
Abstract
Background. The gateway behavior hypothesis posits that change in a health behavior targeted for modification may promote positive changes in other untargeted health behaviors; however, previous studies have shown inconsistent results. Aims. To examine the patterns and predictors of change in untargeted health behaviors in a large health behavior change trial. Method. Using repeated-measures latent class analysis, this study explored patterns of change in untargeted physical activity, alcohol consumption, and smoking behavior during the first year of the Women’s Health Initiative dietary modification trial that targeted total fat reduction to 20% kcal and targeted increased fruit and vegetable intake. Participants were healthy postmenopausal women who were randomly assigned to either the low-fat dietary change intervention (n = 8,193) or a control (n = 12,187) arm. Results. Although there were increases in untargeted physical activity and decreases in alcohol consumption and smoking in the first year, these changes were not consistently associated with study arm. Moreover, although the results of the repeated-measures latent class analysis identified three unique subgroups of participants with similar patterns of untargeted health behaviors, none of the subgroups showed substantial change in the probability of engagement in any of the behaviors over 1 year, and the study arms had nearly identical latent class solutions. Discussion and Conclusion. These findings suggest that the dietary intervention did not act as a gateway behavior for change in the untargeted behaviors and that researchers interested in changing multiple health behaviors may need to deliberately target additional behaviors.
Behavioral risk factors, including tobacco use, alcohol consumption, physical inactivity, and unhealthy diet, account for approximately a third of cancer deaths worldwide (World Health Organization [WHO], 2015a) and are leading causes of premature death in the United States (Behrens et al., 2013). Moreover, these behavioral risk factors cluster together (Chou, 2008; Lee et al., 2012; Poortinga, 2007), and most adults report engaging in multiple health-risk behaviors (Fine, Philogene, Gramling, Coups, & Sinha, 2004; Loprinzi, Branscum, Hanks, & Smit, 2016; Reeves & Rafferty, 2005). For example, only 2.7% of U.S. adults are sufficiently active, eat a healthy diet, are nonsmokers, and have a recommended body fat percentage (Loprinzi et al., 2016). Multiple health behavior change (MHBC) interventions, which target at least two health-related behaviors either simultaneously or sequentially (Prochaska, Prochaska, & Prochaska, 2013), can be used to efficiently change multiple behaviors and reduce the time and expense of interventions (Nigg, Allegrante, & Ory, 2002; Prochaska, Nigg, Spring, Velicer, & Prochaska, 2010; Prochaska, Spring, & Nigg, 2008). Although MHBC interventions have shown some success (King et al., 2015; Prochaska & Prochaska, 2011; Spring, King, Pagoto, Van Horn, & Fisher, 2015), much is still not well understood about their mechanisms of change (Klein et al., 2017). For example, there is conflicting evidence regarding whether the effects of behavior change interventions spill over to behaviors that are not targeted by the intervention (Mata et al., 2009; Spring et al., 2012). Spillover has implications for MHBC intervention design. Specifically, examination of untargeted change can inform whether interventions aiming to foster changes in multiple domains need to target each behavior, or can effectively target just one behavior, due to the positive cascading effects of the intervention on untargeted behaviors (Nigg et al., 1999; Wilson et al., 2015).
Studies examining whether involvement in an intervention targeting a single health behavior is associated with changes in other behaviors have provided some evidence of spillover (Berg et al., 2012; Dutton, Napolitano, Whiteley, & Marcus, 2008; Fleig, Lippke, Pomp, & Schwarzer, 2011; Halliday et al., 2014; Halliday et al., 2017; Prochaska & Sallis, 2004; Rhew et al., 2007; Weinstock, Petry, Pescatello, & Henderson, 2016; Wilcox, King, Castro, & Bortz, 2000). An advantage of this approach is that it permits the examination of potential gateway behaviors, or health behaviors that, when intervened upon, influence positive changes in other untargeted health-related behaviors (Clark et al., 2005; Emmons, Marcus, Linnan, Rossi, & Abrams, 1994; Nigg et al., 1999; Nigg, Lee, Hubbard, & Min-Sun, 2009). Most of the experimental evidence on the gateway behavior hypothesis is derived from physical activity interventions examining untargeted dietary change, with mixed results of spillover (Dutton et al., 2008; Fleig et al., 2011; Halliday et al., 2014; Halliday et al., 2017; Prochaska & Sallis, 2004; Rhew et al., 2007; Wilcox et al., 2000). Diet has also been proposed as a gateway behavior (Emmons et al., 1994; Wilcox et al., 2000), although few studies have actually examined the diet gateway hypothesis (Foster-Schubert et al., 2012; Johannessen, Oettingen, & Mayer, 2012). In one example, 2 weeks following a diet intervention among undergraduate dieters, participants reported being more physically active in the previous 2 weeks than they were normally, suggesting diet intervention spillover (Johannessen et al., 2012). Although evidence of spillover is equivocal, examining single health behavior interventions for spillover remains relevant because of the potential to reduce time, cost, resource, and participant burden of interventions, relative to multiple health behavior interventions (Halliday et al., 2017; Prochaska & Sallis, 2004).
The lack of consistent support for the gateway behavior hypothesis may be due in part to combining participants with distinct patterns of untargeted behavior change. Examining interindividual variability in behavior change may provide a richer picture by revealing subgroups of participants who show similar patterns of change in untargeted health behaviors. Additionally, sociodemographic, medical history, and psychosocial variables may predict different patterns of change. Determining the predictors of untargeted behavior change can inform future interventions regarding subgroups that are especially inclined toward certain behavior change patterns.
The purpose of the current study was to investigate patterns and predictors of change in untargeted health behaviors in the first year of a large dietary change intervention, the Women’s Health Initiative (WHI) dietary modification (DM) trial, and, more specifically, to examine whether women assigned to the DM intervention had positive spillover in untargeted behaviors compared with those assigned to the control arm. The untargeted behaviors of interest were lack of physical activity, heavy drinking, and cigarette smoking, which, along with unhealthy diet, are referred to as the “big four” behaviors relevant to health outcomes (Pronk, Peek, & Goldstein, 2004). We used adherence to behavioral recommendations from national organizations to evaluate whether change occurred over the year and to identify distinct subgroups of participants with different patterns of engagement in untargeted health behaviors. Based on the gateway behavior hypothesis, we hypothesized that the intervention arm would have different subgroups of change in untargeted behaviors compared with the control arm, with some subgroups showing improvement in untargeted health behaviors. We also examined whether sociodemographic, medical history, and psychosocial variables were related to membership in the subgroups of women with similar patterns of untargeted behavior change.
Method
Study Population
The WHI was a 15-year National Institutes of Health–funded epidemiological study examining the health of postmenopausal women in 40 clinical centers across the United States (Matthews et al., 1997; WHI, 1998). There were three clinical trials (DM, hormone replacement therapy, and calcium and vitamin D) and an observational study. Postmenopausal women aged 50 to 79 years old (N = 48,835) were recruited for the WHI DM trial beginning in 1993 and were followed an average of 8.1 years, with the trial ending in 2005 (Ritenbaugh et al., 2003). Eligibility criteria also included consuming greater than 32% energy from fat (see Figure 1 for participant flow). The DM trial was designed to test the primary hypotheses that a low-fat diet reduces the risks of breast cancer and colorectal cancer. Whether this intervention would likewise reduce the risk of cardiovascular disease was a secondary hypothesis. In brief, at baseline, women were randomly assigned to the dietary change intervention arm (n = 19,541) or a control arm (n = 29,294). In the first year, women in the intervention arm received an intensive small group-based intervention aimed at reducing total dietary fat intake to 20% of daily energy, and increasing fruit and vegetables to five servings per day and grains to six servings per day. The intervention, however, did not encourage weight loss or calorie reduction, and women were told during the signing of the consent forms that this was not a weight loss study. In addition, the intervention did not provide smoking cessation or physical activity guidance (Howard, Manson, et al., 2006; Tinker et al., 1996). Subsequent years focused on maintaining dietary changes. Details of the DM trial recruitment methods, eligibility, and design are reported elsewhere (J. Hays et al., 2003; Tinker et al., 1996). In general, the primary and secondary hypotheses of the WHI DM trial were not supported over the follow-up period. Specifically, the treatment arm did not show statistically significant reductions in the risk of invasive breast cancer (Prentice et al., 2006), colorectal cancer (Beresford et al., 2006), or cardiovascular disease (Howard, Van Horn, et al., 2006). All 40 participating clinical centers and the clinical coordinating center at the Fred Hutchinson Cancer Research Center received institutional review board approval for the WHI, and all women provided informed consent (Tinker et al., 2007).

Flowchart of participants through the study.
Measures
Dietary Intake
Dietary information was collected with the Food Frequency Questionnaire (Tinker et al., 1996). All DM participants completed the Food Frequency Questionnaire at baseline and Year 1. Participants were asked about the types and amounts of foods consumed in the previous 3 months. In the current study, the change in daily percent energy from fat, number of fruit and vegetable servings, and number of grains servings were used.
Untargeted Behaviors
For the purpose of this analysis, adherence was dichotomized according to behavioral guidelines for each untargeted health behavior: 500 or more metabolic equivalent (MET)–minutes per week of moderate to vigorous physical activity (MVPA) (Garber et al., 2011; Kushi et al., 2012; U.S. Department of Health and Human Services [HHS], 2008), seven or fewer drinks per week (U.S. Department of Agriculture, 2015), and not smoking.
Participants answered questions regarding the frequency, length, and intensity of walking, moderate exercise, and vigorous exercise. Moderate and vigorous physical activity were combined to assess adherence to MVPA guidelines, which suggest 500 or more MET-minutes per week of MVPA (≥4.0 METS) (Garber et al., 2011; HHS, 2008; Kushi et al., 2012). Women were asked to record the frequency and amount of their consumption of medium servings of beer, wine, and liquor, which provided information about the average number of drinks per week. Participants were asked whether they currently smoked cigarettes.
Additional Predictors of Untargeted Behavior Change
Baseline sociodemographic characteristics included age, U.S. region, race/ethnicity, education, family income, marital status, and employment status. Medical history variables included body mass index (kg/m2) (World Health Organization, 2015b) and self-reported history of chronic disease (including any of the following: diabetes, high cholesterol, hypertension, cardiovascular disease, or cancer). Physical functioning was measured using the 10-item Physical Functioning subscale from the RAND 36-Item Health Survey (R. D. Hays, Sherbourne, & Mazel, 1993). Social support was assessed using nine items from the Medical Outcomes Study questionnaire (Sherbourne & Stewart, 1991). Social strain was evaluated using four items from a measure about the negative aspects of social relationships (Antonucci, Kahn, & Akiyama, 1989). Due to the skewed nature of the data, quartiles of physical functioning, social support, and social strain were used. A modified six-item version of the Center for Epidemiologic Studies–Depression Scale was used to assess depressive symptoms (Radloff, 1977). A cutoff score of 5 or more, which corresponds to the cutoff score of 16 on the full 20-item Center for Epidemiologic Studies–Depression Scale, was used to indicate current depression (Uebelacker et al., 2013; Wassertheil-Smoller et al., 2004; Wilcox et al., 2003).
Statistical Analyses
Only participants who had complete data for all study variables were included in the present analysis (see Figure 1). The final sample consisted of 20,380 participants, with 8,193 intervention and 12,187 control participants.
Descriptive statistics, including means and standard deviations for continuous variables and proportions for categorical variables, were calculated for the baseline sociodemographic, medical history, and psychosocial variables, and the untargeted health behaviors at baseline and Year 1. Study arm differences in guideline adherence were examined using chi-square tests. To verify that there were group differences in the targeted dietary variables, study arm differences were examined using independent samples t-tests for each dietary variable at baseline and Year 1.
We used repeated-measures latent class analysis (RMLCA) to identify subgroups in the overall sample and study arms. That is, RMLCA was used to determine the number of classes necessary to explain the variation in untargeted health behaviors between baseline and Year 1 (Lanza & Collins, 2006). The latent classes in RMLCA are defined by individuals’ adherence to each behavioral guideline across time, and individuals with similar patterns will be members of the same latent class (McCarthy, Ebssa, Witkiewitz, & Shiffman, 2015). Adherence to guidelines for each untargeted behavior was coded 1 = adherent to guidelines and 2 = nonadherent to guidelines. Models were estimated using PROC LCA, Version 1.3.2 (Lanza, Dziak, Huang, Wagner, & Collins, 2015) in SAS 9.4 (SAS Institute Inc., Cary, NC).
Latent class models in the full sample were used to select the optimal number of latent classes (Collins & Lanza, 2010; Lanza, Bray, & Collins, 2013): interpretability, the Akaike information criterion (AIC), the Bayesian information criterion (BIC), entropy (a measure of classification certainty), and the likelihood-ratio statistic (G2, a measure of absolute model fit). Item-response probabilities, or the probabilities of observed responses to each behavioral guideline given membership in a particular latent class, were used to assign labels to latent classes. An item–response probability of greater than .5 was used to interpret latent classes that had a high probability of adherence to the behavioral recommendation (Collins & Lanza, 2010; de Vries et al., 2008; Fitzpatrick et al., 2015; Kang et al., 2014).
Next, we examined whether the latent structure differed between the two study arms. First, we examined whether measurement invariance held by comparing a model in which all parameters were allowed to vary across arms and a second in which the item-response probabilities were constrained to be equal across arms (Collins & Lanza, 2010). If the models fit equally well according to the AIC, BIC, and likelihood ratio difference test, this would suggest that the pattern of untargeted behavior change is similar across arms. We also examined whether the number of and interpretation of latent classes was identical across arm by running separate RMLCA models for each.
Predictors of Latent Class Membership
A multinomial logistic regression was used to explore the predictors of class membership. To assign class membership, the posterior probabilities, or the probabilities of latent class membership for participants, conditional on their response patterns, were used (Goodman, 2007).
A p < .01 significance level was used to adjust for the size of the data set increasing the chance of significance and to account for the large number of analyses being conducted.
Results
As can be seen in Table 1, the intervention and control arms had similar baseline characteristics. There were no significant study arm differences in any of the dietary components at baseline (Supplemental Table S1, available in the online version of this article). However, by Year 1, the intervention arm significantly decreased percent energy from fat and increased daily fruit and vegetable and grains servings, relative to the control arm.
Baseline Characteristics by Study Arm and for the Total Sample.
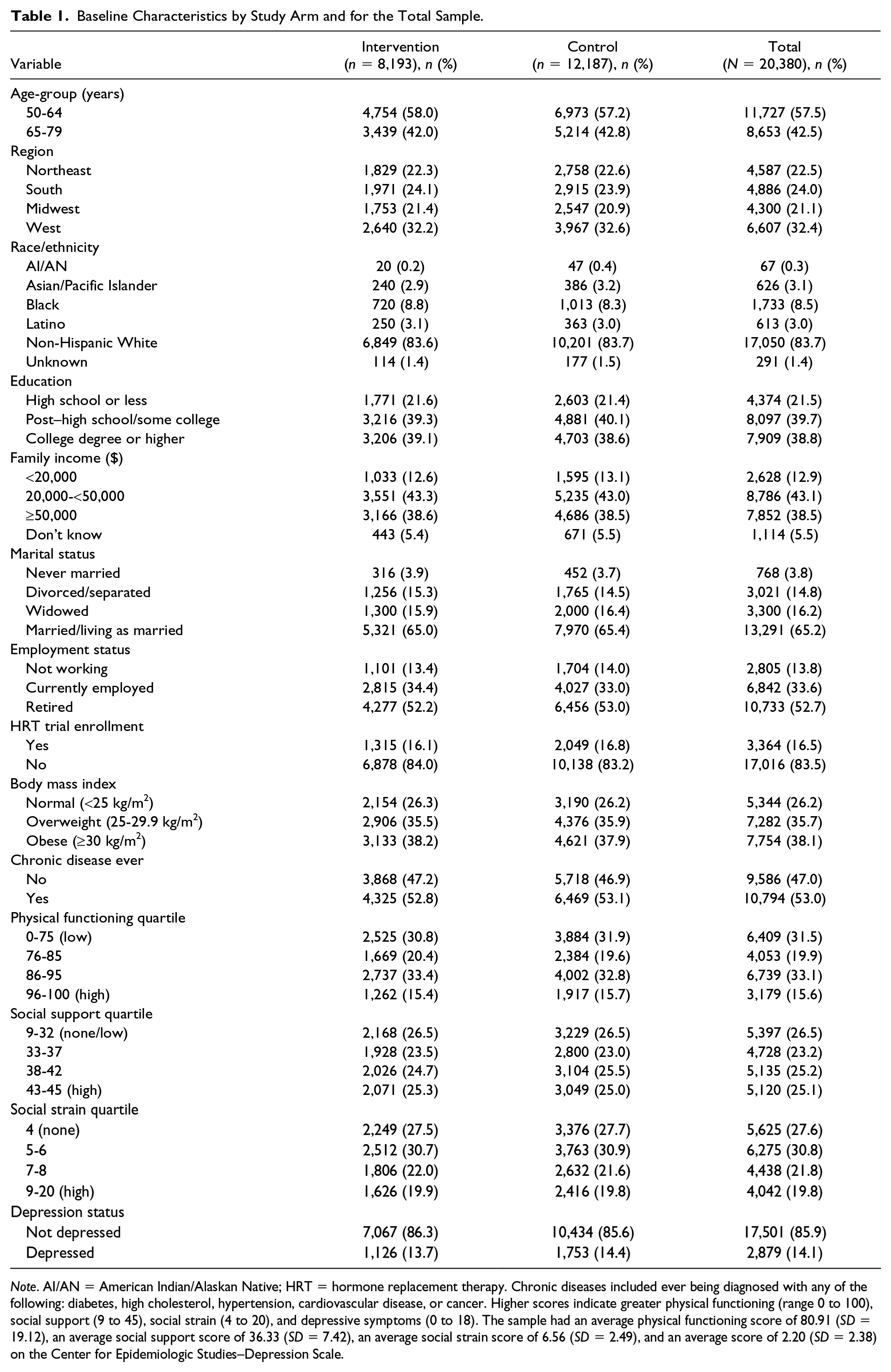
Note. AI/AN = American Indian/Alaskan Native; HRT = hormone replacement therapy. Chronic diseases included ever being diagnosed with any of the following: diabetes, high cholesterol, hypertension, cardiovascular disease, or cancer. Higher scores indicate greater physical functioning (range 0 to 100), social support (9 to 45), social strain (4 to 20), and depressive symptoms (0 to 18). The sample had an average physical functioning score of 80.91 (SD = 19.12), an average social support score of 36.33 (SD = 7.42), an average social strain score of 6.56 (SD = 2.49), and an average score of 2.20 (SD = 2.38) on the Center for Epidemiologic Studies–Depression Scale.
Table 2 shows adherence to guidelines for untargeted behaviors at baseline and Year 1. Women tended to engage in less than the recommended amount of MVPA, drink at most moderately, and be nonsmokers at both time points. The proportion adherent to MVPA guidelines significantly increased in both the intervention (22.0% to 31.5%) and control arm (22.1% to 30.8%), although the difference between arms was not significant. The proportions of heavy drinkers and smokers remained similar between baseline and Year 1 and were not significantly different between the study arms.
Adherence to Behavioral Guidelines for Untargeted Behaviors at Baseline and Year 1.
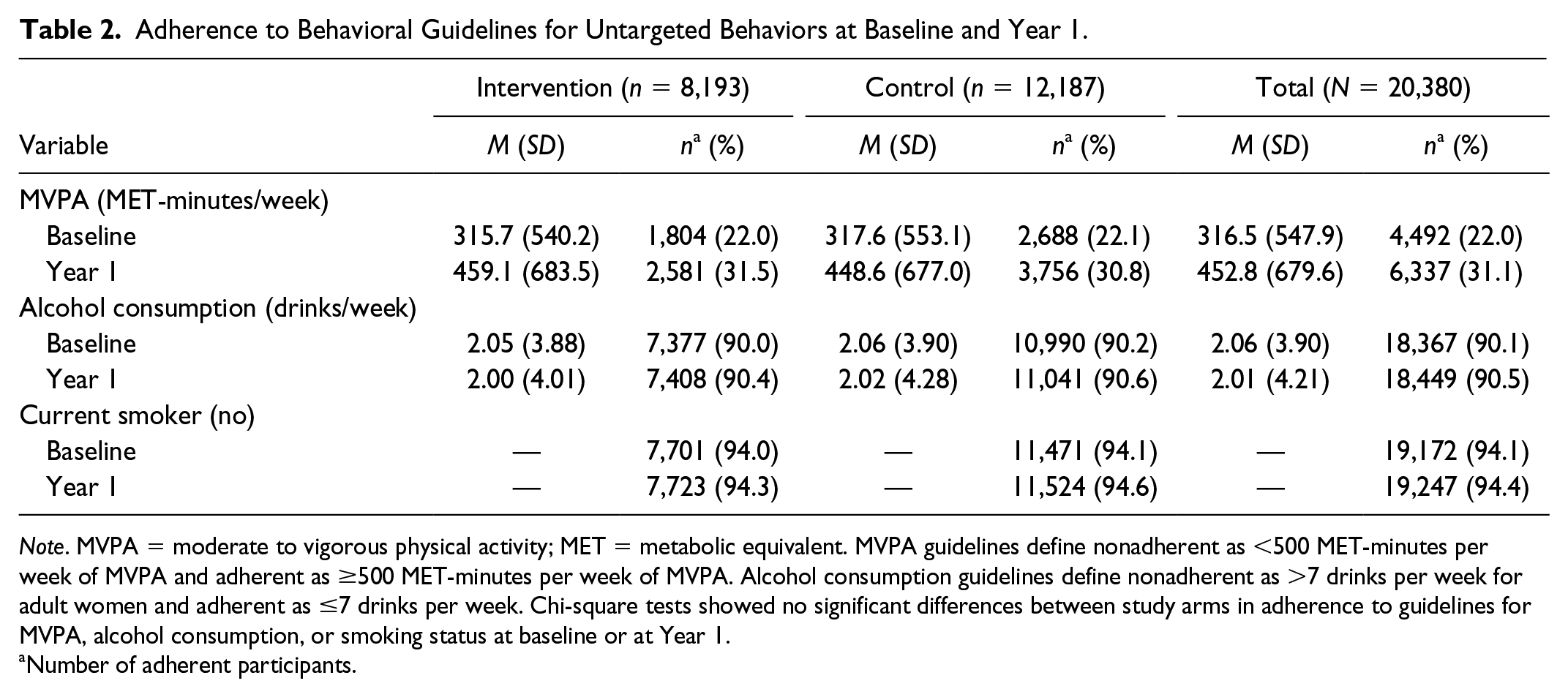
Note. MVPA = moderate to vigorous physical activity; MET = metabolic equivalent. MVPA guidelines define nonadherent as <500 MET-minutes per week of MVPA and adherent as ≥500 MET-minutes per week of MVPA. Alcohol consumption guidelines define nonadherent as >7 drinks per week for adult women and adherent as ≤7 drinks per week. Chi-square tests showed no significant differences between study arms in adherence to guidelines for MVPA, alcohol consumption, or smoking status at baseline or at Year 1.
Number of adherent participants.
Results of the RMLCA
Based on examination of indices of model fit and classification precision, a three-class model was selected for the total sample (Table 3). Table 4 shows the latent class prevalences and item-response probabilities for the total sample’s three-class solution. We labeled the most prevalent class, which was characterized by low probability of adherence to physical activity guidelines and high probability of adherence to alcohol consumption and smoking guidelines, as Low Exercisers (85%). We labeled the class defined by low probability of adherence to physical activity and alcohol consumption guidelines and high probability of nonsmoking as Heavy Drinkers (10%), and the class with high probability of adherence to alcohol consumption guidelines but low probability of adherence to physical activity and smoking guidelines as Current Smokers (5%). As can be seen in Table 4, the item–response probabilities for adherence were very similar within each class between baseline and Year 1, which suggests that, although there were unique subgroups, there was relative stability in adherence status. In addition, all classes had high probability for adherence to at least one guideline. None of the classes had a high item–response probability for adherence to MVPA guidelines, but all classes did show an increase in the probability from baseline to Year 1.
Model Fit Indices for Models With One to Three Classes.
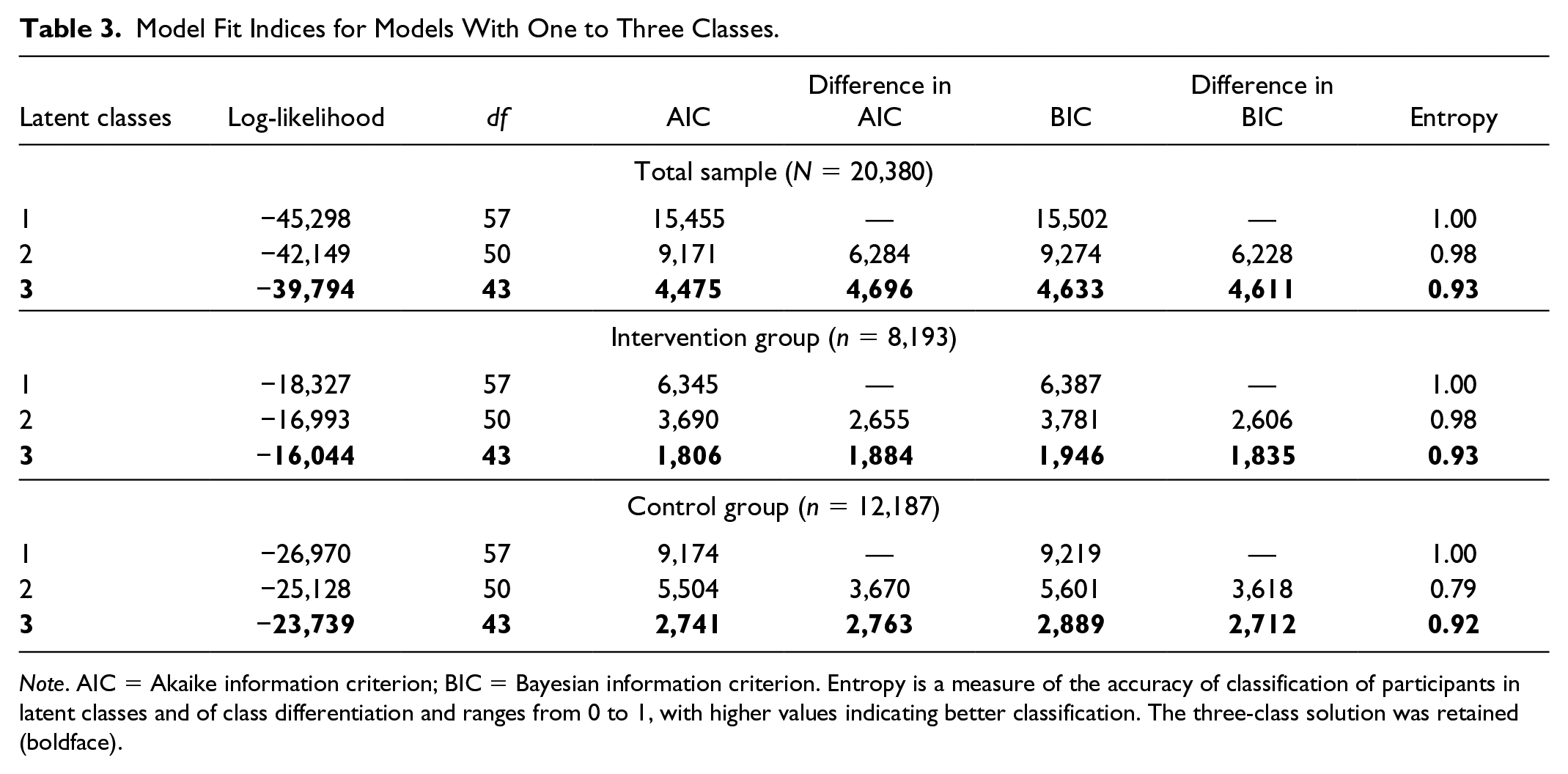
Note. AIC = Akaike information criterion; BIC = Bayesian information criterion. Entropy is a measure of the accuracy of classification of participants in latent classes and of class differentiation and ranges from 0 to 1, with higher values indicating better classification. The three-class solution was retained (boldface).
Latent Class Prevalences and Item–Response Probabilities for Three–Latent Class Models in the Total Sample (N = 20,380), Intervention Group (n = 8,193), and Control Group (n = 12,187).
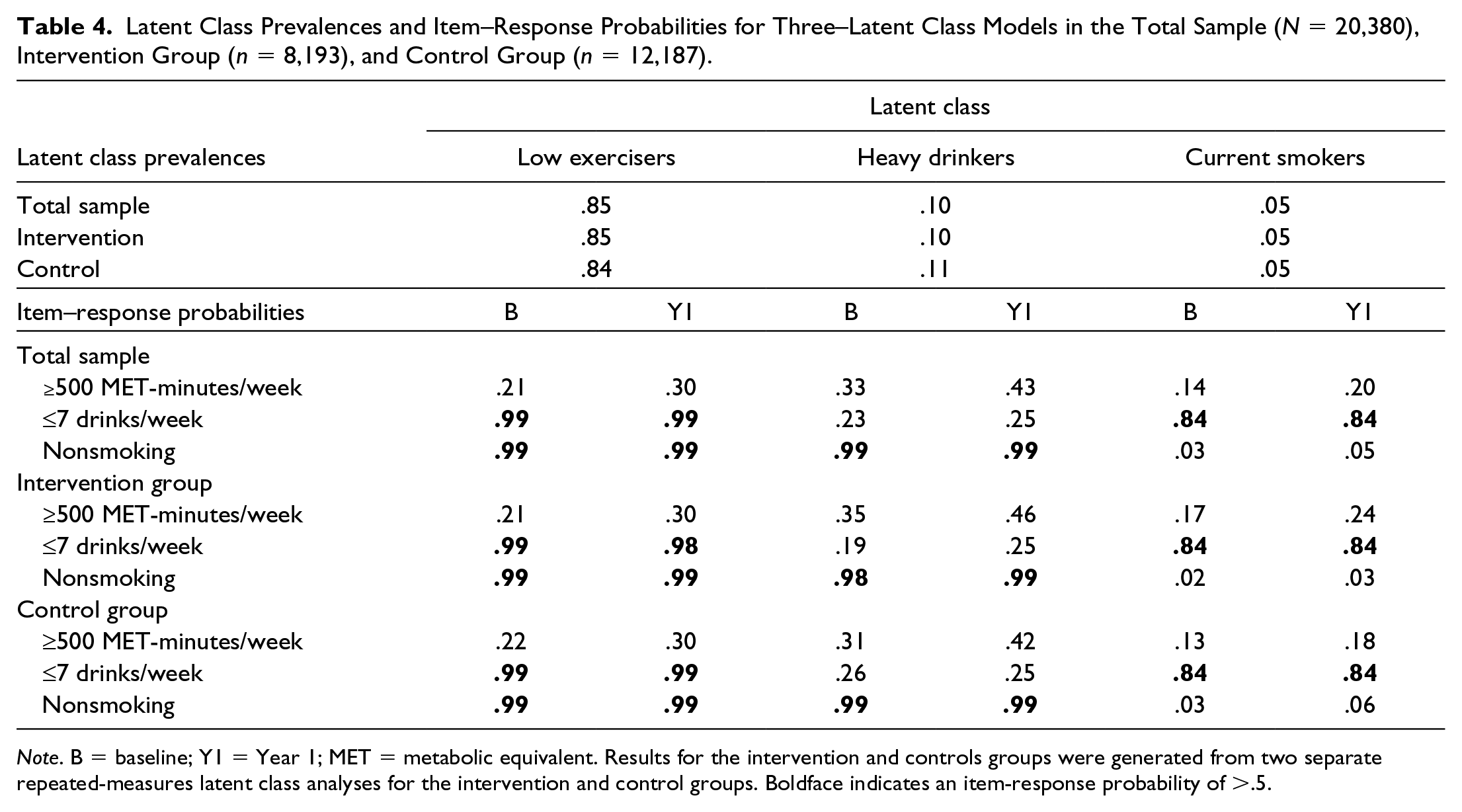
Note. B = baseline; Y1 = Year 1; MET = metabolic equivalent. Results for the intervention and controls groups were generated from two separate repeated-measures latent class analyses for the intervention and control groups. Boldface indicates an item-response probability of >.5.
Study Arm Differences in Latent Classes
The item-response probabilities were not significantly different across the study arms (Supplemental Table S2, available in the online version of this article). Separate models for each study arm were also examined, and a three-class solution was selected (Table 3). The class prevalences and item-response probabilities for the three-latent-class solutions were highly similar across the study arms, and the interpretation of the classes was the same as the model conducted with the entire sample (Table 4). The latent structures were determined to be highly similar. Indeed, the latent class prevalences were the same, within rounding error, for each arm when the item–response probabilities were constrained to be equal across the arms (Supplemental Table S3, available in the online version of this article). Thus, it was concluded that the predictors of latent class membership could be examined with measurement invariance applied in the three-class solution.
Predictors of Latent Class Membership
A multinomial logistic regression analysis was conducted to determine the predictors of class membership with the most prevalent class, Low Exercisers, serving as the reference group (Table 5). Women in the Heavy Drinkers class had greater odds of being 50 to 64 years old, having at least some college education, earning $20,000 or more per year, and having higher physical functioning. In addition, women in the Heavy Drinkers class had significantly lower odds of being from the South or Midwest, being Black, Latino, or in the other race/ethnic groups’ category, or being overweight or obese. Women in the Current Smokers class had significantly greater odds of being Black, being unmarried, not being currently employed, and being enrolled in the HRT trial. Moreover, women in the Current Smokers class had significantly lower odds of being 64 years old or younger, being overweight or obese, having higher physical functioning, having higher social support, and not being depressed.
Predictors of Latent Class Membership.
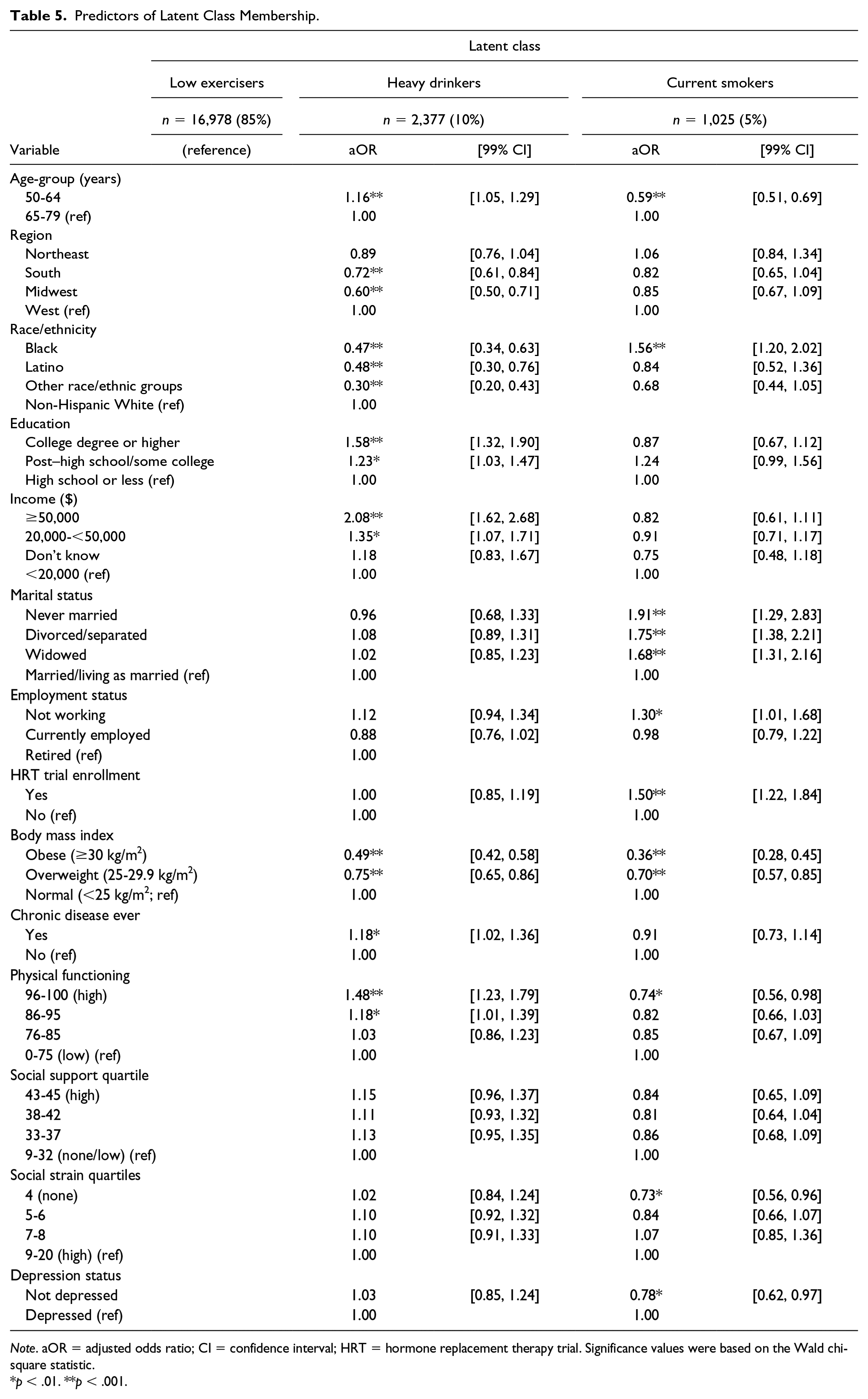
Note. aOR = adjusted odds ratio; CI = confidence interval; HRT = hormone replacement therapy trial. Significance values were based on the Wald chi-square statistic.
p < .01. **p < .001.
Discussion
The current study examined the gateway behavior hypothesis, which suggests that there would be positive changes in untargeted health-related behaviors when a behavior is intervened upon (Nigg et al., 1999; Nigg et al., 2009), in the first year of the WHI dietary modification (DM) trial. In line with previous gateway behavior studies, there was evidence that untargeted behaviors, particularly physical activity, improved over the first year of the study, but assignment to the intervention arm was not predictive of changes. Moreover, although there were distinct subgroups of participants based on their adherence to the guidelines for each untargeted behavior, the probability of adherence changed only slightly from baseline to Year 1, and the study arms had highly similar behavioral subgroups. The findings suggest that improvements in untargeted behaviors may have been a result of simply participating in the trial, rather than of the DM intervention, and support the notion that substantial changes in health behaviors are unlikely to occur without specific targeted intervention on those health behaviors (Paiva et al., 2012).
To our knowledge, the present study is the first to use RMLCA to identify distinct subgroups of participants with different patterns of untargeted health behaviors in response to a single health behavior intervention. Three distinct subgroups were identified: Low Exercisers, (85%), Heavy Drinkers (10%), and Current Smokers (5%). The latent classes had similar probability of adherence to each behavioral guideline at both time points, but there was no evidence of change within any latent class. In addition, the latent class structure was similar for each study arm. As a whole, the results of the RMLCA provide evidence that the intervention did not promote positive changes in untargeted health behaviors.
There were also distinct predictors of class membership in the multivariable analysis. For instance, relative to the Low Exercisers class, women in the Heavy Drinkers class were more likely to have greater family incomes and education. These results may seem counterintuitive at first, but they are consistent with results from other studies that have shown that higher alcohol consumption is associated with factors typically assumed to predict engagement in health-promoting behaviors. For example, studies have shown that women who report heavy drinking (i.e., more than seven drinks per week) are more likely to be more highly educated and have higher incomes (Espeland et al., 2006; Li et al., 2010). It may be that women who are heavy drinkers are able to afford the expense of daily alcohol consumption or that it is a socially acceptable behavior among their peers.
Strengths of the current study include the use of a large prospective sample and use of RMLCA to examine the gateway behavior hypothesis. Limitations include the generalizability of the results to other populations since women in the WHI were healthy volunteers. We also had a relatively small number of smokers and heavy drinkers who may have been more resistant to change and may not represent the general U.S. population. In addition, all health behaviors were self-reported. Smoking and alcohol consumption tend to be underreported and physical activity tends to be overreported when measured by self-report (Newsom, McFarland, Kaplan, Huguet, & Zani, 2005). Future studies could use calibrated measures or more objective measures to help correct for this measurement error. In addition, women in the intervention arm weighed an average of 2.2 kg less at the end of Year 1 relative to the control arm (Howard, Manson, et al., 2006), and it is possible that women in the intervention arm did not engage in more physical activity than the control arm because their dietary change sufficiently achieved weight loss. However, this assumes that women’s motive for engaging in physical activity was weight loss, which was not an aim of the DM trial. Future research could examine motivations for engaging in untargeted behaviors in a single health behavior intervention trial. To be consistent with previous studies examining spillover (Halliday et al., 2017; Rhew et al., 2007; Wilcox et al., 2000), we focused on change in the first year of the intervention, though patterns of untargeted behavior change may differ when examined over a longer time. Finally, due to the timing and frequency of variable measurement, we were unable to examine the timing of change in untargeted behaviors. Ecological momentary assessment, which has been used in observational studies to examine MHBC (Conroy et al., 2015), could be used to establish, with greater precision, changes in untargeted health behaviors as the targeted behavior changes.
The results have the potential to inform practice. As previously described, the gateway behavior hypothesis suggests that when a behavior is targeted, positive spillover effects can be expected in untargeted health behaviors (Nigg et al., 2009). Results showed that there were changes in untargeted health behaviors but that these changes were generally not related to study arm, suggesting that there was not consistent evidence that dietary change acted as a gateway behavior for untargeted physical activity, alcohol consumption, or smoking in the present study. These add to the existing body of gateway behavior studies that suggest that there are few consistent changes in untargeted health behaviors in the context of single health behavior interventions (Dutton et al., 2008; Wilcox et al., 2000). Although there were no uniform positive changes in untargeted health behaviors, there were also no substantial deteriorations in any behavior. This implies that women who changed their dietary behavior were not more likely to experience concurrent decrements in other health behaviors and that, at least in the context of the first year of a dietary modification trial, untargeted health behaviors do not necessarily need to be monitored for deterioration.
In the present study, the untargeted health behaviors were not directly addressed by the intervention, which provided one method of testing the gateway behavior hypothesis. Indeed, the results suggest that, at least for some untargeted behaviors, a dietary modification intervention is not on its own sufficient to change untargeted health behaviors and that, if change in these behaviors is desired, behavior-specific treatment may be necessary. However, a full behavior-specific treatment may not be necessary to promote positive changes in other behaviors. For example, some behavior change principles that could be applied to other health behaviors were taught in the intervention, such as self-monitoring and problem-solving skills (Tinker et al., 1996). Perhaps intervention participants would change their untargeted behaviors if they were taught how to apply these same skills to change other behaviors (Noar, Chabot, & Zimmerman, 2008). The objective of the DM trial was not MHBC, but it is possible that, even with minimal additional intervention, physical activity, alcohol consumption, and smoking may have systematically improved among intervention participants. Determining the minimal intervention required to induce change in multiple health behaviors is an area of MHBC intervention research that has the potential to further reduce participant and resource burden.
Conclusion
The results of the present study suggest that there were improvements in health behaviors that were not targeted by the intervention, particularly physical activity, in the first year of the WHI DM trial. These improvements, however, were not related to the receipt of the DM intervention. Moreover, although there were participants who changed their adherence to behavioral guidelines in the first year of the trial, the vast majority remained the same. Based on the results from this study, future interventions that aim to modify multiple health behaviors, particularly diverse behaviors or ones that are especially difficult to change, should consider the addition of behavior-specific components, rather than relying on behavior-general spillover effects.
Supplemental Material
HEB831756_Supplemental_Material – Supplemental material for Is There a Spillover Effect of Targeted Dietary Change on Untargeted Health Behaviors? Evidence From a Dietary Modification Trial
Supplemental material, HEB831756_Supplemental_Material for Is There a Spillover Effect of Targeted Dietary Change on Untargeted Health Behaviors? Evidence From a Dietary Modification Trial by Elizabeth A. Sarma, Anne Moyer, Catherine R. Messina, Helena H. Laroche, Linda Snetselaar, Linda Van Horn and Dorothy S. Lane in Health Education & Behavior
Footnotes
Acknowledgements
The authors would like to thank the following people: Program Office: Jacques Rossouw, Shari Ludlam, Joan McGowan, Leslie Ford, and Nancy Geller (National Heart, Lung, and Blood Institute, Bethesda, MD). Clinical Coordinating Center: Garnet Anderson, Ross Prentice, Andrea LaCroix, and Charles Kooperberg (Fred Hutchinson Cancer Research Center, Seattle, WA). Investigators and Academic Centers: JoAnn E. Manson (Brigham and Women’s Hospital, Harvard Medical School, Boston, MA); Barbara V. Howard (MedStar Health Research Institute/Howard University, Washington, DC); Marcia L. Stefanick (Stanford Prevention Research Center, Stanford, CA); Rebecca Jackson (The Ohio State University, Columbus, OH); Cynthia A. Thomson (University of Arizona, Tucson/Phoenix, AZ); Jean Wactawski-Wende (University at Buffalo, Buffalo, NY); Marian Limacher (University of Florida, Gainesville/Jacksonville, FL); Jennifer Robinson (University of Iowa, Iowa City/Davenport, IA); Lewis Kuller (University of Pittsburgh, Pittsburgh, PA); Sally Shumaker (Wake Forest University School of Medicine, Winston-Salem, NC); Robert Brunner (University of Nevada, Reno, NV); Karen L. Margolis (University of Minnesota, Minneapolis, MN). Women’s Health Initiative Memory Study: Mark Espeland (Wake Forest University School of Medicine, Winston-Salem, NC). For a list of all the investigators who have contributed to WHI science, please visit: ![]() .
.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The WHI program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through contracts HHSN268201100046C, HHSN268201100001C, HHSN268201100002C, HHSN268201100003C, HHSN268201100004C, and HHSN271201100004C.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.