
Abstract
Background. Despite evidence that social network members influence the eating behaviors of adults, no study to date has had the primary aim of examining children as support partners for parents in a weight loss intervention. Aim. To evaluate parent adherence with eating/exercise goals and weight loss in a 6-month study engaging children as support partners. Method. Adults with obesity (body mass index ≥ 30 kg/m2, n = 102) and at least one child ≥12 years were randomized to a child support or control group. In the child support group, children enrolled with their parent and engaged in a supportive behavior 2 days/week. In the control group, there was no enrolled child support. Parents in both groups selected a healthy eating strategy and daily step goal. Results. There was no difference in weight loss between the child support and control groups (−5.97 vs. −5.42 lbs, p = .81). In the child support group, 30% of children did not engage in the study. The majority of parents whose children did not engage withdrew from the study. In secondary analyses, parent adherence with eating/exercise goals increased with the days of child support (p < .001). For all participants, low chaos in the home environment (p < .04) and increased parent adherence with follow-ups (p < .008) predicted weight loss. Conclusions. We found no treatment effect of child support on weight loss. Active child support of eating/exercise goals appeared to facilitate goal adherence, while anticipated but unrealized child support may have had iatrogenic consequences. Further investigation of family-focused weight loss interventions is warranted.
There is substantial evidence that social network members such as family members and friends play a role in the eating and exercise behaviors of adults (Carson et al., 2013; Cruwys, Bevelander, & Hermans, 2015; Higgs & Thomas, 2016; Leahey, Doyle, Xu, Bihuniak, & Wing, 2015; Shakya, Christakis, & Fowler, 2015; Winston et al., 2015). Data from randomized trials and observational studies suggest that network member support for and/or undermining of healthy eating and exercise behaviors predict weight loss among adults with obesity (Kiernan et al., 2012; Wang, Pbert, & Lemon, 2014; Winston et al., 2015). However, weight loss trials that have enrolled social network members as support partners have had inconsistent results (Black, Gleser, & Kooyers, 1990; Gorin et al., 2005; Kumanyika et al., 2009; Wing & Jeffrey, 1999). While some studies show weight loss benefits (Black et al., 1990; Wing & Jeffrey 1999), others have found a benefit only if network members also lose weight (Gorin et al., 2005; Kumanyika et al., 2009). Further research is needed to identify effective strategies to engage social network members in weight loss interventions.
In the Small Changes and Lasting Effects (SCALE) trial, a 1-year behavior change weight loss study among adults with obesity, we found that participants whose children supported their eating goals had greater weight loss compared with those without child support (Winston et al., 2015). We also found less weight loss as family functioning decreased (Phillips et al., 2017). Together these findings suggest that child support along with family functioning may be factors in successful weight loss.
The relationship between the family functioning (cohesion and conflict), household chaos (disorganization), and parent weight loss has been examined in a limited number of studies (MacRae, Darlington, Haines & Ma, 2017; Martin-Biggers, Quick, Zhang, Jin, & Byrd-Bredbenner, 2017). In an examination of family functioning and food-related behaviors among mothers, low family conflict and low household chaos were associated with healthier eating behaviors (Martin-Biggers et al., 2017). Conceptually, poor family functioning and household chaos may negatively influence meal planning and adherence to eating goals (Martin-Biggers et al., 2017). Household chaos may also increase stress levels that can lead to increased cortisol levels and secondary stimulation of appetite (MacRae et al., 2017; Sominsky & Spencer, 2014).
Family-based weight loss interventions have traditionally addressed childhood obesity (Faith et al., 2012). To our knowledge, no published study to date has had the primary aim of examining children as support partners for parents engaged in a weight loss intervention. The primary objective of this study was to evaluate the feasibility of incorporating child support in a 6-month weight loss intervention targeting parents with obesity. A secondary objective was to examine the relationship between family functioning, particularly disorganization in the home environment, and parent weight loss. We hypothesized that parents with support from their children would have greater adherence to their eating and exercise goals and greater weight loss compared with participants without child support. We also hypothesized that poor family functioning and disorganization in the home environment would be associated with less weight loss.
Method
Participants and Setting
Participants were parents (age ≥18 years; body mass index [BMI] ≥30 kg/m2) who had at least one child ≥12 years old who could support their eating and exercise goals. Participants were recruited at the George Washington University Medical Faculty Associates adult internal medicine practice, which provides care to patients of diverse socioeconomic background and medical complexity. Recruitment was advertised via flyers, video advertisement in practice waiting areas, and emails to physicians and staff. Exclusion criteria were active heart disease, active cancer, uncontrolled thyroid disease, advanced chronic obstructive pulmonary disease, untreated depression or anxiety, active eating disorder, engagement in another weight loss program, current use of weight loss medications, use of chronic systemic corticosteroids, inability to control meal content, and pregnancy. Enrolled participants provided written informed consent. The study was approved by the institutional review board at George Washington University.
Measures
Participants completed a questionnaire at enrollment that included self-reported demographics and the following measures: Confusion, Hubbub, and Order Scale (CHAOS; Matheny, Wachs, Ludwig, & Phillips, 1995) and the McMasters family assessment device general functioning subscale (Byles, Byrne, Boyle, & Offord, 1988). The CHAOS is a 15-item questionnaire that rates the degree of disorganization and noise in the home. Items include the following: “There is often a fuss going on at our home” and “It’s a real zoo in our home.” Each item is rated on a 4-point scale (1 = very much like your home; 4 = not at all like your home). The total CHAOS score was calculated by summing the items after reverse scoring eight items so that high values represent high chaos. The McMasters general functioning subscale is a 12-item scale that measures six dimensions of family functioning. Scores were calculated by reverse scoring the items so that high values represent healthy family functioning and dividing the sum by the number of items with valid responses. A score ≥2 is considered unhealthy family functioning.
Weight was measured using a SECA 813 high-capacity scale with participants in light clothing and without shoes. Height was measured using a SECA 213 portable stadiometer without shoes.
Procedure
Enrollment and Goal Setting
After providing informed consent, participants were randomly assigned to one of two groups. While participants in both arms of the study had eligible children, only participants randomized to the child support group were enrolled with their child as a support partner. Participants randomized to the control group were enrolled alone.
The principal investigator and a trained clinician assistant conducted the study interviews and intervention. The principal investigator is a board-certified primary care physician and researcher specializing in obesity medicine with substantial experience delivering behavior change weight loss interventions. The clinician assistant was a graduate student in public health who received training in conducting human research, obtaining informed consent and assent, and delivering the study intervention.
During the enrollment interview, parent participants in both study groups identified their eating challenges and selected strategies to address these challenges from the following list of options: water instead of sweetened beverages, a fruit or vegetable instead of an unhealthy snack, stop buying unhealthy snack foods, half the main meal fruits or vegetables, main meal on a 10-inch plate, healthy breakfast daily, limit starch at each meal to ¼ plate or less, reduce bread intake to one serving per day, and stop eating fast food. Most of the eating strategies were previously identified and tested in the SCALE trial (Phillips-Caesar et al., 2015). Participants selected a strategy for which they had high confidence (rating of at least 8 out of 10) for adhering at least 6 days/week. As an aid, participants received educational material on how to interpret nutrition labels. Participants were encouraged to select an additional eating goal after achieving adherence with their initial goal for at least 1 month. Participants in both study groups received an Omron HJ-720IT pedometer at enrollment and set a daily step goal utilizing step data from Week 1 of the study. Participants in both study groups contracted to adhere to both eating and step goals at least 6 days/week.
At enrollment, participants in the child support group provided contact information for one child whom they identified as a potential support partner. The clinician assistant then attempted to contact the nominated child and enroll her or him as a support partner. Informed consent was obtained for children ≥18 years old, and informed assent for children 12 to 18 years old. The enrolled child reviewed the following options for supporting their parent, adopted from the SCALE trial (Winston et al., 2015): verbal encouragement, joining in the behavior change, not bringing unhealthy snacks, purchasing heathy foods, helping to prepare healthy meals, trying new recipes, and helping with household chores. The clinician assistant then helped the parent and child select a mutually agreeable support behavior, allowing for a different supportive behavior not on the list. The clinician encouraged discussing nonsupportive behaviors that the child should avoid.
Follow-up Sessions
The clinician assistant contacted parent participants at routine intervals (weekly for the first 3 months, then biweekly for 3 months) to obtain self-reports on the number of days in the previous week parents achieved their eating and step goals. As in our previous weight loss trial (Phillips-Caesar et al., 2015), we defined adherence as the proportion of days in the previous week the participant achieved the set goal. When adherence was less than 6 days/week, the participant and clinician assistant engaged in a problem-solving exercise to identify challenges to achieving the goal (Perri et al., 2001) and discussed potential solutions. The participant selected a solution to incorporate the upcoming week. In addition, parents in the child support group reported how many days in the previous week their child had engaged in the agreed-upon supportive behavior. Follow-ups for both groups were mostly by phone but occurred in person at Months 3 and 6, with body weight measurements at each of these visits. Monthly contact with children in the child support group were exclusively by phone, during which children were asked to provide feedback on their ability to engage in their contracted supportive behavior. Treatment fidelity was monitored by direct observation of the clinician assistant at routine intervals.
Statistical Analysis
Descriptive statistics were calculated using means and proportions. Student’s t tests were used to compare the following outcomes between parents in the child support versus control groups: (1) number of sessions participants were adherent to eating and exercise goals 6 days/week and (2) weight loss at study midpoint (Month 3) and completion (Month 6).
In the child support group, unadjusted linear regression models were used to examine the relationship between days of child support reported by parents and the following dependent variables: (1) parent confidence in achieving eating goals, (2) number of follow-up sessions parents reported adherence with eating and step goals 6 days/week, and (3) parent weight loss at study completion.
CHAOS scores were divided into quartiles with the highest quartile (score ≥31) reported as a high score and scores <31 as a low score. Weight loss at Months 3 and 6 were stratified by high and low CHAOS scores and compared by randomization group using Student’s t tests. A similar analysis was done for McMasters scores stratified by score ≥2 (poor family functioning) versus <2. Multivariate regression models were used to examine predictors of weight loss at Months 3 and 6 adjusted for parent age, gender, enrollment BMI, and randomization group. CHAOS scores were used as continuous variables in regression models.
Results
A total of 102 parent participants were randomized, 61 to the child support group and 41 to the control group. In the child support group, 43 children were engaged in supporting their parent (Figure 1). The remaining 18 children identified as potential support partners could not be reached for enrollment and their parents did not report that they provided support. Only 1 parent in this group of 18 completed the study. There were 31 parents who completed the study in the control group (75% completion rate), and 32 parents in the child support group (52%). The majority of dropout in the child support group occurred among parents whose children did not engage in the study (65.5%).
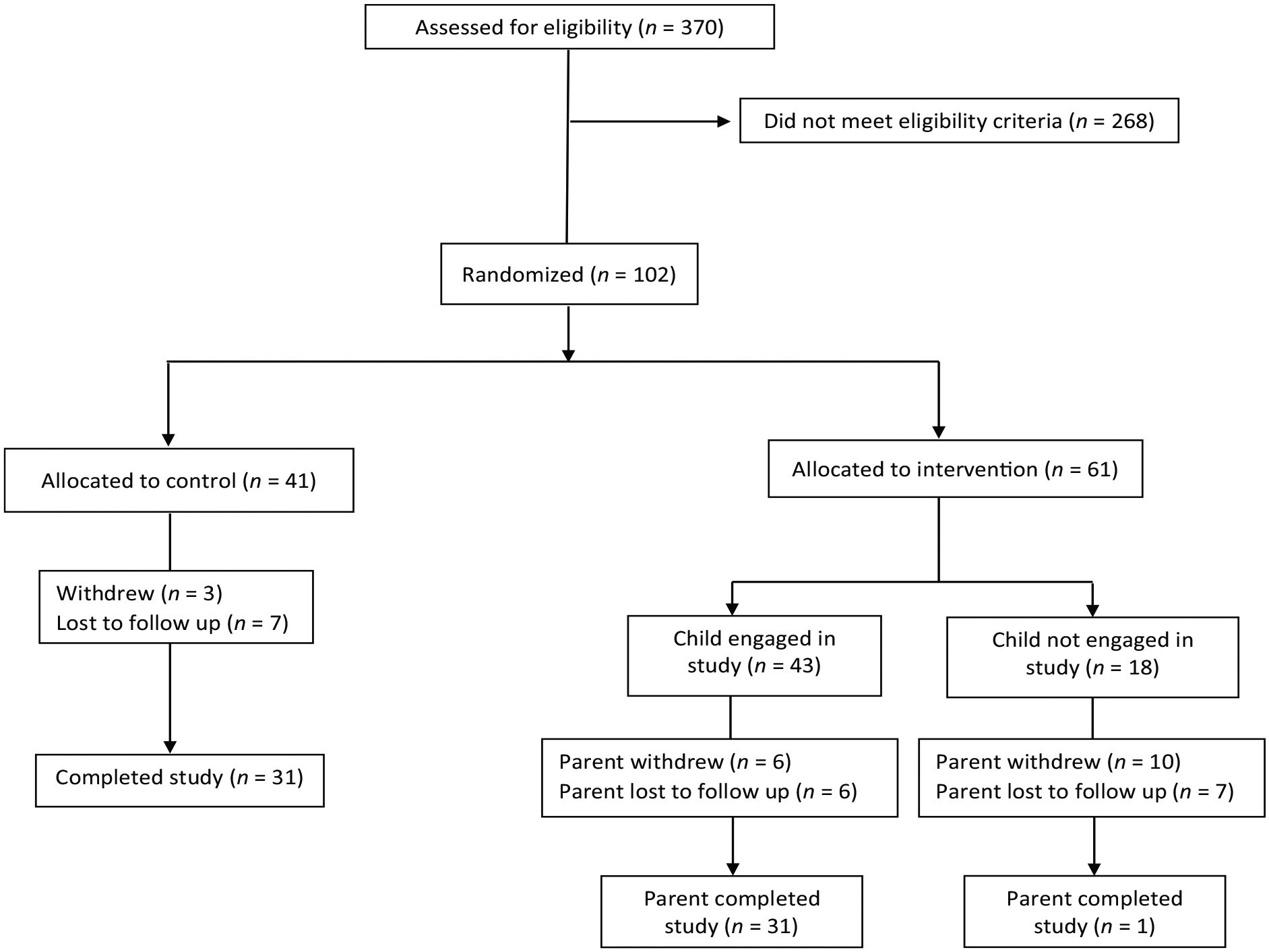
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Table 1 shows the baseline characteristics of parent participants. Participants were primarily female (95%), mean age 56 years, and 64% were employed. There was no significant difference between study noncompleters versus completers in the following characteristics: age, percent completing high school, employment status, or marital status. Table 2 shows the baseline characteristics of the children enrolled as support partners. The majority of children were female (88%), 18 years or older (88%), and reported contact with their parent at least once a day (72%). All child support partners <18 years old lived with their parent, 39% of child support partners ≥18 years old lived with their parent.
Demographics of Parent Participants Stratified by Randomization Group.
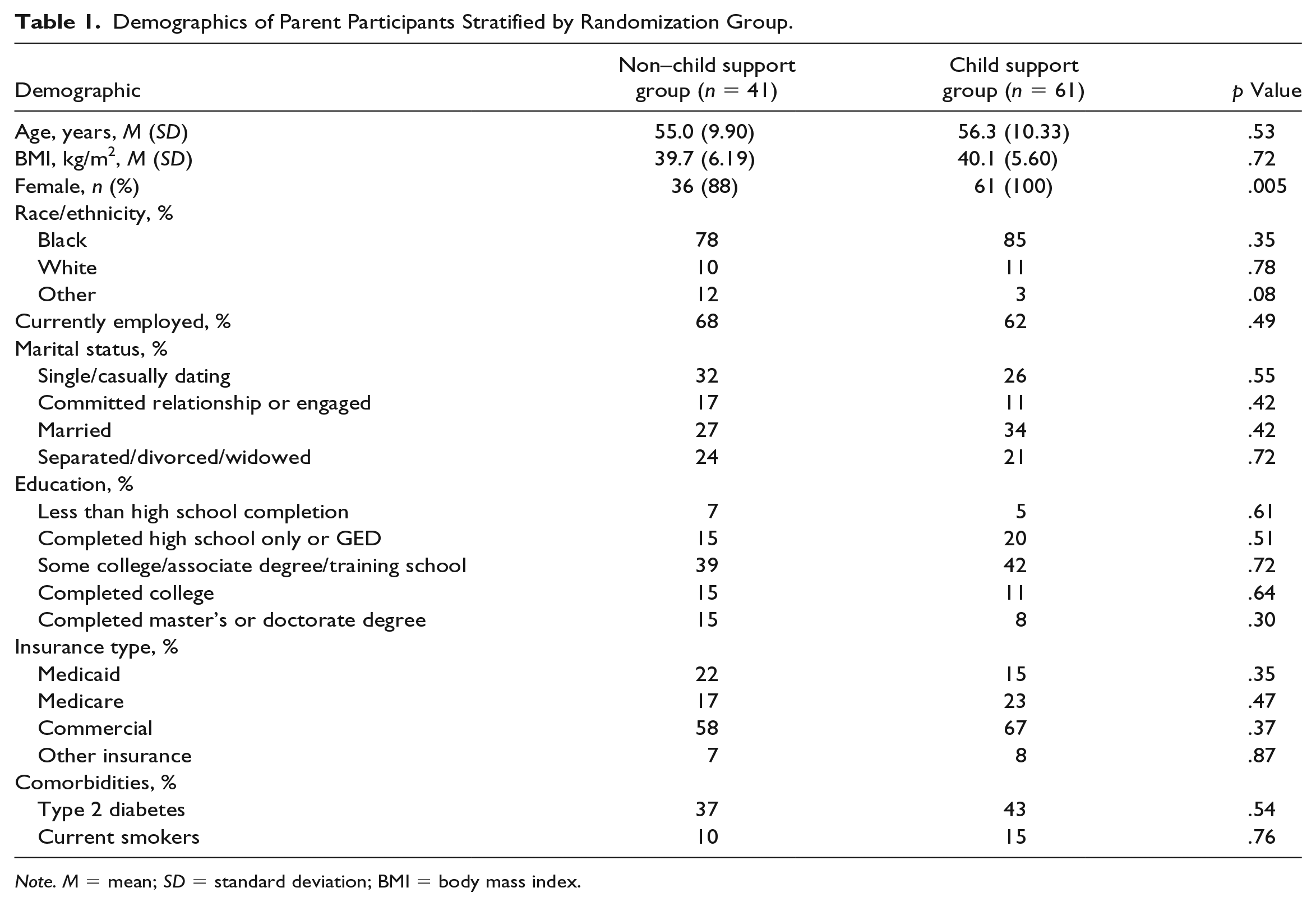
Note. M = mean; SD = standard deviation; BMI = body mass index.
Child Demographics (n = 33).
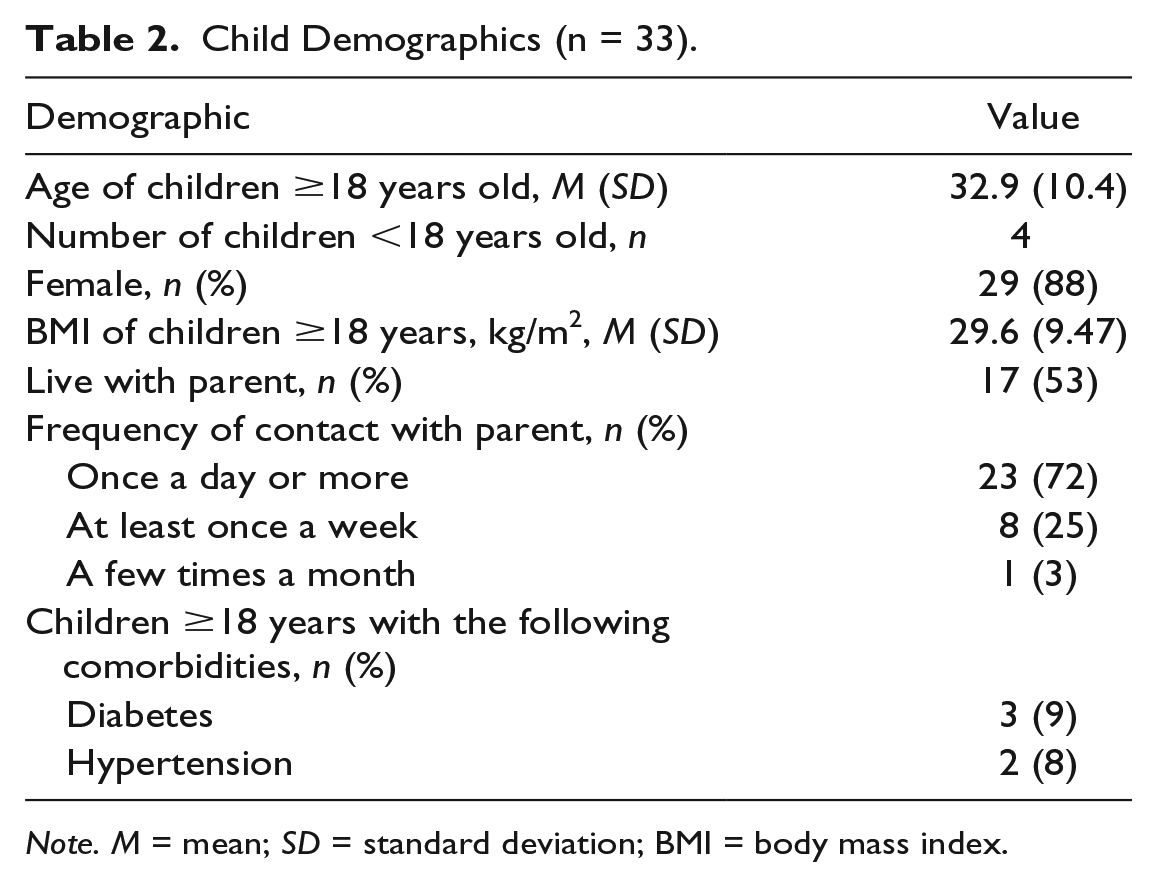
Note. M = mean; SD = standard deviation; BMI = body mass index.
The most commonly selected eating goals at enrollment were healthy breakfast (32%), fruit or vegetable instead of an unhealthy snack (21%), and half the main meal fruits or vegetables (10.7%). Table 3 shows the supportive behaviors that children contracted to engage in at enrollment. There were four child support partners <18 years old, and their supportive behaviors did not differ from the adult children. There was no significant difference in the percentage of children who selected the three most frequent supportive behaviors when examined by the living location of child or CHAOS score.
Child Supportive Behaviors.
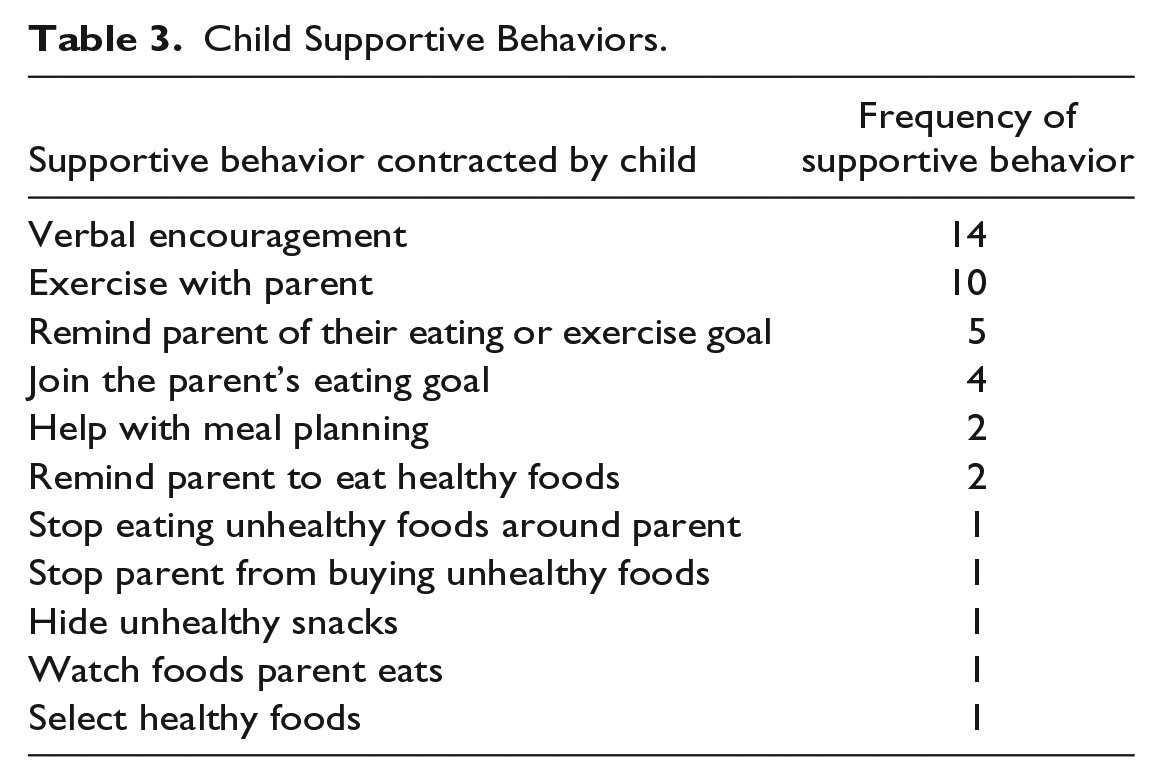
Table 4 shows the primary study outcomes. Mean weight loss was not significantly different between the study groups at midpoint (Month 3) or closeout (Month 6). There was also no significant difference between study groups in the mean number of sessions participants reported adherence to their eating or step goals (p = .77 and .79, respectively). Participants who selected a second eating goal during the course of the study (n = 19) had greater weight loss at study completion compared with those who did not (−7.42 vs. −1.29 lbs, p = .01).
Parent Weight Loss by Randomization Group.
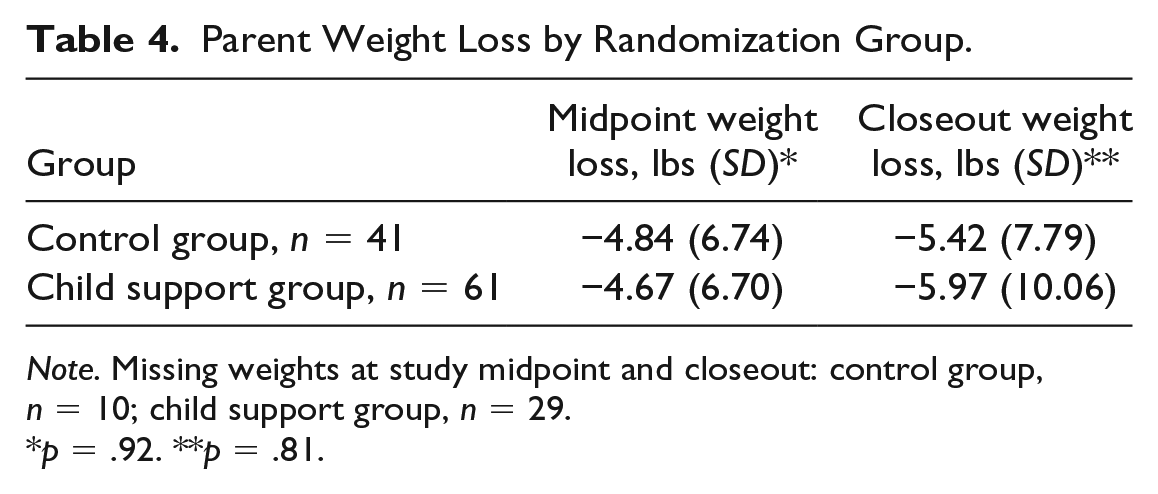
Note. Missing weights at study midpoint and closeout: control group, n = 10; child support group, n = 29.
p = .92. **p = .81.
In subgroup analyses, the number of sessions that participants in the child support group reported adherence to their eating goal ≥6 days/week increased as the days of child support increased (parameter estimate 0.18, standard error [SE] = 0.03, p < .0001). Participant adherence to their step goal ≥6 days/week also increased as days of child support increased (parameter estimate 0.09, SE = 0.02, p = .0001). Increased days of child support did not predict increased weight loss (parameter estimate −1.74, SE = 3.30, p = .14). In an unadjusted linear regression model, the number of sessions that participants reported high confidence in achieving their eating goals increased as the days of child support increased (parameter estimate 0.22, SE = 0.03, p < .0001).
Table 5 shows secondary analyses of adherence with eating goals and weight loss stratified by the following groups: control group (n = 41), participants in the child support group whose children were not engaged in the study (n = 18), and participants in the child support group whose children were engaged (n = 43). One-way analysis of variance (ANOVA) testing showed a significant difference between groups in the mean number of sessions in which participants were adherent to their eating goal (p = .0014), and step goal (p = .047). Pairwise comparison using Tukey’s test showed significantly less adherence with eating goals among parents in the child support group whose children did not engage in the study versus parents whose children did engage in the study (significant at the .05 level). Pairwise comparison of the step goal showed a difference in adherence at the .05 level between parents in the child support group whose children did not engage versus the other two groups. There were significantly fewer follow-up sessions completed by parents in the child support group whose children did not engage compared with the other two groups (p < .0001). Among parents in the child support group whose children did not engage, 72% completed three or fewer sessions and 39% completed only the enrollment interview.
Parent Adherence With Goals by Child Engagement.
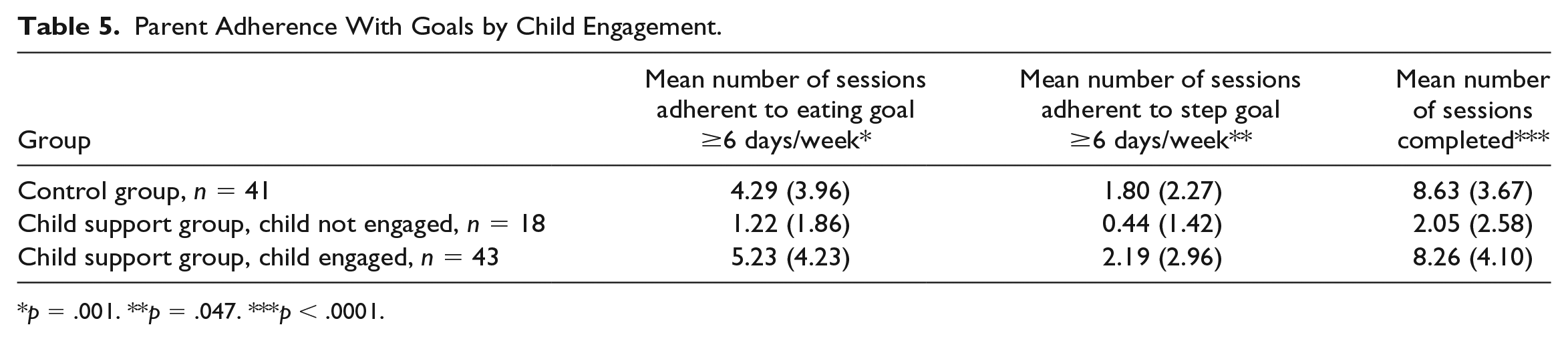
p = .001. **p = .047. ***p < .0001.
Table 6 shows weight loss by CHAOS score. Weight loss was significantly greater among participants with low CHAOS scores at study midpoint (p = .001), and closeout (p = .04). Participants with McMasters score <2 (indicating healthy family functioning) had borderline greater weight loss at study completion compared with participants with scores ≥2 (−7.64 vs. −2.92 lbs, p = .056). When examining the relationship between participants’ eating behaviors and CHAOS scores, a higher percentage of participants with high CHAOS scores reported overeating when feeling sad or in a negative mood compared with those with lower CHAOS scores (72% vs. 45%, p = .02). In post hoc analyses, there was no significant difference in mean CHAOS score between participants in the child support group whose children engaged versus those whose children did not engage in the study. There was also no significant difference in mean CHAOS scores between participants who completed the study versus those lost to follow up.
Weight Loss by CHAOS and McMasters Scores.
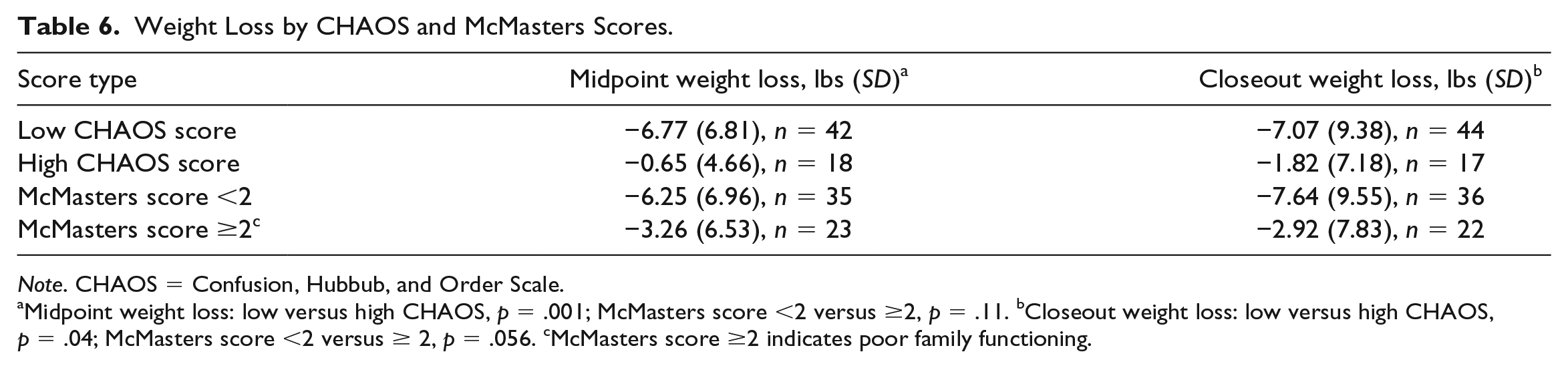
Note. CHAOS = Confusion, Hubbub, and Order Scale.
Midpoint weight loss: low versus high CHAOS, p = .001; McMasters score <2 versus ≥2, p = .11. bCloseout weight loss: low versus high CHAOS, p = .04; McMasters score <2 versus ≥ 2, p = .056. cMcMasters score ≥2 indicates poor family functioning.
Table 7 shows two multivariate regression models examining predictors of parent weight loss adjusted for parent age, gender, enrollment BMI, and randomization group. Weight loss at study midpoint increased as the CHAOS score decreased (p = .034), and adherence to follow-up sessions increased (p = .003). There was also greater weight loss at study completion as the CHAOS score decreased (p = .044), and adherence to follow-up sessions increased (p = .008). Parent selection of a second eating goal was added as a covariate in this model.
Predictors of Weight Loss at Study Midpoint and Closeout.
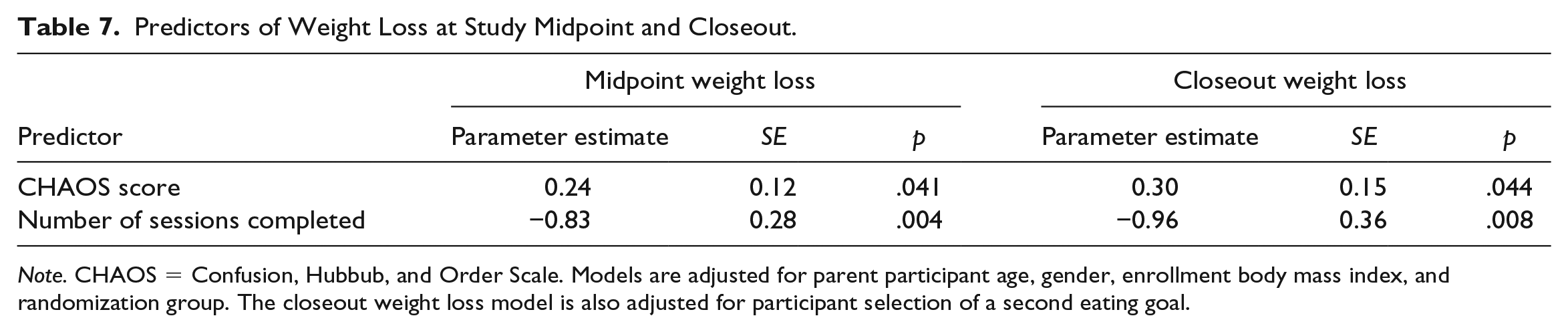
Note. CHAOS = Confusion, Hubbub, and Order Scale. Models are adjusted for parent participant age, gender, enrollment body mass index, and randomization group. The closeout weight loss model is also adjusted for participant selection of a second eating goal.
Discussion
This study examined engaging children as support partners for parents in a behavior change weight loss study. The primary outcome was no significant difference in weight loss between parents enrolled in the child support versus control groups. Secondary analyses showed (1) greater adherence to eating and exercise goals among parents in the child support group as days of child support increased and (2) greater weight loss as CHAOS scores decreased and adherence with follow-up sessions increased.
To our knowledge, this is the first published study with the primary aim of engaging adolescent and adult children as support partners for parents in a weight loss study. We found no significant difference in weight loss between parents in the child support versus non–child support groups. However, we had 18 parents in the child support group whose children did not engage in the study. These parents were less adherent to their goals and the majority were lost to follow up. It may be that they anticipated the support of their child and when they did not receive it this led to study nonadherence. The children who did not engage in the study were all adults. A primary reason parents gave for lack of child engagement was their child’s busy work schedule.
Within the child support group, parent adherence with eating and exercise goals increased as days of child support increased. Also, parents’ confidence in achieving their eating goals increased with days of child support. These findings indicate a positive role for child support in encouraging parent eating/exercise behavior change.
When examining the relationship between family home environment and weight loss, we found that weight loss increased as CHAOS scores decreased. A high score on the CHAOS represents a chaotic, disorganized, and hurried home environment (Matheny et al., 1995). The relationship between the family home environment and childhood obesity has been examined (Bates et al., 2018), but limited studies have investigated this relationship among adults with obesity. MacRae et al. (2017) examined the relationship between chaos in the home and dietary fat intake among parents of preschool-age children. The investigators found that chaos in the home environment was positively associated with parental fat intake. Martin-Biggers et al. (2017) examined the relationship between household chaos and food-related behaviors among mothers and their preschool-age children and found that low household chaos was associated with healthier food choices. The investigators also found that mothers with high family conflict and chaos were more likely to engage in emotional and disinhibited eating behaviors. In our study, we found that parents with high CHAOS scores were more likely to report overeating when they were in a sad or negative mood.
Our study has limitations. We had a 39% attrition rate that introduces the potential for follow-up bias. The highest percentage of dropout occurred among participants randomized to the child support group whose children did not engage in the study. We attempted to contact these participants to investigate their reasons for dropout but were unable to reach them. It is possible that among participants randomized to the child support group, lack of engagement by their child played a role in their decision to discontinue the study. Our power to detect an effect was lower than we had planned given that our final sample size was smaller than expected, and there was larger than expected within group variance in weight. A post hoc test showed that our actual power for detecting a 20 lbs difference in mean closeout weights between study groups, assuming SD of 40 lbs was 0.50. Therefore, the chance of a type II error was higher than expected. An additional limitation was that parent adherence with eating goals was self-reported. Finally, while we asked parents about behaviors that their children engaged in that undermined their study goals, they generally only reported supportive behaviors.
In conclusion, we found no significant difference in weight loss between study groups. However, 30% of children in the child support group did not engage in the study. Participants whose children did not engage had poor adherence with follow-ups and the majority did not complete the study. Within the child support group, parents reported greater adherence to goals as the frequency of child support increased. For all participants, weight loss increased as chaos in the home environment decreased. Our results suggest a potential role for child support in parent eating and exercise behavior change and indicate that chaos in the home environment plays a role in weight loss success.
Footnotes
Acknowledgements
We thank Michael Rohrbaugh, PhD, for contributing to manuscript revisions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant funding from the Margaret Q. Landenberger Foundation.