
Abstract
Gallic acid, a catechin polyphenol in tea, completely inhibited angiogenesis in assays of human tissue at 10−3 M. Psoriasis is a skin disease caused by excessive secretion of angiogenenic factors by keratinocytes and stromal skin cells. In a double-blind pilot study, six subjects with bilateral plaque psoriasis were treated with 10−2 M gallic acid in a cream base or with a cream base placebo over 8 weeks, four times a day, and treatments were randomly assigned to either the left or the right side. The gallic acid cream was well tolerated, but it did not reduce the psoriasis more than the placebo. One subject wanted to extend treatment for an additional 8 weeks. At the end of 16 weeks, the subject had complete resolution of the psoriatic plaque treated with gallic acid cream. In contrast, the plaque treated with placebo cream was not reduced and stayed equivalent to week six. Gallic acid is inexpensive and does not cause side effects. A longer trial evaluating 10−2 M gallic acid cream for the treatment of psoriasis seems indicated.
BACKGROUND
An herbal weight loss supplement containing rhubarb, ginger, astragalus, red sage, and turmeric was developed by a Chinese scientist, Wei Kaiyuan, PhD, who was trained in Western scientific principles and Traditional Chinese Medicine (TCM). To optimize the effect on weight loss, multiple herbs were combined and dissolved in an aqueous decoction according to the principles of TCM. Different combinations of the supplement components were tested in rodents after removal of one ingredient at a time to identify compounds that were not contributing to efficacy for weight loss. The best combination stimulated a 30–40% reduction of body weight in a pilot study using obese rodents in China.
Since it was the tenth combination tested that had the strongest effect on weight loss, the best combination was called Number Ten (NT). While in the United States giving an invited presentation at the Pennington Biomedical Center for obesity research, Dr. Kaiyuan patented his work on the weight loss treatment. An 8-week human pilot study was conducted at the Pennington Center in 24 healthy women who were 18–60 years of age with a body mass index (BMI) of 25–35 kg/m2. They were randomized to the following four groups: 1. Oral freeze-dried NT at 6 g/day, 2. Oral bed dried NT at 6 g/day, 3. Oral freeze-dried NT at 12 g/day and 4. Placebo. The dose was escalated over 3 weeks and maintained for 8 weeks. There was a dose-related problem with diarrhea, and this was determined to be caused by sennosides contained in the herbs. Sennosides are the active ingredient in some laxatives sold without requiring a prescription. 1
NT was not a practical obesity treatment in humans due to the laxative effect that was not previously observed in rodent studies. Our lab continued to investigate the individual active components in NT other than sennosides in collaboration with the Zhijun Liu laboratory at Louisiana State University Agricultural Center, which has expertise in fractionation of herbal decoctions. Angiogenesis is the formation of new blood vessels, and when inhibited, it has been shown to be a potential treatment for obesity in rodent studies. 2 We collaborated with the Eugene Woltering lab at the Louisiana State University Health Sciences Center laboratory in New Orleans that developed an assay for angiogenesis using human placental vein tissue. 3 Based on fractionation and testing in the placental vein assay, we determined that sennosides and gallic acid were both active in the assay to inhibit angiogenesis. Gallic acid is a polyphenol in tea and common foods such as berries, and it is considered safe by the European Food Safety Authority to feed animals used to provide meat for human consumption. Using black raspberry as a source of gallic acid, partial inhibition of angiogenesis was demonstrated at 10−4 M and complete inhibition of angiogenesis was seen at 10−3 M.4,5
Toxicology studies of gallic acid in pregnant rats were conducted and showed no adverse effects or reproductive pathology below the dose of 860 mg/kg/day. 6 Next, orally administered gallic acid was evaluated for treatment of obesity. A randomized, placebo-controlled clinical trial was conducted to measure weight loss after treatment with the combination of NT and gallic acid. No weight loss or reduction in food intake was observed after 8 weeks in subjects with a body mass index of 25–35 kg/m2. Unfortunately, the human pharmacokinetic studies of gallic acid demonstrated that blood levels did not exceed 10 micromolar despite escalating the dose. 7 This suggested that a saturable transport system exists in the gut for the absorption of gallic acid. Since blood levels of 10–100 times higher than 10 micromolar are required to suppress angiogenesis,4,5 it was clear that gallic acid would not be an effective oral therapy for obesity.
We continued to study inhibition of angiogenesis by gallic acid as a therapeutic for other diseases. Because angiogenesis is only active in normal adults during fetal development and menses, inhibition of angiogenesis should have minimal side effects in nonpregnant adults. Angiogenesis occurs during wound healing, but wounds are technically pathological and temporary. Inhibition of angiogenesis can be discontinued, if necessary, during the wound-healing process. Angiogenesis is involved in many disease states, including the three leading causes of blindness: diabetic retinopathy, wet macular degeneration, and neonatal oxygen toxicity. In addition, angiogenesis is a driver of psoriasis, an inflammatory disease of the skin. 8
Psoriatic skin lesions form after elevated keratinocyte proliferation and infiltration of immune cells. The lesions have increased vascular density, tortuosity, and permeability. 8 Pro-angiogenic factors in the skin such as vascular endothelial growth factor (VEGF), angiopoietins, tumor necrosis factor alpha, interleukin-8, and interleukin-17 all become unregulated and induce angiogenesis. 9 These factors are secreted by keratinocytes and stromal cells, which contribute to angiogenesis and remodeling. 10 Thus, angiogenesis is the central pathogenic mechanism in psoriasis. Since different tissues can have unique responses to angiogenesis inhibitors and stimulators, we developed an assay using human fat rather than placental vein as a general model for adult tissue angiogenesis. 11 To evaluate the efficacy of gallic acid as an angiogenesis inhibitor, we conducted a gallic acid dose–response curve of angiogenesis inhibition in human adipose tissue and in human placental vein tissue. We observed similar effects for inhibition of angiogenesis by gallic acid in both assays. Considering that psoriasis lesions are on the external surface of the skin, topical concentrations of gallic acid can be used that are sufficient to inhibit angiogenesis. Accordingly, we performed a pilot trial to see if gallic acid cream could be a potential treatment for psoriasis.
METHODS
In vitro angiogenesis assay
The placental vein assay and the fat assay have been described, and they are the only assays of angiogenesis that can measure both the angiogenic switch and the proliferation phase in human tissue.3,11 Briefly, placental vein tissue was obtained from placentas that would otherwise be discarded, and subcutaneous abdominal fat tissue was removed during surgical procedures for other purposes. The placental tissue or fat was placed in 96-well plates containing human thrombin (0.05 IU in 4 mcL/well). The tissue fragments were covered with 100 µL clotting media consisting of fibrinogen 3 mg/mL (Sigma Chemical Co., St. Louis, MO) and epsilon amino caproic acid 0.5% (Sigma Chemical Co., St. Louis, MO) dissolved in human placental vein angiogenesis media (HPVAM, Medium 199 (GibcoBRL, Gaithersburg, MD) with antibiotic/mycotic solution containing 100 U penicillin, 100 U streptomycin sulfate, and 0.25 amphotericin beta per mL (GibcoBRL, Gaithersburg, MD). The mixture was allowed to clot overnight in a humidified incubator with 5% CO2 and 95% room air at 37°C. After gelling, the clot was supplemented every 2–3 days with 100 µL angiogenesis medium containing 20% bovine serum in media 199 (GibcoBRL, Gaithersburg, MD), bringing the contents in each well to 200 µL. Antiangiogenesis test compounds were added in antiangiogenesis medium every 2–3 days.
Grading of angiogenesis assay
After fat was seeded into wells, initiation of angiogenesis was allowed for 4 days before the addition of test compounds. The assay was graded by visual inspection every two to 3 days when the medium was replaced using a 20× lens on an inverted microscope, and this extended over a 2-week period. Each well was visually divided into four quadrants, and the angiogenesis was graded from 0 to 3 in each quadrant on length from three sprouts to vessels growing to the periphery with the total score for each well between 0 and 12 (see Fig. 1). The assay has been validated by Hornick et al. 12
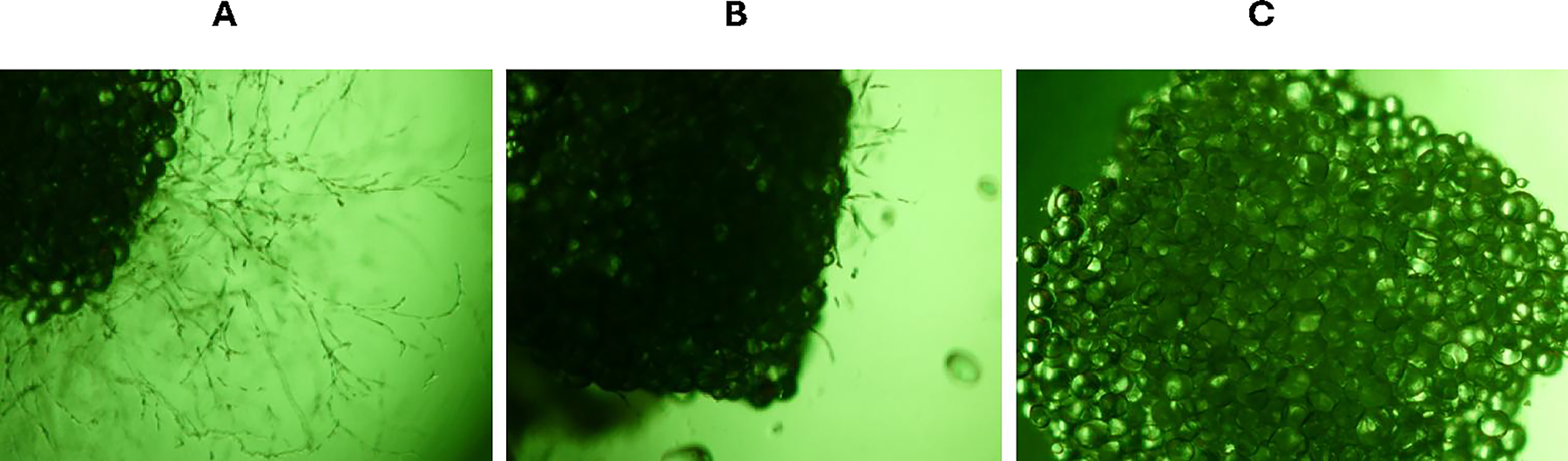
Photographs of immobilized human adipose tissue pieces undergoing angiogenesis in fibrin-thrombin clots at baseline after plating, at the initiation of angiogenesis, and with a full growth of blood vessels in the control. Photographs were taken using an inverted microscope at a 20X magnification.
Clinical trial
This clinical trial was approved by the Pennington Biomedical Research Center Institutional Review Board (IRB), Baton Rouge, Louisiana. The IRB reviewed the protocol April 21, 2004, which was prior to the 2005 requirement that clinical trials be registered on a clinical trials registry. Thus, the trial had IRB approval, but no clinical trial registration number. We did not publish the trial earlier since we wanted to test other food components that inhibited angiogenesis by mechanisms different from VEGF inhibition, the primary mechanism by which gallic acid inhibits angiogenesis. We have not observed synergy between antiangiogenic compounds with different mechanisms, so we are publishing the pilot trial, since it could have treatment implications. Six subjects at least 18 years of age or older with bilateral plaque psoriasis were enrolled in the clinical pilot trial. Pregnant or lactating females were excluded from the trial.
On the screening visit, subjects gave their informed consent, completed a medical history form, which was reviewed with the subject and a physical examination was performed. The subjects came to the screening visit having fasted except for water from 9 pm the prior night, and blood was drawn for a chemistry panel measuring glucose, creatinine, potassium, uric acid, albumin, calcium, magnesium, creatine phosphokinase, alanine transaminase (ALT), alkaline phosphatase, iron, total cholesterol, triglycerides, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol (LDL; Chemistry 15 panel) and a complete blood count measuring hemoglobin, hematocrit, mean cell volume, platelet count, and white blood cell counts of the granulocytes, neutrophils, eosinophils, and basophils (CBC). The subjects were given equipment for skin patch testing. They were asked to place a 1-inch gauze pad with gallic acid cream on a hairless area of their skin like the inner arm 2–3 days prior to their baseline visit. The patch was covered with an occlusive dressing for 48 h unless the patient developed pain, itching, or irritation in which case the patch was to be removed. If the subject had a negative test characterized by no itching, pain, or irritation, they were randomized into the study.
Subjects randomized into the study were given two tubes of cream; one tube had just the cream base, and the other had the cream base with 10−2 M gallic acid. Subjects were asked to apply the assigned creams to the assigned psoriatic plaques (right or left) four times a day for 8 weeks. The creams were assigned to the right or left plaque randomly such that the investigator and the subjects were blinded to the side to which the gallic cream versus the placebo cream was assigned. The subjects were seen at baseline and every 2 weeks to have the Psoriasis Area and Severity Index (PASI) scored, have a photograph taken of the bilateral plaques chosen for treatment, and be asked about any adverse events. The PASI was graded for both treated plaques at baseline and at every biweekly clinic visit. The PASI is a validated qualitative grading system based on the erythema, scaling, and thickness of the plaque assessed on a scale from 0 to 3 for a maximum total score of 9 for each plaque.13,14 A physical examination, CBC, and chemistry panel were performed again at the end of the study on week 8.
Statistics
PASI was analyzed using a linear mixed-effects model in SAS (PROC MIXED). Fixed effects included Treatment (gallic acid vs. placebo), Time, and the Treatment-by-Time interaction. Treatment was modeled as a within-participant, and a patient-specific random intercept was specified to account for within-participant correlation because of the paired design. Repeated measurements over time within each participant-by-treatment plaque were modeled using a compound-symmetry residual covariance structure. Model-based least-squares means were estimated for each Treatment × Time combination.
In like manner, angiogenesis was analyzed using mixed-effects models in SAS with fixed effects for concentration (Group), day, and Group × day. Correlation among repeated measurements within an experimental unit over days was modeled using a compound-symmetry residual covariance structure. LS-means were estimated for each Group × day combination. Within each day, pairwise comparisons among concentrations were conducted using sliced differences with Tukey adjustment. All tests were two-sided at α = 0.05.
RESULTS
The inhibition of angiogenesis by gallic acid was tested in placental vein tissue and in adult human adipose tissue pieces at concentrations ranging from 10−3 to 10−6 M versus placebo. Grading of vessel growth was performed by visual inspection, and Figure 1 shows a representative appearance of what the view of the fat tissue looks like at 20× magnification. In fat tissue, 10−3 M gallic acid completely inhibited angiogenesis, and 10−4 M caused partial inhibition (Figs. 2 and 3). In both assays, the 10−6 M and 10−5 M concentrations were not different than the control, indicating no statistically significant angiogenesis inhibition. The 10−4 M concentration gave a significant partial inhibition, and the 10−3 M gave complete inhibition of angiogenesis compared to the control in both tissues (P < .0001 for both).
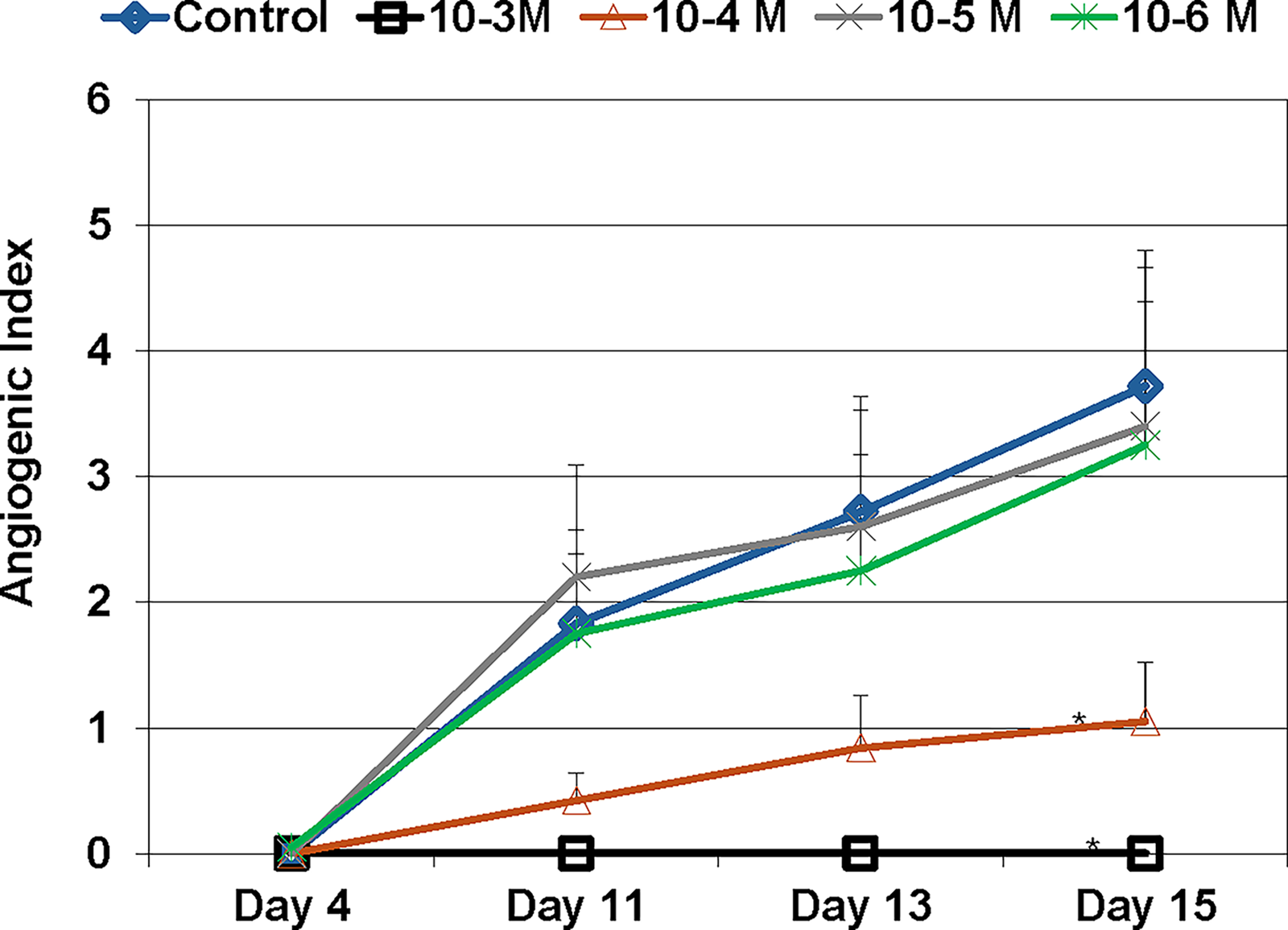
Gallic acid treatment of placental vein pieces immobilized in fibrin-thrombin clots. Tissues were plated and allowed to grow for 4 days before starting treatment with gallic acid every 2 to 3 days. Measurements on days 4, 11, 13, and 15 have been graphed. Each line on the graph represents a separate assay with 20 pieces of placental vein tissue. The 10−4 M concentration of gallic acid gave a significant partial reduction in angiogenesis compared to the control, and the 10−3 M concentration gave complete suppression of angiogenesis (*P < .0001 for both). Values were determined by visual inspection. Each well was visually divided into four quadrants, and the angiogenesis was graded on a 0–3 scale based on the length of the vessels from three sprouts to vessels growing to the periphery of the well. The total score for each well was between 0 and 12 (see Fig. 1). This visual assay has been validated by Hornick et al. 12
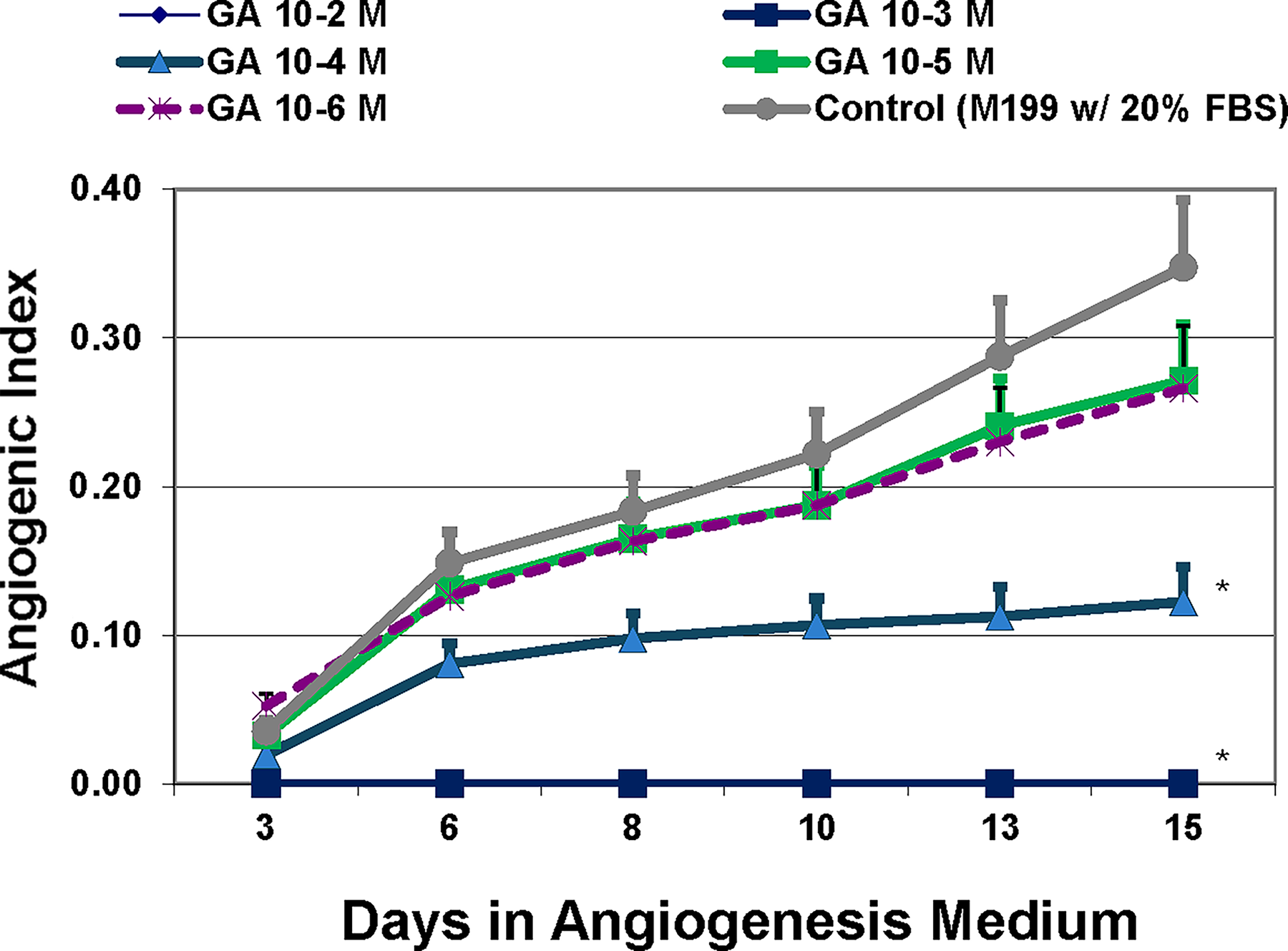
Gallic acid treatment of fat tissue pieces immobilized in fibrin-thrombin clots. Tissues were plated and allowed to grow for 4 days before treatment with gallic acid every 2–3 days. Each line on the graph represents a separate assay with 20 pieces each. The 10−4 M concentration of gallic acid gave a significant partial reduction in angiogenesis compared to the control, and the 10−3 M concentration gave complete suppression of angiogenesis (*P < .0001 for both). Values were determined by visual inspection and were graphed using data from days 3, 6, 8, 10, 13, and 15. Each well was visually divided into four quadrants, and the angiogenesis was graded on a 0–3 scale in each quadrant using the length of the vessels from three sprouts to vessels growing to the periphery of the well (see Fig. 1). The total score for each well was between 0 and 12.
Six subjects participated in the trial. All were of the White race, and there were five females and one male. The demographics of the study subjects are presented in Table 1. The chemistry panel that was done to screen for clinically significant disease had analytes outside of the normal range in a few instances, but these abnormalities were not believed to be clinically significant. The glucose was between 100 mg/dL and 125 mg/mL in four participants, but there were no subjects with diabetes. Potassium was below 5.5 meq/L but was between 5 and 5.3 meq/L in three subjects; this was felt to be due to red cell trauma during phlebotomy. Three subjects had a total cholesterol below 163 mg/dL, and four had LDL cholesterol less than 100 mg/dL. One subject had a uric acid of 7.4 mg/dL, one person had an ALT of 8 IU/L, and one person had an iron of 29 mcg/dL but was not anemic. These analytes were repeated at the end of the study and showed no clinically significant changes. The CBC had some minor variations outside the normal range, but they were not felt to be clinically significant. The hemoglobin was 0.2 G/DL above normal in one subject at screening and 0.2 G/DL below normal at the end of the study in two other subjects, with the hematocrits being consistent with the hemoglobins. Platelets were normal at screening and rose to 546 × 10−3 at the end of the study in one subject. The white blood cell counts were elevated to less than 11,000 at screening in two subjects and returned to normal at the end of the study. The skin test did not give irritation in any of the subjects. The mean PASI scores from the six subjects at 8 weeks for the plaque treated with gallic acid cream versus the side treated with the placebo cream were compared every 2 weeks (Fig. 4). Both creams caused a significant reduction in the PASI scores over the 8 weeks (P < .0001). Although the plaque treated with the cream base (pink) did not have as much improvement as the plaque treated with gallic acid 10−2 M cream, the 58% reduction in the PASI by the placebo cream was not significantly different from the plaque treated with the gallic acid cream (P = .9707).
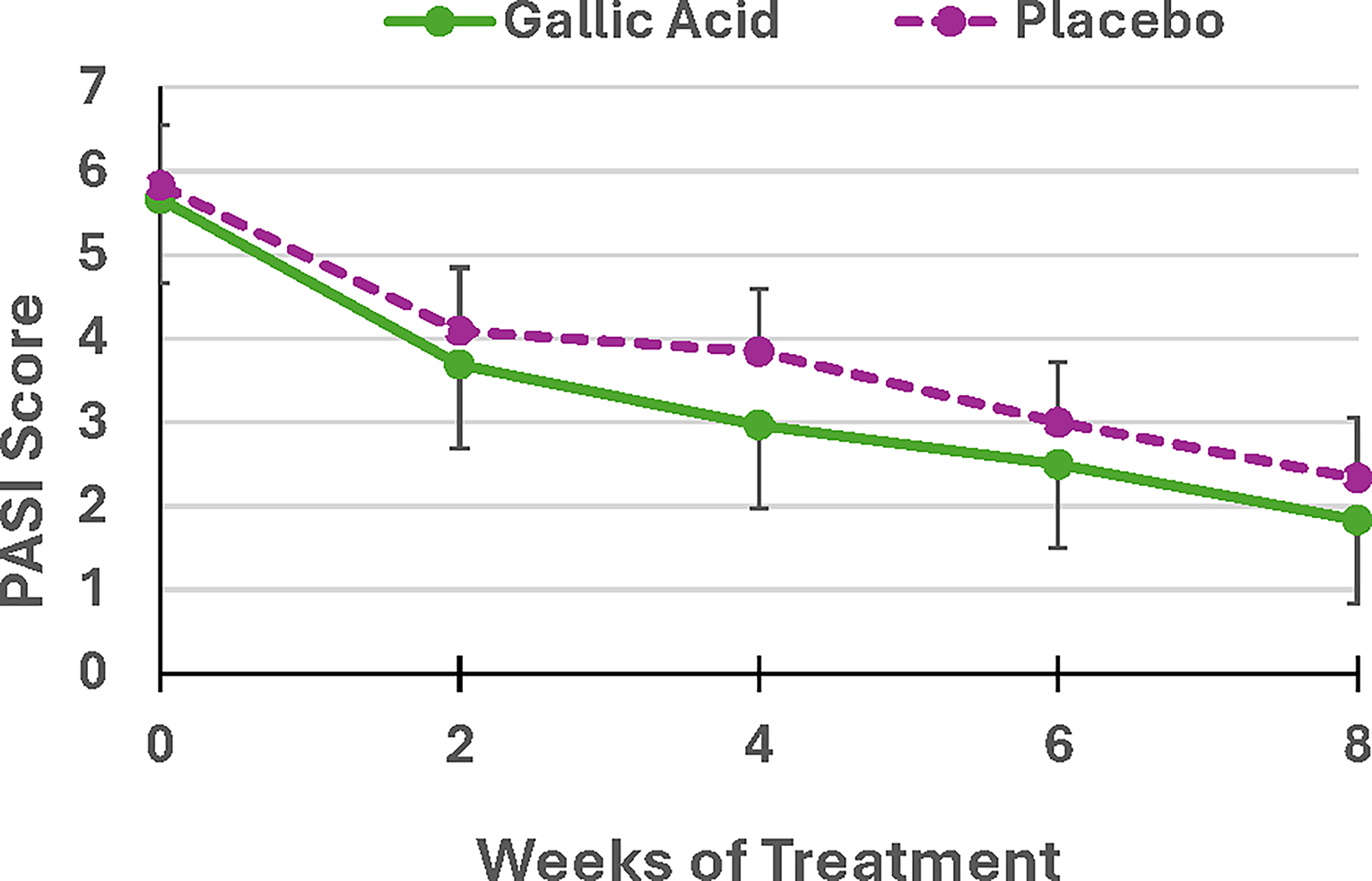
Mean PASI scores from the six subjects at 8 weeks for the plaque treated with gallic acid cream versus the side treated with the placebo cream. Both creams had a significant reduction in the PASI scores over the 8 weeks (P < .0001). Although the plaque treated with the cream base (pink) does not have as much improvement as the plaque treated with gallic acid 10−2 M cream, the difference is not significant (P = .9707).
Baseline Demographics

Height (Ht) in centimeters; body mass index (BMI) in kg/m2; systolic blood pressure (S BP), diastolic blood pressure (D BP) in millimeters of mercury (mmHg); heart rate in beats per minute (B/min); age in years (Yrs).
One subject had remaining cream of both types and wanted to continue to treat both psoriatic plaques for an additional 8 weeks. Her PASI values in the psoriatic plaque treated with the placebo cream base showed no further improvement after week 6, but her psoriatic plaque treated with 10−2 M gallic acid cream showed complete resolution at the end of the total 16-week period (Figs. 5 and 6). None of the subjects had any adverse events, and there were no significant changes in the chemistry panel, CBC, or on the physical exam.
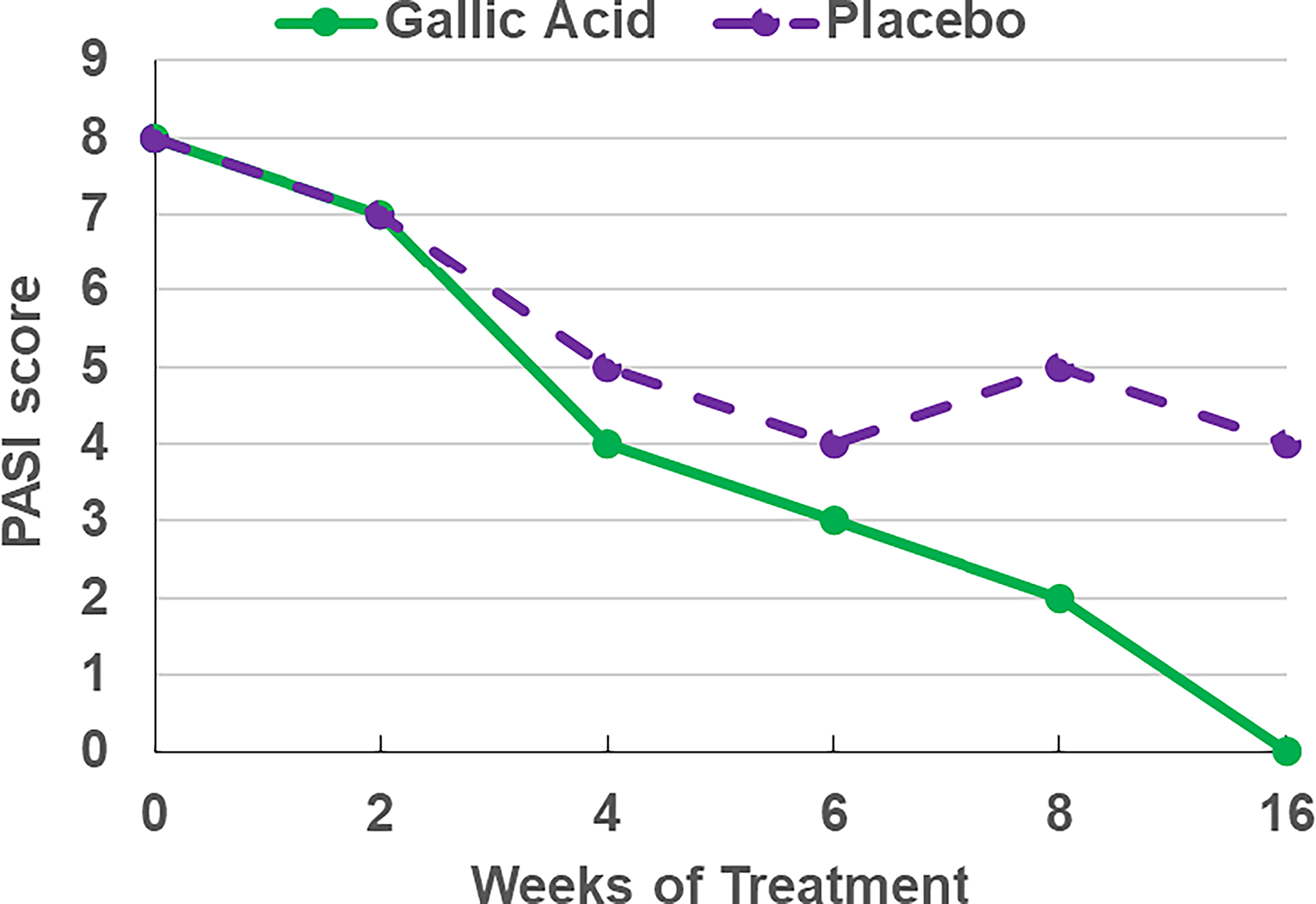
PASI scores over the 16-week period in the single subject that extended her treatment progressed to complete resolution of the plaque treated with gallic acid 10−2 M cream (green) compared to the placebo that had no change after 6-weeks.
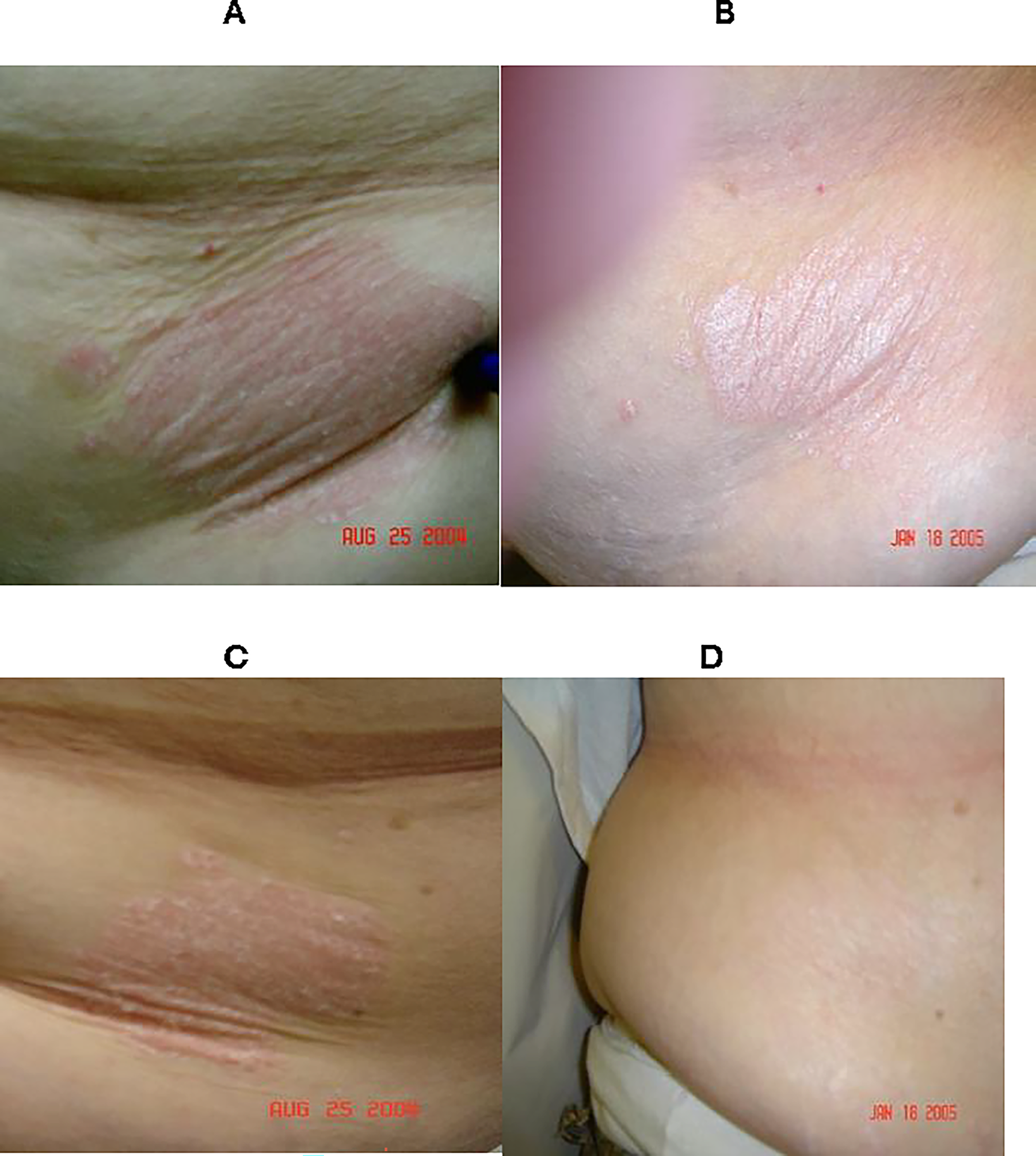
Pictures of the single subject that extended her treatment for an additional 8 weeks:
DISCUSSION
The result of the angiogenesis assays clearly showed that gallic acid is able to completely inhibit angiogenesis in the placental vein and fat tissue assays at 10−3 M concentration. The 8-week trial, as it was designed, did not show a difference between gallic acid and placebo. However, the resolution of the plaque treated with the 10−2 M gallic acid cream for 16 weeks in one patient who continued the treatment raises the possibility that angiogenesis inhibition to reverse psoriasis plaques is a slow process and requires a treatment time of greater than 8 weeks. There was a significant reduction in the PASI in the 8-week study in both groups compared to baseline. One could argue that both gallic acid and the placebo were equally active in reducing the psoriasis. This, however, is unlikely to be the explanation for more than one reason. The gallic acid cream had a 10-fold higher concentration of gallic acid than the concentration of gallic acid which completely suppressed angiogenesis in the fat cell assay. In addition, the cream was placed in direct contact with the lesion, increasing the likelihood of a direct effect on inhibiting the angiogenesis driving the psoriasis. Even more convincing is the data from large dermatology trials showing that similar reductions in the PASI were seen the placebo groups. For example, Lebohl et al. evaluated roflumilast, a topical phosphodiesterase four inhibitor in two randomized and placebo-controlled phase 3 trials lasting 8 weeks and involving 880 subjects at 40 clinical centers. Twenty-five percent of the subjects in the placebo group reduced their PASI score by at least 50%, but less than 7% and 3% of the placebo group reduced their PASI score by 75% and 90%, respectively. Less than one percent (0.8%) of the placebo group in this large trial had complete resolution of their psoriasis measured by the PASI score as was the experience of our patient who used gallic acid cream for 16 weeks. Thus, there is expectation of a placebo response equal to 50% measured by the PASI in over 25% of clinical trial participants, but seeing a complete resolution from placebo would be quite rare. 15
The cream was safe and well-tolerated with no reported adverse events. In addition to the cream being safe, it is not like oil-based ointments or tar-based treatments to which people with psoriasis object. The cream rubbed on the plaque was absorbed by the skin and was not objectionable to the subjects. Although this trial did not give a positive result during the 8-week trial, in view of its safety, tolerability and the one subject who had a complete resolution after 16 weeks, further evaluation of gallic acid cream is indicated. Angiogenesis inhibition may act over a period of time longer than 8 weeks and require a controlled trial lasting four to 6 months. If a longer trial gives results similar to the one patient who had resolution of her psoriasis lesion in 16 weeks, gallic acid might represent a safe, well-tolerated treatment for plaque psoriasis. Being able to use a cream rather than an ointment or tar would have cosmetic advantages and reduce the risk of getting oil stains on nice clothing. Gallic acid is also inexpensive, so if gallic acid turns out to be an effective treatment for psoriasis, it would also be cost-effective.
AUTHORS’ CONTRIBUTIONS
R.R.G., A.A.C., and F.L.G. designed and conducted research and wrote, reviewed, and edited the article, D.Z. led the statistical analysis and contributed to the interpretation of the results. R.R.G. and F.L.G. had primary responsibility for the final content. All authors read and approved the final article.
ETHICAL CONSIDERATIONS
This clinical trial received ethical approval from the Pennington Biomedical Research Center Institutional Review Board (IRB), Baton Rouge, Louisiana. The protocol was reviewed and approved on April 21, 2004, which preceded the 2005 requirement for mandatory registration of clinical trials in public registries. As a result, the study had full IRB approval but no clinical trial registration number.
CONSENT FOR PUBLICATION
All authors declare they have obtained written informed consent to publish.
Footnotes
AUTHOR DISCLOSURE STATEMENT
The authors declare no competing financial interests.
FUNDING INFORMATION
This trial was funded from the Greenway development account in the Pennington Biomedical Research Foundation that was generated from charitable tax-deductible contributions.