
Abstract
This study focuses on the mechanisms by which professional service providers effectively influence customers to adhere to their expert guidance and advice. Eliciting customer adherence is a critical concern for professional service firms since customers of these need-based (rather than want-based) services are often reluctant to adhere, and nonadherence can result in serious negative consequences to customer well-being and firm resource utilization. The study examines this scenario by developing a conceptual framework that integrates the following three theoretical areas: professional services theory, advice utilization theory, and social cognitive theory. The framework proposes associations between professional service provider actions and customer reactions, including adherence to expert advice, adherence intentions, and organizational resources needed to serve the customer (time cost and monetary cost). The study empirically tests the hypothesized relationships based on professional service provider-customer (physician-patient) interactions in a large health care organization setting using both primary survey data and objective, longitudinal customer data encompassing a 48-month period. Results indicate that advice giving frequency and focus on negative consequences impact customer outcomes and the effects are moderated by perceived customer efficacy and service provider efficacy. The findings shed light on the underlying dynamics of customer adherence to advice in professional service settings and provide guidance as to how that adherence can be effectively elicited.
In a number of professional service contexts, negative outcomes may result when customers do not act on or adhere to the expert advice of service providers. As examples, customers may face suboptimal returns or even losses if they ignore investment portfolio advice from their financial planner; customers risk complicated tax scenarios if they do not maintain detailed income and investment records as recommended by their certified tax accountant; and patients risk developing or exacerbating chronic diseases if they ignore their physician’s guidance related to diet, exercise, tobacco use, or medication. When well-reasoned expert advice is not followed, customers’ well-being may be compromised and additional resources from service organizations may be required to manage consequences that might have been prevented.
Professional services typically involve customized expert guidance and require interdependence between customers and service providers for beneficial outcomes (Chan, Yim, and Lam 2010). Mills and Morris (1986) refer to these as complex services, where customers share some responsibility for outcomes. Consequently, professional service providers’ success in influencing customer behavior is contingent on the willingness and ability of the customer to engage in the recommended behaviors. Financial planners are often unsuccessful in persuading clients to change habitual overspending behaviors, for example (Grubman, Bollerud, and Holland 2011).
The fundamental nature of professional services can create a challenge for service providers who offer expertise-based guidance. While some professional services can be viewed as a want service, which is a discretionary service that offers some level of intrinsic or hedonic appeal, many professional services are services that customers need but may not want and, in fact, may avoid using or fail to follow through on their responsibilities when they do use them (Berry and Bendapudi 2007). The possibility of customer reluctance for need services is salient in that customers may not accept the participant role and may not adhere to the service provider’s expert advice that is necessary for a positive outcome or result (Bendapudi and Leone 2003).
It is not fully known under what conditions customer motivation to adhere to service provider advice may be offset by customer reluctance to invest required resources, including time, physical, and cognitive effort (Buttgen, Schumann, and Ates 2012; Dellande, Gilly, and Graham 2004). Empirical evidence of the effects of specific professional service provider approaches on customer behavioral outcomes is limited and, within existing studies, research is equivocal in terms of what factors determine whether professional service customers do or do not follow advice.
We examine three interrelated research questions to address these knowledge gaps. First, is there a relationship between the frequency with which a professional service provider advises a customer (recommends specific actions) and subsequent customer outcomes? Second, how are customer outcomes influenced by the focus of the advice, such as explaining potential negative consequences of certain behaviors? Third, do customer efficacy and service provider efficacy—the presence of belief in a successful outcome—moderate the relationship between service provider expert advice and customer outcomes? In combination, these questions allow us to identify the mechanisms by which professional service providers influence customer adherence to expert advice.
The contributions of our research are highlighted in Table 1, which compares our research to studies across a variety of contexts and disciplines that examine expert professional service provider-customer interactions. We link professional services theory to theoretical perspectives from the advice taking literature, using social cognitive theory to explain important boundary effects and proposing what is, to our knowledge, the most theory-based conceptualization of how professional service providers motivate adherence to expert advice. We apply this integrated framework to examine novel factors related to advice giving and taking in professional service contexts. As indicated in Table 1, no prior research has examined the effects of advice giving frequency or service provider focus on negative consequences of nonadherence. No known studies have examined customer outcomes capturing adherence to advice or adherence intentions. We know of only one recent study that examined efficacy (self and other) as a moderating variable (Yim, Chan, and Lam 2012), but effects were tested with self-report outcome measures and cross-sectional data.
Empirical Studies of Professional Service Provider-Customer Interactions and Related Customer Outcomes.
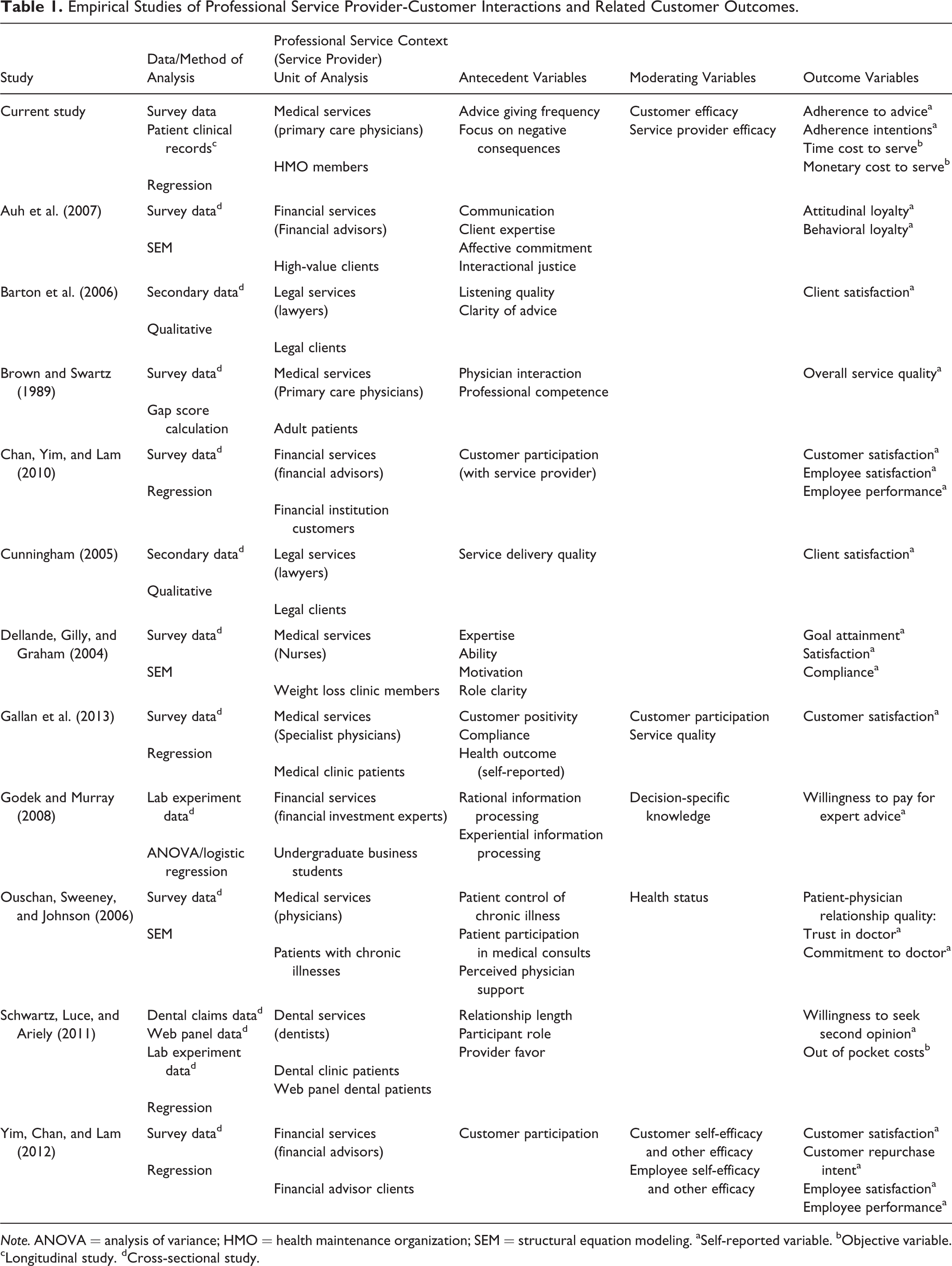
Note. ANOVA = analysis of variance; HMO = health maintenance organization; SEM = structural equation modeling. aSelf-reported variable. bObjective variable. cLongitudinal study. dCross-sectional study.
Empirically, our research contributes by testing our framework with a longitudinal study based on a unique data set comprising individual-level perceptual data and objective service utilization data. This longitudinal approach is critical for making causal inferences about how service providers influence customer adherence over time; a cross-sectional study alone cannot capture this. Our use of objective outcome data, in addition to self-reported, perceptual customer outcomes, allows us to examine unbiased, objective measures that capture actual service utilization behavior. We are aware of only one other study (Schwartz, Luce, and Ariely 2011) that examines objective outcomes but none that examine objective outcomes capturing time and monetary costs resulting from client nonadherence. In this research, we identify important approaches that professional service providers can leverage to influence customer behavior and increase adherence to expert advice. Increased adherence not only improves customer well-being but also helps sustain organizational resources that otherwise could be lost due to customer nonadherence.
In the sections that follow, we present a conceptual framework, develop a set of hypotheses integrating theoretical perspectives, and report empirical analyses that test the predicted relationships. We examine customer adherence to service provider expert advice in a medical setting where the primary care physician plays a role in influencing patient health behaviors. Specifically, we investigate the degree to which physician approaches motivate more healthful patient diet and exercise behaviors and impact subsequent use of related health care resources. The medical setting is appropriate because research indicates that patients are often reluctant to adhere to physicians’ expert advice regarding detrimental health behaviors, and nonadherence has a clear impact on both patient well-being and future need for health care resources (DiMatteo 2004; Gigerenzer et al. 2008). Further, a significant stream of research has established the relevance and importance of service quality theory in health care contexts and the role of interpersonal interaction between the health care provider and the patient in achieving desired outcomes (e.g., Dagger and Sweeney 2007; Dagger, Sweeney, and Johnson 2007; McColl-Kennedy et al. 2012). The economic impact of medical costs has created an imperative of better resource management and the prevention of negative outcomes—as an alternative to the treatment of negative outcomes—is a widely acknowledged priority by medical service organizations (e.g., Blumenthal 2012; Woolf 2008).
Conceptual Framework and Research Hypotheses
Our conceptual model, shown in Figure 1, is designed to explain scenarios in which a professional service provider offers specific behavioral advice that the customer may or may not adhere to in the future. By examining important moderators of the expert advice-customer adherence relationship, we consider contingencies that can help us gauge when advised customer behaviors are likely to be motivated and when they are not.
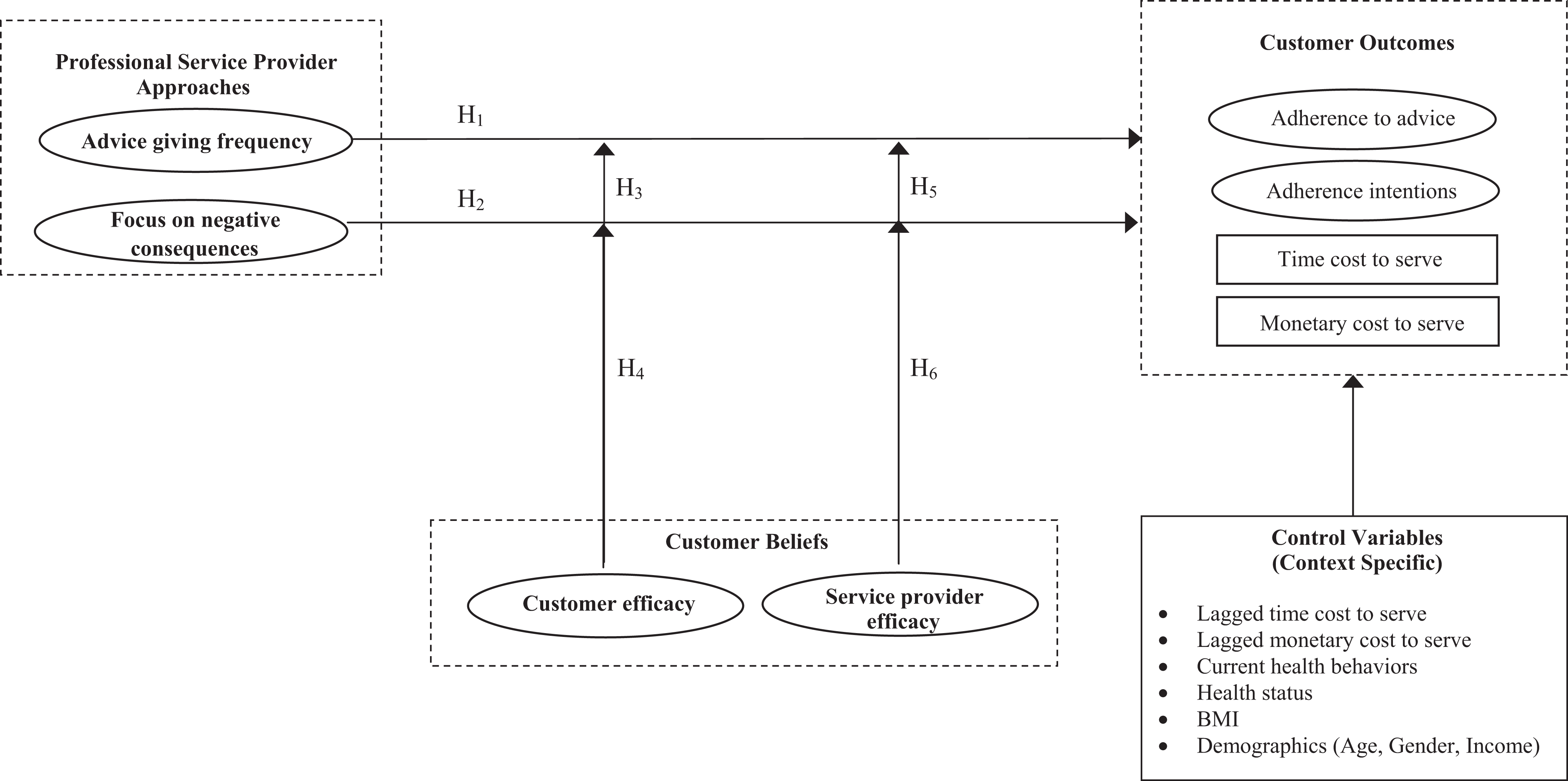
Proposed conceptual model of the effects of professional service provider approaches on customer outcomes.
We propose that two critical determinants of adherence to expert advice are advice giving frequency and focus on negative consequences of not adhering to the advised behaviors. We also propose that both customer efficacy and service provider efficacy will act as moderators of the relationships between these determinants and customer outcomes, after explicitly controlling for their direct (i.e., main) effects. Customer efficacy we define as a customer’s belief that he or she is able to engage in the behaviors advised by the service provider. Service provider efficacy we define as a customer’s belief that the professional service provider is able to effectively help the customer engage in the advised behaviors.
We consider a set of four customer outcomes, comprising two perceptual outcomes adherence to advice and adherence intentions and two objective outcomes that capture firm resources required to provide related services to the customer (time cost and monetary cost). We define adherence to advice as the extent to which the customer has followed the advice of the service provider and define adherence intentions as the extent to which customers plan to adhere to service provider advice in the future. Time cost to serve we define as how many times a customer required related services. Monetary cost to serve we define as the financial expenditures required to cover related customer services. These objective variables ostensibly are influenced by the extent to which customers do or do not adhere to the expert advice, and the resource costs to the organization reflect the provision of services that may not have been required if customers had adhered to professional advice.
The conceptualization in Figure 1 is based on the integration of three distinct theoretical streams: professional services theory, advice utilization theory, and social cognitive theory. Professional services theory helps to establish and explain key attributes of the exchange relationship between the expert provider and the customer that determine critical service outcomes (Chan, Yim, and Lam 2010; Von Nordenflycht 2010). We define professional services as labor-intensive performances informed by complex knowledge, provided by a highly educated, formally credentialed workforce (see Greenwood et al. 2005). Torres (1991) identified the main features of a profession as a specific knowledge base and the regulation and control of its application, and Von Nordenflycht (2010) identifies knowledge intensity and a professionalized workforce as distinguishable characteristics of professional service firms. High-value professionals who embody the intellectual capital of the firm are at the front line of the service exchange so the norm is an asymmetry of expertise (Von Nordenflycht 2010, 2011). Professional service providers form the basis of an organization’s relationships with customers who often view their primary allegiance as to the service provider rather than to the organization (see also Greenwood et al. 2005). This type of allegiance is facilitated by the consistent level of member competence and expertise maintained through professional education and licensing procedures. Public knowledge of professions’ legal and regulatory controls creates a mechanism that signals reliability and trustworthiness to consumers (Von Nordenflycht 2010; Zucker 1986).
Advice utilization theory explains critical factors that influence how customers perceive advice and the determinants of whether they use or do not use advice offered by professional service providers (Bonaccio and Dalal 2006). Factors include characteristics of the advisor (i.e., professional service provider), the advice recipients, and the specific type of advice received (Sniezek, Schrah, and Dalal 2004, Tost, Gino, and Larrick 2012; Yaniv 2004). Following the advice taking literature, we define advice utilization as “the extent to which a client follows advice” (Bonaccio and Dalal 2006). Client utilization of advice is critical to business relationships due to the complexity of information necessary to support decisions and actions in professional services contexts (Godek and Murray 2008; Jonas and Frey 2003; Sniezek, Schrah, and Dalal 2004).
The moderating effects we propose are consistent with social cognitive theory, specifically research on social exchange related to self-efficacy and other efficacy (Bandura 1986; Lent and Lopez 2002, Vancouver et al. 2002). Social cognitive theory posits that beliefs about self-efficacy influence the probability of an individual initiating a certain behavior and then continuing the efforts despite the presence of barriers or hardship (Bandura 1986). Self-efficacy beliefs help to determine not just persistence of actions but also how much effort is expended. According to social cognitive theorists, who emphasize the role of social influence, in a close customer-employee relationship, the perceived capabilities of relationship partners, or other efficacy, matters in addition to self-efficacy (Bandura 1997, 2001; Yim, Chan, and Lam 2012).
Advice Giving Frequency
We define the construct of customer perceptions of advice giving frequency as the incidence of provider-customer interactions in which expert advice is provided. Bonaccio and Dalal (2006) assert that advice utilization is influenced by the quantity of interaction between the service provider and the client. Cues clients receive during face-to-face interactions with service providers create perceptions of trustworthiness, and trust is an established predictor of advice acceptance and subsequent behavior (Schwartz, Luce, and Ariely 2011; Sniezek and Van Swol 2001; Van Swol and Sniezek 2005). Zucker (1986) conceptualizes process-based trust as a product of interpersonal interactions, reputation, and general signs of professionalization.
The marketing literature reports that professional service provider-customer interactions help establish strong relationships, clarify expectations, and motivate involvement in the service (Auh et al. 2007; Dellande, Gilly, and Graham 2004; Hibbert, Winklhofer, and Temerak 2012). These interactions and the trust that often develops lead the exchange parties to feel bound and to demonstrate reciprocity (Luo 2002). Reciprocity motivates customers who are provided with expert guidance to dedicate resources such as time and effort toward adhering to service provider advice (Sniezek, Schrah, and Dalal 2004).
Studies from specific professional domains, for example, law, medicine, and financial services, report that increased discussion and “time to talk” are critical attributes associated with adherence to service provider advice (Cunningham 2009; Vick and Scott 1998; Zolnierek and DiMatteo 2009). There is mixed empirical evidence, however, as studies also report weak or insignificant relationships between expert guidance and customer outcomes due to intervening barriers (Bardia et al. 2007; Moore et al. 2003). Nevertheless, following theory from social psychology and other disciplines and research results that show improved outcomes from increased expert service provider counsel (Cunningham 2009; Makoul and Curry 2007), we propose that advice giving frequency will positively affect perceptual assessments such as adherence to advice and adherence intentions.
Concerning our objective outcome variables, we predict that advice giving frequency due to actual differences in adherence (i.e., changes in health behavior) will reduce the organization’s costs to serve (both time cost and monetary cost). We draw our support from the medical literature (where research is evidence-based and rarely theoretical in nature). Numerous medical studies show that adhering to a healthful diet and a regular physical activity regimen reduces patient health risk, ultimately conserving health care resources (Manson et al. 2004; Pronk 2012). Insufficient physical activity and poor diet are two of the four modifiable risk factors associated with approximately 40% of preventable mortality in the United States (McGinnis, Williams-Russo, and Knickman 2002). Studies have found that counseling patients about diet and exercise was associated with positive improvements (Durant et al. 2009; LeBlanc et al. 2011; Loureiro and Nayga 2006; Post et al. 2011), and medical experts argue that physician counseling of patients in face-to-face clinical encounters is instrumental to efforts to improve patient health behaviors (White and Danis 2012). Following these arguments and prior empirical findings, we hypothesize:
Focus on Negative Consequences of Customer Behavior
We define the construct of focus on negative consequences as a service provider’s emphasis of potential adverse customer outcomes likely if advice is not followed. In a professional services encounter, the focus of advice or guidance provided may be an integral determinant of customer outcomes (Brotman 2009; Gallan et al. 2013). In the context of ongoing relationships, valued in complex professional services, information asymmetries encourage customers to rely on specific knowledge provided by the expert provider (Schwartz, Luce, and Ariely 2011). Dalal and Bonaccio (2010) report that there are varying types of advice and that recommending against a particular action or behavior—as is the case in discussing negative outcomes of unadvised behaviors—is a type that some consumers prefer. Discussing negative consequences requires the communication of relevant domain-specific information about varying courses of action, an advice type highly valued by consumers (Dalal and Bonaccio 2010; Van Swol and Sniezek 2005).
The effects of information about risk and negative consequences on motivation have been explored in the consumer behavior literature through the study of psychological mechanisms. Communicating the potential for negative consequences can offset customers’ self-positivity bias and weaken beliefs of invulnerability, thereby motivating behavioral change (Brewer et al. 2004; Menon, Block, and Ramanathan 2002). For example, attorneys who use this approach to demystify the implications of specific legal decisions for their clients are likely to motivate client behavior that adheres more closely to attorney counsel (Brotman 2009). Some research suggests that medical customers who understand the implications of risks related to behaviors are more likely to follow, rather than disregard, service provider advice (Allegrante et al. 2008; Bowman, Heilman, and Seetharaman 2004; Luce and Kahn 1999; Post et al. 2011).
To some degree, research results are equivocal in providing evidence that advising customers of potential consequences influences their behaviors (Bendapudi and Leone 2003; Yim, Chan, and Lam 2012). Professional service provider advice designed to convey the negative consequences of certain behaviors may not only be complicated but also be particularly difficult to implement (Berry and Bendapudi 2007). In the medical provider-customer context, advised changes in health behaviors may seem onerous as hedonic goals can compete with health goals. The customer may also be uncertain that changes in behavior, even if achieved, will substantively improve health (Wiseman, Cuevas-Rodríguez, and Gomez-Mejia 2011). Also, if expert advice about potential threats is perceived as a restriction of freedom, it may bring about the negative psychological state of reactance and lead to an outcome opposite of the one intended (Dalal and Bonaccio 2010). Such barriers to advice adherence may explain why communicating potential adverse effects of particular behaviors has had limited success in motivating behavioral change in some contexts (e.g., smoking, sedentary behavior; Woolf 2008).
Acknowledging that service providers must present a convincing case relative to potential negative consequences, and noting the mixed evidence, we follow advice utilization and risk-related consumer behavior theories as well as research evidence from multiple fields to predict that focus on negative consequences will have positive impact on both perceptual and objective outcomes. As such, we hypothesize:
Moderating Effects on Customer Outcomes
While our proposed hypotheses predict direct effects of advice giving frequency and focus on negative consequences, the mixed nature of prior research findings suggests that important moderating factors may be at work. A principal research question then becomes, what makes the frequency and focus of the advice more or less effective in professional service contexts? Individual consumer characteristics and perceptions often moderate the relationship between service provider-customer communication and customer behaviors (Cunningham 2009; Franciosi et al. 2004; Keller and Lehmann 2008; Keller, Lipkus, and Rimer 2002). We follow social cognitive theory in proposing that customers’ perceptions of their own efficacy affect the relationship between service provider advice and customer outcomes that reflect adherence to that advice (Bandura 2001). Following advice utilization theory, we propose that customers’ perceptions of their service provider’s efficacy also affect the advice-customer adherence relationship.
Customer Efficacy
Although service provider advice is informed by specialized expertise, customers may be reluctant to adhere to advice because of the nonmonetary costs involved (time, effort, and hedonic deprivation) and overall inertia related to the interruption of habitual behaviors. These factors underscore the established role of perceived self-efficacy in overcoming reluctance and facilitating behavioral change (Bandura 2005). Self-efficacy has a strong association with optimism, that is, the belief that goals can be achieved despite obstacles (Peterson 2000). Individuals are likely to be more motivated to take specific actions when they perceive their resource investments will result in desired outcomes (Buttgen, Schumann, and Ates 2012). Customer efficacy is an individual characteristic categorized as state like or open to development (as opposed to trait like, or relatively difficult to change; Luthans et al. 2007). The malleable nature of customer efficacy suggests that it can not only be identified but also be influenced and encouraged.
We propose that customer efficacy plays a role in determining whether the frequency of advice and focus on negative consequences results in desired adherence behavior. This is consistent with the social cognitive theorists’ arguments that self-efficacy’s influence on behavior not only is direct but also impacts other antecedents that facilitate or inhibit behaviors (Bandura 2005). For a high-efficacy customer, the effect of focusing on negative consequences should be enhanced because confidence and positive outcome expectations will motivate action as well as reinforce resilience (Bandura 1986).
While the positive relationship between self-efficacy and performance is established in social psychology research, a growing number of rigorous studies report a negative relationship between the variables (Moores and Chang 2009; Vancouver et al. 2002; Vancouver, More, and Yoder 2008). Self-efficacy theory posits that consumers with high self-efficacy allocate more resources to a task, thus strengthening their performance (Bandura 1997; Vancouver et al. 2002). However, higher self-efficacy can also lower a consumer’s perceived need to allocate time and effort to a goal or behavior (Vancouver, More, and Yoder 2008). Moores and Chang (2009) find that overconfidence explains this negative impact of self-efficacy. Like Vancouver et al. (2002), they use perceptual control theory to explain why a high level of self-efficacy can produce an inaccurate belief that a certain goal state has been achieved, resulting in decreased effort and performance. This negative impact of overconfidence is similar to the phenomenon of egocentric advice discounting studied in the advice literature, where overconfidence drives consumers to exaggerate their status and limits their efforts to achieve goals (Yaniv 2004).
While recognizing the importance of studies that show negative effects of self-efficacy, our predictions take the more traditional perspective that self-efficacy will positively influence the relationship between expert advice and customer adherence to it. In line with this, we hypothesize the following:
Service Provider Efficacy
A second individual characteristic that we propose as a moderator of service provider advice on customer adherence is perceived service provider efficacy, that is, the service provider’s ability to effectively help the customer adhere to the advised behaviors. Two interrelated elements can contribute to this variable: heterogeneity in customer predisposition to being positively affected by a service provider and variation in the ability of professional service providers to demonstrate a level of efficacy that influences customer behaviors.
Lent and Lopez (2002) argue that the interpersonal dimension in relationships warrants consideration of efficacy beliefs about the other party in the relationship as well as about the self. They conceptualize other-efficacy beliefs as a person’s perceptions about another person’s ability to perform particular behaviors and assert that beliefs about the efficacy of the other person can affect whether a response is positive or negative. This perspective is supported by social cognitive theory, which suggests that customer perceptions of service provider capabilities strongly influence behaviors and facilitate more desirable outcomes (Bandura 1997, 2001; McLaughlin, Yang, and van Dierdonck 1995; Yim, Chan, and Lam 2012).
Jodlbauer and Jonas (2011) cite empirical evidence linking perceived service provider competence to customer trust and integrity as well as to advice utilization. Other studies have associated perceptions of capability with interpersonal influence in psychological and behavioral outcomes such as compliance and task performance (Auh et al. 2007; Dellande, Gilly, and Graham 2004; Hibbert, Winklhofer, and Temerak 2012). Referencing an example of Lent and Lopez (2002), a client’s favorable assessment of a therapist’s efficacy can result in an enhanced working relationship and stronger commitment and involvement in the therapeutic process.
Like customer efficacy, service provider efficacy is open to development and can be influenced. In summary, we predict that customer perceptions of a particular service provider’s ability to effectively influence behavior should affect customer adherence to expert advice. Confidence in the service provider, similar to confidence in oneself, limits the impact of uncertainty and creates motivation and the expectation of a positive outcome. As such, we offer these hypotheses:
Research Methodology
Data
We empirically test our hypotheses in a health care setting where the medical service provider (primary care physician) offers advice for customer (patient) health behaviors. Health care is a service in which patients often fail to comply with their physician’s advice even though nonadherence may adversely impact their personal well-being and health care resource utilization. The primary health care context is also a strong exemplar of the principal characteristics of professional services. Health care services are highly knowledge intensive and involve a professional workforce.
Our research design combines survey data that capture patients’ self-reported health behaviors and perceptions of their primary health care service provider with 48 months of individual-level data on the time and monetary costs of providing the patients’ health care services. To collect the data, we worked with a health maintenance organization (HMO) that operates medical clinics and hospitals in the southwestern United States and is one of the largest HMOs in the country. The HMO provided contact information for 5,775 of its members. Our survey sampling frame included randomly selected individuals who were current members of the HMO health plan, were at least 18 years old, were not employed by the HMO, and had visited one of the service provider’s medical offices in the prior 2 years. The contact information included a unique identification number and e-mail address for each member.
We sent e-mail messages to the full sampling frame, with a letter from the HMO Health Plan’s CEO inviting potential respondents to participate in an online survey and offering a US$10 coupon for use at any of the HMO’s pharmacies upon completing the survey. We conducted a total of three follow-ups. In the first two, we e-mailed nonrespondents after 2-week intervals, augmenting the offer with an opportunity to participate in a drawing to receive a US$50 gift card. In the third and final follow-up, nonrespondents were contacted by telephone 2 to 3 days before the e-mail was sent to convey the importance of their input to the study. We ultimately received a final sample of 2,205 usable responses, after eliminating data from 87 respondents who provided incomplete information, for a response rate of 38%. The respondents were primarily female (70%) between the ages of 35 to 65 (77%), with at least some college education (69%) and an average household income exceeding US$50,000 (95%).
We matched the survey responses with corresponding objective data from the HMO’s patient clinical records using the unique ID number assigned to each member in the sampling frame. The database comprises a total of 48 months (24 months pre-survey and 24 months post-survey) of individual-level data including physician office (primary care and specialists), emergency room, and hospital visits, health care service provider costs to provide treatment, and demographic information. While the data we received included only an encrypted patient ID and not patient or physician names or other identifying information, we took special precautions to protect the data due to privacy concerns. The procedures for collecting, managing, and analyzing the data received approval by both the university’s and HMO partner’s institutional review boards. Combining the perceptual data from our survey responses at the individual patient-level with 48 months of objective clinical data is key to our research design in that it allows us to perform a longitudinal analysis of the proposed effects on two objective outcomes capturing the time and monetary costs to serve the customer.
Construct Measurement
We examined four outcomes as a function of two service provider approaches—advice giving frequency related to customer diet and exercise behaviors and the service provider’s focus on negative consequences of poor health behaviors to the customer—and two moderators—customer efficacy in engaging in healthful diet and exercise behaviors and service provider efficacy in helping the customer to engage in those behaviors. We describe each of these variables subsequently and offer additional detail on the variables’ measurement in the Appendix. Descriptive statistics and construct correlations for the key variables are presented in Table 2.
Descriptive Statistics and Correlation Matrix for Key Constructs.
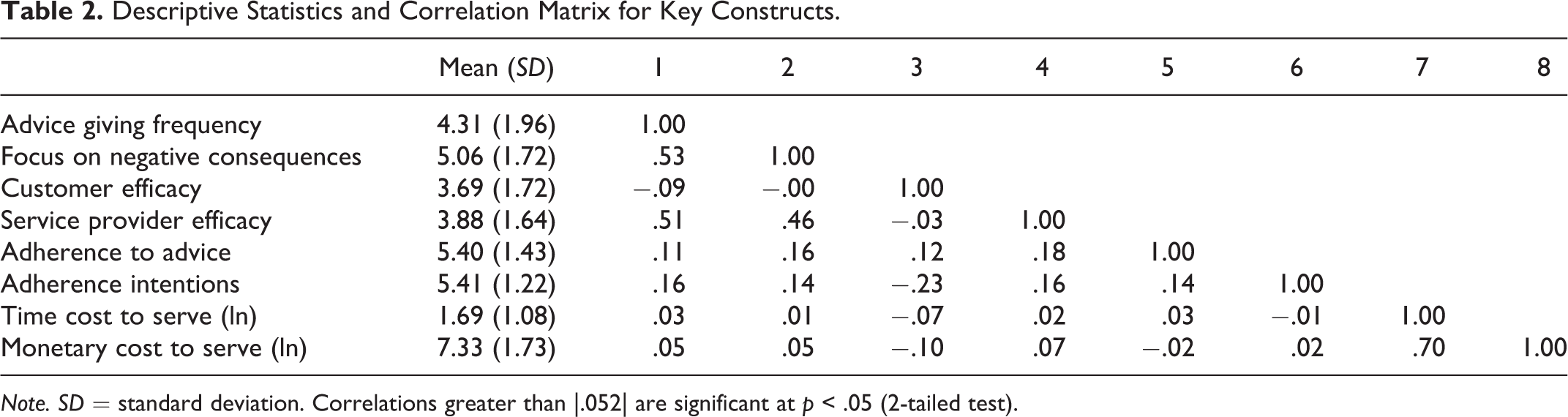
Note. SD = standard deviation. Correlations greater than |.052| are significant at p < .05 (2-tailed test).
Dependent variables
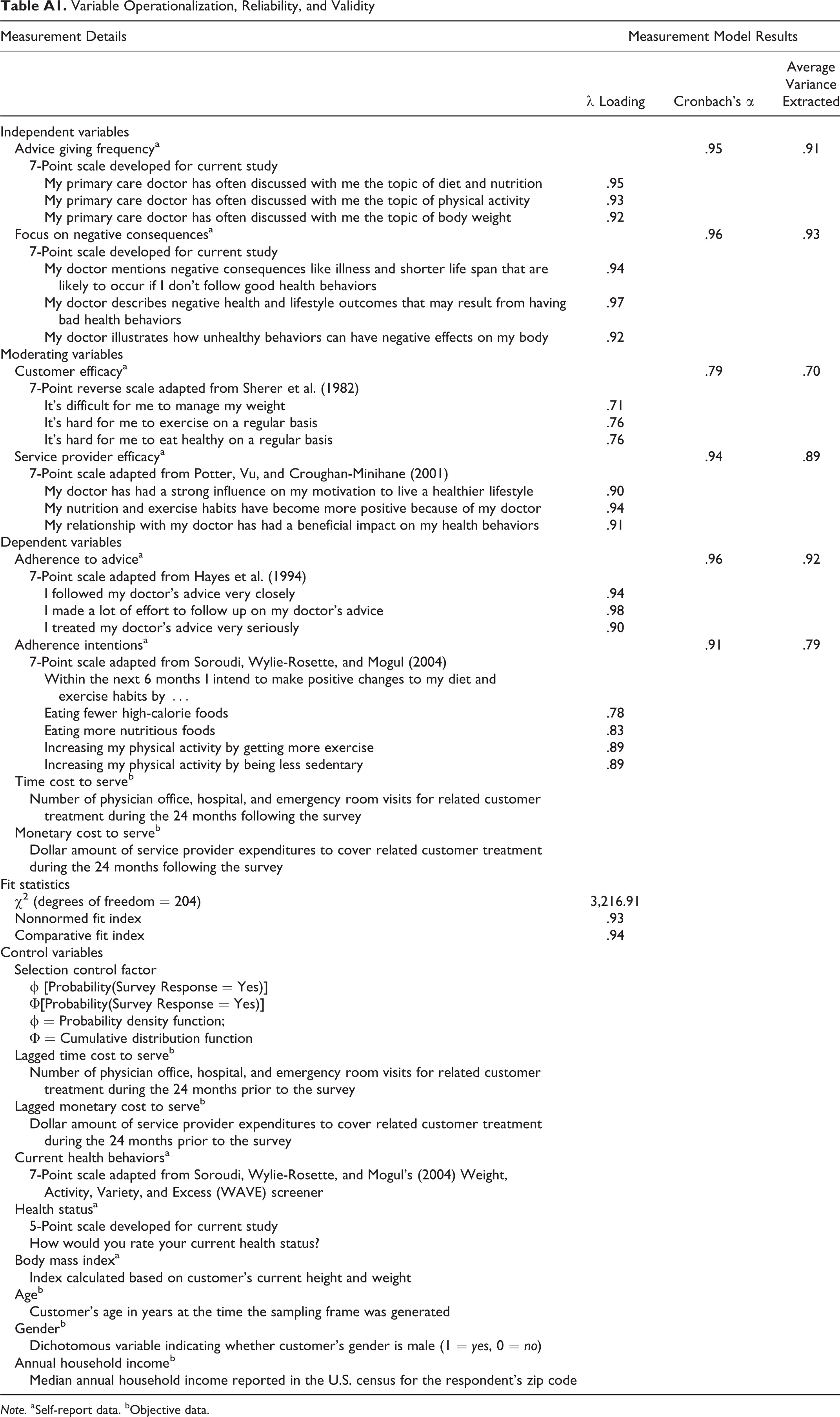
We used customer self-reported data to examine adherence to advice and adherence intentions. In both cases, the dependent variables were measured strictly relative to diet and exercise behaviors. We measured adherence to advice by adapting a 3-item, 7-point scale from Hayes et al. (1994), capturing the extent to which the patient had followed the primary care physician’s advice about diet and exercise up to a specific point in time. Adherence intentions capture the extent to which patients plan to adhere to the physician’s advice regarding diet and exercise in the 6 months following the survey. We measured these intentions using a 4-item, 7-point scale adapted from Soroudi, Wylie-Rosette, and Mogul (2004). We report the results of a confirmatory factor analysis supporting the reliability and validity of the scales in the Appendix. The Cronbach’s α for each scale is greater than .75 and the average variance extracted exceeds the minimum recommended score of .50, supporting the reliability of each construct scale (Bagozzi and Yi 1988). The scales also exhibit discriminant validity since the squared correlation between each pair of constructs is less than the average variance extracted for each construct and the χ2 value of a measurement model that constrains the correlation between variables to 1 is greater than the χ2 value of a model that does not impose this constraint (Fornell and Larcker 1981). We used mean scores for the constructs in the regression analyses.
We used objective patient clinical records to examine the time and monetary costs dedicated to serving each customer. Again, both dependent variables were measured based on organizational costs to provide health care services for patient treatment linked to diet and exercise behaviors. Time cost to serve the customer measures how many times a patient required health care services for related treatment based on the number of physician office, emergency room, and hospital visits in the 24 months following the survey. Monetary cost to serve the customer measures the financial expenditures based on the dollar amount paid by the HMO to cover related patient treatment in the 24 months after the survey. We identified related patient treatment using standardized clinical condition codes indicated in the clinical records for each patient visit. A panel of physicians and medical researchers affiliated with our HMO partner developed a set of clinical condition codes that have been medically established as related to diet and exercise behaviors. In our operationalization of the costs to serve, we included only service related to these conditions and excluded any visits or expenditures for preventive reasons; visits involving treatment for injuries, pregnancy, or mental health; and visits for laboratory tests. We log transformed the time and monetary cost measures to improve distribution normality.
Independent and moderating variables
Because no scales existed, we followed standard procedures to develop scale items for the two constructs capturing customer perceptions of their service provider’s approaches for discussing health-influencing behaviors. The first phase involved interviews with nine primary care physicians in different regions of the United States to establish their experiences and attitudes toward patients’ behaviors. The second phase involved developing an initial set of constructs and scale items related to customer interactions with their medical service provider based on the physician interviews as well as measures from the health care literature (e.g., Davis, Emerenini, and Wylie-Rosett 2006; Potter, Vu, and Croughan-Minihane 2001). We tested the items in an online pilot study with a national panel of 253 consumers. In a third phase, we refined and retested our scale items with an online national panel of 502 consumers. We used confirmatory factor analysis to further refine the scales for advice giving frequency and focus on negative consequences included in the final study of the HMO panel. As the results of the measurement model presented in the Appendix indicate, the scales meet standard minimum thresholds for construct reliability and for discriminant validity based on the comparisons between the average variance extracted and correlations between variables and the χ2 of the restricted and unrestricted measurement models previously described.
We examined the moderating effects of customer efficacy and service provider efficacy as follows: customer efficacy was measured using three 7-point reverse-scaled items adapted from Sherer et al. (1982), capturing the extent to which the patient finds it difficult to engage in the diet and exercise behaviors advised by the physician. We measured service provider efficacy using a 3-item, 7-point scale adapted from Potter, Vu, and Croughan-Minihane (2001) capturing the extent to which the patient perceives that the physician is able to effectively help the patient engage in the advised diet and exercise behaviors. The measurement model results reported in the Appendix support the construct reliability and discriminant validity of each scale. We used mean-centered, average scores for each of the latent constructs in subsequent regression analyses.
Control variables
We controlled for selection bias from systematic survey nonresponse by following Heckman’s (1979) two-step procedure. First, we estimated the probability of responding to the survey using relevant information for all customers in the sampling frame: customer age, gender, and a dummy variable indicating whether the customer’s primary care physician was part of the service provider’s network. Second, we created the inverse Mill’s ratio for each respondent, which represents the probability of responding to the survey. We included the inverse Mill’s ratio as an independent variable in the empirical model to control for unmeasured characteristics of survey response.
We controlled for omitted variables by including the lagged dependent variable as a predictor in the two models examining time and monetary costs to serve the customer. To control for the individual-level differences across customers, we included three measures of the customer’s health: current health behaviors, health status, and body mass index (BMI). Current health behaviors were measured using a 7-item index adapted from the Weight, Activity, Variety, and Excess (WAVE) screener, a key measure of diet and exercise behaviors in the medical literature (Soroudi, Wylie-Rosette, and Mogul 2004). Health status was measured using a single item on a 5-point scale where 1 = poor and 5 = excellent. We calculated the customer’s BMI based on each customer’s self-reported height and weight in the survey data. We also controlled for relevant customer demographics. Customer age and gender were captured from the HMO’s member database. Age represents the customer’s age in years at the time the sampling frame was generated. Gender was included as a dummy variable measured as 0 for female and 1 for male. We used the respondent’s zip code in the HMO member database to estimate each customer’s median annual household income as reported in the U.S. Census.
Model Specification
We estimated the following model specification using restricted maximum-likelihood estimation: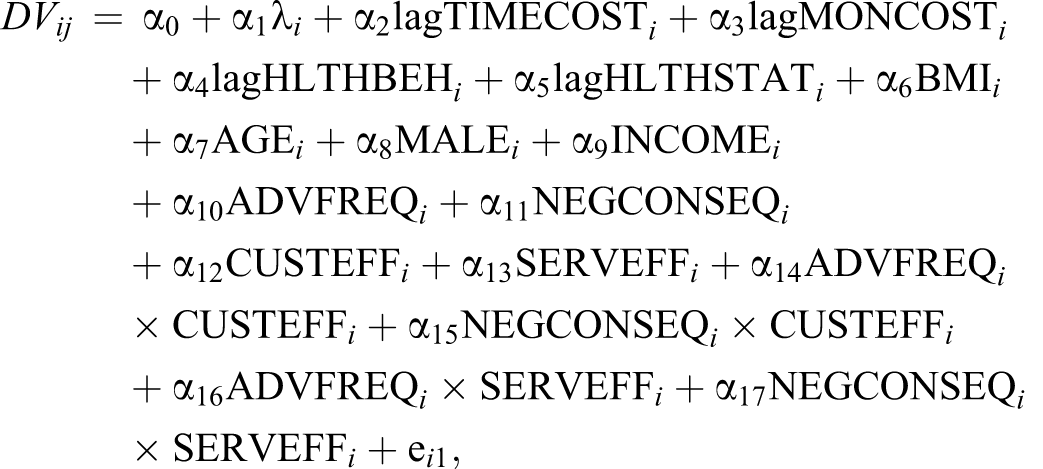
where “lag” indicates that the measure was taken from the period before the dependent measure observation (i.e., t − 1), and all other independent variables are measured at time t. In addition, DV
ij
= customer i’s health care service outcome;
j = adherence to advice, adherence intentions, time cost to serve, or monetary cost to serve; λ
i
= selection control factor for customer i; TIMECOST
i
= number of medical office or emergency room visits for customer i; MONCOST
i
= dollar amount of service provider spending for customer i; HLTHBEH
i
= current health behaviors of customer i; HLTHSTAT
i
= health status of customer i; BMI
i
= body mass index of customer i; AGE
i
= age of customer i; MALE
i
= dummy variable indicating the gender of customer i; INCOME
i
= annual household income of customer i; ADVFREQ
i
= advice giving frequency related to customer i’s diet and exercise behaviors; NEGCONSEQ
i
= service provider’s focus on negative consequences to customer i; CUSTEFF
i
= customer i’s confidence in ability to engage in healthful behaviors; SERVEFF
i
= customer i’s perception of service provider’s effectiveness in helping customer engage in healthful behaviors.
Results
To test the hypotheses, we ran a series of regression analyses to estimate models for adherence to advice, adherence intentions, time cost to serve, and monetary cost to serve as dependent variables. We evaluated the appropriateness of the sample size included in the estimation of each of our four models for achieving sufficient predictive power. We used statistical software to calculate the required sample size to achieve specified levels of power based on the specification of each model and a comparison of the full model with a reduced model. The sample size for each of our models (see Table 3) did not exceed the required sample size at the 80% power level, indicating that our model estimations were not overpowered beyond this generally accepted level.
Empirical Results for Customer Outcomes.
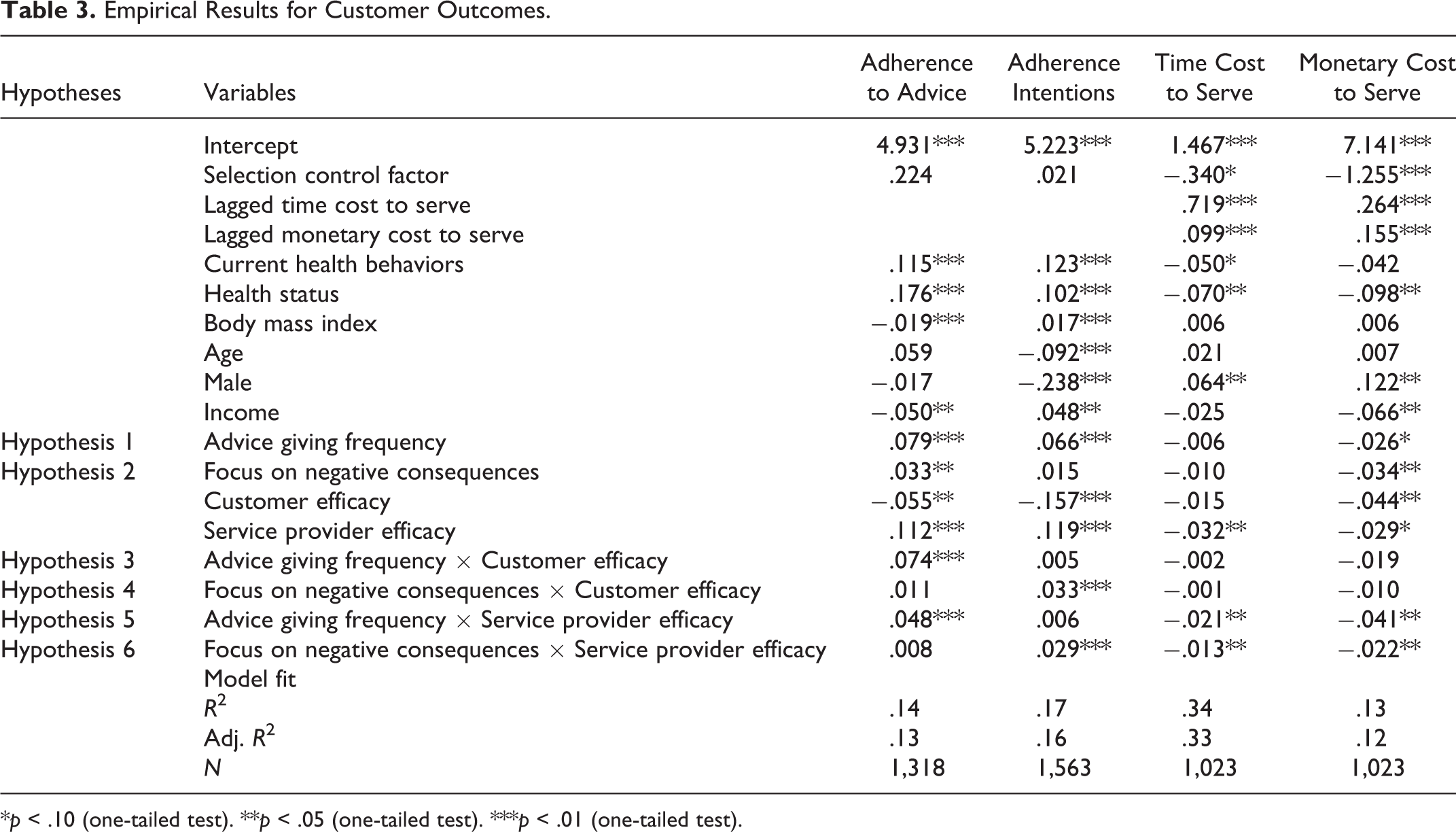
*p < .10 (one-tailed test). **p < .05 (one-tailed test). ***p < .01 (one-tailed test).
In addition, because our outcome variables capturing adherence to advice and adherence intentions were measured using the same survey instrument as our independent and moderating variables, we followed Lindell and Whitney (2001) to test for common method variance by comparing the correlation coefficients using a marker variable. Specifically, we selected a variable capturing the extent to which survey respondents utilize informational resources provided by our HMO partner (e.g., website, newsletter, and health fairs). This variable was measured on the same survey instrument as our independent, moderating, and perceptual outcome variables but is not predicted to be theoretically linked to patients’ current adherence or adherence intentions to advice from their primary care physician. We found that the coefficients did not change, offering evidence that this bias is not a significant issue. We present the nonstandardized coefficients for each of the models in Table 3.
Our test of the customer adherence to advice model offers support for Hypotheses 1a and 2a; both advice giving frequency related to customer diet and exercise behaviors and focus on negative consequences of poor health behaviors have positive main effects on customer adherence to service provider advice (.079, p < .01 and .033, p < .05, respectively). We also find support for Hypothesis 3a, suggesting that the relationship between advice giving frequency concerning diet and exercise behaviors and customer adherence is moderated by customer efficacy (.074, p < .01), as shown in Figure 2 (Panel A). In other words, frequent advice related to diet and exercise behaviors increases adherence to the advice when customers believe they can self-regulate those behaviors. Our results further indicate that the advice giving frequency-adherence link is moderated by service provider efficacy (.048, p < .01), supporting Hypothesis 5a. As Figure 2 (Panel B) indicates, the impact of frequently advising customers about their health behaviors on adherence is greatest when service provider efficacy is high. Hypotheses 4a and 6a were not supported in that focus on negative consequences was not moderated by customer efficacy or by service provider efficacy. As such, it appears that the impact of focusing on the potential negative consequences of customers’ health behaviors on adherence does not depend on customers’ beliefs about their own efficacy or the effectiveness of the service provider.
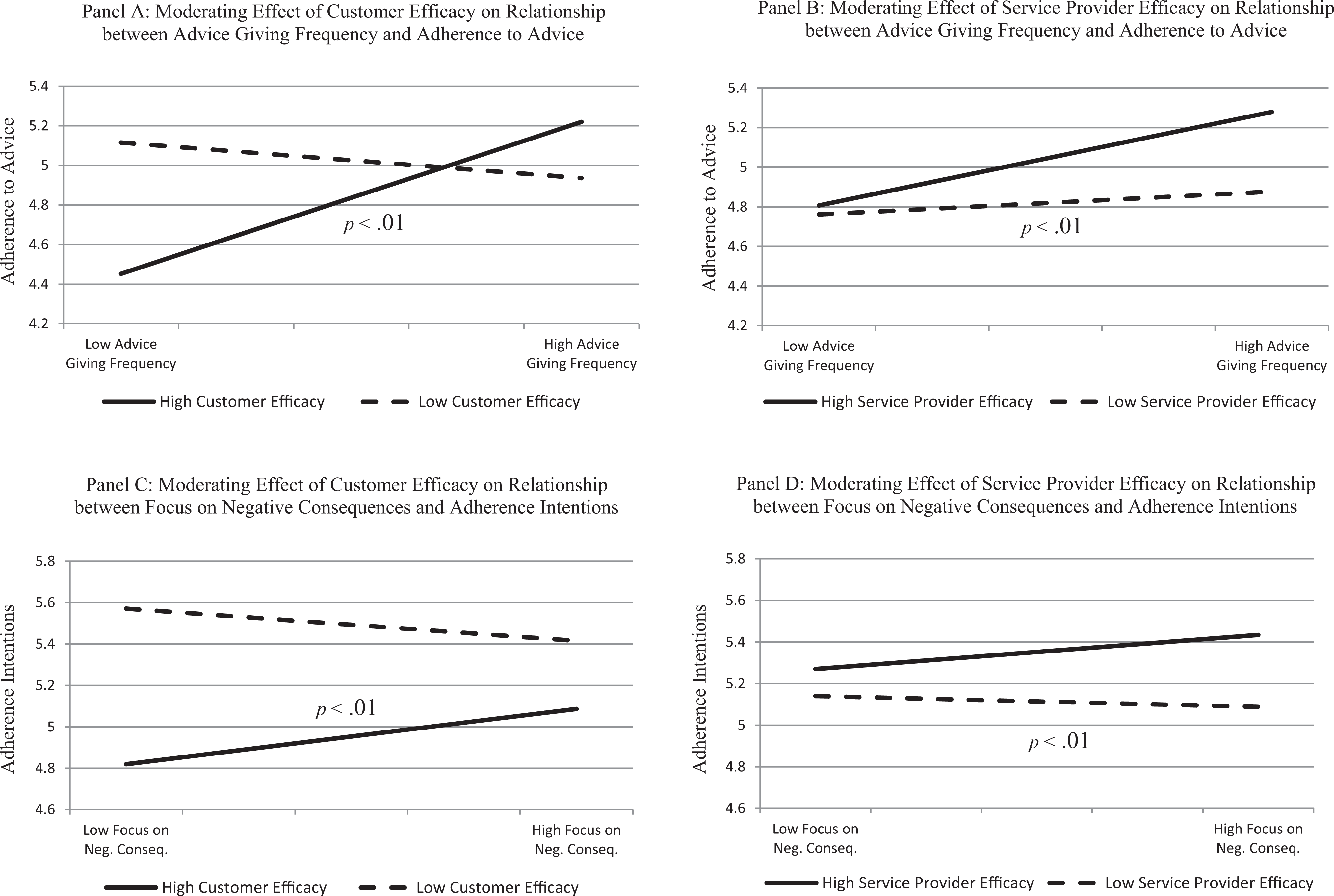
Significant moderating effects on adherence to advice and adherence intentions.
In the adherence intentions model, the frequency with which the service provider advises the customer on diet and exercise behaviors is positively associated with the customer’s intentions to engage in healthier behaviors in the coming months (.066, p < .01), supporting Hypothesis 1b. Although focusing on negative consequences of the patient’s health behaviors did not have a significant main effect on adherence intentions, as predicted by Hypothesis 2b, this aspect of the service provider’s approach was moderated by both customer efficacy and service provider efficacy. For Hypothesis 4b, customer efficacy moderates the relationship between service provider focus on negative consequences and customer adherence intentions (.033, p < .01). That is, as illustrated by Figure 2 (Panel C), the positive relationship between focusing on negative consequences of customers’ health behaviors and adherence intentions is enhanced when customers believe they have high efficacy in regulating their diet and exercise behavior. Our analysis also indicates that the relationship between service provider focus on negative consequences and customer adherence intentions is moderated by service provider efficacy (.029, p < .01), as predicted by Hypothesis 6b. As Figure 2 (Panel D) illustrates, focusing on negative consequences of customers’ health behaviors has a greater association with increased adherence intentions when customers perceive that the service provider demonstrates high levels of efficacy. We did not find support for Hypotheses 3b or 5b, suggesting that the impact of advice giving frequency related to customer’s health behaviors on adherence intentions does not depend on either customer efficacy or service provider efficacy.
Our examination of factors that impact the time cost to serve the customer indicates that customer perceptions of service provider efficacy are key. While advice giving frequency and focus on negative consequences did not have significant main effects on the time cost to serve customers, both dimensions of the service provider’s approach were moderated by perceptions of service provider efficacy (−.021, p < .05 and −.013, p < .05, respectively). Supporting Hypotheses 5c and 6c, advice giving frequency and focus on negative consequences are most effective at reducing time cost to serve customers when customers believe that service provider efficacy is high. We illustrate these moderating effects in Figure 3 (Panels A and B), respectively. In contrast, we did not find support for Hypothesis 3c or 4c. The effects of advice giving frequency or focus on negative consequences do not appear to be moderated by customer efficacy.
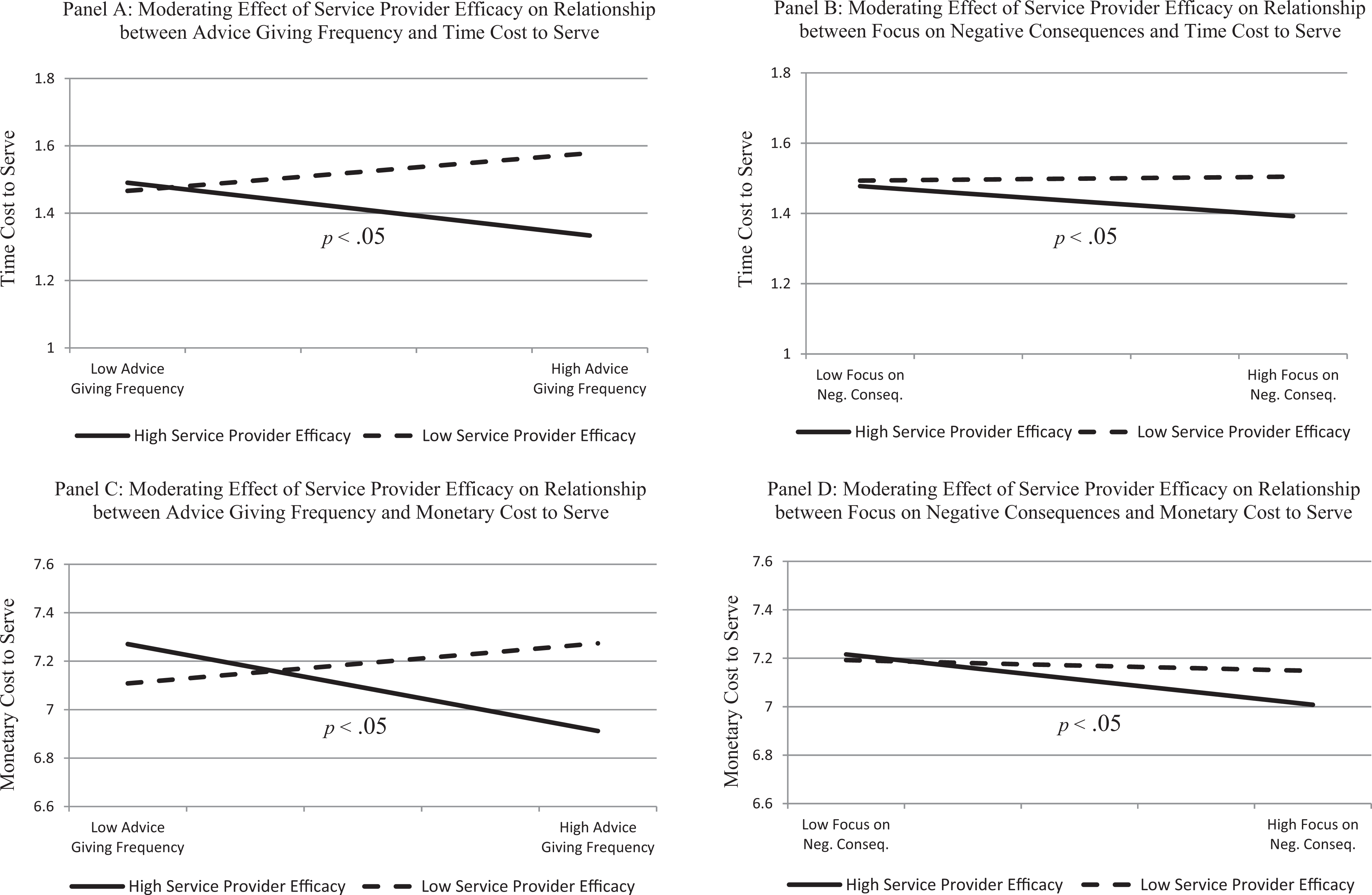
Significant moderating effects on time and monetary costs to serve.
We find that service provider efficacy is also an essential variable in understanding the effects of advice giving frequency and focus on negative consequences on the monetary cost to serve the customer. Consistent with our predictions in Hypotheses 1d and 2d, both advice giving frequency and focus on negative consequences have a significant direct effect in reducing the monetary costs to serve customers (−.026, p < .10 and −.034, p < .05, respectively). The impact of both variables on the service provider’s monetary cost to provide health care was moderated by perceptions of service provider efficacy, supporting Hypotheses 5d and 6d. As presented in Figure 3 (Panels C and D), the advice giving frequency and the focus on negative consequences are more effective at reducing monetary costs of providing service to the customer when customers perceive a higher degree of service provider efficacy (−.041, p < .05 and −.022, p < .05, respectively). As with time cost to serve, customer efficacy did not have significant moderating effects on either advice giving frequency or focus on negative consequences; thus, Hypotheses 3d and 4d were not supported.
Discussion
A customary role of professional service providers is to give advice with the goal of facilitating customer well-being while managing and sustaining organizational resources. Yet research reveals a common disconnect between professional service providers’ advice and customers’ adherence to that advice. For professional service providers in sectors such as medicine, law, engineering, architecture, consulting, and financial planning, the ability to motivate customers and influence their behaviors is an important issue that merits attention and investigation. We introduce a multifaceted model of professional service provider influence with diverse antecedent, moderating, and outcome variables and provide a strong test of that model using an original data set that enables us to closely examine customer perceptions and behaviors over a multiyear period. The level of support for our hypothesized relationships is notable, given the general difficulty to identify moderating effects (e.g., Aiken and West 1991; Voss, Godfrey, and Seiders 2010).
Our perceptual outcome variables capture both current adherence to advice and intended future adherence. Although counter to our predictions, we see alternating moderating effects of customer efficacy and service provider efficacy on these variables. These differences in effects across the two outcomes may be because patients who have already engaged in behavior consistent with physician advice do not plan to make further efforts, but patients who have not followed medical advice do plan to do so. In this sense, current adherence to advice and adherence intentions may be an either/or perception: if customers are currently adhering to advice, they do not intend to increase future adherence; they intend to increase adherence only if they do not currently adhere.
Results for the moderating effects of customer efficacy also were not as predicted. Although the results for the two perceptual outcomes support our hypotheses, we find no significant moderating effects related to our objective outcome variables. This finding is consistent with a number of recent studies reporting weak effects of self-efficacy on performance, so it was not totally unanticipated. Although customer efficacy did not exhibit moderating effects related to the costs to serve, outside of this variable we find overall support for the predicted drivers of reduced organizational costs to serve.
Finally, we see some divergence in the effects across the two outcome variables measuring costs to serve the customer related to nonadherence to advice. Advice giving frequency and focus on negative consequences both show significant direct effects on monetary cost to serve but not on time cost to serve. This may suggest that adherence to advice is better captured by the financial costs involved in providing service related to adherence than by frequency of visits, which represents our measure for time costs. Since the frequency of visits does not account for the length of time the customer spends with the service provider during each visit, the monetary cost to serve may capture aspects of the resources required to serve the customer that are not captured by our time cost measure. In the sections that follow, we discuss the implications of our findings for theory, research, and professional service provider practice.
Implications for Theory and Research
Professional service provider-customer exchange is a fertile area for the application of new conceptual and theoretical perspectives. We integrate and apply theories related to professional services, advice utilization, and social cognition to provide a framework for our study of customer adherence to expert advice in need-based services such as medical care. Professional services theory explains the essential role of expertise as value in the dyadic service provider-customer exchange. It suggests that frequent guidance and focused advice reduce information asymmetry, allowing professional service providers to effectively influence and motivate customers (Greenwood et al. 2005; Von Nordenflycht 2010). Our findings add to the literature lacking robust empirical investigations, with longitudinal analysis examining customers’ adherence to advice over time (see Table 1). By helping to explain the mechanism by which customer adherence to advice can be influenced, our study provides insights into how professional service firms might promote customer well-being yet sustain organizational resources by managing costs to serve.
Our research contributes to the advice taking literature and helps to extend that theory into services research. Theoretical implications are relevant not only for advice taking research but also for advice giving, which is less studied (Jonas and Frey 2003). Advice research is also limited in its examination of the role of individual differences, which we explicitly capture in our tests of moderating effects (Bonaccio and Dalal 2006). Most important, advice utilization in contexts of prior interactions, familiarity, and relationship-based exchange has rarely been examined. As Schwartz, Luce, and Ariely (2011) affirm, this is a significant void to fill.
Our examination of the moderating variables customer and service provider efficacy, which represent customer beliefs fundamental to service exchange, offers insights relevant to key psychological characteristics. Customer efficacy significantly moderated perceptual outcomes (adherence to advice for advice frequency and adherence intentions for focus on negative consequences) but did not moderate the cost to serve variables. This may indicate that high self-efficacy customers (contrary to their self-reported perceptions) are inclined to discount both service provider advice and underlying risk addressed by that advice, perhaps due to overoptimism and strong self-belief. A growing body of empirical studies reports a negative influence of self-efficacy on performance (e.g., Moores and Chang 2009; Vancouver et al. 2002), and prior research in health care suggests that self-efficacy may cause individuals to underestimate risks and make suboptimal health decisions (Goldberg, Halpern-Felsher, and Millstein 2002). Overall, the moderating role of customer efficacy is not well understood, and the idea that it always works to a customer’s advantage is debatable. We contribute to the social cognitive and advice taking literatures by considering the phenomenon of overconfidence or egocentric discounting and highlighting its role in advice utilization (e.g., Sniezek, Schrah, and Dalal 2004).
Service provider efficacy affected all outcome variables, supporting basic theoretical tenets that the professional service provider has a distinct ability to influence customers who believe a specific provider is effective in facilitating adherence to advice. Service provider efficacy captures, in part, customer trust in provider competence at the interpersonal or dyad level that is a focal point of professional services. It reflects the perceived capabilities of a specific service provider and thus extends beyond the broad effects of a profession’s credibility. Advice frequency coupled with high service provider efficacy appears to be a consistently strong motivating force, probably because the likelihood of a successful outcome appears greater to customers.
In medical settings, considerable research has examined the participation of customers in their own care by focusing on aspects of communication, such as how patients relay information to their doctors about their condition and treatment preferences (e.g., Gallan et al. 2013; McColl-Kennedy et al. 2012; Wen and Kosowsky 2013). We consider the dynamics of customer compliance with expert service provider advice after that advice has been offered (post-encounter), that is, by examining the extent to which consumers behaviorally adhere to advice using both perceptual and objective behavioral outcomes over time.
Advice giving frequency and focus on negative consequences represent service provider actions that are flexible, modifiable, and potentially strategic. Service providers can elect to have longer (shorter) discussions with customers and focus more (less) on the consequences of behavior. Our moderating variables too are mutable: Customer efficacy and service provider efficacy are characteristics that can be influenced. As such, our findings have meaningful implications related to service provider impact on customer behavior.
Implications for Practice
Our research provides empirical evidence that can be used by professional service providers across multiple sectors. The practical implications of our research are straightforward because the four aspects of expert advice giving that we examined can be implemented (advice giving frequency and focus on negative consequences), influenced (service provider efficacy), and detected (customer efficacy) by the service provider. Professional service providers can leverage these factors to execute approaches that improve customer well-being and help sustain organizational resources.
First, our results highlight the importance for professional service providers to frequently discuss the need for customer adherence to specific behaviors. The need for effective consultation and advice is recognized in professional service contexts, but studies across sectors show that, for a variety of reasons, advice is often only minimally offered by professional service providers (e.g., Auh et al. 2007). When it is provided, the relevant implications are not always well presented to customers (Puustinen, Kuusela, and Rintamaki 2012). For example, despite the fact that unhealthy diet and lack of physical activity are linked to numerous chronic diseases, research finds that the negative consequences of these unhealthy behaviors are discussed in only 25% of medical office visits (Gigerenzer et al. 2008). Professional service providers who want to have successful relational exchanges may be hesitant to recommend actions they realize their customers will be reluctant to take (Post et al. 2011). Also, they may be unsure of how to address psychological factors that underlie entrenched behaviors such as excessive spending by financial services customers (Grubman, Bollerud, and Holland 2011). Our findings indicate that, despite these barriers, professional service providers should systematically and frequently allocate time to consult with customers and discuss advised behaviors.
Second, our findings indicate that it is essential for professional service providers to give customers the “why”—a compelling reason to adhere to the focal advice based on the unwanted outcomes that may result from nonadherence. While the literature is mixed on the effectiveness of emphasizing risk factors, our results suggest that clear communication about the potential for negative outcomes plays a significant role. Berry and Bendapudi (2007) present the case of a physician advising a patient to stop smoking cigarettes. During the clinical visit, the physician reminds the patient of the multiple times they have discussed the patient’s need to change this behavior. Our findings suggest that the physician may have been more effective in motivating patient adherence by explicitly emphasizing the harmful effects of the patient’s smoking behavior and the serious, or even fatal, health consequences of nonadherence to the given advice.
Third, our research shows that professional service organizations seeking to be more effective in encouraging customer adherence to advice would be wise to invest in enhancing customer perceptions of service provider efficacy. Service providers can influence perceptions of their efficacy by calling the customer’s attention to positive outcomes achieved through the course of their working relationship, deliberately noting how the service provider has helped the customer achieve those successes and generally reinforcing perceptions of competence. Helping customers form a causal link between working with their service provider, and making beneficial behavioral changes offers professional service providers an opportunity to more effectively motivate customers.
There are several specific actions primary care physicians might take to strengthen patients’ perceptions of service provider efficacy. For example, a physician generally begins the process of advising a patient currently engaging in unhealthy diet and exercise behaviors by conducting a thorough assessment to identify any health conditions that may be linked to the patient’s health behaviors. During subsequent clinical interactions, the physician can review with the patient any incremental improvements in behaviors or outcomes, such as increased physical activity, weight loss, lower cholesterol levels, or lower blood pressure. This approach carries into other professional service settings. For example, an architect working with a client on the renovation or construction of a home can highlight to the client success in meeting building code inspections during the construction process based on the architect’s expert guidance. This could help customers form a causal link between working with their service provider and making beneficial changes in their behaviors.
Our findings suggest that the role of customer efficacy may be less straightforward than service provider efficacy. For a customer whose self-efficacy is strong, overconfidence in future outcomes may interfere with adherence. Also, this customer may be more likely to discount service provider advice. For example, a financial planner may face significant challenges counseling a customer on managing personal debt to avoid detrimental effects to the customer’s credit score or even personal bankruptcy. A customer with high self-efficacy may discount the advice of the financial planner based on a false sense of confidence about his or her own ability to contain the personal debt. As such, a fourth implication of our findings is that it may be more effective for a service provider to recognize and temper aspects of this advice-related self-efficacy—rather than attempt to foster this customer trait—to gain better adherence to advice.
From an organizational resource perspective, the ability of professional service providers to effectively influence behavior is critical, as unsuccessful attempts to advise customers can drain time, energy, and emotions as well as financial resources (Grubman, Bollerud, and Holland 2011). In health care, policy experts argue that emphasizing disease prevention is the most financially sustainable strategy. Our research partner’s chief executive, commenting on the impact of reduced patient utilization, noted that what may appear to be relatively small effects to someone outside of health care translate into millions of dollars in cost reduction in his organization.
Limitations and Future Research
A limitation of our research is the focus on one professional service sector, that is, health care. Although the organization we studied is a large, diverse HMO with its own clinics, hospitals, and clinicians, our sample was composed exclusively of HMO members. While this was necessary for our methodological approach of tracking individual-level behavioral data over time and linking it to survey data, future studies should involve both broader samples of medical customers (with varying levels of health care insurance) and consumers of other types of professional services. Our sample also was limited geographically to the southwestern United States. Customers in other geographic regions of the United States and other countries may exhibit differences in perceptions and behaviors.
A second potential limitation of this study involves characteristics of the four dependent variables examined. While our dependent variables of adherence to advice and adherence intentions capture both current and planned adherence, measured by validated scales, these measures are limited in that they are self-report measures subject to common method bias. Our health care utilization outcome variables capture longitudinally measured behavioral data, and our post-survey observation period spanned 24 months. It is important to note that, given the low frequency of primary care physician visits, this is a relatively constrained period in which to assess effects. However, it allows us to provide a stringent test of our hypotheses.
Given the interdependence of the service provider and customer in achieving successful outcomes in many professional service settings, another fertile area for research is the service provider-customer dyad. Prior research has reported that dyadic interaction is a strong determinant on outcomes such as customer satisfaction (Ma and Dubé 2011; Yim, Chan, and Lam 2012). With continued exploration of service provider-customer interactions, we can gain more comprehensive knowledge of additional determinants of professional service provider effectiveness.
Our research aims to theoretically explain and empirically demonstrate the dynamics that underlie professional service provider motivation of customers to adhere to expert advice. The findings provide insight into underexplored aspects of the professional service provider-customer relationship. Our study addresses the crucial question of how professional service providers can positively influence customer behaviors but more remains to be learned. Researchers across disciplines would do well to seriously explore factors that moderate the relationship between professional service provider actions and approaches and subsequent customer responses and behaviors.
Footnotes
Appendix
Variable Operationalization, Reliability, and Validity
| Measurement Details | Measurement Model Results | ||
|---|---|---|---|
| λ Loading | Cronbach’s α | Average Variance Extracted | |
| Independent variables | |||
| Advice giving frequencya | .95 | .91 | |
| 7-Point scale developed for current study | |||
| My primary care doctor has often discussed with me the topic of diet and nutrition | .95 | ||
| My primary care doctor has often discussed with me the topic of physical activity | .93 | ||
| My primary care doctor has often discussed with me the topic of body weight | .92 | ||
| Focus on negative consequencesa | .96 | .93 | |
| 7-Point scale developed for current study | |||
| My doctor mentions negative consequences like illness and shorter life span that are likely to occur if I don’t follow good health behaviors | .94 | ||
| My doctor describes negative health and lifestyle outcomes that may result from having bad health behaviors | .97 | ||
| My doctor illustrates how unhealthy behaviors can have negative effects on my body | .92 | ||
| Moderating variables | |||
| Customer efficacya | .79 | .70 | |
| 7-Point reverse scale adapted from Sherer et al. (1982) | |||
| It’s difficult for me to manage my weight | .71 | ||
| It’s hard for me to exercise on a regular basis | .76 | ||
| It’s hard for me to eat healthy on a regular basis | .76 | ||
| Service provider efficacya | .94 | .89 | |
| 7-Point scale adapted from Potter, Vu, and Croughan-Minihane (2001) | |||
| My doctor has had a strong influence on my motivation to live a healthier lifestyle | .90 | ||
| My nutrition and exercise habits have become more positive because of my doctor | .94 | ||
| My relationship with my doctor has had a beneficial impact on my health behaviors | .91 | ||
| Dependent variables | |||
| Adherence to advicea | .96 | .92 | |
| 7-Point scale adapted from Hayes et al. (1994) | |||
| I followed my doctor’s advice very closely | .94 | ||
| I made a lot of effort to follow up on my doctor’s advice | .98 | ||
| I treated my doctor’s advice very seriously | .90 | ||
| Adherence intentionsa | .91 | .79 | |
| 7-Point scale adapted from Soroudi, Wylie-Rosette, and Mogul (2004) | |||
| Within the next 6 months I intend to make positive changes to my diet and exercise habits by … | |||
| Eating fewer high-calorie foods | .78 | ||
| Eating more nutritious foods | .83 | ||
| Increasing my physical activity by getting more exercise | .89 | ||
| Increasing my physical activity by being less sedentary | .89 | ||
| Time cost to serveb | |||
| Number of physician office, hospital, and emergency room visits for related customer treatment during the 24 months following the survey | |||
| Monetary cost to serveb | |||
| Dollar amount of service provider expenditures to cover related customer treatment during the 24 months following the survey | |||
| Fit statistics | |||
| χ2 (degrees of freedom = 204) | 3,216.91 | ||
| Nonnormed fit index | .93 | ||
| Comparative fit index | .94 | ||
| Control variables | |||
| Selection control factor | |||
| φ [Probability(Survey Response = Yes)] | |||
| Φ[Probability(Survey Response = Yes)] | |||
| φ = Probability density function; | |||
| Φ = Cumulative distribution function | |||
| Lagged time cost to serveb | |||
| Number of physician office, hospital, and emergency room visits for related customer treatment during the 24 months prior to the survey | |||
| Lagged monetary cost to serveb | |||
| Dollar amount of service provider expenditures to cover related customer treatment during the 24 months prior to the survey | |||
| Current health behaviorsa | |||
| 7-Point scale adapted from Soroudi, Wylie-Rosette, and Mogul’s (2004) Weight, Activity, Variety, and Excess (WAVE) screener | |||
| Health statusa | |||
| 5-Point scale developed for current study | |||
| How would you rate your current health status? | |||
| Body mass indexa | |||
| Index calculated based on customer’s current height and weight | |||
| Ageb | |||
| Customer’s age in years at the time the sampling frame was generated | |||
| Genderb | |||
| Dichotomous variable indicating whether customer’s gender is male (1 = yes, 0 = no) | |||
| Annual household incomeb | |||
| Median annual household income reported in the U.S. census for the respondent’s zip code | |||
Note. aSelf-report data. bObjective data.
Acknowledgement
The authors thank Allan Einboden, chief executive officer of the Scott & White Health Plan, for his support of the study, and thank the Editor and JSR reviewers for their thoughtful and constructive suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.