
Abstract
This exploratory study examines measures of one drop-in center’s efforts to improve health outcomes of gay, lesbian, bisexual, and transgender (GLBT) youth by facilitating out-group secondary social ties. Hatch Youth, located in Houston, Texas, aims to increase self-esteem and decrease negative health outcomes by encouraging GLBT youth to be part of Houston’s greater GLBT community. Survey data (N = 614) collected between October 2003 and April 2013 were entered into logistic regression models. Attending Hatch Youth for 6 or more months was associated with having a social group outside of school (adjusted odds ratio [aOR] = 2.07; 95% confidence interval [CI] = [1.33, 3.20]), being out to that social group (aOR = 2.34; 95% CI = [1.35, 4.03]), and interacting with the GLBT community outside of Hatch Youth (aOR = 2.33; 95% CI = [1.50, 3.54]), when referenced against youth attending less than 1 month. Having a good family relationship in the last 90 days (aOR = 2.48; 95% CI = [1.67, 3.70]) and having a social group outside of school (aOR = 2.57; 95% CI = [1.67, 3.97]) were associated with higher self-esteem. Higher self-esteem was associated with practicing safe sex (aOR = 1.86; 95% CI = [1.25, 2.75]) and not using street drugs (aOR = 0.45; 95% CI = [0.24, 0.83]). Interacting with the GLBT community outside of Hatch Youth was associated with practicing safe sex (aOR = 1.64; 95% CI = [1.12, 2.42]). Drop-in centers can strengthen secondary social ties among youth. Because questions remain about how drop-in centers can assist youth aging out of their programs to find other supportive secondary social ties, additional studies examining similar drop-in centers are needed.
Gay, lesbian, bisexual, and transgender (GLBT) youth frequently live in environments less supportive of their sexual orientation or gender identity and expression than their heterosexual, cisgender peers. The minority stress theory posits that youth living in less supportive environments feel compelled to hide their orientation and identity, which leads to greater negative effects on their physical and mental health (Frost, Lehavot, & Meyer, 2015; Gordon & Meyer, 2007; Meyer, 1995, 2003). Researchers have found that GLBT youth living and attending school in environments less tolerant of homosexuality or gender variation experience greater psychological distress, depressive symptoms, suicidal ideation, avoidant coping, substance use (alcohol, tobacco, and other drugs), and riskier sexual behavior (Bradford, Reisner, Honnold, & Xavier, 2013; Budge, Adelson, & Howard, 2013; Doty, Willoughby, Lindahl, & Malik, 2010; Hatzenbuehler, Pachankis, & Wolff, 2012; Nadal, Davidoff, Davis, & Wong, 2014; Robinson & Espelage, 2013; Russell, Ryan, Toomey, Diaz, & Sanchez, 2011; Ryan, Huebner, Diaz, & Sanchez, 2009; Testa et al., 2012; Toomey, Ryan, Diaz, Card, & Russell, 2010). In contrast, GLBT youth who live and attend school in more tolerant environments experience less psychological distress and substance use, and they are more likely to report higher perceived social support, self-esteem, and better overall health in general (Hatzenbuehler, 2011; Hatzenbuehler, Birkett, Van Wagenen, & Meyer, 2014; Ryan, 2010; Simons, Schrager, Clark, Belzer, & Olson, 2013).
Social ties theory helps understand how living in less supportive environments may contribute to negative health outcomes. Social ties theory posits that the health of GLBT youth is affected by the strength of primary (family members and close friends) and secondary (members of organizations, classmates, and coworkers) social ties. When facing intolerance from their primary social ties, GLBT youth may experience a loss of social support. This lack of social support can create a loss of perceived control and self-efficacy (Thoits, 2011). The result is lowered self-esteem and an increase in stress levels and undesirable health outcomes. Evidence suggests that GLBT youth who also identify as a racial or ethnic minority, transgender, or as non-gay identified (e.g., bisexual, queer, another sexual orientation counter to the hegemonic gay–straight dichotomy) may experience an even greater loss of social support from primary and secondary social ties less familiar and uncomfortable with the non-hegemonic identities. These intersecting identities can result in additional negative health outcomes (Mustanski, Garofalo, & Emerson, 2010; Shilo & Savaya, 2011). Theoretically, these undesirable outcomes could be moderated by supportive secondary ties, especially when these ties include other individuals experiencing and coping with similar issues (Thoits, 2011).
Community-based organizations have attempted to develop and strengthen secondary social ties by establishing drop-in centers for GLBT youth. One such program, Hatch Youth, is located in Houston, Texas. To inform the practice of community-based organizations developing these drop-in centers, the purpose of these exploratory analyses was to examine measures of Hatch Youth’s efforts to improve health outcomes and reduce risk behaviors of GLBT youth by facilitating out-group secondary social ties.
Method
Intervention
Hatch Youth is a drop-in center designed to improve mental health and reduce behavioral risk outcomes by increasing social support among GLBT youth. Research suggests this approach should be effective (Gavin, Catalano, David-Ferdon, Gloppen, & Markham, 2010; Hatzenbuehler, 2009; Hatzenbuehler et al., 2014). Hatch Youth, formed in 1987 as the Houston Area Teen Coalition of Homosexuals (H.A.T.C.H.), hosts weekly social and peer support meetings for GLBT youth. Each Hatch Youth meeting lasts 3 hours and is divided into three sections. During the initial social hour, new visitors are welcomed and oriented to the center and its services. Participants are encouraged to socialize, talk to facilitators, use computer stations, play games, and enjoy refreshments. The second section is a consciousness-raising hour. Facilitators or invited guests lead a presentation or activity about a relevant topic, such as sexuality, substance use, HIV/sexually transmitted infection, healthy relationships, general health/wellness, GLBT current issues, and history of GLBT culture and oppression. These presentations follow a 3-month rotating schedule to maximize participants’ exposure to key topics. The final hour consists of a youth-led peer support group where participants talk about the events and issues in their lives and/or work together to process a specific topic. Adult facilitators (volunteers from the community who have completed a 1-day training developed by paid Hatch Youth staff) monitor the group and contribute only when needed to halt or prevent disrespectful or abusive behavior. Facilitators also watch for signs of—and screen for—symptoms of abuse, depression, substance use, and self-harm/suicide. In addition to the weekly meetings, Hatch Youth exposes youth to Houston’s adult GLBT community. For example, representatives from various community groups may talk to the youth about their organizations or take the youth on field trips to age-appropriate GLBT community events.
In 2003, the organization came under the auspices of the Montrose Center, the largest GLBT mental health service provider in Houston, Texas. Aside from fortifying the program with formal policies and procedures, very few changes were made to the program’s original model. In 2012, the program’s title was changed to Hatch Youth, removing the acronym to reflect inclusion of all sexual minorities, but keeping the name “Hatch” due to its unique and well-known local brand identity. The meetings are open to all GLBT identifying youth. Hatch Youth is promoted on its website, on the Montrose Center website, and in brochures distributed to local schools and other youth-serving organizations. As part of Hatch Youth, the Montrose Center also sponsors a local radio show cohosted by Hatch Youth participants. The radio show helps promote the program and allows youth to interact with members of Houston’s larger GLBT community.
Study Design
This exploratory, secondary data analysis examined the duration of attendance, demographic characteristics, and indicators of primary and secondary social ties using survey data from Hatch Youth intervention participants. This information was collected from October 2003 to April 2013. Participants who attended Hatch Youth meetings during the months of October and April were asked to complete the survey. To protect the confidentiality of participants, Hatch Youth did not collect names or contact information on the youth, nor did they assign participant identification numbers. Participants completed 614 surveys over a 10-year period. Participants received no compensation. The institutional review board of the first author’s home institution approved study procedures.
Measures
Participants responded to various behavioral and psychosocial measures. All survey items included a “refuse to answer” option. In addition, participants provided demographic information.
Duration of Hatch Youth Attendance
One item asked participants how long they had been coming to Hatch Youth. Responses options included less than 1 month, 1 to 3 months, 3 to 6 months, 6 months to 1 year, and more than 1 year. For analysis, responses were collapsed into three categories: less than 1 month, 1 to 6 months, and 6 or more months.
Time Interval
Data were collected annually in the months of October and April from 2003 through 2013. Each month of data collection was treated as a period of time and entered into analytic models to control for differences in time intervals that might have arisen from changing social acceptance of GLBT persons.
Strength of Primary Social Ties
One item was used as an indicator of the strength of primary social ties, which focused on the youths’ relationships with their families. Participants were asked how they would rate their relationship with their family in the last 90 days. Response options ranged from 1 = very poor to 5 = very high. For analyses, responses were dichotomized into weaker ties (1-3) and stronger ties (4-5).
Strength of Secondary Social Ties
Three items were used as indicators of the strength of secondary social ties, which focused on the youths’ relationship with their social group outside of school. Participants were asked about their agreement with statements concerning whether they had a social group outside of school. They were also asked about their level of outness to their respective social groups. Response options ranged from 1 = strongly disagree to 4 = strongly agree. For analyses, responses were dichotomized into disagree (1-2) and agree (3-4). Participants were also asked how frequently they interact with the GLBT community outside of Hatch Youth. Response options ranged from 1 = never to 5 = very often. For analyses, responses were dichotomized into less interaction (1-3) and more interaction (4-5). After dichotomizing, all three items were entered independently into analytic models.
Risk Behaviors
Four items were used to determine risk behaviors. Participants were asked how often they drank alcohol, used street drugs, and used tobacco in the last 90 days. Response options ranged from 1 = never to 5 = very often. For analyses, responses were dichotomized into not often (1-3) and often (4-5). Participants were also asked if they engaged in safer sex, if sexually active, in the last 90 days. Response options ranged from 1 = never to 5 = always. For analyses, responses were dichotomized into not often (1-3) and often (4-5).
Participant Characteristics
Demographic characteristics included age (continuous), gender (male, female, or transgender), sexual orientation (gay, bisexual, and other), and race/ethnicity (White, Black, Hispanic, or other).
Data Analysis
To describe the youth likely to remain in Hatch Youth for 6 or more months, Student’s t, chi-square, or Fisher’s exact tests were used to examine bivariate associations between the duration of attendance and demographic variables. Because our sample was composed of younger adolescents, aged 13 to 18 years, many health outcomes were rare. This resulted in small sample sizes when accounting for demographics. To avoid large confidence intervals, most measures were dichotomized.
An adjusted ordinal logistic regression model was used to estimate the odds of continuing to attend Hatch Youth based on demographic characteristics. Adjusted binary logistic regression models were used to estimate the extent to which duration of attendance in Hatch Youth was associated the indicators of primary and secondary social ties, to estimate the odds of having positive mental health outcomes, and to estimate the odds of engaging in risk behaviors based on statistically significant demographic and psychosocial characteristics. Stata 13 (StataCorp, 2013) was used for all statistical analyses.
Results
Attendance
Bivariate associations between duration of attendance and demographic characteristics are summarized in Table 1. Variables significant at the bivariate level (p < .05) were entered into an adjusted ordinal logistic regression logistic model. Duration of attendance was regressed on demographic characteristics (Table 2). Older youth were more likely to attend Hatch Youth over time (adjusted odds ratio [aOR] = 1.40; 95% confidence interval [CI] = [1.27, 1.54]). Compared with males, female youth were less likely to attend over time (aOR = 0.70; 95% CI = [0.49, 1.00]) and transgender youth were more likely to attend over time (aOR = 9.49; 95% CI = [4.04, 22.19]). Gay- and bisexual-identified youth attended at similar rates, but youth identifying with other sexual orientations were less likely to attend over time (aOR = 0.24; 95% CI = [0.14, 0.42]). Compared with White youth, Hispanic youth were less likely to attend over time (aOR = 0.63; 95% CI = [0.42, 0.93]). No statistically significant differences were found between White and Black youth or youth with other race and ethnicities.
Demographic Characteristics and Bivariate Associations With Duration of Hatch Attendance (N = 614).
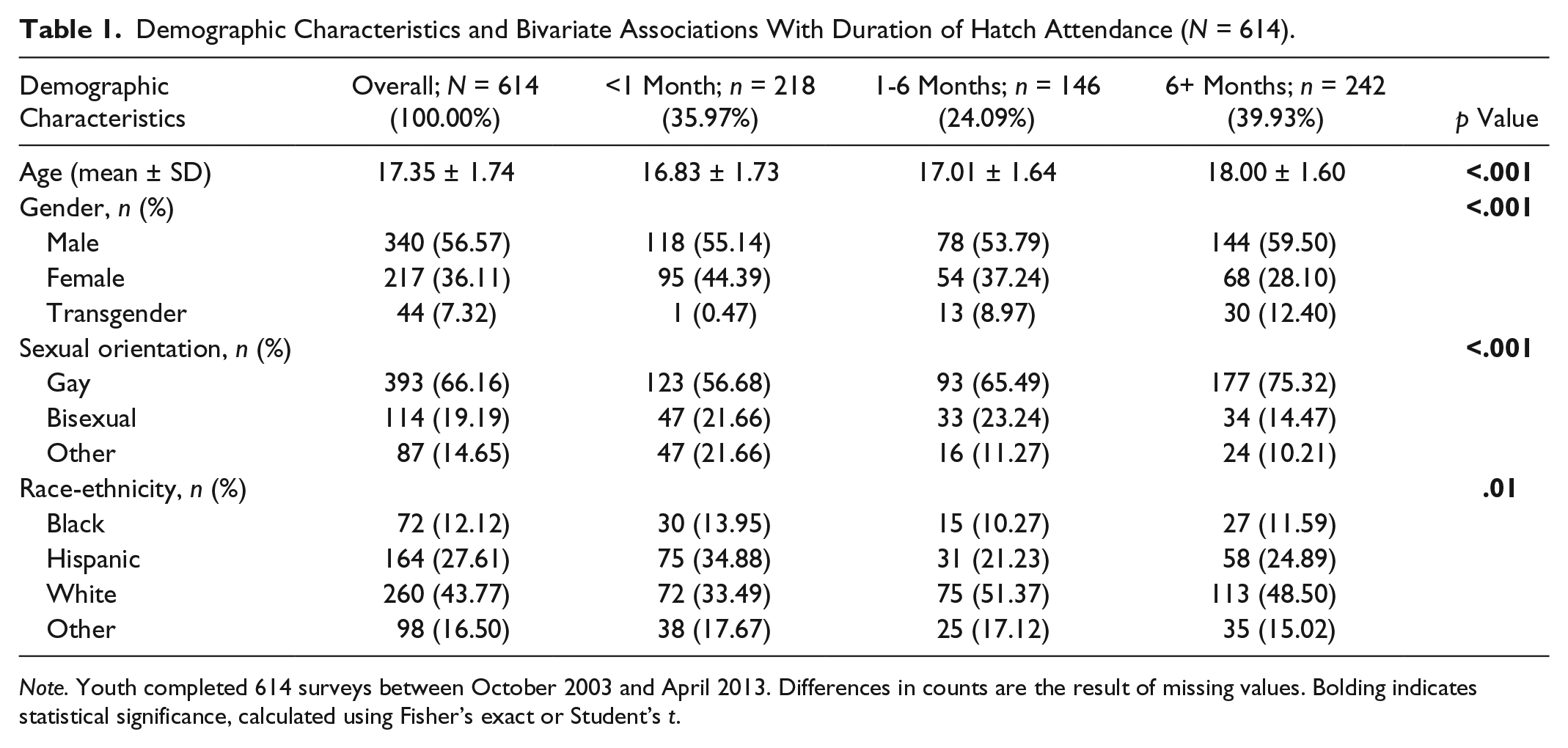
Note. Youth completed 614 surveys between October 2003 and April 2013. Differences in counts are the result of missing values. Bolding indicates statistical significance, calculated using Fisher’s exact or Student’s t.
Odds of Remaining Involved in Hatch Based on Ordinal Logistic Regression (N = 614).
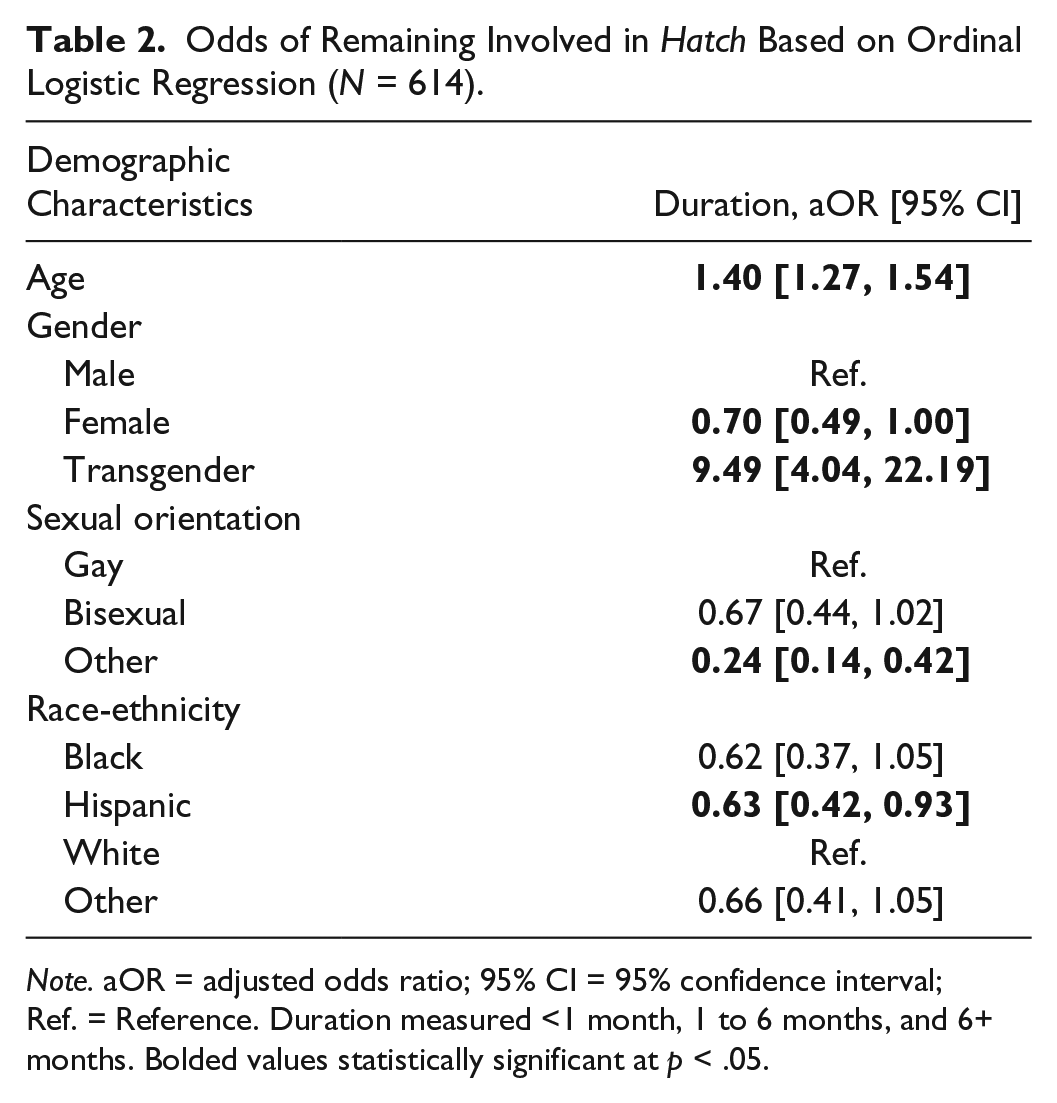
Note. aOR = adjusted odds ratio; 95% CI = 95% confidence interval; Ref. = Reference. Duration measured <1 month, 1 to 6 months, and 6+ months. Bolded values statistically significant at p < .05.
To estimate the extent to which duration of attendance in Hatch Youth was associated with the indicators of primary and secondary social ties, the indicators of social ties were regressed on the duration of attendance and demographic variables using an adjusted binary logistic regression model (Table 3). Duration of attendance and demographic characteristics were not associated with having stronger primary social ties with family in the last 90 days. However, attending Hatch Youth for 6 or more months was associated with having a social group outside of school (aOR = 2.07; 95% CI = [1.33, 3.20]), being out to that social group (aOR = 2.34; 95% CI = [1.35, 4.03]), and interacting with the GLBT community outside of Hatch Youth (aOR = 2.33; 95% CI = [1.50, 3.54]), when referenced against youth attending for less than 1 month. Increased age was associated with having a social group outside of school (aOR = 1.18; 95% CI = [1.06, 1.32]) and being out to the social group (aOR = 1.16; 95% CI = [1.03, 1.32]). Variables associated with being less out to the social group included identifying as bisexual (aOR = 0.40; 95% CI = [0.24, 0.67]) or another sexual orientation rather than gay (aOR = 0.41; 95% CI = [0.22, 0.67]) and being Hispanic rather than White (aOR = 0.51; 95% CI [0.31, 0.83]).
Adjusted Associations With Indicators of Social Support (N = 614).

Note. aOR = adjusted odds ratio; 95% CI = 95% confidence interval; GLBT = gay, lesbian, bisexual, and transgender; Ref. = Reference. Bolded values statistically significant at p < .05.
Mental Health
To examine the relation between positive mental health outcomes (high self-esteem and confidence in ability to handle problems) and participant characteristics, bivariate analyses were conducted (Table 4). Variables significant at the bivariate level (p < .05) were entered into adjusted binary logistic regression models to estimate the odds of having positive mental health outcomes (Table 5). High self-esteem and confidence in ability to handle problems were regressed on demographics, psychosocial characteristics, risk behaviors, and duration of attendance, independently. Statistically significant variables were then entered into the final model.
Bivariate Associations With Mental Health Outcomes (N = 614).

Note. Youth completed 614 surveys between October 2003 and April 2013. Differences in counts are the result of missing values. Bolding indicates statistical significance, calculated using Fisher’s exact or Student’s t. GLBT = gay, lesbian, bisexual, and transgender.
Odds of Having Positive Mental Health Outcomes (N = 614).

Note. To arrive at the most parsimonious model, values significant at bivariate level (p < .05) were entered into Models 1 to 4. Values significant in each model were entered into the final model. Bolding indicates statistical significance. OR = odds ratio; β = slope; 95% CI = 95% confidence interval; GLBT = gay, lesbian, bisexual, and transgender; Ref. = Reference.
The odds of having high self-esteem were lower among females than males (aOR = 0.49; 95% CI = [0.32, 0.76]) and were also lower among youth who used street drugs (aOR = 0.41; 95% CI = [0.19, 0.87]). The odds of having high self-esteem were higher among those who reported having a good family relationship (aOR = 2.48; 95% CI = [1.67, 3.70]), having a social group outside of school (aOR = 2.57; 95% CI = [1.67, 3.97]), and practicing safe sex (aOR = 1.73; 95% CI = [1.13, 2.65]).
Females and transgender youth were less likely than males to feel confident in their ability to handle problems (aOR = 0.53, 95% CI = [0.35, 0.82] and aOR = 0.32, 95% CI = [0.15, 0.69], respectively). The odds of feeling confident in one’s ability to handle problems were higher among those who reported having a good family relationship (aOR = 3.13; 95% CI = [2.10, 4.66]), having a social group outside of school (aOR = 1.82; 95% CI = [1.18, 2.81]), and interacting with a GLBT community outside of Hatch Youth (aOR = 2.32; 95% CI = [1.51, 3.56]).
Risk Behaviors
To examine the relation between risk behaviors (often drink alcohol in last 90 days, often use street drugs in last 90 days, often use tobacco in last 90 days, and often engage in safe sex) and participant characteristics, bivariate analyses were conducted (Table 6). Variables significant at the bivariate level (p < .05) were entered into an adjusted binary logistic regression model to estimate the odds of engaging in risk behaviors given demographic and psychosocial characteristics (Table 7). Risk behaviors were regressed on demographic and psychosocial characteristics independently. Statistically significant variables were then entered into the final model. Older youth were more likely than younger youth to drink alcohol (aOR = 1.23; 95% CI = [1.06, 1.43]). However, over time, alcohol use in general slightly decreased (aOR = 0.95; 95% CI = [0.91, 0.99]). Youth with higher self-esteem were less likely to use street drugs (aOR = 0.45; 95% CI = [0.24, 0.83]). Hispanic youth were less likely than White youth to use tobacco (aOR = 0.40; 95% CI = [0.23, 0.70]), and youth with a social group outside of school were more likely to use tobacco (aOR = 2.37; 95% CI = [1.52, 3.69]). Females were less likely to report often engaging in safe sex, if sexually active (aOR = 0.56; 95% CI = [0.38, 0.84]). However, youth more likely to report often engaging in safe sex were older (aOR = 1.14; 95% CI = [1.02, 1.28]), interacted with the GLBT community outside of Hatch Youth (aOR = 1.64; 95% CI = [1.12, 2.42]), and had higher self-esteem (aOR = 1.86; 95% CI = [1.25, 2.75]).
Bivariate Associations With Risk Behavior Outcomes (N = 614).

Note. Differences in counts the result of missing values. Bolding indicates statistical significance, calculated using Fisher’s exact or Student’s t. GLBT = gay, lesbian, bisexual, and transgender.
Odds of Engaging in Risk Behaviors (N = 614).

Note. To arrive at the most parsimonious model, values significant (p < .05) at bivariate level were entered into Models 1 and 2. Values significant in each model were entered into the final model. aOR = adjusted odds ratio; 95% CI = 95% confidence interval; GLBT = gay, lesbian, bisexual, and transgender. Bolded values statistically significant at p < .05.
Discussion
Attending Hatch Youth for 6 or more months appears to strengthen secondary social ties, particularly for youth who were older, gay, and White. Hatch Youth likely builds within-group secondary social ties through the social hour, the peer-led support group, and the interactions between youth and adult volunteer facilitators. Our findings suggest the program strengthens the out-group secondary social ties examined in this study. For example, a social group outside of school appears to strengthen participants’ interactions with the GLBT community outside of Hatch Youth. These interactions are significant because youth age out of the program at the age of 21 years. Leaving the program with strong secondary social ties external to Hatch Youth is critical for participants to affirm GLBT identities and healthy behaviors. These out-group secondary social ties are likely facilitated by inviting members of community groups into Hatch Youth meetings to educate youth about their groups and by taking the youth on field trips to age-appropriate GLBT community events. Identifying how GLBT drop-in centers, including Hatch Youth, can best facilitate the formation of strong out-group secondary social ties for youth preparing to age-out of their programs is important to future research.
Duration of attendance had no statistically significant impact on primary social ties as measured by how youth would rate their relationship with their family in the last 90 days. While the lack of significance could be the result of measurement error (i.e., the only assessment was a single-item measure developed by program staff), a more cogent explanation is that the program was not developed to strengthen primary social ties. Instead, the model was developed at a time when most GLBT youth could not expect support from family members. However, while not all GLBT youth can expect support from primary social ties, anecdotally, more parents with GLBT youth are wanting to support their youth, despite lacking the confidence, knowledge, and skills to do so. Research is needed to identify best practices for drop-in programs like Hatch Youth also seeking to strengthen primary social ties.
Examining the direction of the odds ratios in Table 2 and not just at statistical significance (parameter estimates were wide for some categorizations due to small counts), there is evidence to suggest that Hatch Youth was less effective at retaining females, racial and ethnic minorities, and non-gay-identified youth. Additionally, while a number of factors were related to positive mental health outcomes that could be attributed to participating in Hatch Youth, including having a social group outside of school and interacting with the GLBT community outside of Hatch Youth, female and transgender participants did not demonstrate having the same mental health benefits. As discussed by Mustanski et al. (2010) and Shilo and Savaya (2011), racial and ethnic minority youth, transgender youth, and youth rejecting the hegemonic heterosexual–homosexual dichotomous sexual identity labels might experience weaker social ties, increasing their need of programs like Hatch Youth. Thus, additional research is needed to identify best practices for drop-in programs like Hatch Youth seeking to be more inclusive.
Hatch Youth showed little evidence of influencing alcohol or street drug use, possibly because Hatch Youth participants are younger adolescents who may not have easy access or exposure to alcohol or drugs. Odds ratios indicated tobacco use was more likely to occur when youth attended Hatch Youth for longer than 6 months and reported having a social group outside of school. Tobacco use is highly prevalent among sexual and gender minorities (Fallin, Goodin, Lee, & Bennett, 2015). Hatch Youth participants may encounter an increased exposure to tobacco products when interacting with the adult GLBT community, or they may rely on tobacco when dealing with uncomfortable social interactions outside of Hatch Youth. Additional research should examine tobacco use behavior and ways to prevent tobacco use among GLBT youth attending drop-in center programs like Hatch Youth.
Hatch Youth participants who were older, interacted with the GLBT community outside of Hatch Youth, and who had high self-esteem were more likely to have reported engaging in safer sex. These findings suggest Hatch Youth may have some promising impact on safe sex practices; however, females were less likely than males to report safer sex practices. Messaging promoting condom use may not be well-tailored to females who may be engaging in sexual activity with males. More research is needed to determine the best way to tailor messages to females and to determine whether unsafe sex is occurring with male partners, which could have implications for HIV/sexually transmitted infection prevention and unplanned pregnancy.
While demonstrating that drop-in programs like Hatch Youth can strengthen secondary social ties, the reader should be mindful of study limitations, such as the exploratory nature of these analyses, when interpreting results. Because of the historical discrimination and a desire to protect the anonymity of Hatch Youth participants, the program does not collect identifiable information on the youth. As a result, the likelihood of participants in the program completing the survey instrument more than once is likely. In addition, this study used secondary data analysis of survey items developed by Hatch Youth program staff. While the single-item measures have face validity, researchers collaborating with drop-in centers are encouraged to assist program staff in identifying published, validated measures. Additionally, as this was an analysis of data from one drop-in center, it may be difficult to generalize the findings to other locations. Future research should compare data from multiple drop-in centers to identify best practices for strengthening social ties.
Implications for Research and Practice
This study demonstrates that Hatch Youth, and perhaps similar programs, strengthens secondary social ties, especially for youth attending the program for 6 or more months. As social ties theory posits, by strengthening secondary social ties and social support, drop-in centers like Hatch Youth have the potential to reduce the health disparities experienced by GLBT youth and influence safer sex practices. Researchers and practitioners should support these programs by identifying best practices and encouraging communities with fewer supports for GLBT youth to establish similar drop-in centers.
Footnotes
Authors’ Note
Research protocols were approved by the University of Texas Health Science Center at Houston Center for Protection of Human Subjects (institutional review board).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the Substance Abuse and Mental Health Services Administration’s Service and Science Initiative.