
Abstract
Many researchers and authorities have recognized the important role that sports clubs can play in public health. In spite of attempts to create a theoretical framework in the early 2000s, a thorough understanding of sports clubs as a setting for health promotion (HP) is lacking. Despite calls for more effective, sustainable, and theoretically grounded interventions, previous literature reviews have identified no controlled studies assessing HP interventions in sports clubs. This systematic mapping review details how the settings-based approach is applied through HP interventions in sports clubs and highlights facilitators and barriers for sports clubs to become health-promoting settings. In addition, the mapped facilitators and barriers have been used to reformulate previous guidelines of HP in sports clubs. Seven databases were searched for empirical research published between 1986 and 2017. Fifty-eight studies were included, principally coming from Australia and Europe, describing 33 unique interventions, which targeted mostly male participants in team sports. The settings-based approach was not yet applied in sports clubs, as more than half of the interventions implemented in sports club targeted only one level of the socio-ecological model, as well as focused only on study participants rather than the club overall. Based on empirical data, the analysis of facilitators and barriers helped develop revised guidelines for sports clubs to implement settings-based HP. This will be particularly useful when implementing HP initiatives to aid in the development of sports clubs working with a whole setting approach.
Keywords
According to the World Health Organization (WHO), health promotion (HP) is “the process of enabling people to increase control over and to improve their health” (WHO, 1986). The Ottawa Charter (WHO, 1986) pointed out the importance of a settings-based approach (Whitelaw et al., 2001) in HP. A setting is “the place or social context in which people engage in daily activities in which environmental, organizational and personal factors interact to affect health and well-being” (Nutbeam, 1998). Different settings, such as schools (Rees et al., 2006), hospitals (Johnson & Baum, 2001), workplaces (Noblet, 2003), or cities (De Leeuw, 2009) have considered this (Golden & Earp, 2012), when implementing HP interventions. The settings approach is rooted in a socio-ecological understanding about health (Dooris, 2004) highlighting the importance of the whole system of the setting (Kokko, 2014b), rather than just individual responsibility, when promoting health.
The socio-ecological model assumes not only that multiple levels of influence exist, namely, the intrapersonal, interpersonal, institutional, community, and policy level but also that these are interactive and reinforcing (Golden & Earp, 2012). However, it is not only the setting that could have an impact on its actors but also the actors that shape the setting, that is, reciprocal determinism (Kokko, Green, & Kannas, 2014). While sports clubs’ core business is centered on sport performance (Kokko, 2011), promoting health (through e.g., the physical environment, the content, or coaching practice) could not only decrease drop out intentions of members within a club (Van Hoye, Heuzé, Van den Broucke, & Sarrazin, 2016) but also enhance sport clubs’ results and performance, as well as the participant’s health outcomes.
Different authors have underlined the potential of sports clubs to become a HP setting (Donaldson & Finch, 2012; Geidne, Quennerstedt, & Eriksson, 2013b; Kokko et al., 2014) in doing their core sporting activity. Indeed, sport clubs reach a large audience and enhance the physical, psychological, and mental health of their participants through sport and physical activity practice (Eime, Young, Harvey, Charity, & Payne, 2013; O’Donovan et al., 2010; Rhodes, Janssen, Bredin, Warburton, & Bauman, 2017; Warburton, Nicol, & Bredin, 2006). However, other research has balanced this enthusiasm by questioning the “myth of healthism” (Holman et al., 1997), which surrounds sports. In fact, sport participants are more likely to use alcohol and steroids than nonsport participants (Holman et al., 1997; Moore & Werch, 2005; Musselman & Rutledge, 2010), and social and gender inequity in sport is still common (Alsarve, 2018; Collins, 2004). Therefore, considering sport clubs as health promoting just because of the benefits of sport practice is reductive, as they could, through their informal educational nature, also have an effect on other health determinants and on community health (Geidne et al., 2013; Kokko, 2014b). The settings-based approach is grounded in previous research demonstrating that interventions developed with an explicit theoretical foundation are more effective than those lacking a theory base (Golden & Earp, 2012). This approach also points out the need to concentrate on creating feasible, effective, and long-lasting interventions in order to test the empirical implementation of the settings-based approach in sports clubs (Kokko et al., 2016).
For sports clubs, the settings-based approach has been adapted using two types of categories (determinants and layers), with determinants (social, cultural, environmental, economic) influencing three layers of the sports club: the macro- (overall policies and orientations of a club), meso- (guidance activities of club officials), and micro-layer (coaches’ activities in guiding, altering, or supporting actions of club members; Kokko, 2014b). Moreover, the settings-based approach emphasizes the belonging within the community and other settings, especially in this case with local authorities, schools, or other organizations that share common infrastructures (Kokko, 2014b). A health-promoting sports club is a setting (which does not need to have physical boundaries) with sustained HP practices at the organization, club, and coach levels of the system (Kokko et al., 2016) where HP actions support the core business, that is, sports performance and development.
Two previous Cochrane reviews focused on the effectiveness of HP strategies developed within sporting organizations to increase participation (Priest, Armstrong, Doyle, & Waters, 2008a) and the effectiveness of policy interventions implemented in sports clubs to instigate or sustain healthy behavior (Priest, Armstrong, Doyle, & Waters, 2008b). Because of the rigorous design criteria of Cochrane reviews, no publications met the inclusion criteria, and therefore, none were included in the above reviews, leading to a lack of clear direction to improve HP in sports clubs. Priest and colleagues (2008a, 2008b) recognized that the only available evidence to answer the questions raised in their reviews were located in uncontrolled case studies. Recently, an integrative review of 44 publications, using the strategies of the Ottawa Charter (WHO, 1986) to understand HP for youth in sports clubs proposed a theoretical model underlining the key elements of HP such as education, participation, policy, priority design, financing and key actors including parents, coaches, and officials in cooperation with related settings (Geidne et al., 2013b). This review did not differentiate between cross-sectional studies and interventions, leading to a lack of identified facilitators and barriers to sports clubs becoming health-promoting settings. Finally, an update of the Cochrane review (Priest et al., 2008a, 2008b) has been proposed, with the aim of measuring effectiveness of interventions implemented through sporting organizations, in particular, to promote physical activity, healthy diet, and reductions in alcohol consumption or tobacco use (Flatz et al., 2016). The present systematic mapping review of a number of empirical studies analyses sports clubs’ HP interventions from a theoretical perspective using the settings-based approach developed by Kokko and colleagues (Kokko, 2014b).
This systematic mapping review analyses how the settings-based approach is applied through HP interventions in sports clubs and maps facilitators and barriers for sports clubs to become health-promoting settings.
Method
Systematic mapping reviews are carried out to map the existing literature and subsequently identify trends and gaps that may lead to future research (Grant & Booth, 2009). Because of the large variety of health outcomes from a settings-based approach (Dooris, 2006) and the ongoing literature review on measuring the effectiveness of HP interventions (Flatz et al., 2016), the present study focused on evidence-driven mechanisms of HP interventions to identify how the settings-based approach was applied to sports clubs. In other words, each article was considered as a case study, collecting empirical data on sport clubs’ practices (cf. Sullivan, Bretschneider, & McCausland, 2003).
A literature search was carried out in the spring of 2017 over a time frame between 1986 and May 1, 2017 in the following databases: Medline, The Cochrane Library, SPORTdiscus, ERIC, PASCAL, PsycInfo, and ISI Web of Knowledge. The key concepts were HP, sports, and intervention used with different synonyms suitable for different contexts.
The main inclusion criteria for study selection were (a) to consider English peer-reviewed articles, (b) to describe a HP intervention within sports clubs, targeting sports participants, coaches, and officials, not only spectators. Interventions are defined in a wider sense as, “to disturb the ‘natural’ order of things or a foreseeable sequence of events” (Hawe & Potvin, 2009), and (c) empirical studies. Excluded studies focused on settings other than sports clubs—defined as having “in common, the provision of opportunities for competition and sports practice, while some can also be considered social organizations, promoting social welfare and health,” (Donaldson & Finch, 2012)—this excludes, for example, (a) extracurricular activities organized by schools and sport-for-development programs organized by communities, (b) sport performance enhancement only, (c) management process without mentioning anything health-related, and (d) protocols and reviews. The first and last authors independently assessed titles and abstracts using Covidence software. In case of disagreement, a decision was made by a third researcher. The PRISMA flow diagram (Moher, Liberati, Tetzlaff, Altman, & Group, 2009) describes the article selection process (Figure 1).
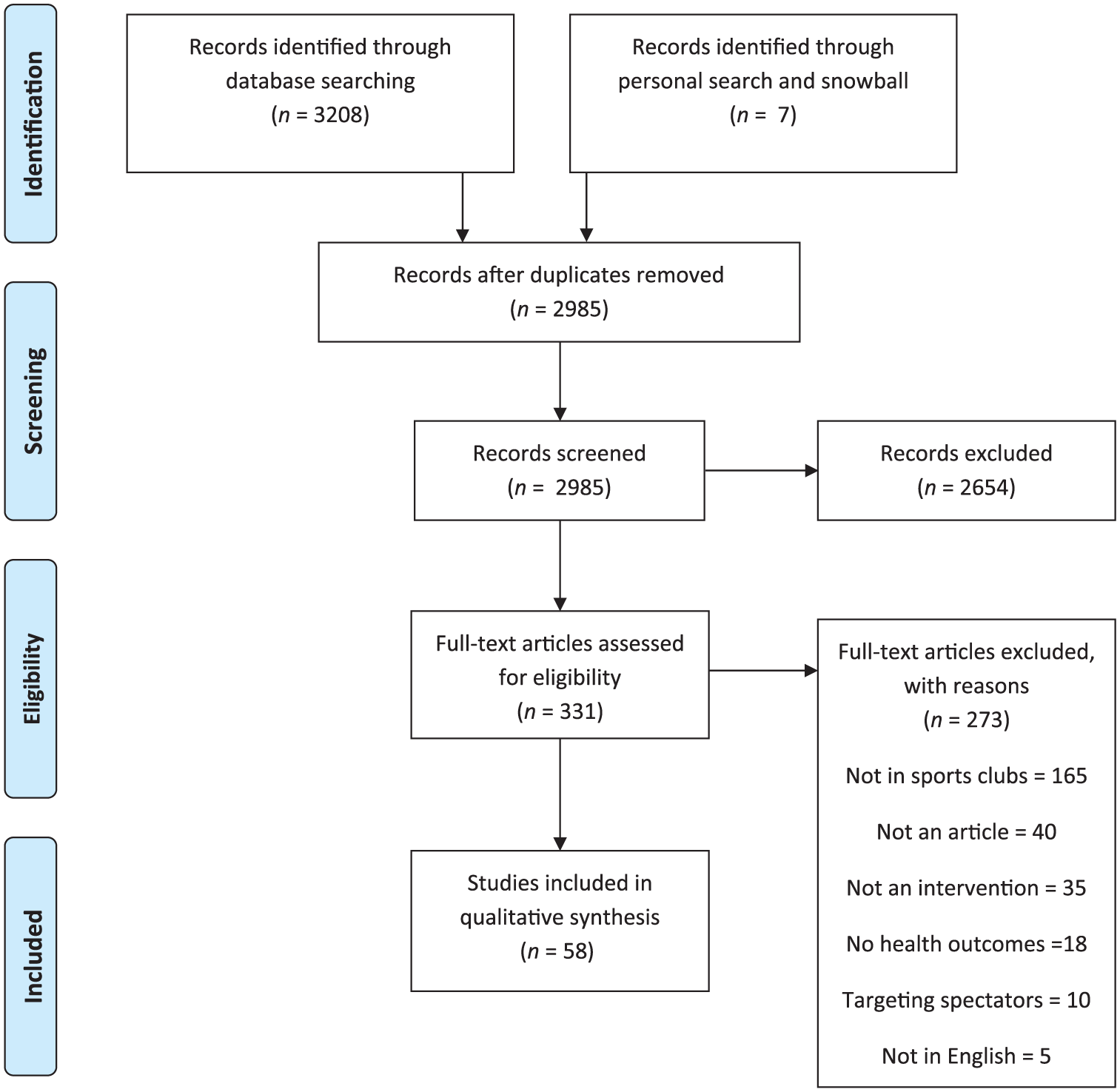
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram for study selection.
Content was extracted and analyzed descriptively, reporting title, date of study, location, characteristics of the intervention (behavior focus, sport, name, public targeted, component of intervention), layer of the sports club included in the intervention (micro, meso, macro; Kokko, 2014b), targeted socio-ecological level (intrapersonal, interpersonal, institutional, community and policy; Golden & Earp, 2012), theory-driven or model-driven intervention (Glanz & Bishop, 2010), and study design and methods used (Supplemental Appendix 1, available in the online version of this article). The layer of the sports club was coded with regard to the actors implicated in the intervention, reported in the articles. For example, if coaches of a sports club were involved in a specific intervention, we coded the intervention as being at the microlevel.
Facilitators and barriers were analyzed qualitatively using a theoretically driven coding process according to the 14 statements of the guidelines for best practice for sports clubs to enhance HP as a part of their activities (Supplemental Appendix 2, available in the online version of this article; Kokko, 2014a). Each facilitator and barrier (both explicitly mentioned as one and interpreted as one) identified represented a meaning unit, which was classified within a statement (Supplemental Appendix 2), and used to reformulate the previously generated guidelines for best practice in sports clubs. As an example of the coding process, the quote “communicating the roles and responsibilities of all groups involved in the program was important for ensuring partnership programs were implemented” (Casey, Payne, Brown, & Eime, 2009; p. 138) was categorized together with other contributing meaning units into Statement 7: “Collaborate with other clubs” (Kokko, 2014a) and then modified to become “Collaborate with other agencies (clubs, health agencies and practitioners), by a building common culture (trust, recognition, shared time) and a process for collaboration (clear roles, shared experiences, contract specification, evaluation of results, power balance between partners).”
Results
Descriptive Analysis
Overall, a total of 58 studies were included in this literature review (Figure 1 and Supplemental Appendix 1). Almost half of the articles were based in Australia, followed by England, the United States, and Canada (Table 1). Only two multicountry articles were found, comparing countries in Europe. Publication dates started in 1995 and proceeded thereafter with two articles before 2000, 32 between 2011 and 2015, and 9 in 2016 and the beginning of 2017 (Table 1). The most common sport settings studied were soccer and rugby or its regional variation. The target group for the intervention was principally sport participants (n = 24 studies) without specifying target group or age. The most targeted behaviors were alcohol (n = 10 studies) and increasing physical activity or sport participation for health benefits (n = 9 studies; Table 1).
Descriptive Information About Included Studies.

Application of the Settings-Based Approach
The reviewed studies included 33 unique interventions, with one being cited five times (the Good sports program, cf. Rowland, Allen, & Toumbourou, 2012a) and two others twice (Healthway, cf. Giles-Corti et al., 2001 and Community Sport Program, cf. Marlier, Cardon, De Bourdeaudhuij, & Willem, 2014). The interventions were mostly delivered at an intrapersonal level (n = 29 studies) followed by institutional, interpersonal, community, and policy-based programs. Some interventions acted on more than one level (Bruun et al., 2014; Geidne, Quennerstedt, & Eriksson, 2013a). Two of the studies (Lane, Murphy, Donohoe, & Regan, 2017; Reilly et al., 2011) were interventions that included several initiatives on all levels (Table 2).
Intervention Characteristics.
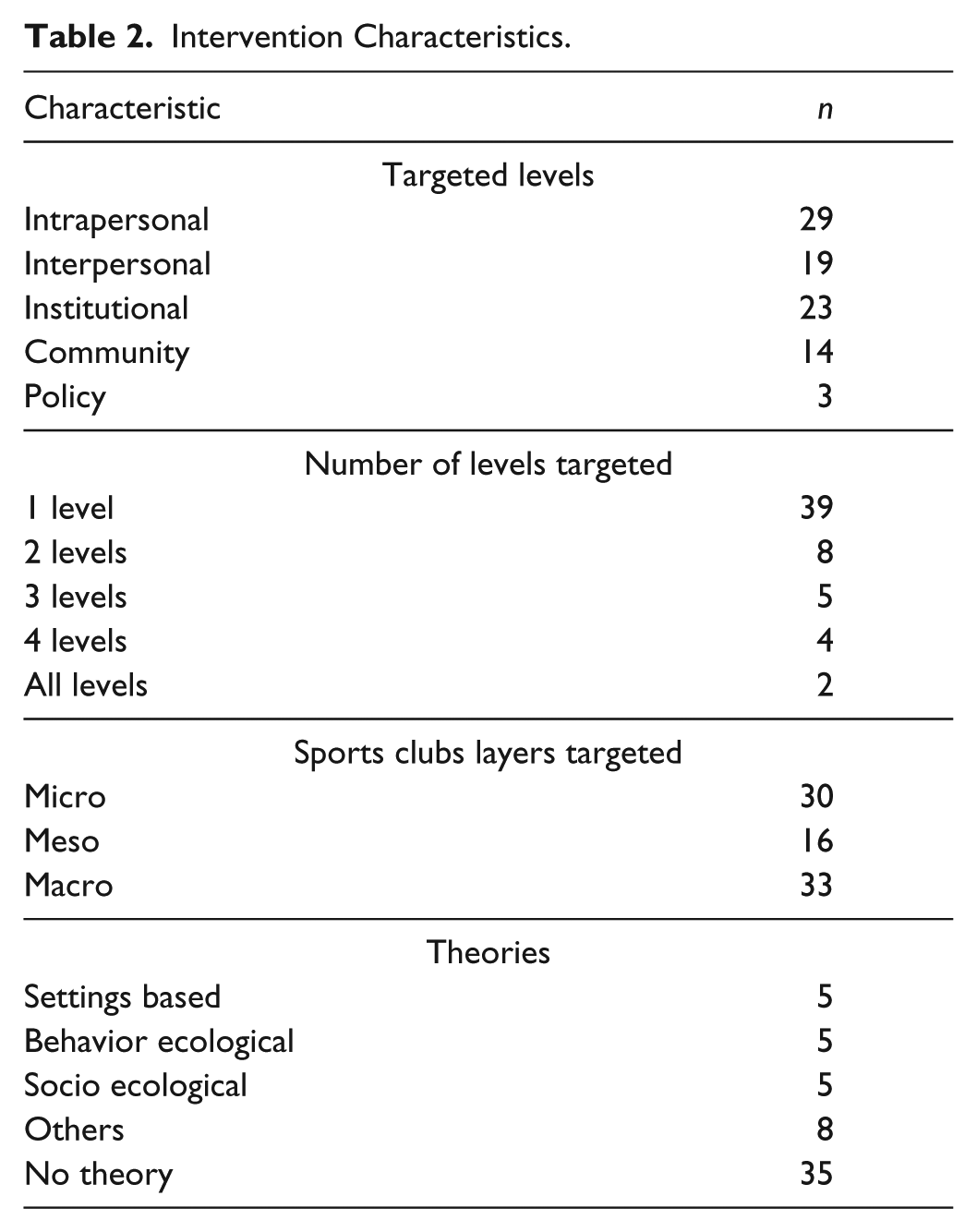
The interventions on the intrapersonal level often consisted of increasing participation in a particular sport together with some sort of health education for the players involved (McConkey, Dowling, Hassan, & Menke, 2013; Tighe & McKay, 2012). The interpersonal interventions included health education for coaches, parents, or families (Gianotti, Hume, & Tunstall, 2010; Larsen et al., 2015), while institutional approaches targeted club officials or staff through, for example, training for policy implementation for responsible alcohol serving practices (Rowland, Allen, & Toumbourou, 2012b) and organizational change strategies (Crisp & Swerissen, 2003).
Interventions that had a community-level component focused, for example, on implementing cross-sector partnerships, capacity-building strategies, and awareness campaigns (Marlier et al., 2014; Misener & Misener, 2016). The only explicitly policy-focused intervention was a system-wide HP program directed at state sporting organizations (Casey, Harvey, Eime, & Payne, 2012). The majority of the studies reported interventions on a single layer, principally the macro- and microelements of the sports club (n = 42 studies; Table 2). More than half (n = 35 studies) of the included studies did not use a specific theory- or model-based intervention. The most common theories used were the settings-based approach, socio-ecological model, and behavioral ecological theory (Table 2).
Study Design and Method
In the reviewed studies, eight were controlled pre- and posttrials (with five randomized), nine were pre- and poststudies (one of them qualitative), and 41 were cross-sectional and included process evaluations, quantitative and qualitative studies, and case studies (Supplemental Appendix 1). The outcomes of the interventions were measured principally through qualitative data collection methods (n = 21 studies). Seventeen studies used unvalidated questionnaires or surveys, and a further eight used validated self-reported measures of health (e.g., self-esteem, quality of life, physical activity). Only two studies (Casey et al., 2012; Lane et al., 2017) used validated measures of HP (HP-SAT and HPSC-index). Seven studies principally collected data on the implementation process, and three gathered objective measurements of behavior (e.g., rate of alcohol in blood, birth rate).
Facilitators and Barriers
The reformulated statements, based on the content of the meaning units in the included studies, are presented in Figure 2 (for details: Supplemental Appendix 2). Statement 1 covered the sports clubs’ will to practice HP in their clubs. Our results have shown that “will” can be described as sports clubs and personal previous experiences and endorsement, organizational readiness, and rationale. Statement 2 described the importance of writing down the aims in a “language of sport.” Our empirical data clarified this last concept, defining it as having a positive message (stemming from positive psychology and a salutogenic approach), but also taking the culture of the club and social inequalities into account. Prioritizing the most relevant HP aims, as Statement 3 entails, had to be done strategically, such as using the socioecological model and relating to the sports clubs’ identity. The financial and human resources of a sports club, targeted in Statement 4, can be quite diverse between organizations. Financial resources can be both subsidiary as well as sponsorship, and the human resources often consist of both paid and volunteer staff often with substantial turnover. Statement 5 focused on the importance of role models and was modified as empirical work describing the importance of time allotment and being recognized as a leader of the development process. Statement 6 was reformulated to include processes by which to engage all of the club officials. Here, a bottom-up approach focusing on trust and shared interests was added from the included studies. Statement 7, regarding collaboration with other clubs, has been extended to include collaboration with related external partners, clarifying the complex process of collaboration, by adopting clear roles and a power balance. The importance of taking costs, time, and also enjoyment into account when evaluating the feasibility of HP aims has been added to Statement 8. Creating a clear implementation plan has been described in more depth, identifying key indicators of this process (e.g., target population, funding mechanism, core objectives) in Statement 9. To communicate the intervention internally (Statement 10) can be helped if the message is clear, explicit, and inclusive as well as visible to both internal and external actors. Strategies to motivate the coaches regarding the importance of HP (Statement 11) have been added, such as fostering interpersonal relationships, autonomy, sense of ownership, and career opportunities. Also, the criteria describing coach education, such as varying support and strategies, using a participatory approach, and focusing on specificity of the public coached have been included in Statement 12. Monitoring (Statement 13) and evaluation (Statement 14) have to be integrated into daily practice, valuing a small-win philosophy and long-term vision, in order to refine future planning.
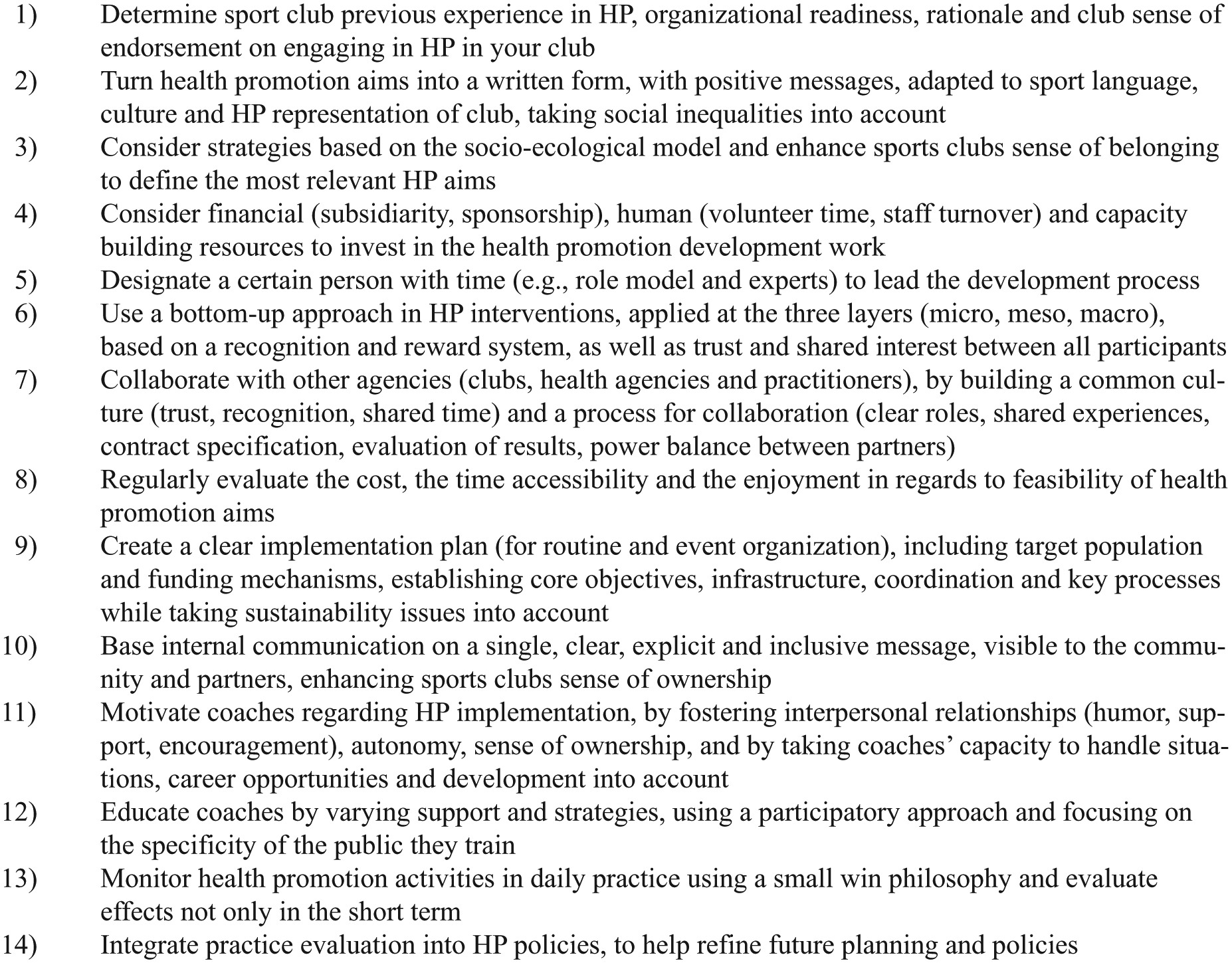
Reformulation of Kokko’s (2014a) guidelines for health promotion (HP) in sports clubs.
Discussion
The present systematic mapping review analyzed how the settings-based approach is applied through HP interventions within sport clubs and mapped facilitators and barriers for sports clubs to become health-promoting settings (Kokko, 2014b).
The analysis of 58 studies has revealed several gaps in the literature. First, the majority of the research reviewed is based in Australia and Europe, with only two multicountry studies. Such results limit an understanding how cultures and sport systems affect sports clubs as health-promoting settings in other parts of the world. Secondly, nearly 60% of the interventions were targeted toward males in team sport settings (rugby, soccer, multiple team sports). As the relationship between sport participation and health behavior is affected by the type of sport (Moore & Werch, 2005), the image of such team sports conveys Bourdieu’s masculine domination (Brown, 2006). Broadening studies to other population groups is needed to better comprehend the impact of the type of sport practice in order to understand how gender, type of sport, and health interact (Robertson, 2003). Third, interventions in almost half of the studies did not differentiate between specific target groups, but targeted sport participants in general, potentially questioning the specificity of sports and physical activity promotion within sport clubs (Geidne & Jerlinder, 2016) and subsequently if sports clubs are recognized as a context for the promotion of adapted physical activity or sports-for-all. Fourth, most of the interventions focused on a single health behavior, in one layer of the sports club and mostly on intrapersonal level rather than adopting a whole setting approach to HP, which could lead to lack of change in the structure and ethos of sport clubs. Fifth, two thirds of the studies were descriptive, and the majority did not use validated measurements, confirming the lack of controlled designs noted in previous literature reviews (Priest et al., 2008a, 2008b) and the challenges associated with conducting randomized controlled trials in sports clubs, due to the tendency for HP interventions to be implemented by actors and not researchers (Baxter, Killoran, Kelly, & Goyder, 2010). It must also be noted that there is a paucity of validated HP measurement tools within sports clubs, with only two validated scales at the macrolayer, the HPSC-index (Kokko, Kannas, & Villberg, 2009), and the HP-SAT (Casey, Harvey, Eime, & Payne, 2011). Therefore, most included studies missed the opportunity to fulfill the challenge of capturing health and behavior change as well as the interactive and reinforcing determinants in the community setting that may affect the effectiveness of the intervention (Golden & Earp, 2012). Furthermore, the absence of rigorous evaluation limits the assessment of effectiveness and may result in interventions with possible negative outcomes being used (Beckman, Svensson, Geidne, & Eriksson, 2017; Liddle, Deane, & Vella, 2017).The lack of evaluation of the implementation process could hinder the identification of facilitators and barriers, as well as understanding how interventions fit in the sports club setting with regard to contextual factors and transferability (Green & Kreuter, 2005).
The application of the settings-based approach in sports clubs is at an early stage. Due to complexity, for example, several levels, of the settings-based approach, it has been previously noted that many HP initiatives work separately or with limited focus, rather than with comprehensive aims and means (Whitelaw et al., 2001). Similar conclusions can be drawn by this present work, as interventions were mostly implemented at one level (intrapersonal), on one layer, and the empirical use of the settings-based approach was not well implemented. The challenge of becoming a health-promoting sports club is a long-term achievement, where HP interventions can be the first steps to achieve a whole setting approach. Efforts are needed to improve practitioners’ confidence in sports clubs as health-promoting settings (Poland, Green, & Rootman, 1999; Van Hoye, Sarrazin, Heuzé, & Kokko, 2015), for example, how to make separate HP initiatives a part of a settings-based approach (Whitelaw et al., 2001). Geidne (2012) argues that HP in settings can be thought of as an early stage of the development of a health-promoting setting, considering a small win philosophy, where “one small win may seem unimportant, but a series of small wins reveals a pattern that may attract allies, deter opponents, and lower resistance to subsequent proposals” (Corti, Holman, Donovan, Frizzell, & Carroll, 1995, p. 194)
As mentioned, the interventions included were mostly implemented at the intrapersonal level, targeting sport participants directly. A previous literature review on health interventions has shown that interventions focusing on structural changes and provision of resources reduced health inequalities, whereas interventions focused on intrapersonal factors were less effective in taking social inequalities into account (Lorenc, Petticrew, Welch, & Tugwell, 2013). Moreover, nearly three quarters of the interventions targeted only one layer, where evidence has shown that multilayer interventions are more effective (Jackson et al., 2006). In other settings, like schools, at least two levels have been targeted (Richard, Gauvin, & Raine, 2011), but this is evidently not the case in sports clubs. The focus on the intrapersonal level slows down the understanding about the interactions between interconnected individual and contextual factors (Golden & Earp, 2012) and prohibits the implementation of a settings-based approach in sports clubs (Kokko, 2014b). Despite this, interventions focusing on more than three levels have all been conducted since 2011 (cf. Bruun et al., 2014; Geidne et al., 2013a; Lane et al., 2017). In addition, the overall number of published articles has increased, showing progression in the development of a thorough settings-based approach in sports clubs.
In reality, this approach is recent within sport clubs (Kokko, 2014b); thus, the empirical application and understanding in intervention implementation is lacking. Considering that sports clubs are settings principally based on volunteer work with a core business centered on sports, (Kokko, Kannas, Villberg, & Ormshaw, 2011) the feasibility of a settings-based approach at each level and layer is currently limited. This issue is further compounded by the fact that sports clubs lack the criteria to evaluate what is needed for them to become health-promoting settings. The reformulated guidelines of this study add some clarity in sections such as relevant tools, methods, and actors that can be used in the sports clubs setting. This is important because all sports clubs begin from their unique starting point and the guidelines will be relevant to the sports clubs if they can identify with them.
Theoretically based guidelines have been published to help support the implementation of the settings-based approach within sports clubs (Kokko, 2014b). The present review has added practical examples of strategies that have worked in previous HP interventions, which helped give more context to the guidelines and a better understanding about the fit of HP interventions into sports settings (Green & Kreuter, 2005), even taking diversity into account. The aim for all sports clubs may not be to fulfill the guidelines in total but to strive for them in a way that makes sense for each particular organization. This can help sports clubs develop beyond implementing separate HP initiatives to evolve into a health-promoting setting. The challenges associated with the volunteer intensive nature of community sport and the context, structure, and organization of local-level sport and clubs (Kokko et al., 2016) force sports clubs to start from different levels and with different ambitions. Or, as Kokko and colleagues (2016) stated, “the current status of HPSC development and research shows a transition from a generic HP in settings approach to a more specific to sports club-based HP—via settings-based HP” (p. 82).
There are also some limitations to this study that should be mentioned. First, sports-based interventions/sport-for-development program, as well as physical activity programs, were not included, because these were initiatives implemented outside the sports clubs setting. However, these types of programs could be used, by communities in cooperation with sports clubs, as a “hook” to get people involved in sports club activities. Second, the review did not measure the effectiveness of interventions, as this work is currently being carried out in a Cochrane review. Third, searching for literature in this field made us realize the overlap between HP and sports management literature, where interventions regarding, for example, organizational change could have similar content and outcomes, but be described with different language and with different frameworks and theories framing them. This could have resulted in us missing some interventions concerning, for example, democracy or integration, because they were not framed within HP. Related to this is that bottom-up initiatives are less researched than externally driven interventions (Geidne & Jerlinder, 2016). Fourth, in this study we were not able to use the determinants of sports clubs (Kokko et al., 2014), due to a difficulty of identifying how they were defined. Future work is needed to conceptualize the settings-based approach in a more testable framework in order to support and identify the key ingredients of sports clubs as health-promoting settings. Finally, using guidelines developed in a Nordic country for an international sample of studies could be a limitation, but considering that the content was supported by a majority of Australian studies and also studies from other European countries made it a strength.
Conclusion
The present systematic mapping review analyzed how the settings-based approach is applied through HP interventions within sports clubs and identified key facilitators and barriers for successful implementation of the settings-based approach in sports clubs.
The results identified several gaps: (a) most research represents Australian and European cultures and sport systems, (b) interventions were principally tested on males in team sports, (c) most studies focused on sports participants with limited engagement with specific population groups, (d) interventions focused on a single behavior rather than global HP, and (e) study designs were principally descriptive and lacked validated measurements. Future research should seek more diversity in terms of a wider geographical reach, type of sport, and participants targeted, but also a more comprehensive approach toward HP, as well as more rigorous evaluation methods. As in other settings, sports clubs implement HP initiatives, but they do not yet use a settings-based approach to HP. As stated previously (Kokko, 2014b), the process is at an early stage and actors need to build on a small win philosophy to develop a long-term vision. The revised guidelines could help sports clubs with implementation and testing of the settings-based approach to HP.
Supplemental Material
HEB831749_Supplemental_Appendix_1 – Supplemental material for Health Promotion Interventions in Sports Clubs: Can We Talk About a Setting-Based Approach? A Systematic Mapping Review
Supplemental material, HEB831749_Supplemental_Appendix_1 for Health Promotion Interventions in Sports Clubs: Can We Talk About a Setting-Based Approach? A Systematic Mapping Review by Susanna Geidne, Sami Kokko, Aoife Lane, Linda Ooms, Anne Vuillemin, Jan Seghers, Pasi Koski, Michal Kudlacek, Stacey Johnson and Aurélie Van Hoye in Health Education & Behavior
Supplemental Material
HEB831749_Supplemental_Appendix_2 – Supplemental material for Health Promotion Interventions in Sports Clubs: Can We Talk About a Setting-Based Approach? A Systematic Mapping Review
Supplemental material, HEB831749_Supplemental_Appendix_2 for Health Promotion Interventions in Sports Clubs: Can We Talk About a Setting-Based Approach? A Systematic Mapping Review by Susanna Geidne, Sami Kokko, Aoife Lane, Linda Ooms, Anne Vuillemin, Jan Seghers, Pasi Koski, Michal Kudlacek, Stacey Johnson and Aurélie Van Hoye in Health Education & Behavior
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Frö program, Institut Français de Suède.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.