
Abstract
Background. As pregnant mothers increasingly engage in shared decision making regarding prenatal decisions, such as induction of labor, the patient’s level of activation may influence pregnancy outcomes. One potential tool to increase patient activation in the clinical setting is mobile applications. However, research is limited in comparing mobile apps with other modalities of patient education and engagement tools. Aim. This study was designed to test the effectiveness of a mobile app as a replacement for a spiral notebook guide as a patient education and engagement tool in the prenatal clinical setting. Method. This randomized controlled trial was conducted in the Women’s Health Clinic and Family Health Clinic of three hospitals. Repeated-measures analysis of covariance was used to test intervention effects in the study sample of 205 patients. Results. Mothers used a mobile app interface to more frequently record information about their pregnancy; however, across time, mothers using a mobile app reported a significant decrease in patient activation. Discussion. The unexpected negative effects in the group of patients randomized to the mobile app prompt these authors to recommend that health systems pause before distributing their own version of mobile apps that may decrease patient activation. Conclusion. Mobile apps can be inherently empowering and engaging, but how a system encourages their use may ultimately determine their adoption and success.
Keywords
The activated patient is a collaborative partner with the health care team (Greene & Hibbard, 2012). In the clinic, this patient asks questions and engages in conversations with providers (Street, Gordon, Ward, Krupat, & Kravitz, 2005). Although they may share in health decisions or delegate decisions to their provider, activated patients have the knowledge, skills, and confidence to enact treatment recommendations (Hibbard & Mahoney, 2010). Within maternity care, patient activation has been linked to maternal health outcomes, including healthy postpartum weight management (Ohlendorf, Weiss, & Oswald, 2015). Patient activation is becoming increasingly important as patients engage in shared decision making regarding prenatal decisions such as induction of labor (Moore, Low, Titler, Dalton, & Sampselle, 2014; Moore, Titler, Kane Low, Dalton, & Sampselle, 2015).
As a modality, mobile applications have the potential to increase patient activation (Ledford, Canzona, Cafferty, & Hodge, 2016). Mobile apps offer patients health-related benefits, to include enhancing self-management (Anderson, Burford, & Emmerton, 2016; Hui et al., 2017; Underwood, Birdsall, & Kay, 2015) and daily monitoring and recording of mood and activity (Reid et al., 2013). Mobile app use is especially prevalent among pregnant mothers (Fleming, Vandermause, & Shaw, 2014; Lee & Moon, 2016; Robinson & Jones, 2014; Tripp et al., 2014; Wallwiener et al., 2016). Most women are not looking to replace or disregard the information given by providers but rather to supplement provider information (Grimes, Forster, & Newton, 2014; Kraschnewski et al., 2014). This media complementarity is endorsed by Sridhar and Chen (2014) who assert that patient use of mobile apps is most effective in supplementing interpersonal health care rather than replacing counseling. Although evidence is emerging about the use of mobile apps to improve patient outcomes in chronic disease management (Hui et al., 2017), evidence to the effectiveness of mobile apps in improving maternity care is limited (Agarwal & Labrique, 2014).
Self-determination theory (SDT) provides an organizing framework for understanding the potential effects of mobile apps as a health intervention (Deci & Ryan, 1985). SDT posits that when an action is self-determined, the individual’s motivation to enact a behavior is stable. This stable motivation results in increased perseverance and maintenance of a target behavior. Moreover, motivation can be enhanced by ensuring that a patient’s social environment meets three psychological needs: autonomy, competence, and relatedness (G. C. Williams et al., 2005; G. C. Williams & Deci, 2001; G. C. Williams, Freedman, & Deci, 1998; G. C. Williams, McGregor, Zeldman, Freedman, & Deci, 2004). That is, when we design an intervention to motivate a target behavior, we should enable the individual to believe the decision to enact a behavior is self-regulated (autonomy), to believe she is able to maintain the change (competence), and to believe that her decision to change is supported by those whose opinion she values (relatedness).
The nature of a mobile app, by its interactive design and personal nature, may support patient autonomy and competence. Mobile apps have the singular functionality to allow the patient to record information during and between appointments, which builds a portable, electronic record of their own health. Women value mobile apps that provide regular notifications and that allow the mother to self-track data (Lupton, 2016), and mobile apps have been demonstrated to engage perinatal women to promote behavior change (Hearn, Miller, & Lester, 2014). However, evidence is mixed on the relative advantage of mobile apps over other modalities of patient education and engagement. Comparing a mobile app, Website, and a paper diary, mobile app users were more likely to self-monitor their diet; however, no effect was detected on actual weight loss (Carter, Burley, Nykjaer, & Cade, 2013). In a comparison of mobile apps against standard paper diaries, patients with type 1 diabetes mellitus reported no significant difference in quality of life, disease-related distress, or glucose levels (Drion et al., 2015). And in a comparison against text messaging, a mobile app was demonstrated to be feasible for delivering smoking cessation support but was not as efficient as text messaging (Buller, Borland, Bettinghaus, Shane, & Zimmerman, 2014).
As patients interact with the information and functionality of an app, they are enabled to become more engaged in their care. Physicians communicate differently with patients who they perceive to be more active in clinic interactions (Street, Gordon, & Haidet, 2007). Physicians can provide autonomy support by assessing the patient’s perspective, offering information, and encouraging self-initiation. Conversely, physicians can be autonomy controlling by pressuring the patient toward a behavior, assuming that their authority is enough to motivate patients (G. C. Williams, Frankel, Campbell, & Deci, 2000). In that context, patient autonomy facilitates patient competence, which physicians can also increase through specific instruction and feedback (Ryan, Patrick, Deci, & Williams, 2008).
When a patient experiences increased competence, she believes she is able to enact and maintain a behavior. This psychological need aligns with the clinical concept of patient activation. Activated patients believe that the role of patient is important, that they have the confidence and knowledge necessary to take action, and that they can enact behaviors to maintain and improve their health (Hibbard, Mahoney, Stock, & Tusler, 2007; Hibbard, Stockard, Mahoney, & Tusler, 2004; S. S. Williams & Heller, 2007).
Within SDT, autonomy does not indicate solely independent action but the feeling of volition that can facilitate any behavior (Ryan & Deci, 2000). The theory prescribes that patients need to experience autonomy and relatedness. This is an important distinction clinically because target behaviors are often identified through shared decisions between a patient and physician (Elwyn et al., 2012; Epstein & Street, 2011; Murray, Charles, & Gafni, 2006). The provider is one of a potential set of valued opinions that may influence a patient’s self-determination. We propose that through autonomy support and increased competence, a mobile app may also have an effect on a patient’s perception of relatedness. In the clinical encounter, prenatal interpersonal processes of care (PIPC) can be a surrogate for relatedness. PIPC conceptually and operationally captures three dimensions of clinical care: communication, patient-centered decision making, and interpersonal style (Hessol, Odouli, Escobar, Stewart, & Fuentes-Afflick, 2012; Wong, Korenbrot, & Stewart, 2004). Evidence has identified a limited association between interpersonal processes of care and risk of Cesarean delivery (Hessol et al., 2012).
In a pilot study, we demonstrated that a mobile app for prenatal education and engagement can improve both patient activation and PIPC (Ledford et al., 2016). The following randomized controlled study was designed to extend the generalizability of that pilot by testing the effectiveness of a mobile application as an alternative to a spiral notebook guide throughout prenatal care in a multisite trial. Within the framework of SDT, it is proposed that providing pregnant mothers with a mobile app is an autonomy-supporting behavior that will increase their competence and relatedness.
Three hypotheses were tested.
Method
The study was conducted in the women’s health and family medicine departments of one community hospital and two medical centers across three states (Georgia, Nevada, and Virginia). In this hospital system, women are distributed a spiral notebook at their obstetric care intake appointment, which is generally scheduled at 8 to 10 weeks gestation. The spiral notebook is designed for two purposes: (1) patient education of what happens throughout pregnancy and (2) patient record keeping of her own pregnancy experience, including space for recording weight, blood pressure, and journaling. The mobile app used in this study was designed for the same two purposes and contained identical content, though via a mobile design interface (available on both Android and iOS platforms). After the pilot study (Ledford et al., 2016), patient feedback on the mobile app was used to create a beta version. Notable differences were a feature for users to change font size, a search function, and weekly reminders. No substantive content changed. This randomized controlled study had one intervention (mobile application) and one control (standard of care–spiral notebook) group. The study was approved by the first author’s institutional review board.
At each hospital, the obstetrics intake nurse serially screened new maternity patients for inclusion criteria from May to November 2015. If patients met inclusion criteria, the nurse invited the patient to talk to a research assistant about the study. Exclusion criteria included conditions that would elevate the patient’s care to complicated obstetrics care (e.g., cardiovascular disease, diabetes mellitus, renal disorder, etc.). This was intended to capture a low-risk obstetrics patient population that would follow a standard 4-week pathway of care, in which patients attend a prenatal appointment once every 4 weeks during pregnancy.
The study used preassigned block randomization (each block n = 40) to balance the conditions throughout recruitment. Following consent and baseline measures, participants were randomized to the two conditions. Providers were blinded to patient participation in the study.
Surveys were completed at four prenatal appointments, 16 to 20 weeks, 28 weeks, 32 weeks, and 36 weeks gestation. All data collection was conducted with paper-and-pencil surveys in the clinic, immediately before and following each clinical appointment. At each appointment, patient weight and blood pressure were also recorded from the patient’s electronic medical record.
At baseline, self-reported measures included demographics, health literacy, and patient activation. Health literacy was assessed using the self-reported Functional, Communicative, Critical Health Literacy Scale (Ishikawa, Takeuchi, & Yano, 2008). Patient activation was assessed with the validated, licensed patient activation measure (PAM; Greene & Hibbard, 2012; Greene, Hibbard, Sacks, & Overton, 2013; Hibbard et al., 2004; Hibbard, Mahoney, Stockard, & Tusler, 2005). The scale includes 13 Likert-type items such as “Taking an active role in my own health care is the most important thing that affects my health,” “I am confident that I can tell doctor concerns that I have even when he or she does not ask,” and “I am confident I can figure out solutions when new problems arise with my health.” The 13 items combine to create a continuous PAM on a scale of 0 (not activated) to 100 (most activated). For hypothesis testing, PAM was repeated at Time 4 (32-week appointment).
At 36 weeks, we also asked patients how many pregnancy-related mobile apps they had used throughout their pregnancy.
For the first hypothesis, use was assessed with three measures. Before each appointment, patients completed three items regarding their use of the education and engagement tool. First, they indicated if they had brought the mobile app/notebook to the appointment with them (yes/no). The initial impetus for creating a mobile app version of the notebook resulted from provider recognition that mothers frequently forgot to bring the notebook to their appointments. A main function of the notebook was for the mother to record information her provider told her during the appointment. The potential of increased portability of a mobile app loaded on the mother’s mobile phone was a primary motivation for the development and evaluation of the app. Second, they reported how frequently they had used the tool over the past month to look for information, and third, they reported how frequently they had used the tool to record information (never, once, weekly, or daily). These responses were transformed to represent how many times mothers had used the tool since their last prenatal appointment, which occur approximately once every 4 weeks, or 28 days (never = 0, once = 1, weekly = 4, or daily = 28).
Following each appointment, patients completed five subscales of the validated PIPC scale (Wong et al., 2004), including elicitation/responsiveness to the patient, explanations of care, empowerment, patient-centered decision making, and emotional support. Responses to each item were transformed onto a 0 (negative perception) to 100 (positive perception) scale, and items are averaged to create subscales. Subscales are then averaged to calculate the overall PIPC scale. Across time points in this study, the PIPC scale’s internal reliability (Cronbach’s alpha) ranged from .787 to .854.
A set of secondary outcomes were collected at delivery. Outcomes recorded from the health record included: gestational age, birth weight, and mode of delivery (vaginal or Cesarean section).
Results
Of the 241 patients who completed consent, 120 were assigned to the mobile condition and 121 were assigned to the notebook condition. Analysis of variance (continuous variables) and chi-square (nominal variables) tests were used to compare the intervention and control groups (see Table 1 for sample characteristics). No group differences were detected.
Sample Characteristics Overall and by Condition (No Significant Differences Detected).

Figure 1 describes the number of and reasons for patient withdrawals per group.
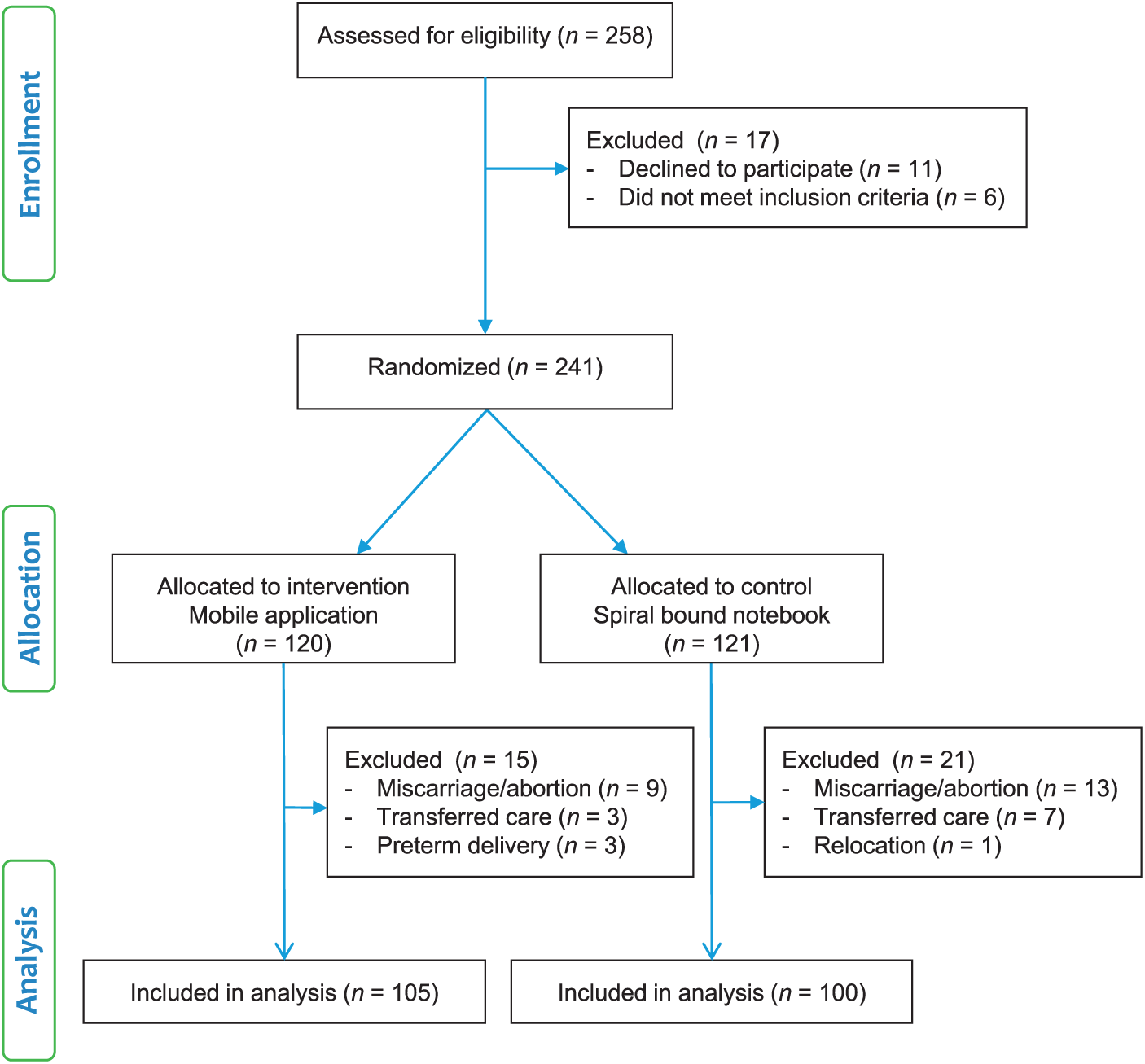
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Additionally, at each time point, some participants did not complete a survey for the following reasons: patient arriving early for appointment (without research assistant notification), patient declining survey after appointment due to time constraints, and clinic canceled appointments due to weather conditions. No one mother missed more than one survey. At 16 to 20 weeks, 5 (2.4%) did not complete the PIPC scale. At 28 weeks, 30 (14.6%) did not complete the PIPC scale. At 32 weeks, 6 (2.9%) did not complete the PIPC scale and 31 (15.1%) did not complete the PAM scale. At 36 weeks, 48 (23.4%) did not complete the PIPC scale. These percentages are similar to the missing rate of 15% to 20% common in psychological studies (Enders, 2003).
For these missing items, we compared women who completed the item with women who did not complete the item. Condition was not related to missingness. Also, no demographic differences were detected between the two groups, creating no pattern of missingness. For the missing items, linear regression imputation was used on individual subscaled items. This imputation replicates the procedure used for missing data in the pilot study.
For the first hypothesis, chi-square tested condition effects on if the patient brought the tool with her to each appointment. Starting at the 16- to 20-week appointment and throughout the remainder of the pregnancy, patients in the mobile group were repeatedly more likely to bring the mobile app to the appointment as compared with women bringing the notebook, χ2(1, 201) = 27.96, p < .001. A repeated-measures analysis of variance (RM ANOVA) model tested intervention effects on the four time-point measurements of patient use of the tool to find information about pregnancy. No significant difference was detected between the two groups. The RM ANOVA was then repeated on patient use of the tool to record information about her pregnancy. Across all time points, the mobile group reported more frequent use than the notebook group, F(1, 203) = 4.37, p < .05, η2 = .02. Therefore, Hypothesis 1 is partially supported.
For the second hypothesis, an ANOVA tested the effect of condition on change in patient activation from baseline to the 32-weeks-gestation measurement. Condition had a significant association with change in patient activation, F(1, 203) = 4.82, p < .05. Across the pregnancy, patient activation in the notebook group increased an average 3.44 points, 95% confidence interval (CI) [0.52, 6.37], whereas patient activation in the mobile group decreased an average 0.91 points, 95% CI [−3.55, 1.73]. Therefore, Hypothesis 2 was not supported: Patients who were distributed the notebook developed greater patient activation than patients who were distributed the mobile app.
In an effort to understand this unexpected difference, a second ANOVA tested group differences on the number of mobile apps downloaded. This test revealed a significant association between condition and the number of mobile apps downloaded, F(1, 163) = 7.91, p < .01. Patients randomized to the notebook group downloaded an average 1.99 mobile apps, 95% CI [1.49, 2.49], while patients in the mobile app group downloaded an average 1.19 mobile apps, 95% CI [0.89, 1.48] (other than the intervention delivered app).
For the third hypothesis, RM ANOVA model tested intervention effects on four time-point measurements of PIPC. Starting at the second survey, the notebook group rated PIPC higher than the mobile app group (see Figure 2.) However, this difference was not statistically different. Therefore, Hypothesis 3 was not supported.
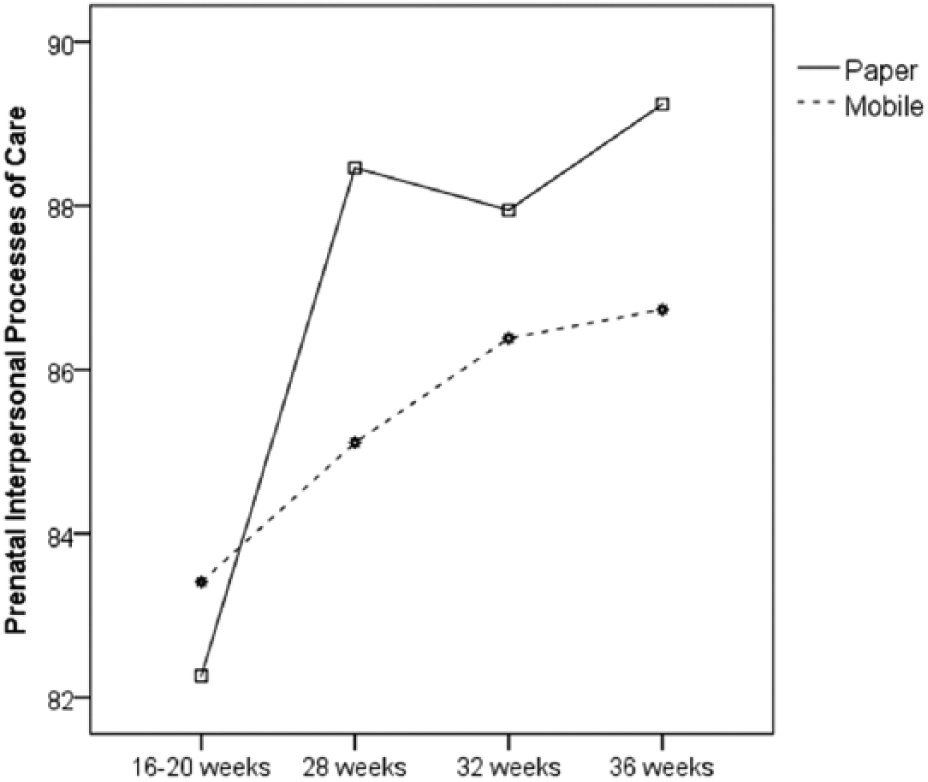
Comparison of traditional paper and mobile app groups on the prenatal interpersonal processes of care.
Though not hypothesized, intervention effects were tested on blood pressure control and weight gain throughout the pregnancy. Intervention effects were also tested on delivery outcomes: gestational age, birth weight, and delivery mode. No difference was detected on health measures throughout the pregnancy, on gestational age, or birth weight. However, a chi-square revealed a significant difference in delivery mode by condition, χ2(1, 167) = 7.89, p < .01. Patients randomized to the mobile app group were significantly more likely to deliver via Cesarean section. The notebook group had a 12.3% Cesarean section rate, while the mobile app group had a 30.2% C-section rate. (for context, in 2015, the U.S. nationwide Cesarean section rate was 32% [Martin, Hamilton, & Osterman, 2016]).
Discussion
Mothers used a mobile app interface to more frequently record information about their pregnancy; however, across time, mothers using a mobile app reported a significant decrease in patient activation as compared with mothers using a paper notebook. Findings in this multisite trial do not replicate findings from the pilot study (Ledford et al., 2016). This multisite trial reflects a more geographically diverse population as well as a sample that is significantly younger and more diverse in education and marital status.
Also concerning is the unexpected and unexplainable association between patient education and engagement modality and childbirth delivery mode. Though we infer no causality in this association, we cannot overlook the potentially negative spiral of decreased patient activation and its potential effects on health outcomes.
Of note is the finding that mothers in the paper group used more mobile apps throughout their pregnancy. Within the SDT framework, it is possible that the issuance of a system-adopted mobile app prompted a type of iatrogenic effect. The issuance may have acted as an autonomy-controlling communicative behavior, which decreased patient motivation to seek information. When mothers in the mobile group were issued the app, it is possible that they were not motivated to seek out prenatal information in that modality, whereas mothers in the notebook group were still motivated to search out a mobile app to supplement the information in the notebook with an electronic modality.
People whose motivation is self-authored have more interest, excitement, and confidence (Ryan & Deci, 2000) than people who are externally controlled. This difference then perpetuates in enhanced performance and persistence (Sheldon, Ryan, Rawsthorne, & Ilardi, 1997) and general well-being (Reis, Sheldon, Gable, Roscoe, & Ryan, 2000), even when people have the same level of self-efficacy for the target behavior (Ryan & Deci, 2000).
Through this theoretical lens, we posit that one interpretation of these results is a critique not on mobile applications as a modality in general but in the delivery of apps to patients. As health communicators and health systems develop and deliver mobile apps to their patient populations, they should be attentive to how that product is delivered. Mobile apps can be inherently empowering and engaging, but how a system encourages (and enforces) their use may determine their adoption and success. This lesson is particularly salient for systems that mandate patient portals for access to health information.
Results here demonstrate two benefits of mobile applications: portability and increased patient record. If health systems are most concerned about these two factors, then mobile applications can provide a solution. However, the three levels of patient-centered outcomes (patient activation, perception of care, and delivery mode) showed no advantage to the use of a mobile app. Providers may see benefit in recommending apps but not necessarily in developing or directly delivering mobile apps to patients. Health systems searching for modalities to activate patients should consider the evident utility of paper notebooks as an education and engagement tool. The authors recommend that health systems pause before distributing their own version of mobile apps that may decrease patient information seeking and patient activation.
Limitations exist for the results presented here. First, findings are limited by the self-report nature of the measures used. Second, this study enrolled only mothers with low-risk pregnancies. It is possible mothers with high-risk pregnancy would have different information needs and needs for autonomy, competence, and relatedness. Also, as the intervention relied on mothers recording clinical information into the mobile app or notebook, it is possible that providers noticed that behavior and altered their own practice to accommodate it. Future research is needed to replicate this study in populations with varying health concerns as health care systems move forward with mobile app development to improve patient education and engagement.
Footnotes
Acknowledgements
This study was conducted within the Military Primary Care Research Network. We acknowledge the clerks, nurses, and staff for welcoming us into their workplace.
Authors’ Note
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Air Force, U.S. Army, the Uniformed Services University of the Health Sciences, or the Department of Defense at large.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Department of Defense (FAM 81-3193).