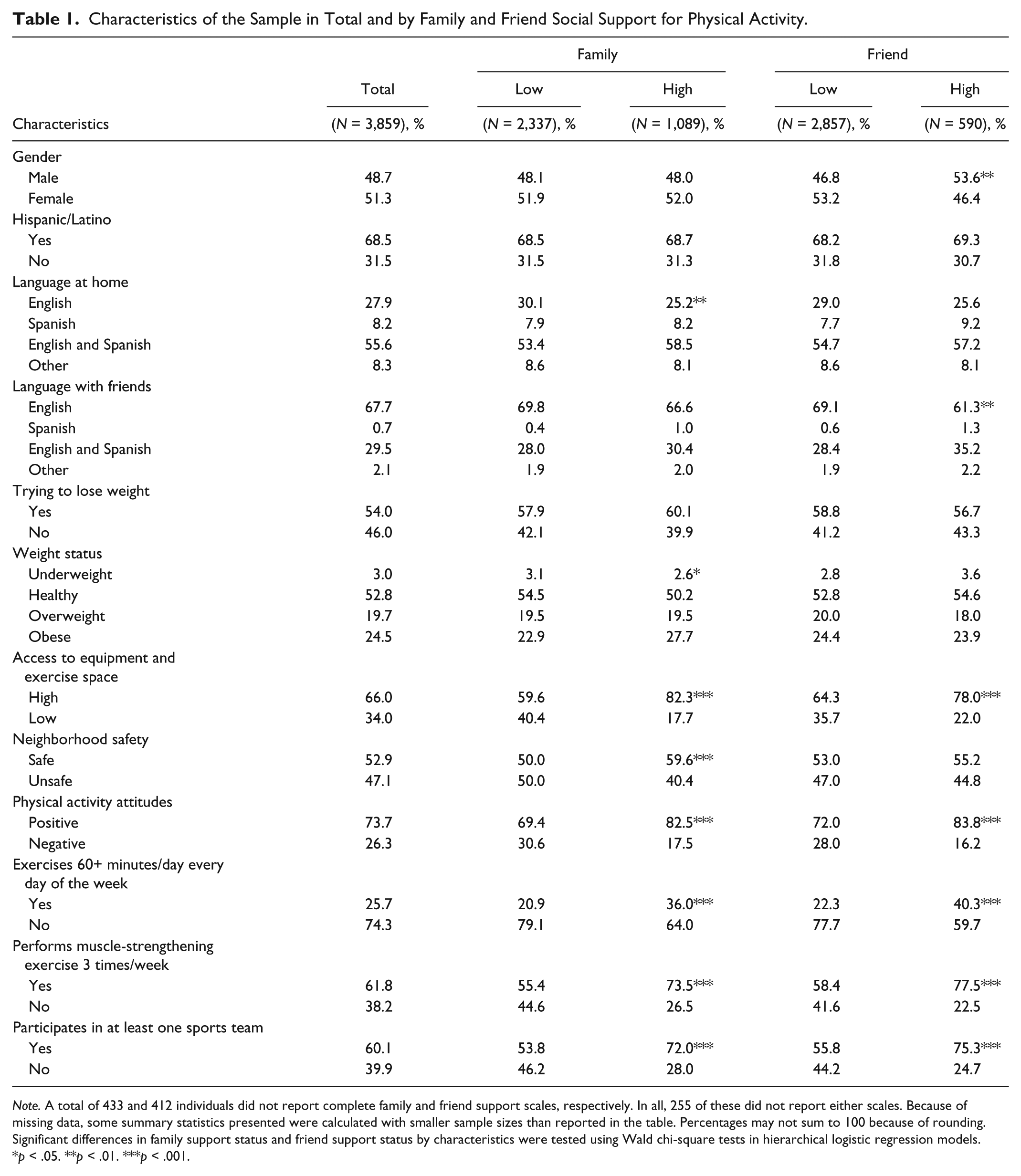
Note. A total of 433 and 412 individuals did not report complete family and friend support scales, respectively. In all, 255 of these did not report either scales. Because of missing data, some summary statistics presented were calculated with smaller sample sizes than reported in the table. Percentages may not sum to 100 because of rounding. Significant differences in family support status and friend support status by characteristics were tested using Wald chi-square tests in hierarchical logistic regression models.
p < .05. **p < .01. ***p < .001.
Table 1 also presents participant characteristics and PA outcomes by level and type of social support. Of those who answered all 10 items in each scale, 31.7% were categorized as having high family support, and 17.8% were categorized as having high friend support. A greater proportion of males reported high friend support. Differences in family support were observed by language spoken at home. Perceived neighborhood safety was associated with family support but not friend support, and support of either type was associated with access to equipment or space for PA, positive attitudes toward PA, and all three PA outcomes.
Table 2 presents the results of hierarchical logistic regression models predicting high family and friend support for PA. All else equal, girls had higher odds of perceiving high family support than boys, while there were no gender differences in perceived support from friends. Latino students were less likely to report high family support as compared with non-Latinos, but there were no differences in friend support by ethnicity. Speaking Spanish or both English and Spanish in the home was associated with higher odds of high family support compared with only English speakers. Similarly, speaking only Spanish or both English and Spanish with friends was associated with higher odds of high friend support as compared with those who spoke only English with friends.
Summary of Hierarchical Logistic Regressions Predicting High Social Support.
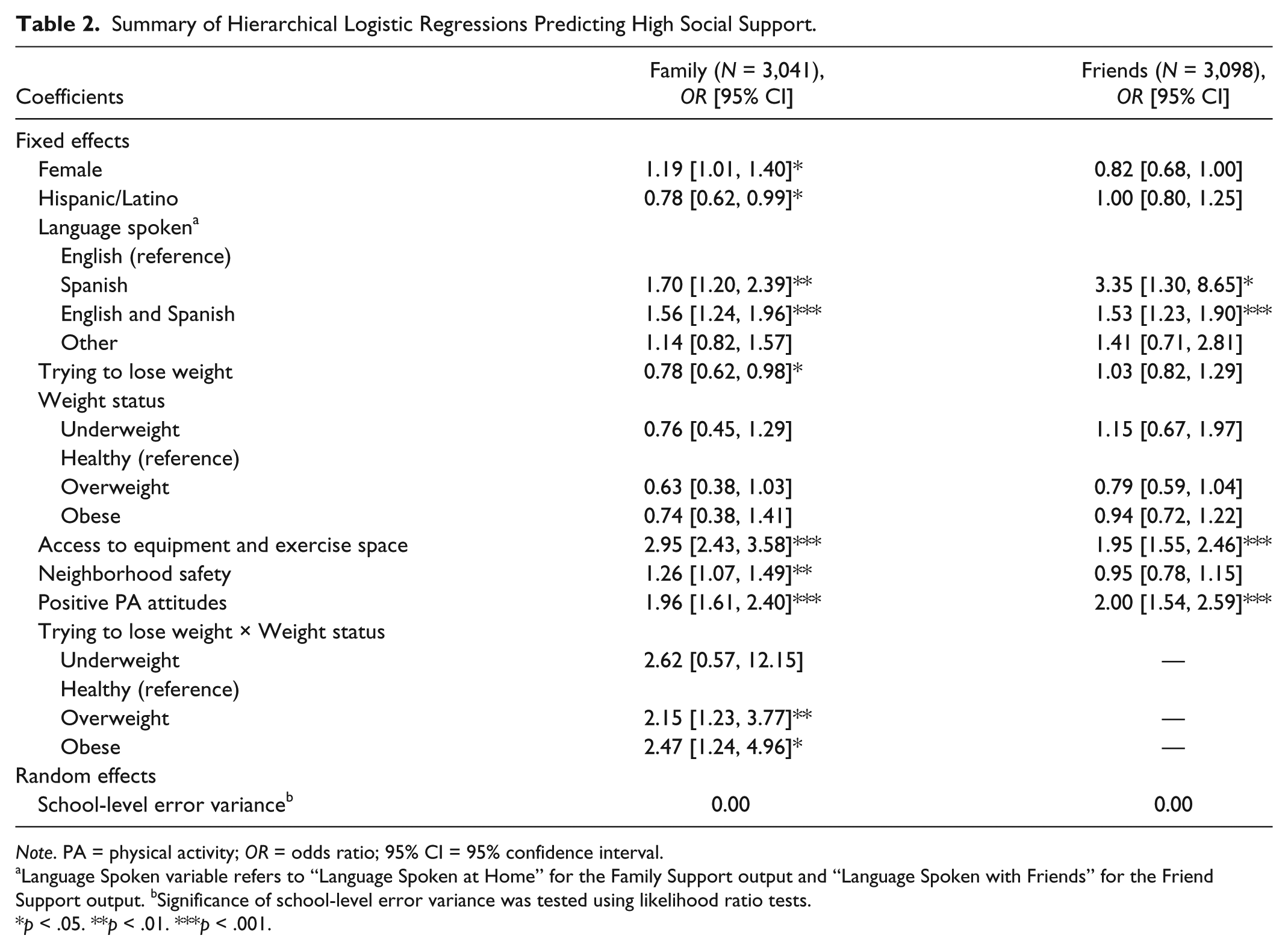
Note. PA = physical activity; OR = odds ratio; 95% CI = 95% confidence interval.
Language Spoken variable refers to “Language Spoken at Home” for the Family Support output and “Language Spoken with Friends” for the Friend Support output.
Significance of school-level error variance was tested using likelihood ratio tests.
p < .05. **p < .01. ***p < .001.
Healthy weight students who reported trying to lose weight had lower odds of perceiving high family support for PA. Among students who were not trying to lose weight, family support and friend support for underweight, overweight, and obese students were not different from that of healthy weight students. The interaction between weight status and intention to lose weight shows that overweight and obese students who reported trying to lose weight had higher odds of perceiving high family support than students of the same weight status who were not trying to lose weight. In addition, students who reported high access to PA equipment or space and those with positive attitudes toward PA were more likely to perceive high friend and family support. All else equal, neighborhood safety was associated with higher odds of family support but not with friend support. The school-level random effect variances were small, indicating that there was little variance in family or friend support for PA that was accounted for by differences at the school level. Analyses conducted using multiple imputation yielded the same findings (see Supplemental Material, available with the online article).
Table 3 presents the results of regression models predicting the three PA outcomes. Significant school-level error variance indicated that there was significant variance in the PA outcomes attributable to variance at the school level. High family support was associated with higher odds of all three outcomes. High friend support was associated with higher odds of performing muscle-strengthening exercises and participating on at least one sports team. Additionally, high friend support was significantly associated with higher odds of an hour of daily PA for students with low access. Girls were less likely to engage in all three PA outcomes than boys, and no differences were observed by ethnicity. Obese students and students who were trying to lose weight had lower odds of participating in an hour of daily PA compared with healthy weight students and those who were not trying to lose weight, respectively.
Summary of Hierarchical Logistic Regressions Predicting Three Outcomes.
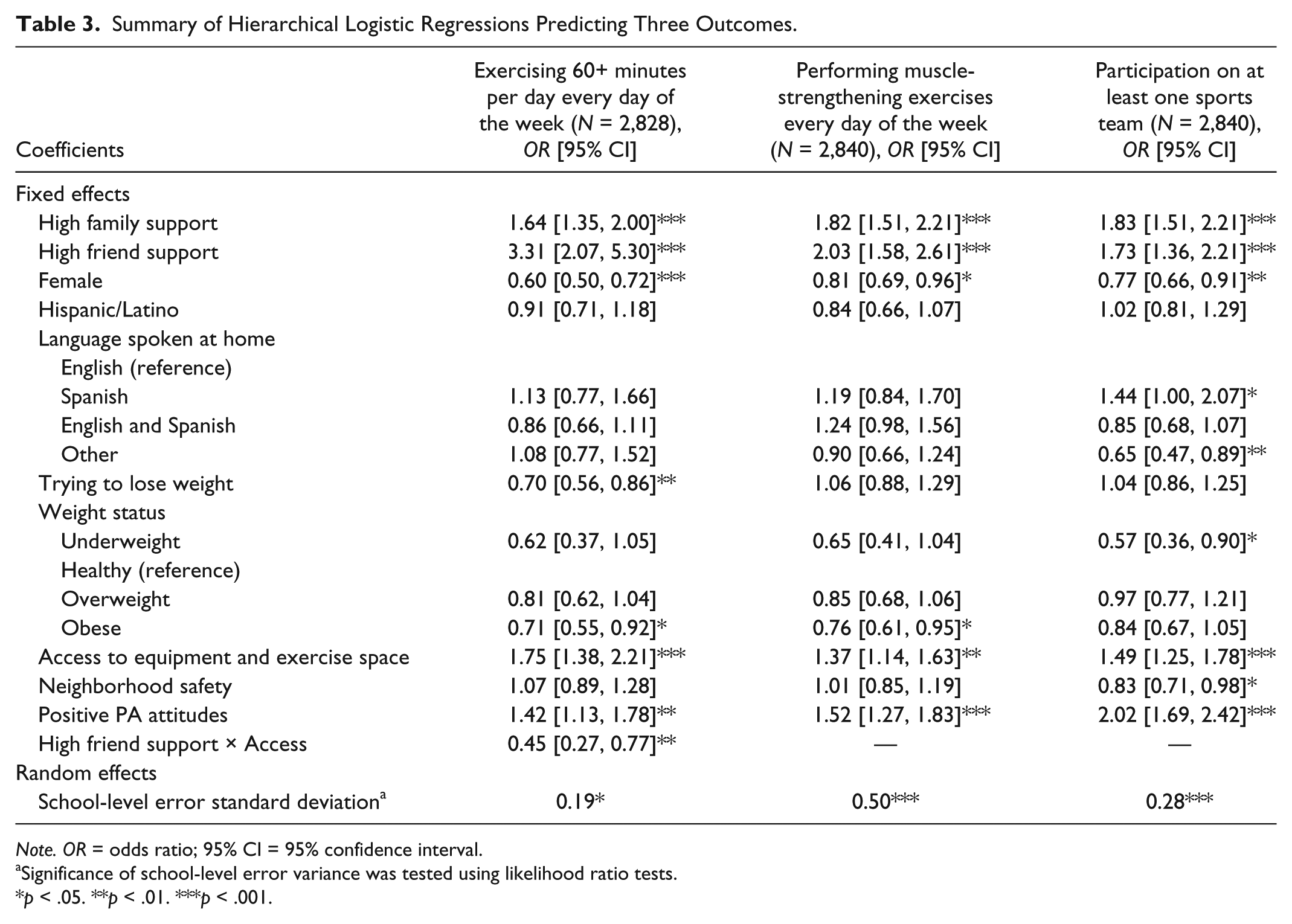
Note. OR = odds ratio; 95% CI = 95% confidence interval.
Significance of school-level error variance was tested using likelihood ratio tests.
p < .05. **p < .01. ***p < .001.
Access to equipment and space for PA was associated with higher odds of meeting the daily PA recommendation for students with low friend support, but the interaction between friend support and access yielded a negative coefficient. Obese students were also less likely to meet the recommendation for muscle-strengthening exercises compared with students with a healthy weight status, while students with more access to equipment and space were more likely to meet it. Speaking Spanish at home was significantly associated with higher odds of participating in sports teams compared with English speakers, as was having access to equipment and space. Underweight students had lower odds of sports team participation compared with healthy weight students, as did students who felt safe being active in their neighborhood. Positive attitudes toward PA were associated with higher odds of all three types of PA. With the exception of language spoken at home, there were no differences in the magnitude or significance of the regression coefficients when compared with the imputed models for all three PA outcomes (see Supplemental Material, available with the online article).
Discussion
The decline in PA during adolescence is a contributor to high rates of overweight and obesity among youth. Social support plays an important role in influencing adolescent PA, but studies examining this relationship have yielded mixed results (De Bourdeaudhuiji et al., 2005; Garcia et al., 1995; Higgins et al., 2003; Prochaska et al., 2002; Trost et al., 2003; Ward et al., 2006; Welk et al., 2003; Wu et al., 2003; Zabinski et al., 2003). This study furthers our understanding of the relationship between social support and PA among diverse, urban middle school–aged youth by examining the correlates of support from family and friends as well as its association with PA outcomes.
The findings of this study underscore the need for efforts to promote regular PA as an attainable and positive lifestyle choice for youth, as only a quarter of the sample reported meeting daily PA recommendations and almost half of the sample was either overweight or obese. Prior research has also identified similarly low levels of PA among this age group (CDC & NCHS, 2013; UCLA Center for Health Policy Research, 2013). More than half of students reported they were trying to lose weight, yet a third expressed negative attitudes toward PA. Furthermore, large proportions of students reported low neighborhood safety and low access to equipment or space for PA, both of which were associated with low perceived support for PA. To encourage PA across all youth, these findings highlight the need for interventions targeting psychosocial factors like social support and environmental determinants of PA, such as access and safety.
Overall, social support for PA from family and friends were both consistently strong predictors of all three PA outcomes. High friend and family support were positively associated with meeting daily and weekly recommendations for PA, and with the likelihood of participating on a sports team. This finding confirms what has been observed in previous studies conducted in higher income and less diverse settings (Duncan et al., 2005; Prochaska et al., 2002) and demonstrates that social support is an equally important component of PA promotion among urban, low-income, multiethnic middle school students. All else equal, students reporting access to equipment or PA spaces were more likely to be active, a finding which aligns with previous research (Garcia et al., 1995). However, social support for PA from friends appeared to be more predictive of meeting daily PA recommendations for students with low access as compared with those with high access. Thus, friend support seems to be especially salient for vulnerable groups of youth with limited resources for PA. To the authors’ knowledge, the interaction between access and support for PA and its association with PA behavior has not been examined in this way, and this finding may provide new understanding of the influence of social support for PA. Efforts to increase social support can be more immediate, low-cost, and sustainable than those addressing access to PA equipment or space. Given the low proportion of students reporting high support for PA from friends (17.8%), there is an opportunity to increase PA levels through interventions promoting group activity and supportive behaviors among peers in this age group.
Similar to previous research, girls were significantly less likely to be active than boys across all three PA outcomes (Prochaska et al., 2002), despite being more likely to experience high family support for PA (Higgins et al., 2003; Wu et al., 2003). It is possible that for some adolescent girls, family support systems are not sufficient to counter self-perceptions of inability or low self-efficacy that result from internalization of gender norms (Chalabaev, Sarrazin, Fontayne, Boiché, & Clément-Guillotin, 2013). Indeed, social support might inhibit PA when prevalent social norms proscribe PA among females. There was no significant difference in PA between students who were Latino and those who were not, when controlling for other factors. Whereas students identifying as Latino perceived less social support for PA from family compared with those who did not identify as Latino, speaking Spanish (either alone or in combination with English) at home was associated with significantly higher odds of perceiving high family support as compared with students who spoke only English. Similarly, speaking Spanish or both English and Spanish with friends was associated with higher perceived friend support. A study of social support among Latino adults found stronger familial support among foreign-born Latinos than their U.S.-born counterparts, suggesting that “retention of culture” may influence perceptions of and actual social support (Almeida, Molnar, Kawachi, & Subramanian, 2009). Our findings suggest that a similar pattern may exist among adolescents and should be studied further.
Interestingly, students who were trying to lose weight had lower odds of being active for at least an hour each day than those who were not trying to lose weight. Obese students also had lower odds of meeting daily PA recommendations. However, overweight and obese students trying to lose weight had higher odds of perceiving high family support for PA compared with overweight and obese students not trying to lose weight. While overweight status has previously been associated with lower perceived support for PA among adolescents (De Bourdeaudhuiji et al., 2005), in our sample, overweight and obese students who expressed interest in losing weight report feeling supported in efforts to be physically active. This finding is promising since parental involvement is key to weight control among children and adolescents (Epstein, Myers, Raynor, & Saelens, 1998). However, it is unclear if and how family support translates into increased activity, and further research should consider the mechanisms by which social support influences behavior.
Limitations and Strengths
Limitations of the study include the use of cross-sectional data in one geographic location, which prevents any causal claims and limits the generalizability of findings. Generalizability is also limited by the fact that study schools had agreed to take part in a larger intervention study and thus may have some unmeasured differences from other schools. Likewise, grade-level sociodemographic data were not available, so it is unclear if there were any differences between respondents and nonrespondents. With the exception of height and weight, data were self-reported by students, and thus susceptible to social desirability and recall bias. In particular, the validity of self-reported PA measures has been questioned, as objective measures of PA tend to find less activity than self-reported measures (Sallis et al., 2000). The PA measures used here were based on prior research and available resources for a large-scale study. Because height and weight data were collected by teachers, there may be inconsistencies in equipment and measurement methods. Significant differences in covariates were detected between students with and without these data, thus generalizability is further limited. Because of time limitations, the survey instrument did not separately examine social support from individuals (e.g., mother, father, siblings); however, previous research has found that youth respond more accurately with shorter and simpler instruments (Robbins et al., 2008). The Sallis Scale has been evaluated for reliability and validity (Sallis et al., 1987) and demonstrated high internal reliability in this study. Finally, this study was conducted in a large sample of students in an urban setting and included a large proportion of Latino students, an understudied group with regard to psychosocial correlates of PA.
Implications for Practice
Our findings indicate that PA promotion remains an important area of work for reducing the prevalence of overweight and obesity in youth. A large proportion of the sample reported wanting to lose weight, however few students met recommendations for daily PA. In addition, social support was consistently predictive of increased activity, suggesting that youth PA interventions should incorporate group activity, possibly collaborating with antibullying efforts to promote peer supportive behaviors, and involve family or parent participation. Different perceptions of support by gender and ethnicity not only suggest that more should be done to make PA normative for all youth but also suggest that building on existing cultural capital could be a promising way to promote PA among Latino students. Findings regarding access to PA equipment and space and neighborhood safety indicate that efforts to increase PA for youth must also consider environmental factors.
Conclusion
Social support for PA from family and friends is a key contributor to increased PA among adolescents. Differences in perceptions of social support by gender, ethnicity, and language emerged and more research is needed to further understand the mechanisms by which these factors influence PA. Additionally, perceived access and safety were significantly associated with both perceptions of support and actual PA outcomes, suggesting that PA interventions should target psychosocial influences on behavior in addition to addressing the physical environment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute of Nursing Research (5R01NR012676) and supported by grants from the National Heart, Lung and Blood Institute at the National Institutes of Health (P50 HL105188 and R25 HL108854).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.