
Abstract
Background:
Language barriers lead to disparities at the end of life (EOL). How providers work with medical interpreters and meet the needs of patients and families with limited English proficiency (LEP) enrolled in hospice remains poorly understood.
Objectives:
To investigate home hospice providers’ experiences when communicating with patients and families with LEP, report the frequency of use of medical interpretation, and ascertain the strategies utilized by respondents to communicate with patients and families with LEP.
Design:
Cross-sectional survey of U.S. based home hospice providers delivering home hospice care.
Results:
A total of 138 surveys were collected. The response rate could not be calculated due to the survey dissemination method. On average 22% of the respondents reported caring for patients/families with LEP. Over-the-phone interpreting (OPI) was the most frequent professional interpreter modality utilized to communicate with patients/families with LEP (81%). Adult family members and hospice staff, who spoke the same language as the patient, were also commonly utilized by respondents (83% and 66%, respectively). Provision of video remote interpreting written hospice and bereavement materials in various non-English languages was viewed as a beneficial interventions for this patient population.
Conclusion:
OPI was most frequently utilized by home hospice providers. Having bilingual hospice staff and non-English language bereavement materials was viewed as an important strategy to support patients and families with LEP.
Key Message
This nationwide U.S. study investigates the experiences of hospice care providers when communicating with patients and families with limited English proficiency. Over-the-phone interpretation was most frequently utilized. Respondents identified bilingual hospice staff and non-English bereavement materials as key strategies to improve communication and support equitable end-of-life care.
Introduction
As of 2021 in the United States, over 67 million individuals speak a language other than English at home, while over 26 million have limited ability to read, speak, write, or understand English, that is, have limited English proficiency (LEP). 1 Language barriers contribute to worse health outcomes for patients with LEP, including poorly controlled pain and decreased patient satisfaction.2–5 Research has shown that patients with LEP have higher rates of psychological distress, poor self-rated health, and greater difficulty comprehending medical information from providers.6–9 When compared to English-proficient patients, patients with LEP are at increased risk for hospital readmission due to difficulty understanding how to manage their symptoms.10,11 Because physical symptoms can change rapidly at end of life (EOL), delivering comprehensive hospice care is imperative even when cultural and linguistic differences are present.
Language barriers contribute significantly to disparities in EOL care.12,13 Language discordance between patients/families and health care providers constitutes an important barrier to hospice enrollment for patients with LEP. 14 Patients who report having a non-English language preference are entitled to a professional interpreter in the health care setting. 15 A study examining barriers to hospice care in diverse populations found that professional interpreters are often unavailable in the community for patients/families with LEP receiving hospice care. 14 The impact of language barriers on disparities in EOL care, including how providers work with medical interpreters and meet the needs of patients and families with LEP enrolled in hospice, remains poorly understood.
While prior research has established that LEP status increases risk for poor outcomes in persons receiving EOL care,12,16,17 limited research has been done to characterize the experiences and challenges that hospice providers face when caring for patients and families with LEP at the EOL. Further, little is known about the frequency of use of various modalities of medical interpretation when providing care to individuals with LEP receiving hospice care. Accordingly, we conducted a nationwide survey of home hospice providers to investigate the prevalence of use and specific types of interpreter services employed by respondents when delivering care to patients with LEP, and the ways in which respondents assessed the language needs of their care recipients.
Methods
Study design and development
We surveyed adult hospice care providers (physicians, nurses, nurse practitioners, social workers, faith leaders, or other hospice team members) who worked for any U.S. based hospice agency. The Weill Cornell Institutional Review Board approved this study.
We designed a 7-item survey de novo after conducting a literature review to clarify our constructs and search for any existing instruments.18–20 A multidisciplinary project team that included a palliative care physician, hospice physician, hospice nurse, and two EOL care leaders of the Hospice Foundation of America (HFA) helped develop the survey. We drafted survey items that were piloted by the project collaborators and other hospice and palliative care disciplines, including a registered nurse, social worker, and chaplain, all of whom provided feedback that allowed us to refine our survey items.
Survey items
We ascertained participants’ demographic status, including their age, gender, and role/discipline, whether they spoke other languages well enough to provide care to patients/families with LEP at the EOL, and their hospice agency’s demographic information. Participants were asked to estimate the frequency with which the hospice agency encounters patients and family caregivers with LEP. A multiple-choice question (with the option for multiple responses) inquired about strategies utilized by the hospice agency to meet and assess the language needs of their care recipients. To estimate the frequency with which providers use medical interpreters and other types of ad hoc interpreters (e.g., hospice staff and, family member), we employed a Likert response scale where the frequency of interpretation service use ranged from 0 (never) to 4 (always). Open-ended questions were employed in an effort to: (1) better understand how home hospice agencies provide bereavement services to family caregivers with LEP and (2) ascertain strategies utilized to communicate with patients/families with LEP.
Study population and data collection
Participants were recruited using three methods. First, respondents were recruited from the Hospice Medical Director (HMD) certification board website (hmbdcb.org), which contains publicly available email contact information for HMDs. Second, we recruited via the VITAS Healthcare hospice listserv of HMDs and third, we recruited via the HFA’s email listserv. HFA is a nonprofit organization dedicated to advancing the mission of hospice care in the United States with an email listserv of approximately 13,500 individuals.
We distributed the survey and collected anonymous responses using REDCap, a web-based research data management application. 21 Our initial survey invitation was sent on February 28, 2024, with 3 reminders sent after the initial email outreach. The survey closed on October 1, 2024.
Statistical analysis
Survey results were summarized with descriptive statistics using SPSS Version 29. One-way ANOVAs were used to examine differences in the frequency of using a specific type of interpreter by U.S. region (Northeast, Midwest, South, and West), role, other languages spoken by providers, gender, or hospice type.
Qualitative analysis
We analyzed qualitative data using a conventional content analytic approach.22,23 Data analysis was approached without a preexisting conceptual framework in order to allow for the coding process to generate new insights. A codebook was developed inductively and revised throughout the data analysis process. During open coding, one coauthor (M.D.S.) independently coded the qualitative data, identifying sections of text representing discrete concepts and applying code. A final set of codes was developed and organized into discrete categories. The coding process was cross validated with two team members (R.D.A. and M.C.R.) to ensure coding validity. Any discrepancies were discussed by the research team and resolved via consensus.
Results
Participant characteristics
A total of 199 respondents began the survey, and data from 138 completed surveys were included in the analysis. We were able to ascertain that 5370 emails were opened while 377 emails were not deliverable to prospective participants from one of the three listservs. Because we do not know how many emails were delivered and opened from the remaining two listservs we are unable to calculate an overall response rate.
Participants’ demographic data are shown in Table 1. Most participants (58%) were above 55 years of age. The most common professional backgrounds of respondents were physicians (45%) and social workers (21%). A little less than a quarter (23%) of participants reported speaking another language other than English well enough to provide hospice care. The most common non-English language spoken was Spanish (13%). Most respondents were employed by hospices in the South (41%) and delivered hospice care in an urban (39%) setting. About two-thirds of respondents worked for non-for-profit hospice organizations (66%).
Sample Characteristics (N = 138)
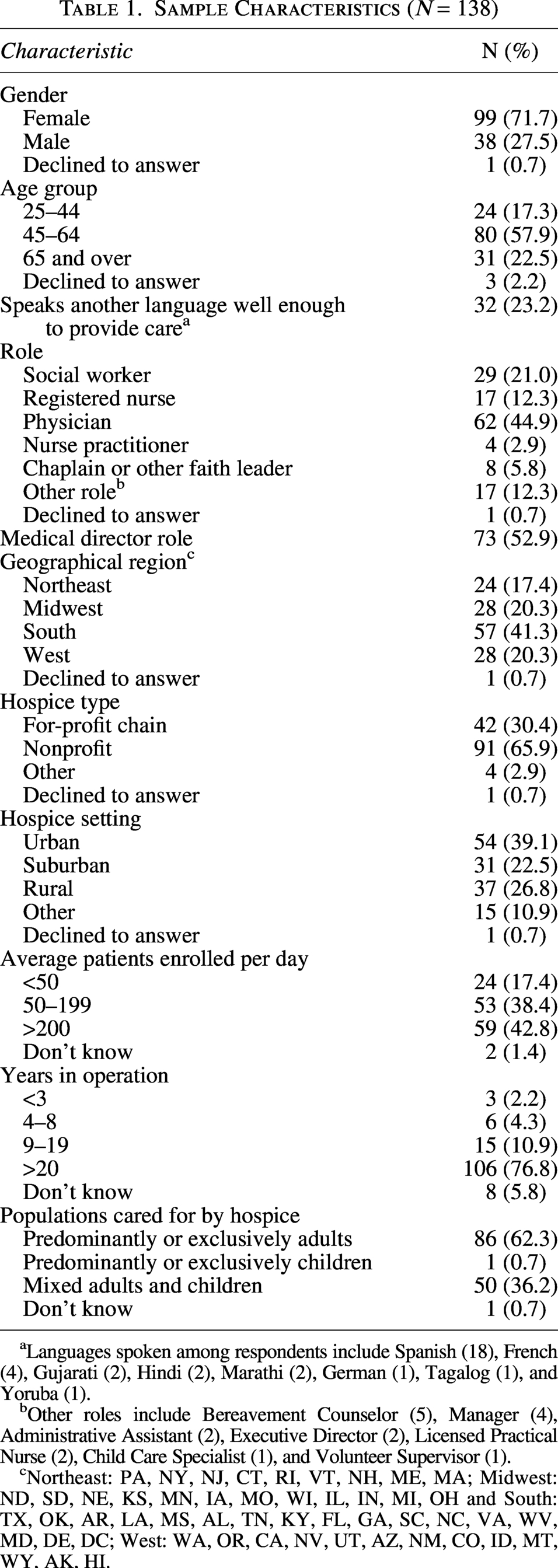
Languages spoken among respondents include Spanish (18), French (4), Gujarati (2), Hindi (2), Marathi (2), German (1), Tagalog (1), and Yoruba (1).
Other roles include Bereavement Counselor (5), Manager (4), Administrative Assistant (2), Executive Director (2), Licensed Practical Nurse (2), Child Care Specialist (1), and Volunteer Supervisor (1).
Northeast: PA, NY, NJ, CT, RI, VT, NH, ME, MA; Midwest: ND, SD, NE, KS, MN, IA, MO, WI, IL, IN, MI, OH and South: TX, OK, AR, LA, MS, AL, TN, KY, FL, GA, SC, NC, VA, WV, MD, DE, DC; West: WA, OR, CA, NV, UT, AZ, NM, CO, ID, MT, WY, AK, HI.
Measures addressing language access
Participants reported that in their perception approximately one in five (22%) of the hospice care recipients have LEP (see Table 2). The two most common non-English languages spoken by patients and family caregivers receiving home hospice care were Spanish and Chinese. Over two-thirds (77%) of participants reported that their hospice agency has a formal policy on providing language assistance for patients and family caregivers with LEP. The most common strategies utilized to meet the language needs of patients and family caregivers with LEP were (1) contracting with interpreter services, (2) documenting patient language preference in electronic medical records, and (3) screening for language ability at intake.
Strategies and Limited English Proficiency Characteristics (N = 138)
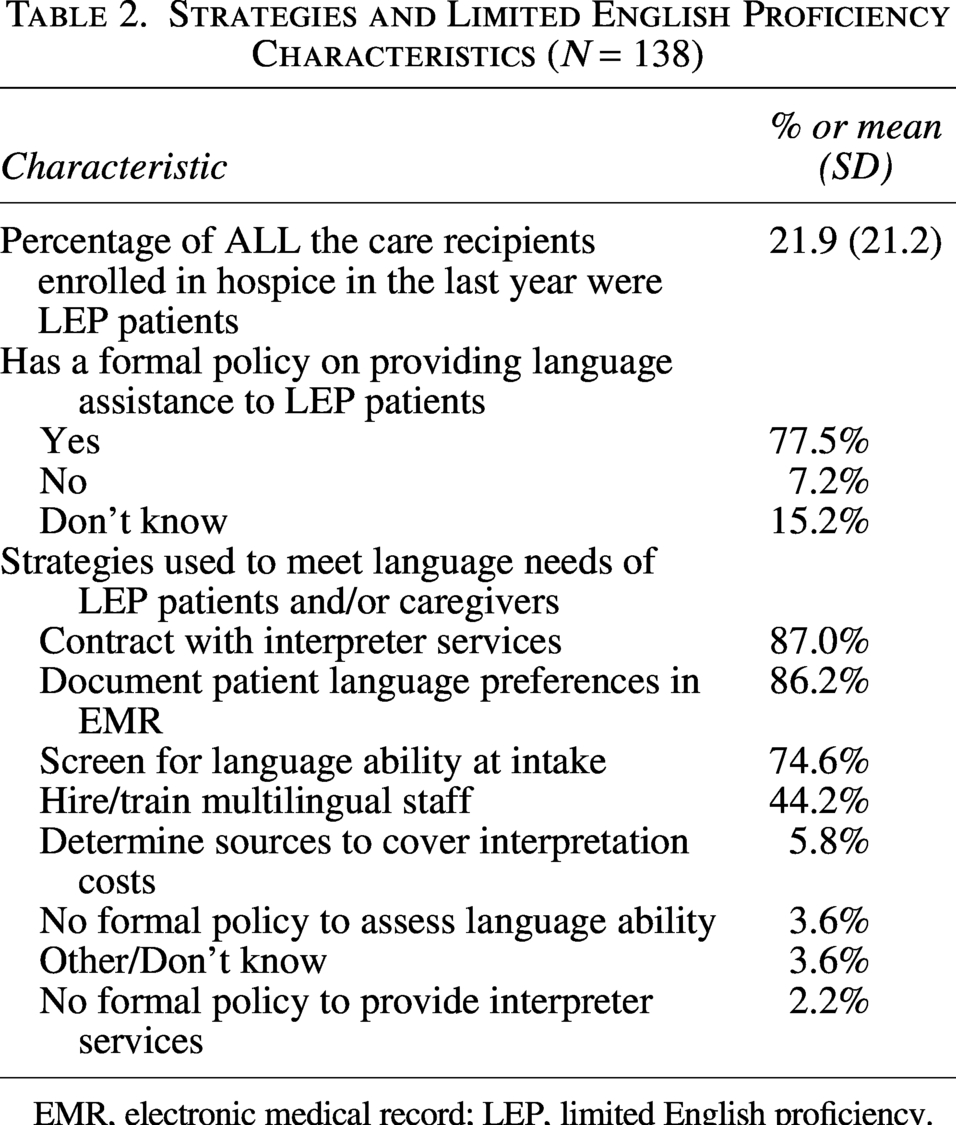
EMR, electronic medical record; LEP, limited English proficiency.
Frequency of Use of Interpreter Services: When asked about the frequency of use of various types of interpreter services available in the home hospice setting, over-the-phone interpreting (OPI) was the most common, with 81% of respondents relying on this resource “Sometimes” to “Always” (Table 3). Approximately 30% of participants reported using video remote interpreting (VRI) “Sometimes” to “Always” and approximately 44% of participants reported using in-person medical interpreters. Only 9% of participants reported “Sometimes” to “Usually” lacking access to any type of interpreter services during patient encounters. Of note, use of adult family members for interpretation was reportedly employed “Sometimes” to “Always” by 83% of participants. Comparably, 66% of participants reported utilizing language concordant hospice staff “Sometimes” to “Always.” Lastly, 78% of participants reported hospice materials printed in various non-English languages were “Sometimes” to “Always” available.
Frequency of Interpretation Service Use Among Respondents (N = 138)
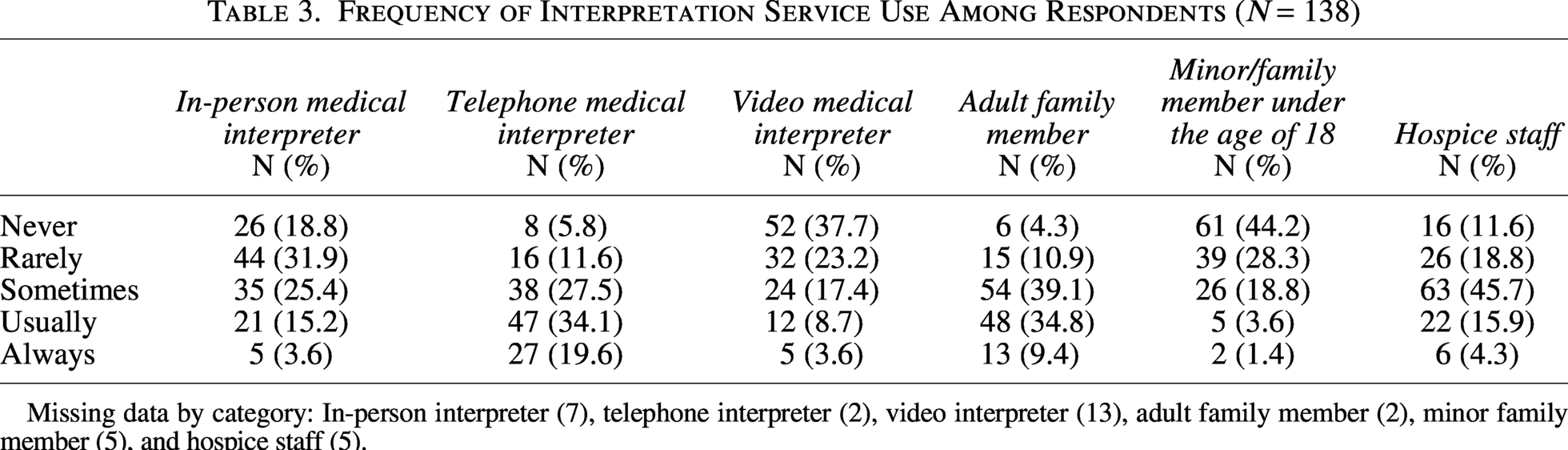
Missing data by category: In-person interpreter (7), telephone interpreter (2), video interpreter (13), adult family member (2), minor family member (5), and hospice staff (5).
Factors associated with utilization of various language services
No significant differences were found in the frequency of medical interpreter modalities (e.g., video, telephone, or in-person) by U.S. region (Table 4). Only use of language-concordant hospice staff and translated hospice materials was associated with significant differences by U.S. region. The Midwest reported the lowest use of hospice staff as ad hoc interpreters, while the West reported the highest use. The West reported the highest use of translated hospice materials, while the lowest was reported by participants located in the Northeast. When comparing responses based on respondents’ disciplines, social workers and physicians were associated with a greater use of telephonic medical interpreters, while nurses reported the lowest frequency [F(6129) = 2.99, p = 0.009]. There were no significant differences in the utilization frequency of various language services by gender, age, or hospice (e.g., profit vs. non-for-profit).
Frequency of Using Specific Language Services by U.S. Region (One-Way ANOVA)
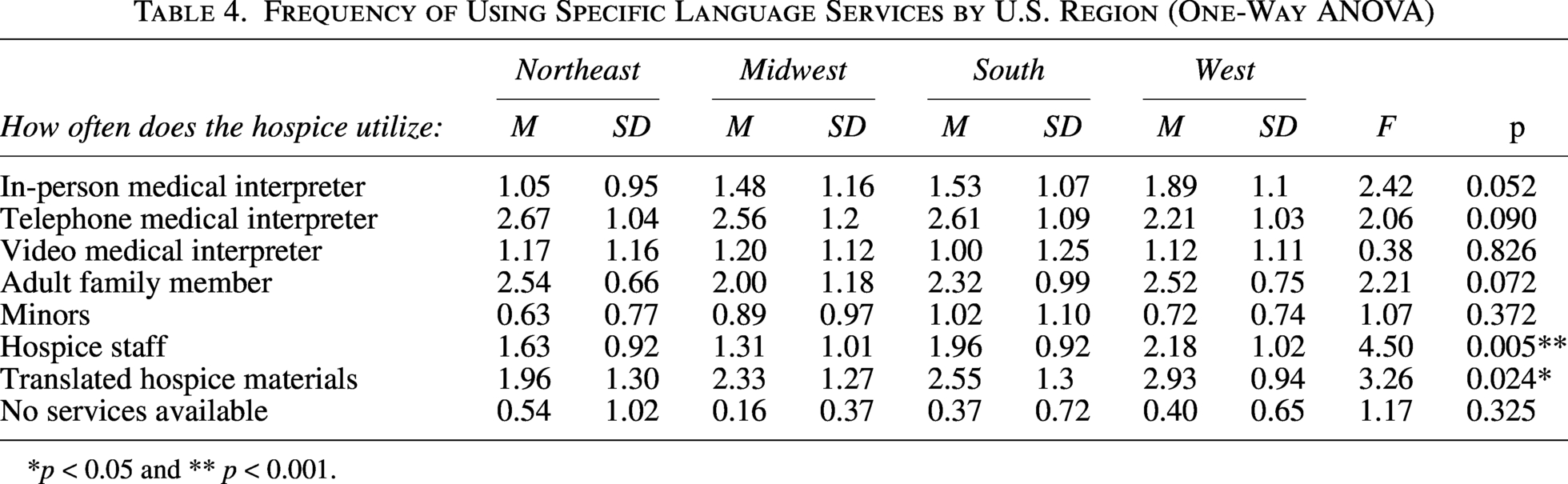
*p < 0.05 and ** p < 0.001.
Provision of bereavement services to family caregivers with LEP
Many participants shared that their agencies provide language-concordant bereavement services (primarily Spanish). Moreover, many hospice agencies reported the use of written materials related to grief and supportive counseling in languages other than English. Hospice agencies strove to refer families to local support groups in their preferred language if the family agreed to a referral. Several participants mentioned that families who do not speak English would often decline bereavement services. Additionally, many participants shared that medical interpreters (mostly via telephone) were utilized to assess the need for and provide bereavement support. Some participants were not sure how bereavement services were provided to families with LEP.
Strategies utilized to communicate with patients/family caregivers with LEP
We identified two major themes: (1) the need for language-concordant home hospice staff (e.g., Chinese- and Spanish- speaking nurses, social workers, and chaplains) and (2) greater access to VRI services. Respondents shared that in rural areas, VRI or OPI is limited due to connectivity issues. Some participants reported “in-person interpreter services are always preferred but often not available.” Other participants shared that regardless of the mode of medical interpretation being employed, professional interpreters should be trained in hospice care specifically. Finally, some participants shared that sometimes medical interpreters are “not accepted by family members” due to preferring family caregivers to do the interpretation. Finally, provision of written and electronic hospice and bereavement materials in various non-English languages was viewed by some participants as beneficial.
Discussion
Our study of home hospice care providers sought to investigate respondents’ experiences when communicating with patients and families with LEP, estimate the frequency of use of medical interpreters, and ascertain the strategies providers use to communicate with patients and families with LEP. Participants across the United States reported that one in fivehospice care recipients have LEP. The majority of participants reported that their hospice agency has a formal policy on providing language assistance for patients/families with LEP. OPI was most utilized by home hospice providers. Use of ad hoc interpretation, such as adult family members and hospice staff who spoke the same language as the patient with LEP, was also commonly utilized by home hospice providers. When looking at geographical location as a factor for medical interpreter utilization, providing care in a Western state was associated with a greater use of language-concordant hospice staff and translated hospice materials. Having bilingual hospice staff and non-English language bereavement materials were viewed as important strategies to provide bereavement support services. Many participants advocated for affordable medical interpreters experienced in the hospice and EOL setting.
It is not known what percentage of home hospice recipients in the United States are either non-English language speakers or have LEP. At present, hospices are not required to collect or report on patient language preference or LEP status. This is a health equity measure that should be addressed in the coming years. In the calendar year 2022, 38.1% of Asian American Medicare decedents and 38.3% of Hispanic decedents received hospice services compared to 51.6% of White Medicare decedents. 24 A nationwide survey of adults who experienced the death of a loved one with a serious illness conducted by the National Hospice and Palliative Care Organization found that 52% of Hispanic respondents said they would need hospice workers who spoke Spanish in order to feel comfortable with their health care provider. 25
To date few studies have evaluated how U.S. based hospice agencies meet the needs of LEP patients and family caregivers receiving home hospice care. Existing studies evaluating health care providers’ utilization practices of medical interpreters delivering EOL care, have found that medical interpreters are underutilized.12,26,27 Working with in-person medical interpreters is viewed as the gold standard in the palliative care and hospice setting given their unique skills to identify nonverbal cues and provide culturally sensitive care.12,26–28 Medical interpreters have both linguistic and cultural competency training. Use of family members as interpreters in EOL conversations is discouraged as they often undermine the quality of interpretation by filtering or providing inaccurate information. 12 However, organizational barriers such as limited financial resources affect home hospice agencies access to various modalities of medical interpretation. The cost of interpreter services varies widely, ranging from $45–$150/hour for in-person interpreters to $1.25–$3.00/minute, for telephone interpreters and $1.95–$3.49/minute for VRI. 29 In our study, remote interpretation (telephone and video) was commonly utilized by home hospice providers, which are services found to be more accessible in the health care setting compared to in-person medical interpreters. Further studies are needed to evaluate how VRI compares to in-person interpretation in the home hospice setting where outcomes include patient symptom burden and family satisfaction with the services provided.
Box 1. Illustrative quotes regarding bereavement services provided to families with LEP
“We send condolence cards and grief support materials in the patient’s primary language.”
“We have translated materials for most common languages and can use interpreter services... We can also refer to multicultural agencies who provide grief and bereavement support.”
“We try to connect them with staff that speaks their language and is culturally competent.”
“Usually telephone interpretation services—Language Line. We have one Spanish-speaking bereavement counselor who is usually assigned to family members who speak/prefer Spanish.”
“Clients are asked if they would like to be referred to a mental health practitioner of their own culture who speaks their language or with hospice grief support specialist and phone interpreter.”
Access to various types of interpreters (i.e., telephone, video, and in-person medical interpreters) varies greatly by hospice agency and specific modes of interpretation (e.g., in-person interpreters) are not often available due to cost issues. Patients have the right to effective communication. Adequate language support can lead to a decrease in health care expenditures as medical interpreters reduce medical errors and decrease readmission rates. 30 Accordingly, more financial resources are needed for medical interpretation in the home hospice setting given current levels of reimbursement. Hospice organizations are generally not directly reimbursed for medical interpreters through Medicare, as the Medicare hospice per diem payment covers all daily care costs. 31 Additionally, we advocate for interpreter agencies to invest in additional training of medical interpreters in how best to communicate with patients/families with LEP receiving EOL (as well as palliative) care.32,33
Our findings suggest that written materials (both print and digital) addressing bereavement and symptoms at EOL be available in a variety of languages. Offering culturally appropriate written materials in the care recipients’ native language demonstrates commitment to respecting the community’s culture and values. We encourage hospice organizations to provide easy-to-read, culturally appropriate, and language-concordant materials to support patients/families with LEP. An important strategy to overcome language barriers in the home hospice setting includes encouraging hospice providers who are native speakers in a nondominant language to undergo a formal language skills assessment and potentially receive formal medical interpreter training.
Box 2. Illustrative quotes regarding respondents’ suggestions for communicating with patients/families with LEP
“The most practical would be video interpreter because we serve such a broad patient population.”
“Web based video is the best we can hope for in reality, although in person would be better.”
“When using an interpreter service, it would be extremely helpful if the service had staff trained in hospice care specifically.”
“An app that provides in the moment translation—with medical terminology built into it.”
“Encourage acceptance by family members of telephone medical interpreter, as many family members as well as patients resist this modality.”
“Inexpensive services covered by insurance and not directly paid for by hospice.”
“Technology to provide video services at minimum. Cost is often prohibited. Need cell phone/internet connection as we are rural.”
“Availability of employees who speak different languages. Familiarity with translation services. We do not use it often so we are unfamiliar.”
“Having staff fluent in the language of the patient is ideal. In the rural setting, teleservices (voice or video) is not reliable.”
“The video language service... is a good tool for clinical visits (nursing and social work). However, my area is spiritual care and I find that the video language service is not as helpful in this context.”
Health care organizations should evaluate innovative approaches to delivering language assistance services to patients and families with LEP. In this context, the potential application of artificial intelligence (AI) for written translations and low-stakes communication in the hospice setting warrants consideration. AI chatbots and voice assistants have the potential to manage appointment scheduling, prescription refills, and reduce administrative burden on hospice staff while helping ensure equitable access to health care services and information for hospice patients and families with LEP. 34 The authors believe that AI tools should complement but not replace medical interpreters. Careful ongoing evaluation will be needed to ensure that any AI-generated tools and interventions are culturally sensitive and produce clinically meaningful outcomes.
The study has several limitations that warrant attention. First, although we were not able to calculate an exact response rate, few providers responded, raising the possibility of nonrespondent bias. Second, the instruments used to ascertain study outcomes were created de novo as we were unable to identify validated measures for these constructs. Third, the survey instruments were developed without the input of a medical interpreter. However, various members of the multidisciplinary project team were bilingual and/or experts in language barriers. Lastly, the majority of the physician respondents were Medical Directors, who typically do less clinical work compared to other team members and may not have updated information. To our knowledge, this is the first study that reports on the frequency of use of medical interpreters in the home hospice setting. Despite relatively few responses, this investigation generates new knowledge regarding the type(s) of interpretation hospice providers routinely utilize to assess symptoms, as well as provide support and bereavement counseling. The reported prevalence of patients with LEP enrolled in home hospice was substantial, which suggests that hospice providers face language barriers on a regular basis. This phenomenon is only likely to grow in the coming decades.
Conclusion
Our findings demonstrate that OPI was most commonly used by home hospice providers. Ad hoc interpretation, including the use of adult family members and bilingual hospice staff, was also frequently employed. Having bilingual hospice staff and non-English language bereavement materials were viewed as important strategies to support patients and families with LEP.
Footnotes
Disclaimer
Views and opinions expressed in the article are our own and do not represent that of our places of work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.