
Abstract
Problem Addressed:
To better understand the factors associated with family cancer history (FCH) information and cancer information seeking, we model the process an individual undergoes when assessing whether to gather FCH and seek cancer information and compare models by sociodemographics and family history of cancer. We used cross-sectional data from the Health Information National Trends Survey (HINTS 5, Cycle 2) and variables (e.g., emotion and self-efficacy) associated with the Theory of Motivated Information Management to assess the process of FCH gathering and information seeking. We completed path analysis to assess the process of FCH gathering and stratified path models.
Results:
Those who felt they could lower their chances of getting cancer (emotion) were more confident in their ability to complete FCH on a medical form (self-efficacy; B = 0.11, p < .0001) and more likely to have discussed FCH with family members (B = 0.07, p < .0001). Those who were more confident in their ability to complete a summary of their family history on a medical form were more likely to have discussed FCH with family members (B = 0.34, p < .0001) and seek other health information (B = 0.24, p < .0001). Stratified models showed differences in this process by age, race/ethnicity, and family history of cancer.
Implications for Public Health Research and Practice:
Tailoring outreach and education strategies to address differences in perceived ability to lower chances of getting cancer (emotion) and confidence in the ability to complete FCH (self-efficacy) could help encourage less engaged individuals to learn about their FCH and gather cancer information.
The collection of family cancer history (FCH) is an effective and inexpensive way to capture information that can guide stratified cancer risk assessment, target screening, and prevention efforts; activate individuals and their family members for screening and/or genetic counseling and testing; and motivate positive behavior change (Ashida et al., 2012; Claassen et al., 2010; deHeer et al., 2017; Koehly et al., 2018; McBride et al., 2013; Ochs-Balcom et al., 2015; Qureshi & Kai, 2008; Rebbeck et al., 2018; Valdez et al., 2010; Yoon et al., 2002). While family health history is widely acknowledged as useful for guiding clinical and public health practice, as few as one third of individuals know their family health information and only 3% have ever used a tool to collect this information (C.G. Allen et al., in press). Researchers have identified factors associated with the likelihood of knowing family health information, finding that women, cancer survivors, and people with higher education are more likely to know their FCH (Hesse et al., 2005; Longo et al., 2010; Weaver et al., 2010). Decreased awareness of FCH is associated with a lack of knowledge about cancer histories among family members, poor communication about health history, and a lack of closeness among family members (Foster et al., 2002; Kelly et al., 2007). Despite recognition of poor uptake of FCH, we do not yet have a clear understanding of the process an individual goes through in deciding whether and how to seek this type of health information.
In addition to being valuable to informing prevention activities, having better FCH knowledge may increase the likelihood that an individual will seek additional information about cancer and other health risks (Kaphingst et al., 2009). Cancer information seeking can include various sources, such as friends, family, health care providers, print, and electronic materials (Finney Rutten et al., 2016). Gaining a clearer understanding of both the process individuals go through in gathering FCH and how FCH collection is associated with information seeking may help support an individual’s overall experience in obtaining FCH. It may also encourage the gathering of additional cancer health information and support individuals in achieving their specific information needs (Finney Rutten et al., 2016; Rutten et al., 2006).
Given the limited understanding of the process of gathering FCH and its association with information-seeking behaviors, we used data from a nationally representative sample to better understand the steps an individual goes through in deciding whether to gather FCH information and how this process affects subsequent health information-seeking behaviors. We used the theory of motivated information management (TMIM) to help conceptualize these processes. According to TMIM, individuals manage sensitive information, such as FCH, in three phases: (a) interpretation of the need to gather information based on the level of uncertainty, (b) evaluation of whether and how to manage information, and (c) a decision about whether to gather sensitive information. This theory is particularly useful in helping to understand the interpersonal process of information seeking for potentially challenging or sensitive subjects such as FCH. Understanding interpersonal processes and mechanisms of gathering FCH could help in developing interventions to address challenges or misconceptions that may arise in this process and subsequent health information-seeking behaviors. The TMIM has been applied previously to explain aspects of the family health history gathering process but has not been extended to consider secondary outcomes such as health-seeking behaviors (Hovick, 2014). In the present study, we aim to (a) report sociodemographics associated with the primary outcome of FCH information management strategy and secondary outcome of cancer information-seeking behavior, (b) model the process an individual goes through in assessing whether to gather FCH information and seek cancer information, and (c) compare these models based on age, race/ethnicity, gender, and family history of cancer.
Method
Data Set
We used cross-sectional data from the Health Information National Trends Survey (HINTS 5, Cycle 2), a population-based survey administered by the National Cancer Institute (2015). This survey was mailed to non-institutionalized, civilian adults aged 18 and older between September and December 2018. Data are deidentified and publicly available (https://hints.cancer.gov/default.aspx). The overall reported response rate for HINTS 5, Cycle 2 was 32.85%. Of the 3,504 respondents, 3,375 responded to the outcome variables in the model and were included in the sample for our main path analysis.
TMIM Model
According to TMIM, an individual goes through three phases when assessing information about a health topic. In the first phase, an individual is motivated to seek information due to their perceived level of uncertainty about a topic (uncertainty discrepancy), which results in an emotional response (emotion). In the second phase, an individual will assess the cost and benefit of the outcome (i.e., is it worth gathering FCH?). Factors that influence this decision include benefits or harms that may come from gathering this type of information (outcome expectation) and the perception that the individual has the skills to complete the task (self-efficacy). In the third phase, the individual makes a decision about whether to avoid or seek the information (information management strategy; Lambert & Loiselle, 2007; Weaver et al., 2010). Our model continues to explore this process by incorporating health-seeking behaviors as a secondary outcome. Prior literature has suggested that how an individual chooses to manage their health information has a direct impact on health-seeking behaviors (Finney Rutten et al., 2016; Rutten et al., 2006).
Variables
We measured uncertainty discrepancy using the question “how well do you know your family’s history of cancer?” with responses ranging from very well to not at all (5-point Likert-type scale) and emotion using the question, “How much do you agree or disagree with each of the following statement: There is not much you can do to lower your chances of cancer?” with responses of “strongly agree to strongly disagree” (4-point Likert-type scale). Self-efficacy is the individual’s perception that they have the skills needed to successfully complete the task at hand, which was measured with the question “How confident are you that you could complete a summary of your family cancer history on a medical form?” (5-point Likert-type scale). FCH information management strategy involves decisions about whether to seek information or avoid information. This was assessed with the question, “Have you ever had a discussion about your family cancer history with any of the following people? If there is no cancer in your family, and you have discussed this, please include that. Mark all that apply” with the response options of biological mother, biological father, biological sister, biological brother, biological children, other biological family members, a health care provider, and I have not discussed. These were re-categorized as not discussed, discussed with one family member, and discussed with more than one person. Responses to discussion with a health care provider (N = 242) were excluded from the current analysis, as our analysis focused on family members. The response option of “more than one person” was automatically aggregated as part of the HINTS data set and thus included responses in which health care providers and one or more family members were selected. Finally, cancer information-seeking behaviors include whether the individual has looked for cancer information. This was assessed with the question, “Have you ever looked for information about cancer from any source” (Yes/No). We were unable to assess outcome expectations (i.e., the benefits and harms that may come from seeking health information), as no question aligned with this construct in the HINTS data set.
Demographic variables included marital status (married, living as married, divorced, widowed, separated, single never married); gender (male/female); annual income (less than US$20,000, US$20,000 to <$35,000, $35,000 to <$50,000, $50,000 to < $75,000 and $75,000 or more); and race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black or African American, non-Hispanic American Indian or Alaska native, non-Hispanic Asian, non-Hispanic Native Hawaiian or other Pacific Islander, and non-Hispanic multiple races), which were grouped into non-Hispanic White (White), Hispanic, non-Hispanic Black (Black), and other races/ethnicities (Other); age (18–34, 35–49, 50–64, 65–74, and 75+); education level (less than high school, high school graduate, some college, and college graduate or more); occupational status (employed, unemployed, homemaker, student, retired, disabled); household size; and whether family members have ever had cancer (yes, no, and unsure). All variables were as of time of survey.
Analysis
Data were analyzed using SAS Version 9.4. To account for probability sampling design and jackknife replicate weights, univariate frequencies and means were weighted to obtain nationally representative estimates for descriptive statistics. Means and standard deviations are reported for continuous measures and frequencies and percentages for categorical variables. Bivariate analyses were run using chi-square tests to assess demographic differences in information management strategies (no discussion about FCH, discussion with one person, discussion with more than one person) and health-seeking behaviors (never looked for cancer information and looked for cancer information).
The main analysis involved describing the process through which FCH may be gathered and the resulting health-seeking behaviors. To assess the process through which FCH is gathered, we completed a path analysis without population weights to maximize sensitivity and power (Lee & Niederdeppe, 2011). The general steps we followed included model specification, model identification, model estimation (testing model fit), re-specification, and reporting of results (Kline, 2015). The initial model included uncertainty discrepancy, emotion, self-efficacy, information management, and other health-seeking behaviors. Based on the poor initial model fit, the model was respecified to include emotion, self-efficacy, information management, and other health-seeking behaviors. Stratified models were then run for (a) family health history, assessing differences in individuals with family history of cancer and individuals without a family history of cancer; (b) race/ethnicity, to evaluate differences between White, Hispanic, Black, and Other; (c) gender (male and female); and (d) age (18–34 and 35 and older). Several model fit indices are reported: Chi-square, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and goodness-of-fit index (GFI). We used the following as criteria for good model fit: chi-square with a p value < .05(Barrett, 2007), RMSEA < 0.08(Hu & Bentler, 1999), SRMR < 0.08(Hu & Bentler, 1999), CFI > 0.90 (Bentler, 1990; Hu & Bentler, 1999), and GFI > 0.95 (Kline, 2015).
Results
The demographic characteristics of the study population are included in Table 1. About half of the individuals were married (n = 1,651, 49.83%) and female (n = 2,054, 51.2%). More than half of the sample (n = 1,676, 56.9%) made US$50,000 per year or more. Most individuals were non-Hispanic White (n = 1,983, 64.77%), between the ages of 50 and 64 (n = 1,113, 30.3%), had at least some college education (n = 2,547, 68.7%), and were employed (n = 1,696, 58.2%). The average household size was 2.3 (SD = 1.35), and most individuals reported having a family member who had cancer (n = 2,463, 69.9%).
Sociodemographic Characteristics of Health Information National Trends Survey Cycle of Sample (N = 3,504).
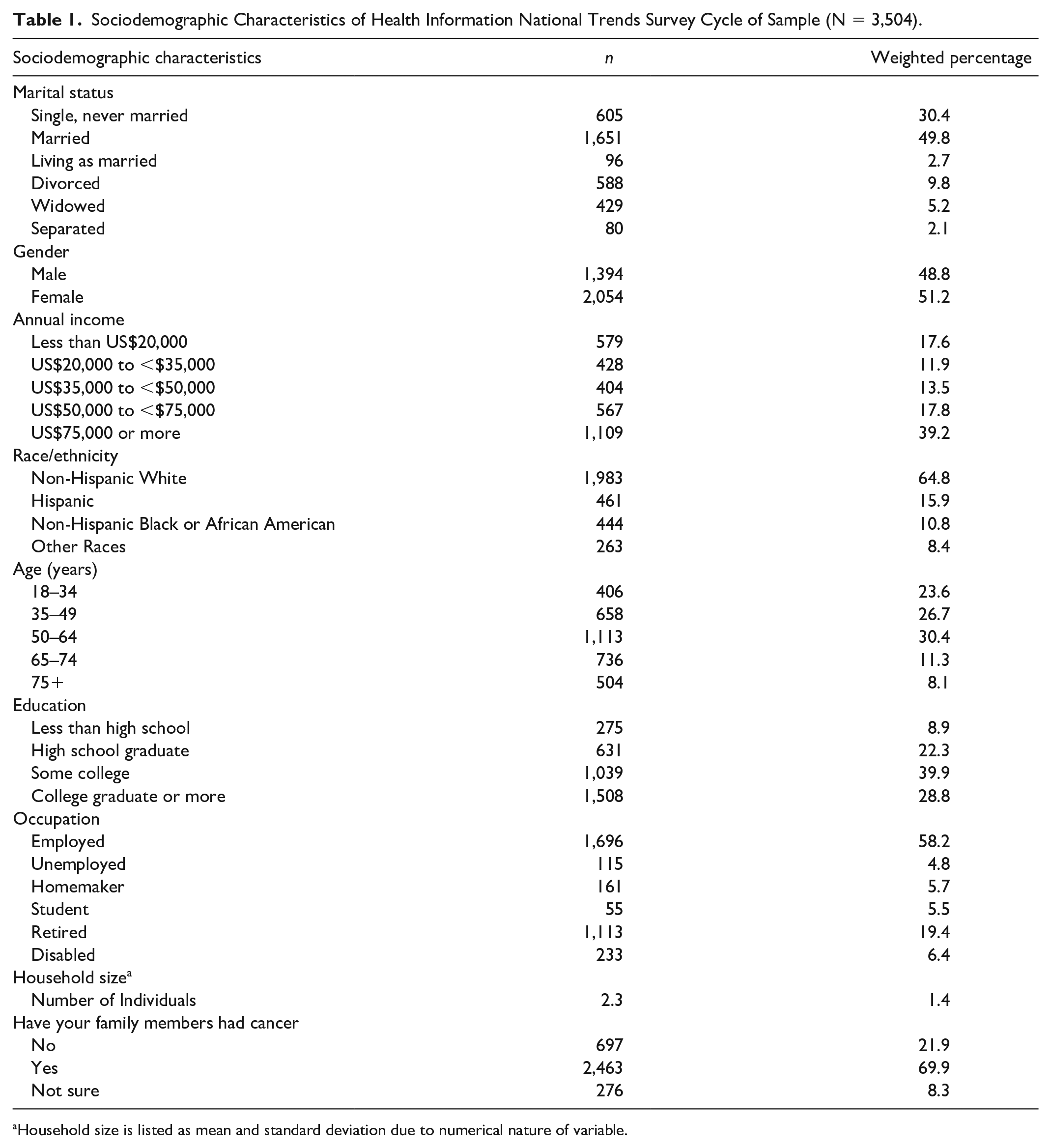
Household size is listed as mean and standard deviation due to numerical nature of variable.
Sociodemographic Associations With Outcomes of FCH Information Management Strategy and Cancer Information-Seeking Behavior
FCH Information Management Strategy
Among all respondents to questions about FCH information, 60.5% (N = 1,876) had discussed FCH with more than one person. Compared with those who never discussed FCH with a family member or health care provider, those who discussed FCH with more than one person were more likely to be married (53.04% vs. 44.84%, p = .0135), be female (55.34% vs. 39.63, p < .0001), earn more than US$75,000 per year (47.0% vs. 26.19%, p < .0001), be non-Hispanic white (72.03% vs. 49.2%, p < .0001), be a college graduate ( 34.55% vs. 19.23%, p < .0001), and have a family history of cancer (81.55% vs. 43.10%, p < .0001; Table 2).
Bivariate Associations of Sociodemographics Associated With FCH Information Management Strategy and Cancer Information Seeking Behavior.

Note. AA = African American; FCH = family cancer history.
Cancer Information-Seeking Behaviors
The majority of respondents (N = 2,786) had sought cancer information. Compared with those who had never sought cancer information, those who sought cancer information were more likely to be married (52.69% vs. 38.91%, p < .0001), be female (54.47% vs. 38.96%, p < .0001), earn more than US$75,000 per year (44.08% vs. 19.98%, p < .0001), be non-Hispanic White (68.55% vs. 49.97%, p < .0001), have graduated from college (32.84% vs. 13.07%, p < .0001), be employed (60.2% vs. 50.6%, p = .02), and have had a family member with cancer (72.31% vs. 60.90%, p = .0022; Table 2).
Process of FCH Gathering
Approximately 60% of respondents stated that they knew their FCH well or very well (uncertainty discrepancy). Most somewhat disagreed or strongly disagreed with the statement, “there is not much you can do to lower your chances of cancer” (emotion; 65.6%). Most reported being very confident (n = 943, 27.44%) or completely confident (n = 860, 22.16%) in their ability to complete a family cancer history (self-efficacy; Table 3). Demographic associations for each of these predictor variables aligned closely with those found among the primary outcome (FCH information management strategy) and secondary outcome (cancer information seeking), except females were no more likely than males to disagree with the statement “there is not much you can do to lower your chances of cancer” (emotion).
Details About Constructs Included in Path Model.
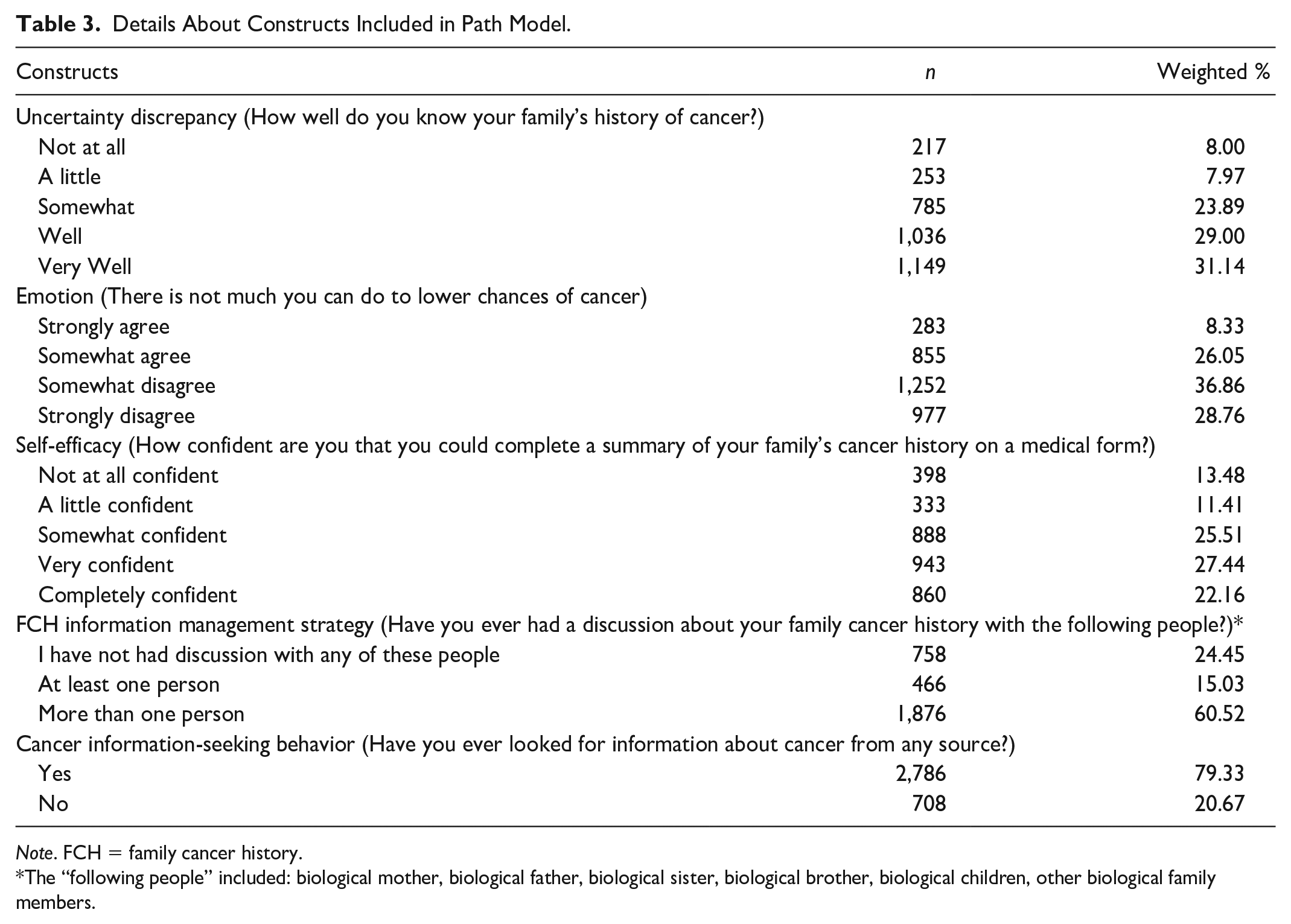
Note. FCH = family cancer history.
The “following people” included: biological mother, biological father, biological sister, biological brother, biological children, other biological family members.
The original path model (data not included) included reported knowledge of FCH (uncertainty discrepancy), perceived ability to lower the chance of cancer (emotion), ability to complete FCH (self-efficacy), discussions with family members about FCH (FCH information management strategy), and cancer information-seeking behavior. This model had a poor fit (RMSEA = 0.25, SRMR = 0.19). When respecifying the model, we removed reported knowledge of FCH (uncertainty discrepancy), as it was the least significant construct in the model (B = 0.01, p = .5).
After removing reported knowledge of FCH (uncertainty discrepancy), the model fit well (RMSEA = 0.085, SRMR = 0.4, GFI = 0.96, CFI = 0.93; Figure 1). Those who felt they could lower their chances of getting cancer (emotion) were more likely to have confidence in their ability to complete FCH on a medical form (self-efficacy; B = 0.11, p < .0001) and more likely to have discussed FCH with family members (FCH information management strategy; B = 0.07, p < .0001). An individual’s self-efficacy or confidence in ability to complete FCH on a medical form was associated with the likelihood to discuss family health information with family members (FCH information management strategy; B = 0.34, p < .0001). Those that discussed family cancer information were more likely to seek other cancer
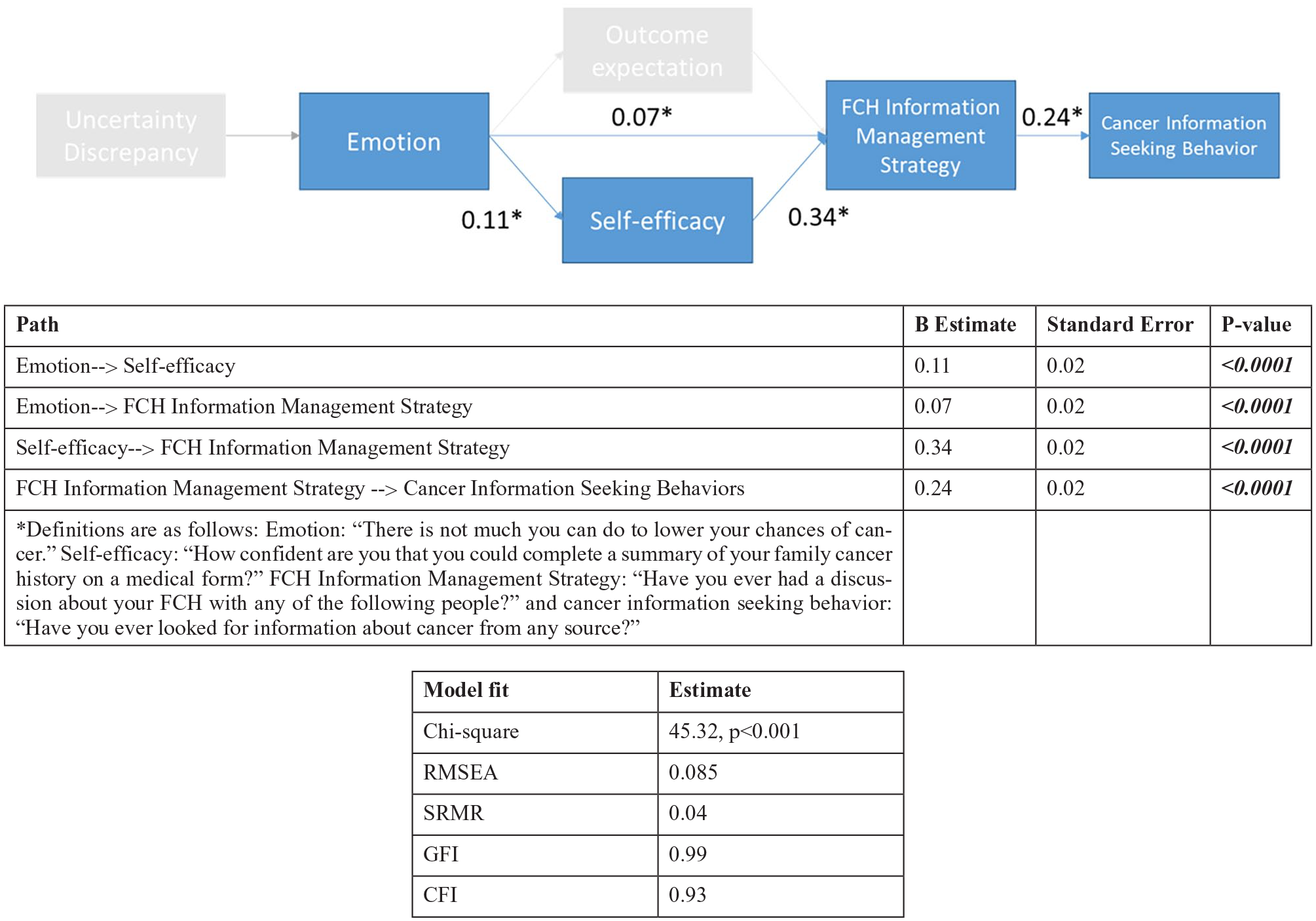
Testing the Proposed Path Model.
Stratified Path Models: Family History of Cancer, Age, Race/Ethnicity, and Gender
Next, we stratified models to assess for differences in the family history of cancer, age, race/ethnicity, and gender. Our stratified models included perceived ability to lower the chance of cancer (emotion), ability to complete FCH (self-efficacy), discussions with family members about FCH (FCH information management strategy), and cancer information-seeking behavior.
Stratification by Family Health History
We first tested stratified path models of those with FCH and those with no FCH (Figure 2). Paths for both those with FCH and those without FCH are similar. Perceived ability to reduce cancer risk (emotion) was positively associated with confidence in the ability to complete an FCH (self-efficacy) in both models, (FCH: B = 0.11, p < .0001, No FCH: B = 0.12, p = .003) and likelihood to have discussed FCH (FCH information management strategy; FCH: B = 0.06, p = .005, no FCH: B = 0.16, p < .0001). Confidence in ability to complete an FCH (self-efficacy) was a predictor of the likelihood to discuss family cancer (FCH information management strategy) for both models (FCH: B = 0.32, p < .0001, no FCH: B = 0.18, p < .0001). Those that discussed family cancer information (FCH information management strategy) were more likely to seek health information (cancer information-seeking behavior) in both models (FCH: B = 0.19, p < .0001, no FCH: B = 0.26, p < .0001). The model fit well for both those with a history of FCH and no history of FCH.
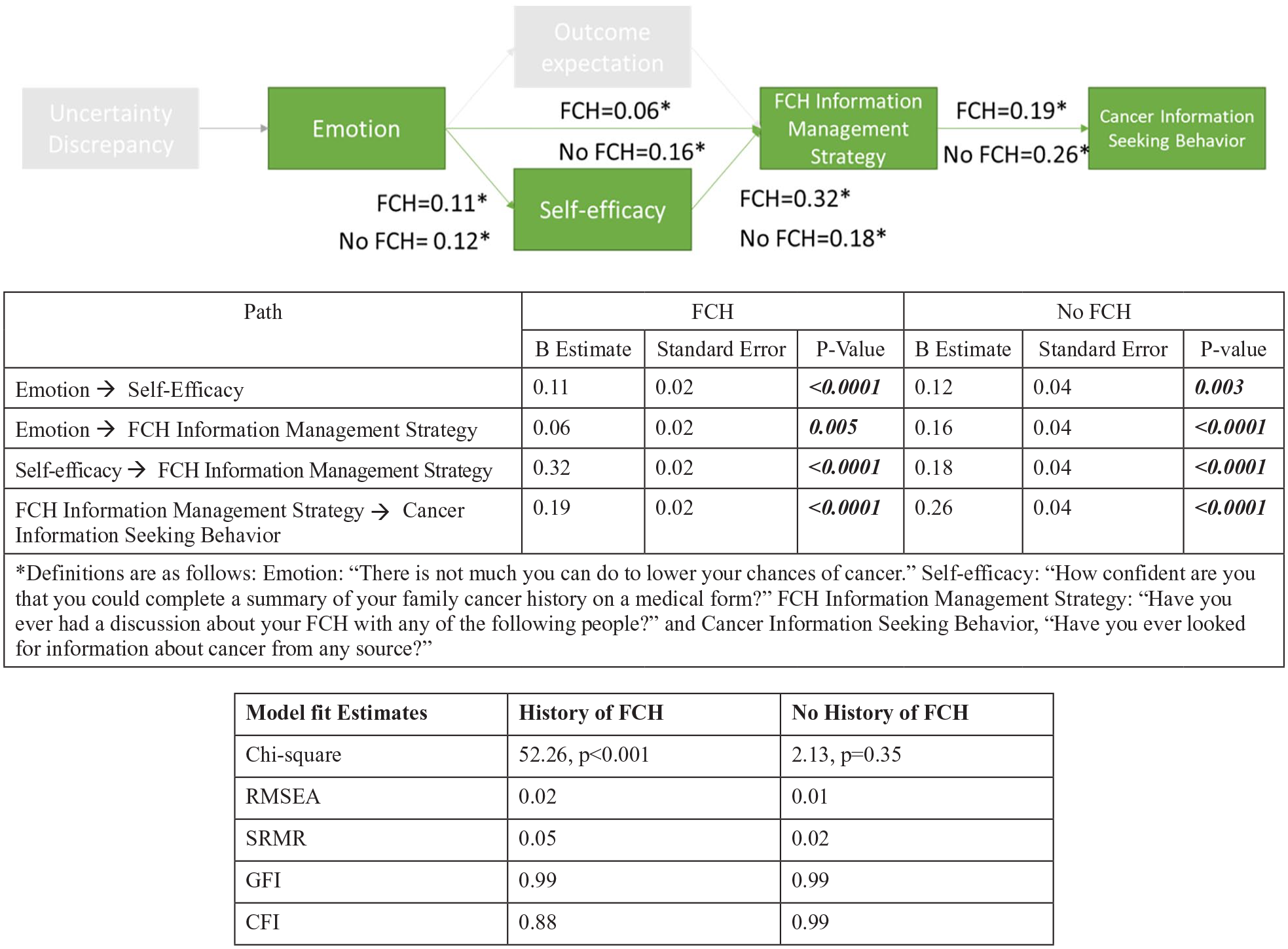
Testing the Stratified Path Model by Family History of Cancer.
Stratification by Age
We stratified by age using the age groups 18 to 34 and 35 years or older (Figure 3). The stratified models were similar with the exception of the relationship between belief in ability to lower chances of cancer (emotion) and likelihood to discuss FCH (FCH information management strategy). Among younger individuals (less than 34 years old), there was no significant association between this belief and likelihood to discuss FCH (B = −0.01, p = .8869); however, among those who are older than 35, there was a significant association between belief in ability to lower chances of cancer (emotion) and likelihood to have sought FCH (FCH information management strategy; B = 0.08, p < .0001). Both models showed good model fit.
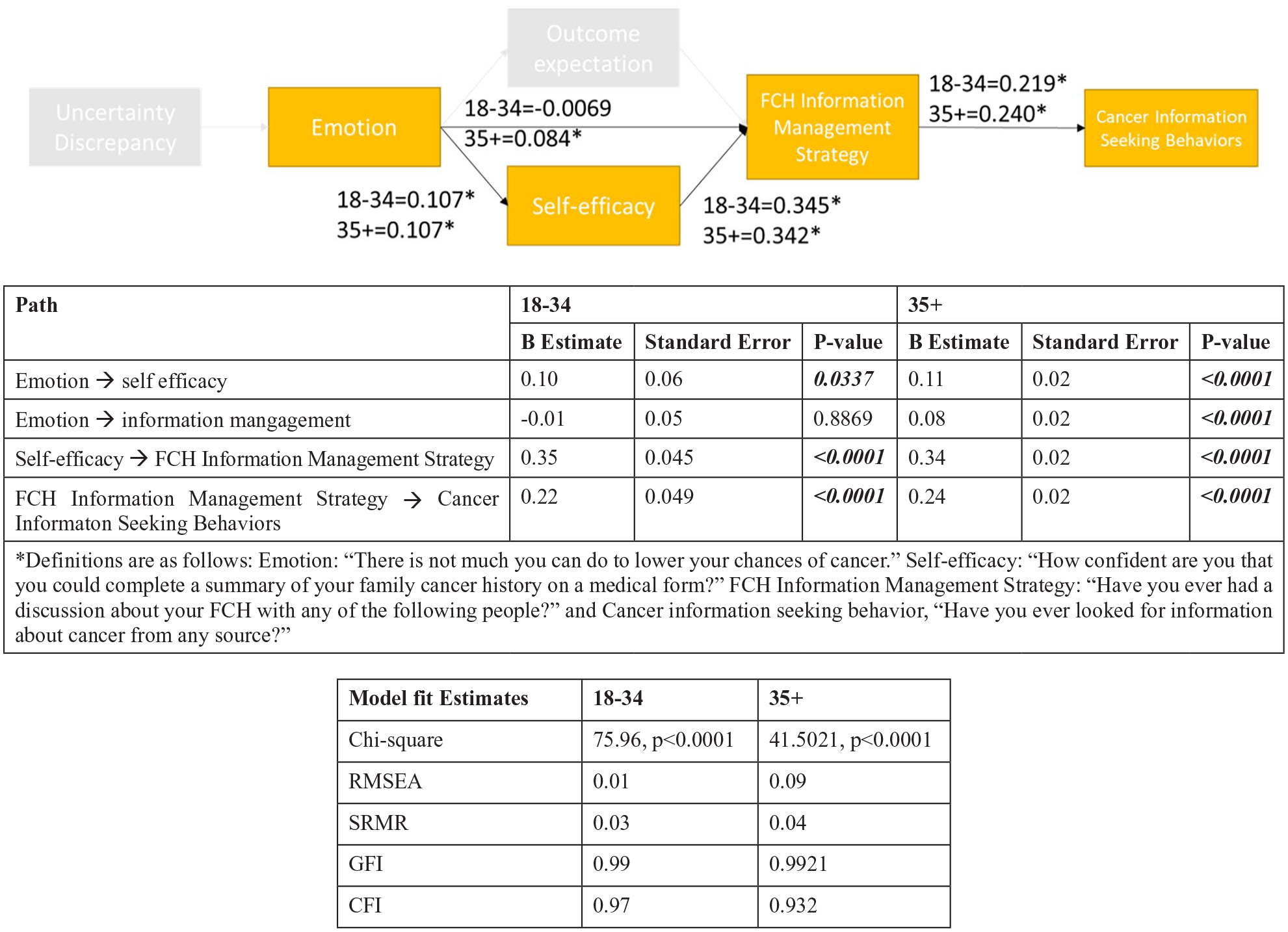
Testing Stratified Path Model by Age.
Stratification by Race/Ethnicity
The stratified models show differences by race and ethnicity (Figure 4). Perceived ability to reduce cancer risk (emotion) was associated with confidence in the ability to complete FCH (self-efficacy) among Whites (B = 0.09, p = .0004) and Hispanics (B = 0.02, p < .0001) but not among Blacks or Other. Perceived ability to lower chances of cancer (emotion) were associated with likelihood to discuss FCH (FCH information management strategy) among Whites (B = 0.07, p = .0027) but not significantly among other races and ethnicities. Confidence in ability to complete a FCH (self-efficacy) was associated with likelihood to discuss FCH (FCH information management strategy) among all races. Likelihood to discuss FCH (FCH information management strategy) was positively associated with cancer information-seeking behaviors among all races. Model fit was decent across each of the four race models.

Testing the Stratified Path Model by Race/Ethnicity.
Stratification by Gender
When stratifying by gender, perceived ability to lower chances of getting cancer (emotion) was significantly associated with confidence in the ability to complete FCH (self-efficacy) for both males (B = 0.09, p < .0001) and females (B = 0.12, p = .003). Perceived ability to lower chances of getting cancer (emotion) were associated with likelihood to have discussed FCH (FCH information management) among males (B = 0.14, p < .0001) but not females (B = 0.03, p = .179). Confidence in ability to complete FCH (self-efficacy) was associated with likelihood to have discussed FCH (FCH information management strategy) among both males and females, and likelihood to have discussed FCH (FCH information management strategy) was associated with cancer information-seeking behaviors among both males and females (Figure 5).

Testing the Stratified Path Model by Gender.
Discussion
The goal of this article was to better understand the factors that influence conversations about FCH and how steps in the process of seeking FCH information may encourage other cancer information-seeking behaviors. We used the TMIM, an established framework that describes the process individuals go through when seeking health information such as FCH to help understand these relationships.
Consistent with previous studies, we found that women, married people, those with a higher income, non-Hispanic Whites, and college graduates were more likely to collect FCH and seek cancer information (Finney Rutten et al., 2016; Rutten et al., 2006). Those less likely to seek this type of information include men, single individuals, non-White individuals, and those with lower health literacy. Recognizing that certain sociodemographic characteristics are associated with a decreased likelihood of discussing FCH could help providers identify and support patients who may need additional encouragement. In addition, health education efforts could be designed to help ensure that materials are available for these audiences (i.e., educational materials specifically designed for individuals with lower literacy; Ruffin et al., 2011). Some efforts have been undertaken to develop tailored materials for specific audiences; however, more resources and materials along with increased dissemination efforts to promote these resources can help those who may be reluctant to collect FCH and seek cancer information (Senier et al., 2015).
Our path model demonstrated that those who believe cancer prevention is possible (emotion) are more likely to have higher confidence in their ability to complete FCH (self-efficacy), which was in turn associated with discussing FCH with family members (FCH information management strategy). Those who discussed FCH with a family member were also more likely to seek additional cancer information. Findings support that gathering FCH involves multiple steps and requires individuals to make decisions throughout this process. Each of the proposed steps is affective, or related to an emotion, rather than cognitive or related to the process of thought or reason. Affective attitudes have been shown to be significantly more powerful predictors of health behaviors, such as FCH collection (Lawton et al., 2009). Interventions that appeal to these affective or emotional responses are commonly used to address various health behaviors and may be an especially effective approach to encourage FCH collection (Ferrer & Mendes, 2018; Slovic et al., 2005). In addition to these affective constructs, there may also be cognitive or functional steps necessary to collect FCH. For example, even if an individual has high levels of self-efficacy or belief that they are able to complete their FCH, practically speaking this requires individuals to have information about specific members of their family and then be able to use this information to complete a tool (Foster et al., 2002; Kelly et al., 2007; Wang et al., 2011). Thus, there may be important additional steps beyond decisions related to FCH information management strategy to consider, such as whether the individual collected FCH using a FCH tool and the accuracy and completeness of FCH.
Stratified models provided insight into the process of FCH gathering and other health-seeking behaviors. The majority of our sample (69.86%) reported a family history of cancer. In bivariate associations, we found that, compared with those who never discussed FCH with a family member or health care provider, those who discussed FCH with more than one person were significantly more likely to have a family history of cancer. Relatedly, bivariate models showed differences in cancer seeking behaviors among those with and without a family history of cancer. However, results from our stratified path models did not show differences in the process of FCH gathering or information seeking between those with and without a family history of cancer. In models for individuals with and without a family history of cancer, all aspects of the path model were significant and positively associated with each other, with only slight differences in beta values between each construct. Thus, our results indicate that individuals with and without FCH go through a similar process when deciding whether to discuss FCH with family members or seek information about cancer. Previous studies indicate that a family history of cancer is positively associated with screening outcomes for related cancers (e.g., if an individual has a relative with family history of colorectal cancer they are more likely to have received colorectal cancer screening; Beydoun & Beydoun, 2008). However, other studies have found that prior personal or family experience with cancer does not have a substantial influence on outcomes related to FCH gathering. For example, past studies using the HINTS data set found that family history of cancer was unrelated to the perceived importance of family history (Allen et al., 2018) and unrelated to information avoidance or information seeking behaviors (Emanuel et al., 2015). These findings align with results from our full model.
Other noteworthy findings include the difference in the effect of the belief that cancer prevention is possible (emotion) on the likelihood to discuss FCH (FCH information management strategy) and seek cancer information by race/ethnicity, gender, and age. The belief that cancer prevention is possible was significantly associated with the likelihood to discuss FCH (information management) among non-Hispanic Whites, men, and those older than age 35 but not among non-Hispanic Blacks, Hispanics, women, and those aged 18 to 34. A previous study using 2013 HINTS data found that non-Hispanic Whites and men were most likely to perceive family health history as not important to their health. The study found that cancer-related perceptions were important predictors in likelihood to perceive family health information as important, and our finding that belief that cancer prevention is possible (emotion) increases the likelihood of FCH discussions with family members among men and non-Hispanic Whites extends these findings. Targeted messages that emphasize how knowledge of FCH could help in preventing cancer may be a useful approach to encourage men to collect their family health history information. It is still unclear whether these messages would be less effective in reaching others with lower rates of FCH collection, including non-Hispanic Blacks, Hispanics, and younger individuals (Halbert et al., 2016). Further exploration of motivators in these populations is warranted.
Our study validates previous findings that the likelihood to collect FCH (information management strategy) was a strong and consistent predictor of other cancer information-seeking behaviors, using a large national sample (Sedrak et al., 2020). These findings support the approach of combining FCH messages with health-seeking messages, for example, incorporating messages about the importance of FCH in places individuals commonly go to seek health information (e.g., internet and provider’s offices). Future studies could further assess what types of health seeking are most likely to be associated with, as individuals can seek information from a variety of sources (e.g., health professionals, internet, and radio; Sedrak et al., 2020).
Our study had some important limitations. The HINTS questions were not designed with TMIM in mind. We used questions from the HINTS data set that aligned as closely as possible with each of the proposed constructs, but questions might not be optimal for measuring the construct. For example, our final models did not include knowledge of FCH (uncertainty discrepancy). According to TMIM, this is an important cue to action and the first step in the process of information gathering. However, uncertainty discrepancy caused poor model fit and was removed from the model. This may have been because the type of question used to assess uncertainty discrepancy (“How well do you know your family’s history of cancer”) did not accurately depict the intended construct. Relatedly, alternative conceptual models could have been considered (e.g., stages of change), possibly resulting in different outcomes. In addition, TMIM is designed to examine a series of linear, sequential steps, using longitudinal data collected from the same individual at multiple time points. However, our data were cross-sectional, so we were unable to assess whether events occurred in the order assigned by TMIM or if some relationships might be reversed. The lack of longitudinal data to appropriately assess the linear relationship of variables is a common challenge when assessing conceptual models. For example, individuals who have high confidence in their ability to complete FCH (self-efficacy) were predicted to be more likely to discuss FCH with family members. It is possible that confidence in the ability to complete FCH (self-efficacy) follows from having already discussed FCH with family members. However, this is a first step toward better understanding the relationships proposed. Finally, we excluded “a health care provider” from the response options for discussions about FCH (information management strategy) because we wanted to focus on discussions with family members. However, the health care provider was a response option for those who indicated that they only discussed FCH with one person (N=242), and the response option “more than one person selected” likely included a health care provider in many cases.
FCH collection is a multi-step process that is influenced by the perceived importance of getting information about the family history of cancer, family dynamics, and the emotional burden associated with gathering this information. Public health efforts to increase awareness and collection of family health history information can be hindered by the limited understanding of the steps involved in this process. Assessing the steps involved, their relationships, and the effect of sociodemographic factors may provide important information that can help refine and target efforts to improve FCH collection. Given the strong association between discussions about FCH information and cancer information-seeking behaviors, messaging could be targeted to sources individuals commonly go to when seeking health information (e.g., health care providers and other trusted information sources). Emphasizing appropriate messages for specific audiences may increase the likelihood that individuals will be motivated to learn about and record their FCH.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Caitlin G. Allen is now affiliated to Department of Public Health Sciences, Medical University of South Carolina, Charleston, SC, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Caitlin G. Allen received support through K00CA253576.
Availability of Data and Materials
Data are available from a publicly available source (HINTS).
Code Availability
Code available upon request to corresponding author.