
Abstract
In this study, we examine the conflicts and unintended consequences that arise from the diverse social conventions constituting a transformative service. We draw on convention theory and an ethnographic study to interpret a community-based palliative care initiative in Kerala (India) as a transformative service system. We contribute to transformative service research by developing a dialectical transformative service system framework that is a synthesis of the calculative conflict-ridden regime of justice and the noncalculative regime of agape based on love. In this framework, the calculative regime of justice has civic conventions at its core and industrial, inspired, market, domestic, and fame conventions as ancillaries. While the regime of justice is associated with the undesired, unintended consequence of conflicts, the regime of agape constitutes a desirable unintended consequence. Our framework provides a microlevel understanding of disputes and their reconciliation, advances a diffused understanding of worth that ruptures the binary of legitimate or illegitimate actions, and delineates the significance of morality. Our study also contributes by explaining agape’s role in transformative service, particularly in health and caregiving.
Accomplishing transformative service is often a collective endeavor that involves multiple collaborating actors (Anderson and Ostrom 2015; Anderson et al. 2013, 2016; Baron et al. 2018; Blocker and Barrios 2015; Skålén, Aal, and Edvardsson 2015). Transformative service research (TSR) primarily draws on service-dominant (S-D) logic to examine service systems (or ecosystems) that integrate resources and cocreate value coordinated through shared institutions (Vargo and Lusch 2004, 2016). However, the S-D logic, which emphasizes individual benefits, resource integration, and value cocreation, advances a market-based understanding of a service system. Drawing on convention theory, or the sociology of conventions, we show the limitations of S-D logic in informing transformative service and offer an alternative dialectical framework that highlights how regimes of justice and agape accomplish transformative service.
Convention theory focuses on common understandings among people that underpin coordinated and collaborative actions since people negotiate the complex, conflicting demands of existence in contemporary societies based on shared conventions (Boltanski and Thévenot 1999). Specifically, we draw on two broad approaches to coordination: the regimes of justice and agape (Boltanski 2012; Boltanski and Thévenot 2006). A regime of justice consists of diverse social conventions—such as professional standards, civic duties, traditions, or markets—which individuals draw on to justify their actions on moral grounds. This regime of justice is based on equivalence, which people calculate using available conventions. Actors may enact conflicting conventions in various contexts. For example, actors may draw on conflicting conventions—such as environmental conventions of sustainability, industrial conventions of regulations and standards, and market conventions that value pricing and monetization—to justify products and services in an environmentally sensitive setting such as the upstream petroleum industry (Finch, Geiger, and Harkness 2017). In this vein, Patriotta, Gond, and Schultz (2011) have documented how stakeholders may deploy plural competing industrial, civic, and market conventions in responding to a nuclear accident. In contrast to such calculations and conflicts, people cooperate out of love and act selflessly in a regime of agape. Therefore, the calculative equivalence and reciprocal expectations that are foundational to justice are set aside in a regime of agape (Boltanski 2012; Boltanski and Thévenot 1999). Agape can create close bonds between service providers and recipients. Indeed, agape can be a key element in creating solidarities in social movements and community initiatives (Summers-Effler 2007).
With its focus on individual benefits, resource integration, and value cocreation, S-D logic emphasizes the market convention of the regime of justice in which self-interest, competition, and detached social relationships are key features (Boltanski and Thévenot 2006). Thus far, the TSR informed by S-D logic engages with justice within the conventions of markets. As a result, transformative themes such as poverty reduction, access to social services, service literacy, and vulnerable consumers (Anderson and Ostrom 2015; Anderson et al. 2013) have been investigated from the perspective of market conventions by attending to how resources are integrated and value is cocreated. We argue that by emphasizing S-D logic, TSR has been monochromatic. In contrast, a transformative initiative requires a broad interface reflective of society and its various conflicts.
While the quest for justice in the market world privileged within S-D logic can be transformative, we foreground other conventions of worth. Social actors and transformative service initiatives often have to deal with the unintended consequences of conflicts between multiple conventions in a regime of justice and their reconciliation. For example, Batifoulier, Da Silva, and Duchesne (2019) show that the French social security system has shifted over time from a dominant anticapitalist convention to a compromise between solidaristic and liberal conventions. In another example, Sreekumar and Varman (2019) show that poor migrants negotiate the conflicting demands of conventions of traditions and commodified relationships to resist dominant consumer acculturation. Such conflicts between conventions are underexamined in the extant TSR informed by S-D logic (Laamanen and Skålén 2015; Skålén, Aal, and Edvardsson 2015). Moreover, we highlight the importance of the regime of agape, a neglected facet of transformative service for a vulnerable group.
We examine conflicting care conventions in a community palliative care service system in Kerala, India (henceforth the community model). Palliative care is an approach that improves the quality of life of patients and their families facing life-threatening illnesses through medical, psychosocial, and spiritual support (World Health Organization 2020). Across the world, professional teams of nurses, physicians, and social workers operating through hospitals and hospices deliver palliative care. With one sixth of the world’s population, India has less than 2% palliative care coverage, and most states have no palliative care awareness or facilities (Rajagopal 2015). In contrast, the state of Kerala provides palliative care to more than 60% of its population through the community model. The community model has transformed patients’ and families’ lives by offering free home-based care encompassing financial, social, emotional, medical, rehabilitation, and bereavement support (Vijay, Monin, and Kulkarni 2020). At the community level, it has produced cascading effects from the palliative care domain into overlapping fields such as geriatric care and mental health. At the institutional level, in response to community mobilization and advocacy, public health organizations collaborate with community organizations to provide home care (Kumar 2013). Therefore, we consider Kerala’s community palliative care service system as a fertile ground for examining transformative service and its unintended consequences.
We develop a dialectical transformative service system framework that is a synthesis of the calculative conflict-ridden regime of justice and the noncalculative regime of agape. By developing the framework, we contribute to TSR in three ways. First, we illustrate how a transformative service inheres a regime of justice with diverse social conventions. While TSR has thus far primarily drawn on institutional theory-informed S-D logic, our framework broadens TSR to include the role of conventions. In our framework, the transformative service is constituted by civic conventions at its core and industrial, inspired, market, domestic, and fame conventions as ancillaries. We identify conflicts arising as unintended consequences of the diverse social conventions constituting the transformative service. Second, we develop a richer conceptualization of transformative service by offering a microlevel understanding of disputes and their reconciliation that transcends the binary of legitimate and illegitimate actions, which is central to theorization based on the understanding of institutions. By attending to the microlevel, we also develop a diffused and context-specific understanding of worth that foregrounds the significance of morality. Third, our framework contributes to TSR by highlighting the regime of agape in a community care setting. In so doing, we transcend the grammar of calculation and exchange to open up an understanding of service based on a sense of solidarity and love.
Theoretical Considerations
In this section, we review TSR with a focus on health care. We then draw on the French convention school to delineate how diverse conventions of justice with conflicting demands and principles come together in transformative service. Finally, we discuss the regime of agape that is central to the community model.
TSR on Health Care
While some researchers have delineated diverse social influences beyond the market logic that underpin transformative service (e.g., Baron et al. 2018; Blocker and Barrios 2015; Skålén, Aal, and Edvardsson 2015), TSR has been lopsidedly informed by S-D logic that highlights exchange through markets within service systems. S-D logic adheres to a research tradition that emphasizes how firms and managers integrate and use resources to create superior market value and secure sustained competitive advantage (Barney 1991; Vargo and Lusch 2004). According to S-D logic, the common purpose of market actors is value cocreation and resource integration through “service-for-service exchange,” with a calculative expectation of exchanging benefits (Vargo and Lusch 2016). Notably, S-D logic has a broad view of resources, and two of its “fundamental premises” suggest that “All social and economic actors are resource integrators” and “Value is co-created by multiple actors, always including the beneficiary” (Vargo and Lusch 2016, p. 8). Hence, S-D logic focuses not only on firms’ and managers’ strategic benefits, but it also extends the resource-based market logic to all types of relations and service systems. Accordingly, both economic (e.g., firms and managers) and social actors (e.g., families and their members; Vargo, Akaka, and Yi 2010) are resource integrators operating with a calculative market logic (Fougère and Skålén 2013).
Several empirical TSR studies, especially within health care, have drawn on S-D logic to attend to resource integration, value cocreation, and service systems, thus remaining confined to the market logic. In a key study examining cancer patients’ value cocreation, McColl-Kennedy et al. (2012) identify five “customer value co-creation practice styles” in which patients’ active involvement secures resource integration. This understanding of patients as benefit seeking, resource integrating, and cocreating customers implies a market logic. Similarly, Frow et al. (2016) studied health care as a service ecosystem of resource integration processes “to develop a typology of co-creation practices” (p. 24).
Sweeney, Danaher, and McColl-Kennedy (2015) elaborate on McColl-Kennedy et al.’s (2012) work to suggest that the more effort patients put into value cocreation, the more satisfied they are. Presuming that patients as customers need to exert efforts to receive health care services underscores a transactional market logic. Furthermore, Anderson et al. (2016) point to market logic when they attend to resource integration and value cocreation in health care under a regime of responsibilization. They identify three resource-integrating practices: accessing, managing, and appropriating and contribute to TSR “by identifying resource-integration practices that a responsibilized consumer must undertake” (Anderson et al. 2016, p. 263). This S-D logic-based approach portrays patients as calculative consumers who must take responsibility for their health care by enacting practices, as in any market. By focusing on value cocreation, resource integration, and service systems, this research, in line with several other health care studies (e.g., Anderson, Nasr, and Rayburn 2018; Breidbach, Antons, and Salge 2016; Danaher and Gallan 2016; Davey and Grönroos 2019; Frow et al. 2016; McColl-Kennedy, Cheung, and Ferrier 2015; Sharma and Conduit 2016; Spanjol et al. 2015), frames transformative service as a calculative market regime emphasizing strategic benefit.
In summary, drawing on S-D logic, TSR has primarily understood transformative service, particularly in health care, from the market logic perspective. In the transformative service we examine, the market logic does not play a central role. Moreover, TSR on health care does not offer insights into the unintended consequences of conflicts that arise when actors follow multiple conventions, and there is a neglect of how these conflicts are resolved. We found that these issues were salient in Kerala’s community model. We now turn to convention theory to provide a broader conceptualization of transformative service.
Convention Theory
Convention theory examines how conventions constitute different evaluations or orders of worth underlying conflicting ways of life (Boltanski and Thévenot 2006). A convention is a publicly recognized interpretation and evaluation of a situation that offers an understanding of the common good (Batifoulier, Da Silva, and Duchesne 2019). Instead of assuming pregiven needs, resources, and evaluations, convention theory regards convention-based coordination as central to these ontologies from which institutions and values emerge (Diaz-Bone 2016). Conventions may have arbitrary origins but provide normative action frameworks (Al-Amoudi and Latsis 2014). For example, Bridson et al. (2017) explain how music fans do not support market conventions and locate artists in the inspired world. These music fans do not see the market world as authentic and thus label the musicians who follow commercial motives as “sellouts.”
Boltanski and Thévenot’s (2006) seminal writing on the sociology of conventions, “On Justification,” challenges sociological frameworks that reify social actions. Specifically, the authors depart from a Bourdieusian emphasis on habitus or dispositions or Durkheimian assumptions of collective reasoning based on group membership. Instead, convention theory adopts a fluid interpretation that foregrounds situations and pragmatism, which shape social actions. There is no single optimal convention for all situations or universal cognitive frameworks for all social actions (Diaz-Bone 2016). Convention theory assumes a plurality of possible ways to structure social coordination. While these regimes can include some strategic behaviors, they are rooted in the coherence, habits, morality, and procedural requirements of a social space (Al-Amoudi and Latsis 2014).
Conventions are not the same as institutional logics that are “socially constructed, historical patterns of material practices, assumptions, values, beliefs and rules” (Thornton and Ocasio 2008, p. 101). Institutional logics are ensembles of higher order meanings, values, norms, and rules that frame how actors make sense of the world and act in legitimate or illegitimate ways in different societal sectors (e.g., state, market, or family) or industries (Cloutier and Langley 2013; Thornton et al., 2012). The idea of logics derives from Durkheimian sociology, which assumes that rules are hierarchically organized, thereby allowing actors to draw on collective rationalities. Indeed, S-D logic draws on institutional theory to better understand resource integration and value cocreation in service systems (Vargo and Lusch 2016). Further, some TSR studies have uncovered how a service can be shaped by contestations between institutions and the practices they condition (Anderson et al. 2016; Baron et al. 2018). Convention theorists offer important insights to these conversations by highlighting that actors do not rely on collective rationalities all the time; all situations do not require an imperative of justification to the same degree, and criticisms are not always rejected via clear-cut argumentation (Boltanski and Thévenot 2006). Accordingly, there are proximate and intuitive ways of coordinating through different conventions (Boltanski and Thévenot 1999). Convention theory also rejects the assumption that social actors make sense of the world in a predetermined way, as dictated by a particular institutional logic. Instead, convention theory assumes that actors draw on elements from different worlds depending on their situations (Cloutier and Langley 2013), and conflicts and disputes inhere moral justifications. For example, Sreekumar and Varman (2019) show that poor Indian immigrants juggle with conflicting conventions depending on their situations. In the Middle East, these immigrants draw on the domestic world’s conventions to resist the dominant market-based consumption culture. However, back in India, the same lower-class return migrants turn to market-based conventions while using their savings from the Middle East to transform their social status and to challenge their low positions in the traditional domestic hierarchy. Similarly, stakeholders in a mobile health initiative may draw on conflicting calculations of the benefits of standardization, including industrial conventions emphasizing planning and efficiency, civic conventions stressing quality for all citizens, and market conventions highlighting monetization and insurance payments (Cappel and Kappler 2019).
Boltanski and Thévenot (1999) describe three regimes of coordination: justice, agape, and familiarity. In a regime of justice, the principle of equivalence is most salient, and it draws on orders of worth that are dependent on socially accepted conventions. In a regime of agape, persons actively cooperate out of a sense of love and abandon equivalence and calculations of reciprocal conduct. In a regime of familiarity, a person is intimately engaged with familiar surroundings and people and follows customs specific to that arena, which are not available to any unfamiliar observer (Boltanski and Thévenot 1999). In this research, we found that a regime of justification and a regime of agape were salient in community palliative care. While this model emplaces care in patients’ communities, caregivers may not be familiar with patients and families. Hence, a regime of familiarity was not as relevant to our context. We explain the regimes of justice and agape in the following sections.
The regime of justice
Conflicting worldviews can often create disputes among individuals or groups. Actors involved in a dispute must adopt an “imperative of justification” by following the rules of acceptability to come to a resolution (Boltanski and Thévenot 1999, p. 360). Justifications equate particular notions of worth located within a world into more generalized notions of the social good. At the heart of justice is the emphasis on equivalence of worth. Boltanski (2012) suggests that people’s agreement on calculations of worth is a condition for creating justice. While individuals may resolve disputes through an agreed-upon principle of equivalence, the contemporary world is comprised of competing principles of equivalence. Boltanski and Thévenot (2006) describe six common principles of equivalence with their attendant notions of worth: civic, market, industrial, domestic, inspired, and fame worlds (see Table 1). These principles of equivalence follow rules of acceptability or conventions characterized by different orders of worth.
Regime of Justification: Different Orders and Indicators of Worth.
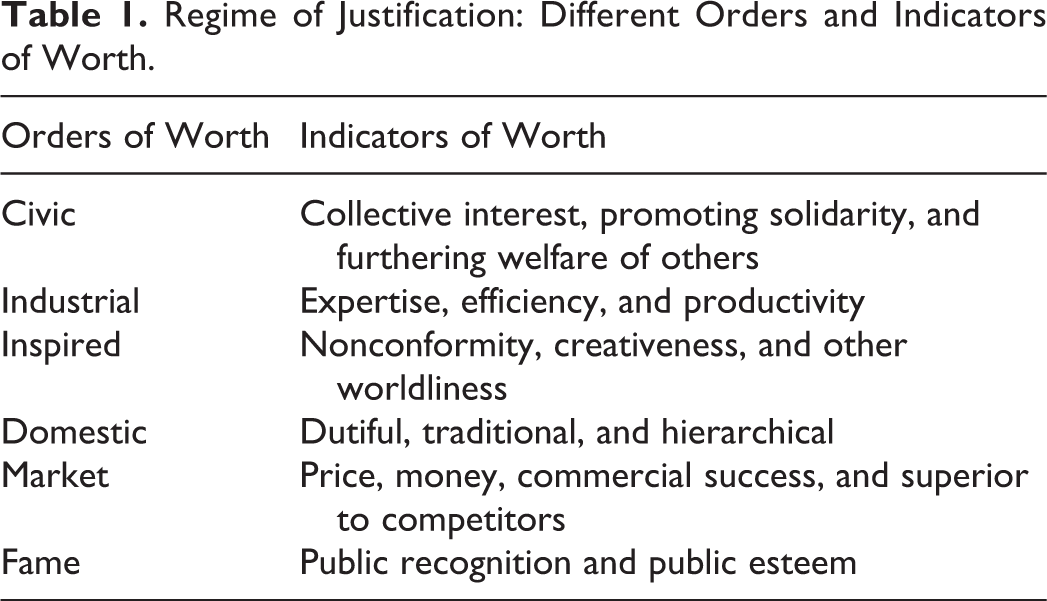
The civic world emphasizes collective interests, fairness, solidarity, and rule-governed behaviors (Thévenot 2001). In the civic world, a sovereign is created by the convergence of human will, as individuals give up particular interests, create solidarity, and work toward the common good (Boltanski and Thévenot 1999). This order of worth centers on collective persons governed by relations of equivalence. In this world, individuals attain worth by placing the collective ahead of their individual interests and forging solidarity. A worthy caregiver in this world, for example, rejects private gains and works for the collective good by collaborating with others and contributing to community health.
In contrast to the civic world, desires are shaped by self-interest in the market world. In this world, people compete for scarce resources to get ahead. Buyers, sellers, and competitors who engage in relations of self-interest populate this world. Here, people are detached from one another, and transactions shape their space of dependence. The worthy in this world can calculate and seize market opportunities (Boltanski and Thévenot 2006). For example, a worthy caregiver in the market world has commercial motivations, may seek to make private gains, and outperforms competitors to meet personal objectives. S-D logic’s emphasis on resource integration and strategic benefiting fits well with the market world.
The industrial world is constituted by “technological objects and scientific methods” (Boltanski and Thévenot 2006, p. 203). It is a world based on efficiency, and worth is measured through formal professional capabilities, performance, productivity, reliability, and predictability. The worthy person in this world is an expert. For example, a worthy caregiver, such as a physician or nurse in the industrial world, has standardized training, technical expertise, and qualifications to efficiently deliver health care. The relationships among experts in this world are effective when they are organized, measurable, and standardized (Boltanski and Thévenot 1999).
In the domestic world, worth depends on following traditions and a hierarchy of trust derived from personal interdependencies (Boltanski and Thévenot 2006). In this world, worth is assigned to a specific individual who is an insider. In our study of community palliative care, membership in a religious order is particularly salient. Worth is based on the intergenerational transfer of traditions and hierarchies and emphasizes duties, etiquettes, and maintaining ties. Worthy individuals in the domestic world are guided by traditions, such as those of a religious or familial nature, and are moved by a call for duty based on these preexisting structures to take responsibility for others who cohabit an order. Worthy caregivers, for example, follow traditions, maintain relations, and fulfill duties faithfully toward affiliated groups.
In the inspired world, the worthy know “how to recognize and welcome what is mysterious, imaginative, original, unspeakable, unnamable, ethereal, or invisible” (Boltanski and Thévenot 2006, p. 160). Here, the worthy are impelled by a higher cosmic order that makes them pursue desirable actions. Worth rests upon attaining a state of grace independent of reputational or financial recognition (Boltanski and Thévenot 1999). Accordingly, it can have many expressions such as creativity, artistic sensibility, and imagination. A worthy caregiver in this world disavows recognition or commercial gains and provides service for its intrinsic worth. For example, a physician following the inspired world’s conventions may shun a lucrative career to create an unconventional health initiative for the poor.
Finally, the world of fame is characterized by a relational order in which others ascribe worth to an individual. In this world, people desire recognition, seek public esteem, and crave respect. People achieve worth by becoming visible and recognized in a space where they can be seen and compared. For example, worthy caregivers in the world of fame are recognized and held in high esteem by the public for their services. In this world, a caregiver can cultivate recognition by using media and other public platforms that accord visibility. Hence, creating a public persona is of prime importance, and the banal is unworthy.
Convention theory attends to disputes in a given context. These conflicts can be internal to a world in which people notice flaws and violations of conventions (Boltanski and Thévenot 2006). Such conflicts are not major and can be resolved by improving the implementation of a world’s conventions. Challenges or tests arising in another world are more radical (Boltanski and Thévenot 1999). These conflicts arise because of different conventions and notions of worth that prevail in a social setting. People may forget these disputes or dismiss them as unfair because they are based on conventions stemming from another world. For example, the market world can reject disputes raised from the civic world as unfair because of contrarian conventions. However, these tests often cannot be negated, and disputes are not easily refuted. Such situations require reconciliation between worlds, which take the shape of compromises or the cohabitation of different conventions, changes to allow one world to dominate, or certain worlds becoming marginalized (Boltanski and Thévenot 2006). For example, if seen as justified in a setting, individuals can marginalize the market world’s conventions and replace them with the civic world’s conventions. Thus, conventions of different worlds lead to disputes that require reconciliations.
In sum, convention theory helps to facilitate understanding of different conventions of justice that cohabit a social space of collective endeavors for transformative service. The framework of conventions does not interpret collective endeavors as conflict-free activities. Instead, transformative arenas are fraught with people pursuing different orders of worth and conventions. Moreover, the same individual can pursue different orders of worth in different situations. Drawing on this reading, we analyze the role of different worlds with associated conventions under a regime of justice in shaping Kerala’s community palliative care.
The regime of agape
Some situations do not require the evaluation of justice and are outside the conflicting conventions described above. Boltanski (2012) suggests that agape as a form of love can be one such alternative to justice. Agape is a free gift that shuns equivalence; it is about detachment from worth and calculations that are central to justice. Agape does not contain desire, and it is sacrificial, unselfish, and gives freely (Belk and Coon 1993; Nygren 1953). As Boltanski (2012) explains, “persons in the state of agape neither hold onto things nor expect things” (p. 114). In articulating this view, Boltanski draws on Kierkegaard’s (1995) notion of love that is not a barter. Agape is not confined to specific spaces and a narrow circle of acquaintances. As Boltanski (2012) notes, “everyone in the state of agape gives to anyone he or she meets. But the one to whom the gift is addressed demands nothing since he or she sets aside the thought of desire” (p. 146). In agape, each person anticipates others’ needs, and those who have more give more, seeing the needs of those who benefit as their own needs. Here, others’ judgments are of little consideration, and as a result, agape abolishes justice (Nygren 1953). Hence, agape is inconsistent with S-D logic’s notion that actors operate with the calculative expectation of exchanging benefits.
Drawing on the work of Arendt (1958), Boltanski (2012) explains that the regime of agape resolves offenses by not punishing or forgiving people as justice would require, but by forgetting and dismissing such acts in the spirit of “life must go on” (p. 115). Agape rejects the past as a temporality that requires calculations of justice and embraces the present as the only temporal orientation. As Kierkegaard (1995) observes, “there must be eternal vigilance, early and late, so that love never begins to dwell on itself, or to compare itself with love in other people, or to compare itself with deeds it has accomplished” (p. 179). Hence, agape is not interactionist in which people’s anticipations of others’ responses would shape their behaviors (Boltanski 2012). Moreover, agape is often tacit and not visible to an outsider unless one interacts with insiders to understand their actions.
Finally, in the contemporary world, it is difficult to find pure regimes of agape from which calculations are entirely absent. As a result, agape coexists with regimes of justice. When people become calculative and enter into disputes, they move toward justice and exit the regime of agape. With such a shift, actions are scrutinized, and calculations of equivalence become dominant. Similarly, a person can shift from a regime of justice, gradually abandoning calculations and surrendering to agape (Boltanski 2012). In the subsequent sections, we examine the dynamics between different conventions and regimes of coordination in Kerala’s community palliative care system.
Research Context and Methods
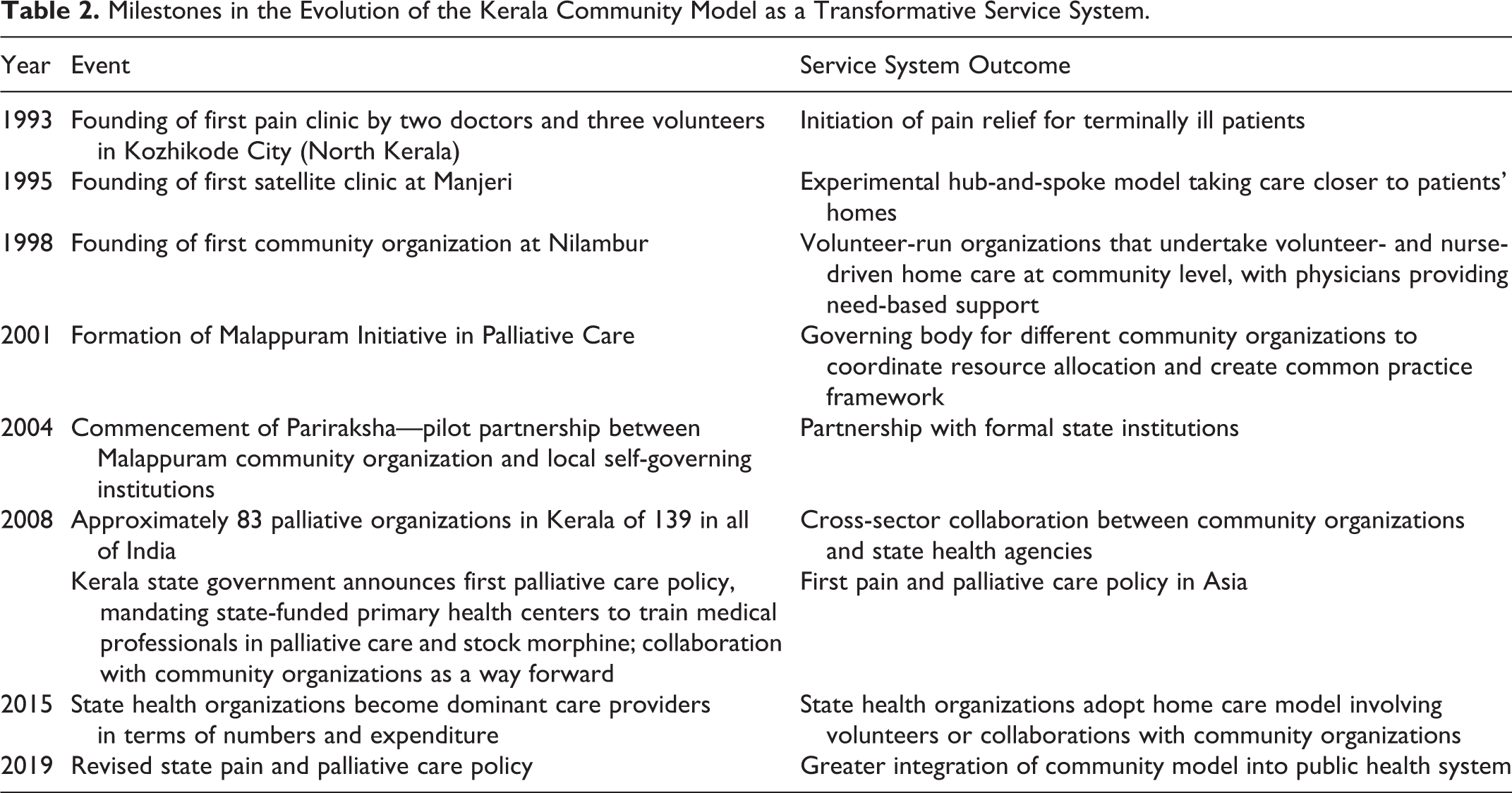
Kerala, located in Southwest India with a long coastline along the Arabian Sea, comprises about 1% of India’s landmass and 3% of India’s population (approximately 35 million). Kerala’s community palliative care started in 1993 as a doctor-run pain clinic at the Kozhikode Medical College (North Kerala) established to provide pain relief for terminally ill cancer patients. Besides a nascent palliative care clinic at Thiruvananthapuram (South Kerala), Kerala had no other facility at that point in time. Kozhikode’s resource-starved clinic drew on volunteers for administrative support. Volunteer engagement intensified with exponentially increasing patient numbers and a growing realization of the need for home care. Subsequently, early stakeholders experimented with different service delivery prototypes, eventually stabilizing a model of networked but financially and operationally autonomous community organizations. In this model, the fulcrum of caregiving, fundraising, and ‘decision-making’ shifted from a few medical professionals to thousands of community volunteers. Table 2 specifies the key milestones in the community palliative care model’s development as a transformative service.
Milestones in the Evolution of the Kerala Community Model as a Transformative Service System.
Volunteers come from heterogeneous social groups of class, gender, religion, and caste and work with patients in their neighboring communities. Volunteers typically are the patients’ proximate and frequent contact points. After receiving training, volunteers go door-to-door in neighborhoods to identify patients; visit families regularly; identify the psychosocial, financial, or emotional aspects of care; and serve as the voice for the patient’s and the family’s needs. Nurses constitute the first level of medical support and provide routine home care with volunteers. Physicians, as the most limited health care resource, conduct home care depending on the case criticality and complexity. Community organizations conduct “outpatient days” for patients’ consultations with physicians. The better-resourced organizations have in-patient facilities (e.g., 10 beds) for patients who needed critical medical attention or a change from their homes. Typically, community organizations pay physicians and nurses for their services, albeit a nominal amount compared to public- or private-sector service. 1 While physicians and nurses address medical symptoms, volunteers alleviate social suffering and collectively improve patients’ and families’ well-being (Kumar 2020).
As community organizations proliferated across Kerala, the scope of care expanded from advanced cancer to early-stage cancer; HIV/AIDS; chronic renal, respiratory, and cardiovascular diseases; mental health; and geriatric conditions (Vijay and Monin 2018). In 2008, responding to community organizations’ advocacy, the Government of Kerala introduced a policy integrating palliative care into the public health system. Currently, there are over 230 community organizations. More than 900 panchayats (village-level local self-governing institutions) designate at least one nurse for palliative care at each primary health center (PHC). Community organizations work formally or informally with the public health system (Kumar 2020; Vijay, Whitelaw, and Clark 2020). The Kerala palliative care system has more services than the rest of India put together.
Data Collection
This study is based on ethnographic fieldwork (Spradley 1980) on Kerala’s community palliative care system over 10 years between 2009 and 2019. During this period, the second author conducted fieldwork at 22 community organizations that were purposively sampled across the geography and founding period. To investigate routine activities, she participated in over 40 home care days (each home care day typically covered four to five patients) with nurses, doctors, and volunteers, during which she observed caregivers’ 2 interactions with patients and families. She attended service review meetings, participated in training sessions for volunteers, and observed how the volunteers introduced new care practices based on patient interactions. Additionally, she participated in international and national palliative care events, which furthered comparative insights into the Kerala model’s distinctive features vis-à-vis other service systems. Thus, her engagement with the palliative care sector was ongoing and deep. In 2019, the first and second authors jointly visited four community organizations to observe the caregivers’ interactions and relationships in such care settings. Field notes and researcher diaries were written either during or directly after the participant observation.
To understand the transformative nature of community palliative care, we conducted 145 in-depth interviews (McCracken 1988) ranging from 30 minutes to 3 hours over a 10-year period. Most interviews were in Malayalam. Fourteen interviews with physicians and state officials were conducted in English. We audio-recorded the interviews, and the audio files were translated into English and transcribed. Participants included physicians, nurses, volunteers, patients, family members, journalists, and government officials. Interviews with caregivers typically followed a narrative approach, beginning with questions about the participant’s background and then moving on to motivations to engage in palliative care, organizational practices, shifts in organization over time, and the impact of palliative care. In the last phase, we focused explicitly on caregivers’ life narratives, backgrounds, ideologies, religious or political commitments, articulations of caregiving, and interactions with other caregivers, patients, and families. We also curated a data set of 1,157 secondary data sources (e.g., newspaper data, journal articles, and organizational documents) published between 1993 and 2020, which helped reconstruct milestones, triangulate the data, and deepen our insights from the interviews and field visits.
Data Analysis
Over the years of fieldwork, we came across conventions from different worlds and witnessed agape in various forms. Our subsequent reading of convention theory gave us a conceptual understanding of the regimes of justice and agape, which guided the data collection and analysis in 2019. Our analysis involved three key stages and used an abductive approach (Dubois and Gadde 2002). First, drawing on Boltanski and Thévenot (2006), we started with an initial analytical framework based on convention theory, which was particularly relevant because the community model comprised disparate groups and diverse situations. We coded all passages—in a sentence or paragraph—corresponding to the “orders of worth” actors mobilized in their justifications for participation. Table 3 provides the semantic markers for each common world and illustrations of the coding process (cf. Patriotta, Gond, and Schultz 2011).
Semantic Markers of the Common Worlds and Illustrative Quotes.
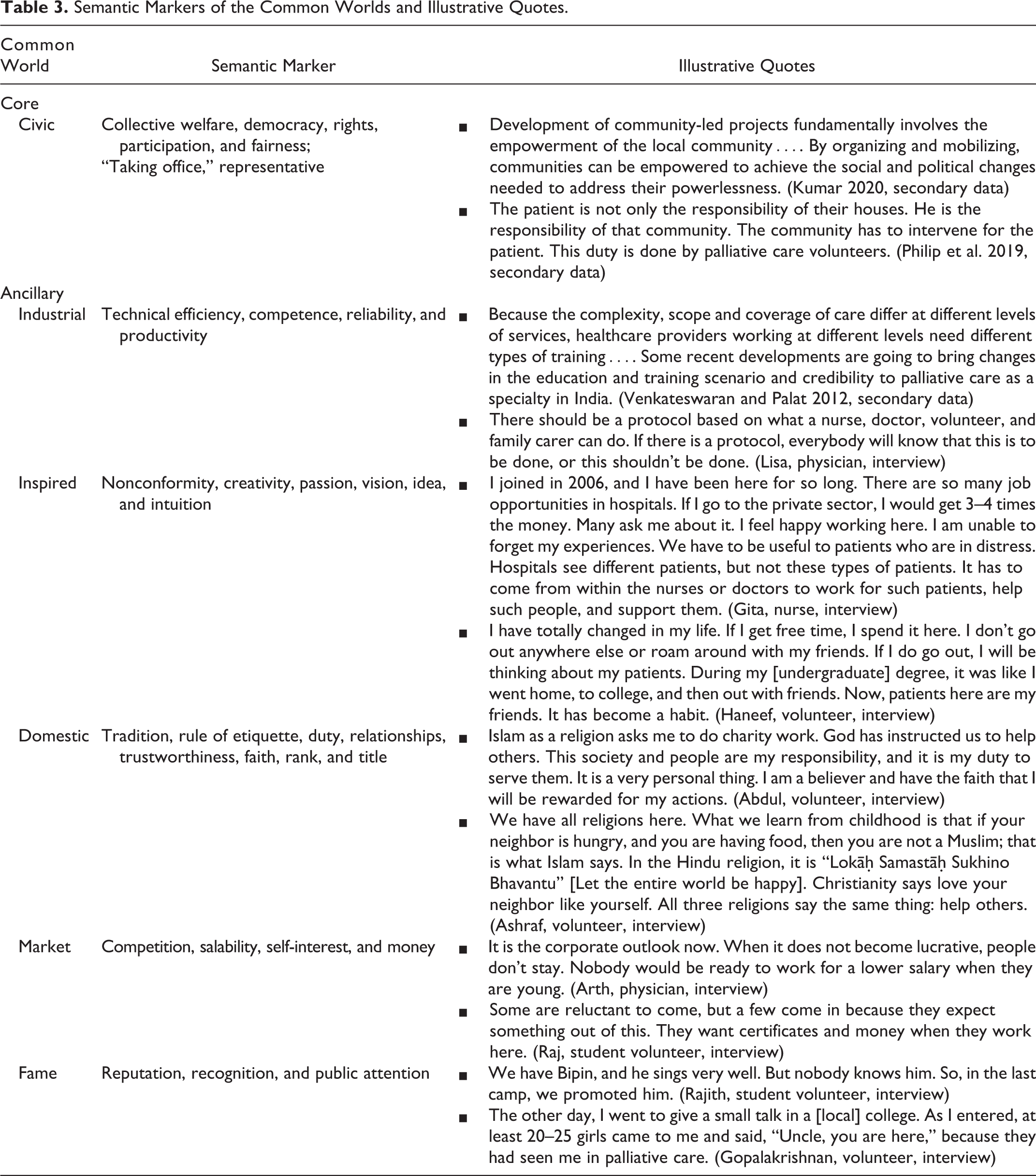
Certain accounts referred to multiple, intersecting worlds. Thus, in our second stage, we attended to conflicts and how they were resolved. Finally, based on an iterative reading of the data and literature, we mapped Boltanski’s (2012) conceptualization of agape to data that evidenced participant accounts of “unbounded care and love” and a “suspension of calculation.” We draw on this analysis to present our findings in the next section. We use pseudonyms to maintain participants’ anonymity, except in cases of explicit consent and when participants’ names and opinions are available in the public domain.
Findings
Our findings show that Kerala’s community palliative care constituted a transformative health care service in which diverse conventions came together under a regime of justice. We also show that a regime of agape is central to such a transformative service. We derive a framework of a transformative service system (see Figure 1) based on our findings as they are interpreted through the lens of convention theory (Boltanski 2012; Boltanski and Thévenot 1999, 2006).

Framework of transformative service system.
The Regime of Justice in the Community Model
The regime of justice is characterized by a distinction between core and ancillary conventions (see Figure 1). The civic world’s conventions constitute the inner core of community palliative care. The outer conventions, which we see as ancillary but not insignificant, are made up of transactional, marginal, or nascent care engagements in the industrial, inspired, domestic, market, and fame worlds.
The core convention of the community model
The civic world
The core constitutive feature of the community model is the civic world. As explained in the research context, caregivers from diverse backgrounds coordinate to deliver community-based care. This model draws on civic conventions in which worth is assigned to collectives that occupy public space, where aspirations anchor around civil and political rights and participation (Boltanski and Thévenot 2006). In the civic world’s defining situations, caregivers commit to solidarity, work in the spirit of a common good, give to society, and alleviate public suffering. The civic world of community palliative care entails mobilizing volunteers, spreading awareness, microfundraising within communities to create ownership, and enlisting support from other institutions.
Anil Paleri was one of the physicians who worked with the first Kozhikode palliative care clinic and participated in the transition to community care. Paleri explained: Once these centers started working independently, it was up to them. Raising funds…everything. The feedback from the community also goes back to the center. We made sure that we did things in a good way, and all the benefits went to the community. This has been a motivator for the people to work. Whatever they do, they get an immediate positive response from the community.
Caregivers included community members, such as farmers or bus drivers, with primary or secondary education. They articulated a moral responsibility to participate alongside medical professionals in care delivery. For example, Unni, an autorickshaw driver who volunteered, shared the moral imperative that draws on the civic world: We give patients and families relief and care. We can’t do this in a day or two. We visit for several days. This gives them the belief that we are there for them. We try and reduce whatever pain and sorrow the patient has. We listen to them patiently, understand their sorrows, and do whatever we can to help them in our own ways. The patients may not admit that they have not taken medicines or food; we need to understand that situation. We may help with their children’s education. The involvement of volunteers is essential. There might be a shortage of nurses and doctors, but area-wise, volunteers do most things.
Unni and Satya struggled with socioeconomic inequities but were committed to civic and political participation in community care as expressions of justice to challenge inequities. In contrast to Unni’s and Satya’s impoverished financial backgrounds, Madhavan, from a middle-class family, engaged in this civic world after retirement. Having spent his professional life working in a multinational conglomerate overseas, he wished to “give something back to society” after retirement. Madhavan noted: That was my passion while working. I wanted to work with an NGO [Non-Governmental Organization]. I had been earning for a long time, and at some point in time, you have to give something back to society. Palliative care is the need of the day. We do everything free of cost. There is a need to help the needy. Not only the poor are in need; it can be anyone. We cannot live like this. You need the support of an entire group of people. That is what I meant by giving back to society—so my existence should benefit people living around me, not just myself.
In sum, caregivers drew on notions of civic responsibility and social justice to describe their commitments and the nature of transformative service. While individuals calculate community caregiving as a form of reciprocal justice, it is infused with a civic order of worth and a moral imperative that offers an alternative to the market logic of buyers and sellers and the industrial logic of efficiency.
The ancillary conventions of the community model
The industrial world
In the industrial world, the worthy are professionals with expertise and those who emphasize an organization’s functionality, reliability, and operational performance (Boltanski and Thévenot 2006). The industrial world surfaces in situations where medical expertise is paramount. Although this world, with its emphasis on trained doctors and nurses, was dominant in the founding years (notably 1993–1997), it became ancillary to the civic world with the spread of the community model after 1998 (see Table 2). At an international seminar in 2004, Suresh Kumar reflected: In this model [doctor-centric], there is no continuity of care…. We have been trying to work on this, and after a lot of deliberations, last year, in August 2001, we started a new program. It’s on a trial run in a small district, one of the poorest districts in Kerala, Malappuram, a district with a population of 4 million. It’s…called Neighborhood Network in Palliative Care (NNPC), aimed at training helpers and volunteers in the community and supporting them with trained professionals. (Kumar 2004 as quoted in Reynolds and Tansey 2004, p. 55) First, in palliative care, they taught symptom management, psychological support, and social support. Then, it came to the second major stage, and some were involved for social service, and others for spiritual reasons. But now, all types of people can do it. Now, palliative care is a right.
Nevertheless, some physicians emphasized the worth encoded in the industrial world. While participating in the civic world of health rights, physicians may also attach worth to the professional world, with its arrangements of qualifications and capabilities to ensure quality (cf. Boltanski and Thévenot 2006). In an article describing the services delivered by the Trivandrum Institute of Palliative Sciences (TIPS) and Pallium India, Krishnan et al. (2018) wrote: Given the vast need for palliative care in the community, a balance of quality care and coverage is challenging. Pallium India’s initiative, which resulted in the creation of a minimum standards tool in palliative care, is aimed at drawing a line below which the service should not drop. Nevertheless, the line seems too low, and services are often inadequate. A weekly home visit is hardly sufficient to ensure reasonable quality of care for a patient with advanced cancer. Palliative care service must maintain some minimum standards, which should be respected. There should be at least a certain number of hours of training. Plus, if you do not follow up with mentored practical training, the effect could be adverse. This is not only for volunteers but also for doctors and nurses. It is easy to do harm. As the expertise drops, the potential to do harm increases. Minimum quality standards are very important because if we don’t follow them, we have the potential to do more harm.
In sum, in the industrial world, worth is assigned to those with technical expertise because they are considered optimal for providing palliative care. As Boltanski and Thévenot (2006) note, in this world, “the scale of qualification underlies a hierarchy of status of worth, a hierarchy marked by competencies and responsibilities” (p. 206).
The inspired world
The inspired world exercises worth with attributes that cannot be measured by the market or industrial forms. These attributes manifest as independent actions, passions, and rejections of dominant norms (Boltanski and Thévenot 2006). Although these situations are not common in our setting, they are exemplified by caregivers who refuse to follow the dominant norms of making money or pursuing stable jobs to chart their course. An illustrative situation was Suresh Kumar’s commitment to community care. He recollected: In 1993, I had two jobs. I was an anesthetist and was also volunteering. By 1995, I moved full-time into [community palliative care]. I was the secretary for six years, then someone else came in. Now, I am a regular member; being a member does not mean I get any extra benefits. It just means I must put a bit more time into this. Doctor Suresh is our role model. He is a very simple person. He enjoys being with us. Almost all the doctors here are very simple, loving, and happy. There is no hierarchy here, so these are elements that differentiate us from other places.
Highlighting a similar calculation of worth, Chitra Venkateswaran shared that her quest for a meaningful affiliation led her to a postgraduate medical specialization in psychiatry. Her subsequent foray into palliative care, however, was transformative: There was always a restlessness to do something more. It was undefined at those stages. I was looking for something that could give meaning. Palliative care principles, or the broader philosophy, apply to every kind of care that you give. I think my life changed after this whole thing. The whole path, approach, me as a person, the way I care for people, the way I manage people, and my team…everything has changed.
The domestic world
The domestic world refers to worth ascribed not just to family relationships, but to relationships of personal dependence (e.g., superiors or visitors) shaped by tradition, hierarchy, and habits (Boltanski and Thévenot 2006). Specifically, in some settings, caregivers highlighted the domestic world’s significance by pointing to religious traditions. Consider Abdul, a founding member of a community organization in Malappuram: Our religion tells us to help others. If we have earned well, then people who are struggling automatically have a share in our earnings. We have been instructed by God to help others, and surely, we will be rewarded for our actions.
While Islamic practices are salient, particularly in North Kerala, Jayakumar, a volunteer at Aluva (Central Kerala), justified his involvement in terms of the Hindu principles of karma: We don’t expect benefits. Maybe we can hope our family will get benefits. Karmanye vadhikaraste ma phaleshu kadachna, Ma karma-phalahetur bhur ma te sangostvakarmani [You have a right to perform your prescribed duty. You are not entitled to the fruits of action. Never consider yourself the cause of your activities’ results, and never be attached to inaction or not doing your duty]. We cannot do our work expecting results. If our work is sincere, we will get some results. But we do not expect results. All we say is that whatever we get is enough.
The market world
In the market world, self-interest, self-promotion, and outperforming competitors are of paramount importance (Boltanski and Thévenot 2006). We found situations in which caregivers offered services temporarily to further market goals. For example, Ram, a 25-year-old, shared how his leadership and communication skills improved after joining community palliative care as a volunteer during his undergraduate degree: I came to palliative care and did a leadership program. I am usually given the responsibility to deliver presentations. We attended a conference. There were people from different countries. I had the responsibility to coordinate things. When [LS] Sir came here for an event, out of 15 people who had gone there, he recognized me. This was because of the work that I did. That is how we build relationships. When we went to [the conference], our presentation won certificates. I have a platform here, which is leadership. I have a chance here.
Consistent with S-D logic’s view of calculations impelling actors (Vargo and Lusch 2016), the market justification illustrates how individuals engage in resource integration and value cocreation, not only for others but also to calculate benefits for themselves.
The world of fame
In this world, recognition and public opinion establish the caregiver’s worth (Boltanski and Thévenot 2006). Some situations highlighted the world of fame in the community model. For instance, Jayesh, a volunteer, shared the following: I got involved with palliative care in a big way. When we would get in a vehicle and drive to my neighborhood, people began to recognize. “I saw you earlier, driving that vehicle. What was that about? Oh okay, this is a very good initiative. It is a very good thing that you are doing. You must do this for people. It is important.” As a result, I got more deeply involved in this. Now, I’m involved in such a way that I cannot leave.
We also found that individuals interested in joining electoral politics realized that community care garnered them grassroots-level legitimacy and recognition, which could help them to further political careers. Participants gave the example of Saji Cherian, an elected representative of the state legislature from Chengannur city, who had worked as a volunteer and headed a community organization. He gained recognition in electoral politics and earned popular votes based on his palliative care work. Satya told us: That is not an area [Chengannur] where CPM (Communist Party-Marxist) has influence. Saji Cherian won beyond the expectations of CPM. He was a popular palliative care volunteer in that district. His success is very good. CPM expected he would win by 5,000 votes. He won by 10,000 votes.
In summary, the civic world defines the core of palliative care. The industrial, market, inspired, domestic, and fame worlds also shape transformative service situations. It is therefore erroneous to attach an individual to a single world. We witnessed a variety of situations because a diverse set of actors came together to offer palliative care. The diversity manifests in multiple orders of worth, which may also lead to conflicts between different worlds.
The Core-Ancillary Conflicts as Unintended Consequences of Multiple Conventions
Although there is a wide range of conflicts between different worlds, we focus on the key conflicts between the civic and ancillary worlds. These conflicts are unintended consequences that arise when caregivers weave together multiple conventions from diverse worlds in a transformative service system. Conflicts arise because worth is put to the test by conventions of different worlds (Boltanski and Thévenot 2006).
Challenging the core from the ancillary
A key dispute in the palliative field is over volunteers participating in the professional domain of palliative care and the potential dilution of professional care. Although the volunteers had been involved in palliative care since 1993, there were still situations where some physicians resented their role. In this clash, the industrial world’s attributes of specializations and expertise are considered worthy and are applied to test the civic world’s worth (Boltanski and Thévenot 2006). Hema is a physician who founded a nonprofit organization and engaged volunteers for palliative care. Consider the following situation Hema raised about monitoring the quality of volunteers’ care: I have been with palliative care for the last few years. We are getting more volunteers, and I know training is important. We train, but we find it difficult. The more volunteers we have and the more we expand…how do you monitor and evaluate them? We are sending people. This is my organization, and I am sending you into the community. They are going as volunteers, but are they doing the right thing? How do we monitor and ensure what our volunteers are doing? Some might be giving them [patients] some information. Some might be treating them. I don’t know! It is a very delicate balance with volunteers because you are not paying them, so they are not accountable to you. There is a sense that I am doing you a favor by volunteering my precious time. Therefore, I am above your rules and regulations. That is not okay because you are coming here to help. The kind of leadership that needs to be demonstrated to volunteers is to say that “we are asking you to undergo a certain amount of training. We are not saying you are not good enough. You want to do a good job. You don’t want to do damage where you intended to do good.” I think it should be mandatory that they go through at least two to three levels of training, and that they are assessed, examined, and then allowed.
Challenging the ancillary from the core
In this type of conflict, disputes arise when the civic world denounces the ancillaries as they manifest in the community model. The conflicts between the core and the market or fame world became particularly salient in more recent years with the increased number of caregivers. Newer entrants may have been offering services for shorter periods and may thus have been impelled by market or reputational gains. Senior caregivers resented such emphases and used conventions from the civic world to challenge these actions. Philip, a volunteer involved since 2003, critiqued quests for worth in the fame and market worlds: Some want to take credit. We avoid taking photos and all. Earlier, if we gave 100 rupees for charity, no one would come to know about it. Now, if people give 10 rupees for charity, they want to take a photo if I am giving 1000, what benefits am I getting? There are some basic things we learned during training. People are getting diverted from that. For the doctors who are here today, it is an earning thing for them. The medicines that they give are prescribed according to the pharma companies. They [doctors] can do it differently without using costly medicines. Earlier, we discussed all the patients’ cases with the doctor. Now, they have no time. One should have interest. Palliative care is not just a job because it is not a very pleasant thing. When we go for homecare, we may have to climb on top of a mountain to see one patient. If I am cursing the mountain and the patient, what palliative care am I going to offer? So, anybody coming for palliative care should not approach it as a salaried position or a job. The attitude of the person is very, very important.
In sum, we witnessed several conflicts between the core and the ancillary worlds. Thus, it has been shown that while a test from the industrial world primarily marks the most salient challenges to the core, denunciations from the civic world challenge the ancillaries.
The Reconciliation of Conflicts in Transformative Service
Conflicts arise as unintended consequences of a transformative service with arrangements in different worlds. We identify three key ways in which conflicts are reconciled: compromise between core world and ancillaries, resolution in one world, and discontinuation of participation (see Figure 1).
The compromise between the core and ancillary worlds
Caregivers may resolve core-ancillary conflicts through compromises. A compromise is a situation in which conventions from opposing worlds are allowed to coexist (Boltanski and Thévenot 2006). Medical professionals, who emphasize professional care, and caregivers, who foreground social care, create compromises by drawing on the conventions of opposing worlds (i.e., the industrial and civic worlds). Some medical experts acknowledge these compromises. For example, despite medical expertise, Rajagopal acknowledged the following in a media article (Malayala Manorama 1995): “volunteers are the backbone of this establishment. Volunteers work hard without expectations of monetary gains. Volunteers carry the primary responsibility at this clinic.” Similarly, Mohammad, a physician employed by a community organization, reflected on the compromise between the industrial and civic worlds: When we see some volunteers’ notes, they know how to manage the patient better than the doctors. They know the patient very well. Community volunteers are people living in the neighborhood. I live far away. They [volunteers] know the patients very well; they know their relatives, and they know who cares for them. Doctors and nurses don’t have those insights. Volunteers are a must.
A compromise between different worlds became salient in collaborations between the community organizations and state-run PHCs. While the latter were expected to collaborate with community organizations, state procedures dictated their everyday functioning. Numpeli described how early community organizations conscripted the PHCs into providing care. While some PHCs expressed interest in supplying medicines and catheters, their nurses were overburdened and unavailable. Numpeli explained a compromise creatively engineered between community organizations and PHCs: In Nilambur and Areakode, the community organizations told PHCs, “We will provide the nurses.” They sent nurses from [community] palliative care to a PHC. This is not a small thing. It could manifest as “we are good people, and you are useless”—that kind of approach. We did not take that approach. We told them, “You can do it. We will help you.” We sent nurses from here, and it was a success.
The resolution in one world
We found that individuals reconcile disputes by using one world’s conventions to justify a moment of truth while holding other worlds as less worthy. Unlike reconciliation as a compromise in which contradictions between core and ancillaries coexist, resolution in one world is achieved by rejecting the ancillaries’ conventions and allowing the civic world’s conventions to dominate. Here, individuals reject all ambiguities that might allow “alternative truths” to emerge (Boltanski and Thévenot 2006, p. 138).
During a field visit to one of the early community organizations, we met Amjad, a volunteer from a working-class family who had dedicated nearly 20 years to community palliative care. He expressed deep anger over a few pioneering physicians receiving media accolades, government and civil society awards, and international recognition since the community model had developed through the grassroots with the support of community actors typically from working-class or lower middle-class backgrounds. With indignation, Amjad remarked, “Palliative care is of the community. How can one individual get an award?” Here, the volunteer equates palliative care with the civic world and rejects the world of fame. The primary order of worth here is the community’s collective participation.
In these situations, dispute settlement between the civic and ancillary worlds occurs by rejecting the latter’s worth. In a similar vein, some senior caregivers denounced a flash mob organized by student volunteers as a palliative care awareness campaign, and they stopped the volunteers from organizing such activities. A volunteer explained, “They [the senior caregivers] say that ‘a flash mob is not palliative care. It is not suitable for us.’ There is such a kind of control here.” Senior members deploying the civic world of participation condemned the youth flash mob initiative as a spectacle for fame. Here, “control” implies that volunteers resolved this conflict in the civic world and rejected the ancillaries’ conventions.
Similarly, some participants opposed the founding of community organizations that identified with a specific religion or party ideology. Philip stated, “There is a new trend now: Christians have a palliative care organization, and Muslims have different ones. Our [community palliative care organization] is a common ground.” He was emphatic that palliative care must be defined by the civic conventions of solidarity and collective welfare rather than the hierarchies and traditional conventions of religion in the domestic world. Thus, while various motivations—including religious or political ideologies or professional commitments—may inform individuals’ actions, participants pointed out that an organization cannot espouse a single religion or ideology.
There is a similar rejection of the market world of money. For instance, Misa, a homemaker who volunteered, shared how even if she could make money during the time she volunteered, this would be incomparable to her service: In this time, I can make 100 rupees more, but what will I do with that money? I can do something for my children. What else can I do? I should do something useful for society. I need only this much money. There are no other needs for me.
The discontinuation of participation
In some situations, neither an acceptable compromise nor a resolution in one world is feasible. Consequently, caregivers may discontinue participation. It was found to be common to see caregivers discontinuing after training or a few months of service. Such caregivers typically failed to come to terms with the civic conventions and found it difficult to sustain services. Mathew, a volunteer trainer, shared how publicity as a marker of the world of fame had limited potency in such care settings: If I am coming for publicity, I cannot stay here because here there is a lot of pain, a lot of compassion, and a lot of care. After a few days, I realize that there is no space because most of them suffer in pain. If I am only looking for fame, there is no space for that. We reach that place automatically [and quit].
We also found instances where participants discontinued participation when the ancillary worlds crowded out the civic world’s worth. For instance, Shafiq shared an example of a failed community organization in Palakkad district: In my region, there was a palliative care organization that began three times and failed. Through this, I learned one lesson. It did not fail because of a shortage of funds. The people founding the organization had problems attracting and retaining people. They were the hindrance to others joining the organization. Like gatekeepers. Later on, I realized it’s all about teamwork. There should be no concept of a leader, or one person who uses the charitable organization for personal benefits that are different from the organization’s aims and purpose.
In summary, we have surfaced the unintended consequence of conflicts between different worlds stemming from the multiple orders of worth. We have also explored three approaches by which individuals reconcile these conflicts. Our findings show that at the core of palliative care is a partial rejection of the regime of justice to offer care. We discuss the regime of agape as an important feature of transformative service in the next section.
The Regime of Agape in the Community Model
In the earlier sections, we have shown how the community model provides transformative service at the interstices of multiple worlds of justice with accompanying conflicts. We also found the regime of agape to be an unintended but highly desirable component of the transformative service system, as illustrated in Figure 1. Here, we detail those moments in which actors discard strategic and calculated actions and operate in a regime of agape where they offer love and unbounded care. Agape is an unintended consequence because caregivers do not strategically design agape to further palliative care. Rather, agape is an emergent feature of the community model when caregivers commit to offering transformative service.
Love and unbounded care
Most caregivers join the community model as part of civic participation. As they immerse themselves in alleviating vulnerable patients’ suffering, they experience agape or giving gratuitously as part of love in certain situations. Agape makes no demands, and one of the pathways to agape is to anticipate what is not requested (Boltanski 2012). Consider Zainab, who had volunteered for 6 years since the start of her undergraduate program. Zainab’s first patient left an indelible impression on her: My first cancer patient that I took care of influenced me tremendously. I met [patient’s name] only three times. Even after we knew he would not be there with me for long, it was a loving relationship. I know his parents, who are also palliative care volunteers, and they are great people. Whatever I have done afterward is for [the patient’s] mother. She is very close to me. I cannot express the emotions I have for her. It is unconditional love toward her. We not only give medical help, but we also provide food, medicines, and educational help for the patients’ children. It is basically total care. Irrespective of caste, creed, and religion, every person benefits. When they go home, patients will not have money to pay rent. They don’t have anyone to help them. We will do something for them, like give them a small mobile phone or food items. We arrange small funds for their small requirements. We are not expecting anything back. This activity doesn’t have a definite time for work. Volunteers first go and check the patient’s condition at their houses and inform us so that we can see if a doctor and nurse are needed. Volunteers are always busy. There is no day and night for them. If someone is unwell, it is a must for the volunteers to check on the patient. Also, the [volunteer] meetings happen in the mornings, evenings, and any time. Once my shift is over at 1:30 p.m., I will be here by 2 p.m. [at the community center], and I stay until 8 p.m. If I have a night shift, I just go and freshen up, and by 12 p.m., I come here. There are limitations to treatment. Through palliative care, we must understand that there are no limitations of care. Can we say that we can give only so much care? No, we can’t say that because we can always give care. But there are limitations to treatment.
Suspension of calculations
In the regime of agape, care as a gift to the recipient is not envisaged with the expectation of a countergift; acts in a regime of agape occur without any particular calculation. As Boltanski indicates (2012), “All persons in agape impoverish themselves in response to the impoverishment they encounter” (p. 147). Indeed, Geeta started volunteering when she and her husband had a 3-year-old daughter and a mortgage. She recollects a patient telling her, “Why do you come here for free work? If you are at home, at least you can pull out the weeds in your front yard.” Despite such reminders of losses, Geeta volunteered full time for years, forfeiting private gains even when her family faced financial hardships, and her husband was the sole breadwinner.
Several elements of giving without calculations in agape are corporeal. For instance, we met a young volunteer in her 20s who donated a kidney to her patient. While such instances are rare, corporeal commitments in the regime of agape are routine. Consider, Satya who had conducted a 2.5-hour training session for volunteers the day we interviewed him despite recovering from a knee fracture; he had started walking only a few weeks before our interview. He explained as follows: In 2.5 hours, when I was teaching the class, I did not know about that pain. This is possible only with that level of dedication. After some time, people think of family, jobs, and other things. These are individualistic things. I am not saying to keep those things aside. But one has to be ready for a “denial.” They have to sacrifice (tejjikyuan tayar avanam) something in life. Without this, people cannot work in palliative care.
Radha, a volunteer from an agrarian family, reminded us of “the insouciance of agape” in giving without any calculation of gain (Boltanski 2012, p. 114): We don’t even take a glass of water from them [patients] when we are there for service. I am not working for money. Everything is going on smoothly. I am not expecting anything from them.
In summary, agape is central to transformative service. We are not suggesting that caregivers always operate in a state of agape, nor are we maintaining that transformative service is not possible without agape. Indeed, prior S-D-logic-informed TSR has shown that interventions and organizations relying on justice can create transformative service (e.g., Anderson et al. 2016; Baron et al. 2018). Rather, we posit that agape is an important facet of the care provided that, when overlooked, renders service provision as a calculative practice enmeshed in a world of equivalence. In the following section, we elaborate on how patients experience the community model as a transformative service.
The Community Model as a Transformative Service
For socially disadvantaged and vulnerable patients, the community model delivered transformative service. Consider Achapan, a 70-year-old from the Adivasi (indigenous or scheduled tribes) community, which was among Wayanad’s poorest. Achapan and his wife lived with their daughter, who had a speech disability, and her son. This family lived atop a hill in a two-room house built through a state welfare housing policy for the Adivasis. When we visited Achapan, he was grieving for his son, who had died 2 weeks prior from an undiagnosed condition. Around 2009, Achapan had suffered a paralytic stroke while doing manual labor and was bedridden for a few years. He had partially recovered and would walk 12 km through Wayanad’s hilly terrain to the nearest PHC for consultations and medicines. Achapan shared the following: I had to climb to go to the hospital. I had to spend money. I cannot walk by myself from here anymore. I cannot travel or walk alone. Now, they [community caregivers] will come here. They give me English medicines [allopathic medicines]. Earlier, I used to buy them. These were very expensive at 200 rupees [monthly expense]. I get 1000 rupees in a month as wages.
While low-income families valued free medicines and regular nursing care, middle-class families valued direct access to professionals and the volunteers’ social support. Consider the experience of Shazia and Naz, a middle-class couple residing in Kozhikode city, whose 3-year-old daughter died of cancer after treatment and two relapses. Their child received palliative care in the last 3 months of her life. In contrast to their long, nightmarish waiting hours at the government hospital for cancer treatment, they were relieved by the round-the-clock access to senior palliative care physicians at their homes. Shazia shared, “It [community palliative care] is given by veterans! These doctors, especially I should say [a senior physician], would pick up the call anytime.” Shazia recalled the volunteers’ care: I was amazed. We actually got to see the volunteers’ strengths. How much they were doing! Even the driver, he comes home. He left this job, and since then, he has still stayed connected. He spreads the word. He talks about this service. He goes to people to tell them more about how it works. They take care of everything there [referring to the community model]. They connect with you so much. They also supported us emotionally, and even after the death, they were with us, and they continue with it. When we go there and come back, we feel happiness.
This community model also transformed the lives of patients confronting social isolation. For instance, Kannan was bedridden after an accident and confined to one room in his parent’s house for 26 years. Kannan’s release from isolation, abandonment, and neglect came when a home care team visited his house for a neighborhood survey: There should be a person in the house who understands. Otherwise, one’s life is hell. We lay in a corner and rotted. We were like birds without feathers—alive but afraid. For people like us who have spinal injuries, this [community organization] is like a big family and is a sandhvanam [palliation], or a blessing. Nine out of 10 of us need emotional support. If we get a person who understands this and just listens to us, that for us is the blood that runs through our body. Now I am like a bird with new wings. I can fly. We have had so much change because of this organization and its camps. Day or night, they do not abandon us. They have good hearts. These people have shown us that they are also like us. They don’t have the notion of being a doctor, nurse, or volunteer. They behave like one of us, sit, and have food with us. It’s not a profit-making venture—it’s not seeking a reputation. We want it to grow; that is our prayer. What one gets from a family, one gets much more here. For a patient who lies in his house without seeing the light of the day, what he gets out of this is a new life.
In summary, the community palliative care model is a transformative service system that has significantly improved health care access, particularly for the marginalized in Kerala. This transformative service attracts caregivers from different walks of life and creates situations involving conventions from different worlds with conflicting orders of worth. Regimes of justice and agape constituted transformative service in Kerala. The two regimes of justice and agape have been shown to be porous, and we found that caregivers can cohabit these positions or move from one to another, depending on their situations, to offer care.
Discussion and Conclusions
In this article, we show that community palliative care is a transformative service that has generated uplifting change and well-being for millions of patients with chronic and terminal conditions in Kerala, India. In a setting where the state-run interventions are overburdened and private enterprises have failed to cater to the poor, community caregivers have offered transformative service to the most vulnerable. Our attention to multiple conventions and the regimes of justice and agape foregrounds the undesirable and desirable unintended consequences of a transformative service system (see Figure 1) and helps to conceptualize a dialectical framework. Accordingly, we make several contributions to TSR.
Incorporating S-D logic, Vargo and Lusch (2016) define a service (eco)system as a “relatively self-contained, self-adjusting system of resource-integrating actors connected by shared institutional arrangements and mutual value creation through service exchange” (pp. 10-11). S-D logic has played an important role in shaping TSR (Baron et al. 2018) and specifically studies on health care (e.g., Anderson et al. 2016; McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015). This research stream has shown that emphases on the cocreation of value and resource integration can foster individual and collective well-being (Anderson 2010). While these studies offer vital insights, they monochromatically limit TSR to the exchange paradigm (Belk and Coon 1993).
In contrast, we argue that transformative service is constituted by a complex palette of relationships. Our study suggests that S-D logic and its concepts, such as resource integration and value cocreation, inadequately explain transformative service because of the focus on calculative market exchanges. Based on our findings, our framework contributes to TSR by conceptualizing a transformative service system as a dialectical synthesis of the regimes of justice and agape. Such a system offers care that generates uplifting change, promotes well-being, and alleviates suffering. In our framework of a transformative service system, actors construct transformative service around the civic world’s core conventions that value solidarity, collective welfare, civic responsibility, and participation. This core world is interwoven with ancillaries—the industrial, market, domestic, inspired, and fame worlds—for service provision. Our framework shows that transformative service involving community participation requires attention to different orders of worth. Indeed, there is a need to broaden our understanding of TSR to include disparate conventions within the regime of justice.
We found that the civic world, which emphasizes moral responsibility and solidarity, is central to transformative service. Our findings show that S-D logic, with its focus on individual gains and responsibilities through cocreation and resource integration, may crowd out the civic world’s imperatives and hamper transformative prospects in settings of stark material inequalities. While this is evident in our Global South context, the limitations of S-D logic can also be determinantal in the Global North. For instance, in their ethnography of a nonprofit delivering transformative value in the United States, Blocker and Barrios (2015) highlight varied processes of constructing communitas, facilitating spiritual flow, and demanding civic responsibility. These elements resonate with our findings of diverse ancillaries (e.g., inspired and domestic worlds) interwoven with a transformative service system’s civic core. Thus, our framework underscores the need for attention to a broader set of conventions.
We further show that such a palette with diverse conventions leads to the unintended consequence of disputes between different worlds. While the institutional perspective in S-D logic (Vargo and Lusch 2016) engages with contestation by focusing on interinstitutional conflicts, attending to conventions offers distinct advantages. For example, although institutional studies point to how services are exposed to competing demands from different institutional logics (Thornton et al. 2012), we know little about how conflicts between different worlds impact service provision at the microlevel of everyday actions (Cloutier and Langley 2013). We surface the multiple conventions governing everyday service situations, the conflicts arising thereof, and their reconciliation. Such a framework foregrounds the unintended consequences of interwoven worlds inherent to a transformative service. These consequences include the conflictual situations that arise when actors draw on the assumptions of ancillaries to challenge the core or when the civic core creates situations of disputes with the ancillaries. If unresolved, these conflictual situations can fragment the transformative service system.
We illustrate three types of conflict resolutions: compromise, resolution in one world, and discontinuation of participation. Conflicts as unintended consequences between linked worlds and conflict resolutions operate in the regime of justice characterized by calculations. We show how caregivers driven by the industrial world deem technical knowledge superior to the civic world’s social interventions. We also report disputes between the market and the civic world in routine actions and explain how individuals reconcile disputes between different worlds. Compromises can be fragile, and they highlight the challenge of multiple, conflicting worlds. Further, if a conflict is resolved by denouncing the civic world in favor of the market or fame wosrld, it may limit the service’s core transformative function. As our finding on the failed organization in Palakkad shows, caregivers may exit the service if the civic worth is crowded out. Thus, we contribute to TSR by explicating microlevel conflict reconciliation. In so doing, we add to the research suggesting that a harmonious view of transformative service does not resonate with empirical realities (Cabiddu, Moreno, and Sebastiano 2019; Echeverri and Skålén 2011; Skålén et al. 2015).
The above reconciliation of conflicts helps TSR move beyond the binary of legitimacy and illegitimacy central to institutional lenses of service systems. Such a binary fails to explain how a transformative service inheres a diverse set of service situations in which people from disparate backgrounds and motivations participate. We show that individuals may locate legitimacy in the framing of worth in a specific world. When different worlds come together, there can be situations of compromise between and cohabitation of diverse notions of worth beyond the binary of legitimacy and illegitimacy. Thus, we delineate a distributed spectrum of legitimacy with diffused boundaries.
Moreover, although some research attends to the role of morality in determining how different institutional logics prevail (cf. Baron et al. 2018; Blocker and Barrios 2015; Breidbach, Antons, and Salge 2016; Frow et al. 2016), these developments remain marginal to service research. Underexamining the moral dimensions of logics obscures a powerful motivator for why actors endorse or denounce one particular logic over another (Cloutier and Langley 2013). Our transformative service system framework foregrounds how caregivers’ morality furthers the civic world’s conventions over the industrial, market, domestic, inspired, or fame worlds. These moral notions trigger disputes between different worlds. Accordingly, individuals reconcile disputes within a specific moral order or devise a new moral framework of action around a compromise. Our study suggests that convention theory offers a vocabulary of morals that deepens our understanding of TSR.
Finally, our framework shows that agape is a highly desirable unintended consequence of transformative service. We found that caregivers suspended calculations based on reciprocal relations central to the exchange paradigm, and impelled by love, they operate in a regime of agape where they set aside the desire for equivalence. Agape’s fundamental tenets are antithetical to those of S-D logic. S-D logic stresses cocreation based on reciprocity (Vargo and Lusch 2016), which is a notion that has informed TSR. For instance, McColl-Kennedy et al. (2012) and Sweeney, Danaher, and McColl-Kennedy (2015) demonstrate how patients, as customers in a market, cocreate value by integrating resources for improved well-being. However, S-D logic and its “service ecosystem metaphor” comprise evaluation and exchange, which entail calculations. Our study shows that perspectives that privilege calculations neglect agapic action, through which caregivers silence their desires and offer unbounded care with no expectation of return or strategic benefit. Agape is based on selfless sacrifice (Belk and Coon 1993), and our findings support its role in this context, with one particular example showing that a young volunteer in her 20s donated a kidney to her patient. Such selfless behavior is also evident in how Geeta ignored her financial debt to volunteer full time for palliative care. Indeed, the lens of agape offers an alternative view of a health care context wherein caregivers improve patients’ well-being through situations of love and the suspension of calculations. Therefore, our framework, with its attention to the regime of agape, offers an important alternative to the dominant S-D logic lens and stands to expand conceptualizations of well-being in TSR.
Our study offers several implications for policy development and practice. The spread of COVID-19 during the writing of this article and the dramatic rise in serious health-related suffering, particularly in low- and middle-income countries, have cast in high relief the need for community health care models (Daniel et al. 2020). There is thus an urgent need to explore service delivery models beyond the prevailing hospital and hospice-based approaches that are limited in coverage and affordability. Kerala’s community model is one exemplary model that offers an alternative (Stjernsward 2005) in remodeling health services to empower communities. However, “community health intervention” is a popular buzzword in public health discourse and can be uncritically deployed, and such efforts obfuscate the plurality and tensions that underpin collaborations between medical professionals and community participants (Kumar 2020; Vijay, Whitelaw, and Clark 2020; Monin, and Kulkarni 2020). Further, these interventions can intentionally or unintentionally privilege the industrial world by evaluating service provisions based on professional standards and benchmarks, thereby crowding out the civic world or regime of agape. Our model shows the centrality of the civic world and agape in such an intervention that prioritizes civic/political rights, solidarity, and love, with several other worlds playing a supportive role. Moreover, designing compromises between different worlds can be central to the working of such transformative service systems. Finally, public health offerings cannot strategically design agape into interventions because this would introduce calculations. As Boltanski (2012) reminds us, agapic love cannot be forced, edified, or brought about intentionally. However, service systems that encourage caregiver interactions that shun or renounce calculated exchanges and reciprocity may gradually create spaces where caregivers can transition, even momentarily, to a regime of agape.
In conclusion, this article contributes by developing a framework highlighting how different regimes and conventions accomplish transformative service, how their relationships unfold, and how conflicts between them arise and are resolved. This article also contributes to TSR research by explaining the role of agape in transformative service. Our study surfaces several questions for future research. How do service providers in the regime of agape overcome the dominance of markets to restrict the influence of the exchange paradigm? How can agape further our understanding of “helping without harming”? How do noncommunity transformative service include different conventions and resolve conflicts? Studies may also attend to how conflicts arise from power struggles, a theme highlighted in the social sciences but not within service research. In settings of poverty and deprivation, the inclusion of actors from diverse backgrounds is critical for transformative services. However, such transformative service systems may have to transcend the narrow confines of markets and seamless resource integration to embrace a dialectic of justice and agape.
Footnotes
Acknowledgment
We are grateful to the special issue editors and the review team for their helpful feedback. We are indebted to the Kerala palliative care community for their generosity and support of this research. We would like to thank Aparna G., Wafa, Vishnu, and Prakash for their research and field assistance during various stages of this project. We are also grateful to David Clark and the End of Life Studies group at the University of Glasgow for collaborative work at various stages.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support for research from University of Birmingham. The second author received partial funding for the last phase (2019) of this research project from Scottish Funding Council under the Global Challenges Research Fund.