
Abstract
Background:
Children with life-limiting conditions often have complex care needs, and their caregivers require expert clinical support after-hours and over weekends to support care at home.
Objectives:
This quality improvement initiative examined usage patterns and impact on caregiving of the nurse-led 24-Hour Clinical Care Line initiated in 2018 by the Canuck Place Children’s Hospice, which provides inpatient and community-based pediatric palliative care and respite for children with life-limiting conditions in British Columbia and the Yukon in Canada.
Methods:
Phone call tracking logs and clinical profiles were analyzed to examine user demographics, temporal usage patterns, and reasons for calling. Families were asked to provide feedback on the service for quality improvement.
Results:
From June 2020 to March 2024, 194 families placed 1106 calls. Mothers/foster mothers made 67% of the calls. Caregivers of children with central nervous system (CNS) and metabolic conditions made a significantly higher number of calls per child on average. Caregivers calling about children aged <1 year represented a disproportionately large group of callers. Parents of children >15 years made significantly fewer calls. The most common call reason was family support (73.1%), followed by providing an update on child status (58.5%), pain and symptom management (50.9%), and care planning (10.9%). Call volume peaked at bedtime and was consistent over nighttime hours and weekends. Late winter and spring were the most popular seasons for calls, following typical temporal influenza patterns.
Keywords
Key Message
Families of children living with serious illnesses benefit from specialized clinical support through 24/7 pediatric palliative nurse-led telephone lines. Staff nurses respond to calls for various complex care needs throughout the day and year-round. Findings suggest value in exploring how this service supports family goals of care and symptom management.
Introduction
Pediatric palliative care (PPC) helps seriously ill children and their families manage disease progression, pain, symptoms, and psychosocial and spiritual needs to support quality of life from diagnosis into bereavement. 1 PPC is delivered across multiple care settings requiring multidisciplinary expertise due to the prevalence of rare illnesses and nuances related to child development. 2 Given the complex needs of these children, caregivers often require specialized after-hours clinical support. During these times, families may rely on emergency and urgent care services, which may be unequipped to meet their specific needs.3–5 Adult literature suggests around-the-clock telephone nursing support alleviates stress and costs for families6,7 and health care institutions 8 by offering timely advice and preventing unnecessary care visits. These services can be helpful for families in regions lacking tertiary health care infrastructure 9 or for families who wish to remain home, 10 but who may need increased clinical support near the end of life. 11 General telephone triage services, such as 811, are offered across Canada, but likewise may not be specialized to assist children with rare, complex conditions. 7
Examination of the utilization and impact of adult palliative care lines is comparatively abundant in the adult literature 12 ; however, only one service was evaluated in Canada for adults receiving home-based care for advanced illness. 13 Evidence is even more limited in pediatric literature. Research on telephone lines for children with serious illnesses includes services in the Netherlands for children with severe anatomical congenital anomalies 14 and in Australia for children with cancer 15 ; however, there is a need for evidence surrounding the value of telephone support within a PPC program. Published evaluations do not explore those services separately.16–21
Canuck Place Children’s Hospice(CPCH) is the leading provider of PPC for over 900 children with serious illnesses in British Columbia and the Yukon. Nearly six million people populate British Columbia, 22 with five health authorities with regional jurisdiction over health services. CPCH operates from two hospices and the tertiary children’s hospital in the Lower Mainland; however, some families on the program live on Vancouver Island, in more remote northern and eastern regions of the province, and in the Yukon territory. Children are referred to the program by health care professionals or family members. The Intake Committee (composed of experienced pediatric palliative clinicians) assesses child eligibility for the program based on diagnosis, function, fragility, and the four categories of life-limiting conditions developed by Together for Short Lives. 23 If a child is not expected to live into adulthood, they are often admitted into the program.
Since opening in 1995, CPCH has provided interdisciplinary inpatient and outpatient consultations in a tertiary pediatric hospital, in addition to services at a freestanding hospice. In 2018, the program expanded to community-based care, including in-home and virtual visits, and a 24-Hour Nurse-Led Pediatric Palliative Clinical Care Line (24-Hour Line). The 24-Hour Line is answered by registered nurses with access to on-call physicians and nurse practitioners employed at CPCH. Caregivers call for advice regarding their child’s emerging symptoms, daily care concerns, medications, medical equipment, end-of-life support, and advice on transfer to hospital. Importantly, the 24-Hour Line allows families with comfort-focused medical directives to reach expert nursing staff who can escalate in-home symptom and psycho-social-spiritual support when the child is imminently dying or has died.
This article describes a quality improvement initiative that aimed to evaluate the utilization patterns of and parent feedback on the CPCH 24-Hour Line, focusing on reasons for calling, characteristics of calls, and implications for PPC delivery.
Methods
Families on the CPCH program have access to the 24-Hour Line, which during weekday operating hours is typically answered by nurses with the hospice community care team. Experienced PPC staff nurses—on shift for an inpatient care assignment—also cover incoming calls “after-hours” and on weekends. Figure 1 summarizes service operations.
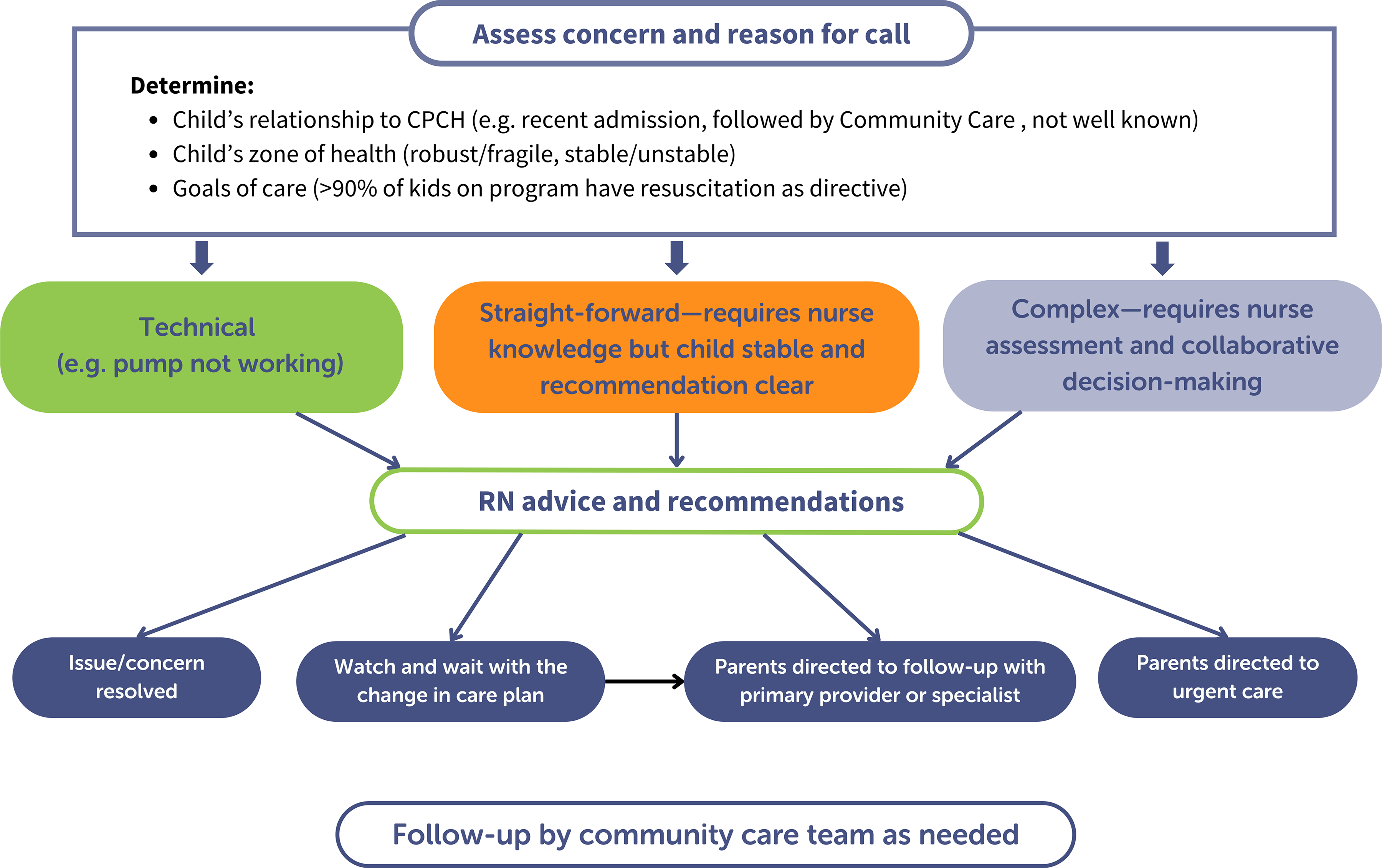
Sequence of events and decision-making in operation of the 24-Hour Line.
Due to increasing demand for the 24-Hour Line since its inception, a quality improvement project was initiated to aid leadership in understanding capacity in staffing, competency, and training. Nurses used paper logs to track the date, time, patient name, reasons for calling, and need for follow-up of incoming calls from June 2020 to March 2024. A nursing student transferred this data into an electronic, deidentified Excel file. A hospice nurse verified 10% of call log entries for quality control and reported a 0% error rate. The hospice database analyst provided illness characteristics and ages of children whose caregivers utilized the service. Regional health authority guidelines classify this call-tracking project as quality improvement, which, therefore, did not require Research Ethics Board review.
Family input and consent to be contacted for surveys are part of hospice practice. To further expand this quality improvement project, families who called in the more recent months of April–June 2024 received email invitations to complete an exploratory survey on their reasons for calling, ratings of helpfulness of the service, and additional open-response feedback on their experiences using the 24-Hour Line. Data was de-identified. Survey respondents could optionally provide contact information for compensation with a $5-e-gift card to a coffee shop.
Data analysis
Negative binomial regression was used to model the number of calls per family. Because call counts are nonnegative integers and preliminary Poisson models indicated overdispersion, negative binomial models were fit using a log link. Separate models were estimated to examine whether call volume differed by (1) diagnostic group, (2) age group, and (3) health authority.
Because calls were aggregated at the family level across available months, there were no missing observations in the analysis of negative binomial regression or chi-squared comparisons. Descriptive statistics were calculated with listwise deletion to address minimal missing data due to illegible, incomplete, or incorrect entries or scanning errors (<1%). Unknown missing data are possible if call logs were misplaced by a busy unit clerk, mistakenly discarded before scanning, or if tracking was disrupted during the inception of the service and the COVID-19 lockdown. Nine months of call logs are missing due to administrative processes and thus are assumed to be Missing Completely at Random for temporal analyses. A chi-squared goodness-of-fit test was used to compare the proportion of calling patients to patients on the program across the group variables. In cases with low expected counts, Fisher’s exact test was used to confirm findings. Significant differences were followed with post hoc examination of standardized residuals, where residuals >|2| describe meaningful over- or underrepresentation of observed proportions. All analyses were conducted using R (Version 2025.05.1 + 513). 24
Results
Over the data collection period, we logged 1106 calls from 194 families. Calls per month ranged from 7 to 61, with 30 on average. Calls per family ranged from 1 to 57, with a median of 2. The 36 months of complete call logs informed analysis. Mothers and foster mothers contributed 67% of calls, while fathers and foster fathers contributed 15% (Fig. 2). The caller’s relationship to the child was missing for 4 calls (0.4%; (Fig. 2). Age of child when a caregiver made their first call was an average of 8.29 years and ranged from 1 day to 21 years.
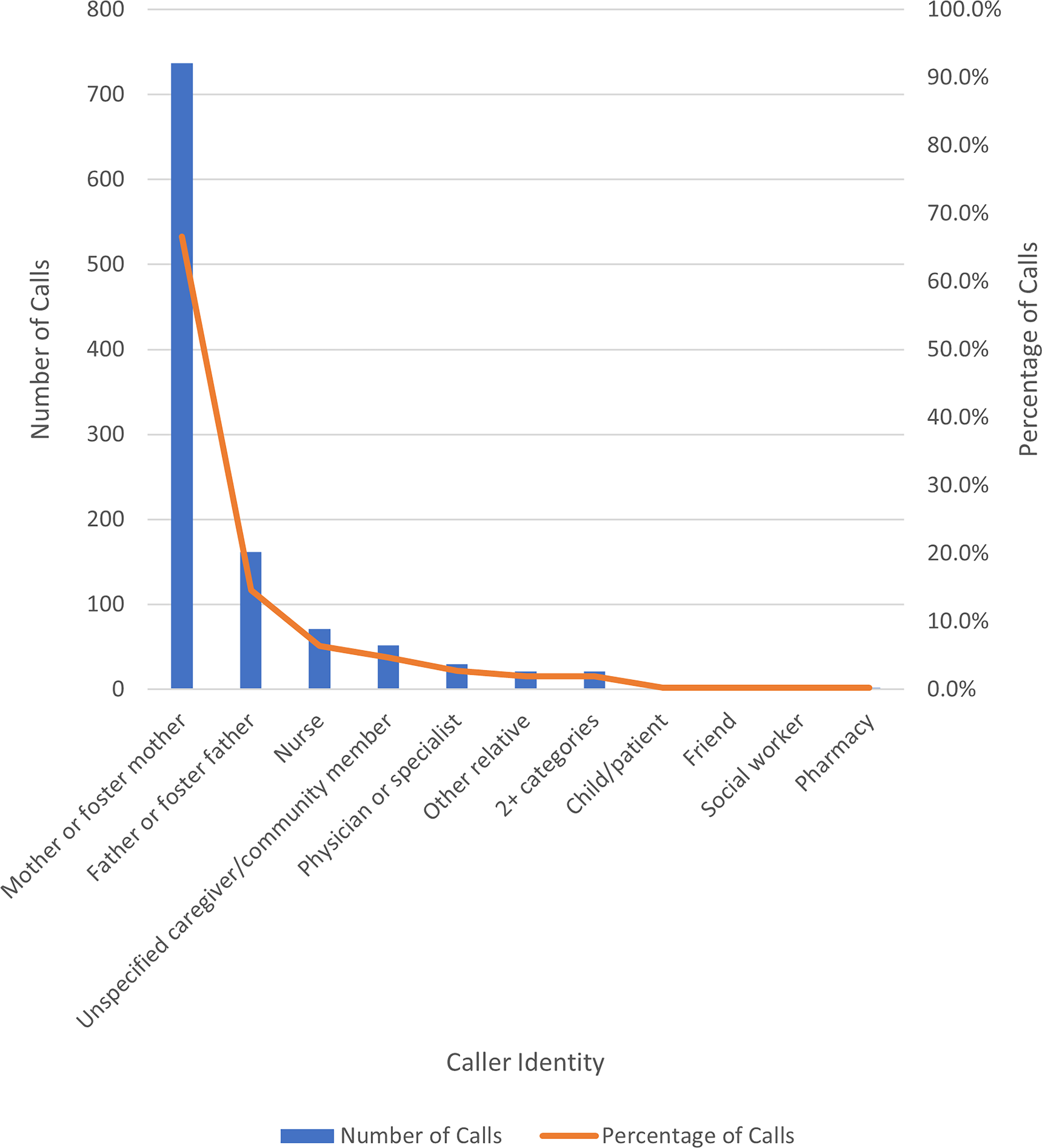
Caller relationship to child (N = 1102).
Comparison between call rates for diagnostics, age, and health authority
Call rate refers to the average number of calls made per child. The mean call rate was 5.7 calls per child. The negative binomial regression revealed that compared to the mean, children 15 years and older reported significantly lower call rates (IRR = 0.61, 95% = [0.45, 0.83], p = 0.001, Supplementary Table S1), reflecting a 39% reduction in expected calls. Children with metabolic (IRR = 2.57, 95% CI = [1.57, 4.20], p < 0.001, Supplementary Table S2) and central nervous system (CNS) conditions (IRR = 1.88, 95% CI = [1.30, 2.74], p < 0.001, Supplementary Table S2) reported significantly higher call rates, reflecting a 157% and 88% increase in expected calls, respectively. Children in Interior Health reported significantly higher call rates (IRR = 1.48, 95% CI = [1.03, 2.11], p = 0.032, Supplementary Table S3), reflecting a 48% increase in expected calls. No other significant differences were found. Rate ratios are reported in Supplementary Tables S4, S5, and S6.
Comparison to CPCH program data on diagnostics, age, and health authority
In the 2022/2023 fiscal year, 524 children were enrolled in the program. We compared the age, diagnosis group, and health authority distributions of children whose families called to those of all children on the program. The age group represented by the 194 patients was determined based on when the child’s family made their first call, whereas the number of calls represented by each age group was determined using the child age on the specific call date. Health authority of one child on the program was missing (0.2%; Supplementary Table S3).
A chi-squared goodness-of-fit test indicated that the distribution of calling patients differed significantly from those on the program based on age group (χ2(4) = 19.70, p < 0.001). Post hoc analyses of standardized residuals (Supplementary Table S7) indicate that the <1 year age group (21.6%) was disproportionately large given their respective proportion in the program (11.8%) (Supplementary Table S1). No significant differences were found for diagnostic groups or health authority.
Reasons for calling
A single call could occur for one or multiple of the following reasons: “Update on status” could be caregivers updating the hospice on a recent development, hospital admission/discharge, or changes initiated by another health care provider. “Family support” involves psychosocial support for caregivers. “Care planning” refers to support for a child’s care coordination such as upcoming hospice admission or arranging orders for in-home respite care from a nurse. “Pain and symptom management” could involve new or evolving symptoms requiring triage support, assessment, and management by the PPC team or through referral. The leading nurse-identified reason for calling was family support (808 calls; 73.1%), followed by update on status (647; 58.5%), pain and symptom management (563; 50.9%), and care planning (121; 10.9%). Call reasons for 4 (0.4%) calls were missing.
Temporal patterns
Call volume was higher during daytime hours and peaked at bedtime at around 9PM. Call volume was relatively lower but consistent during nighttime hours (Fig. 3). Time was missing for 11 calls (1.0%).
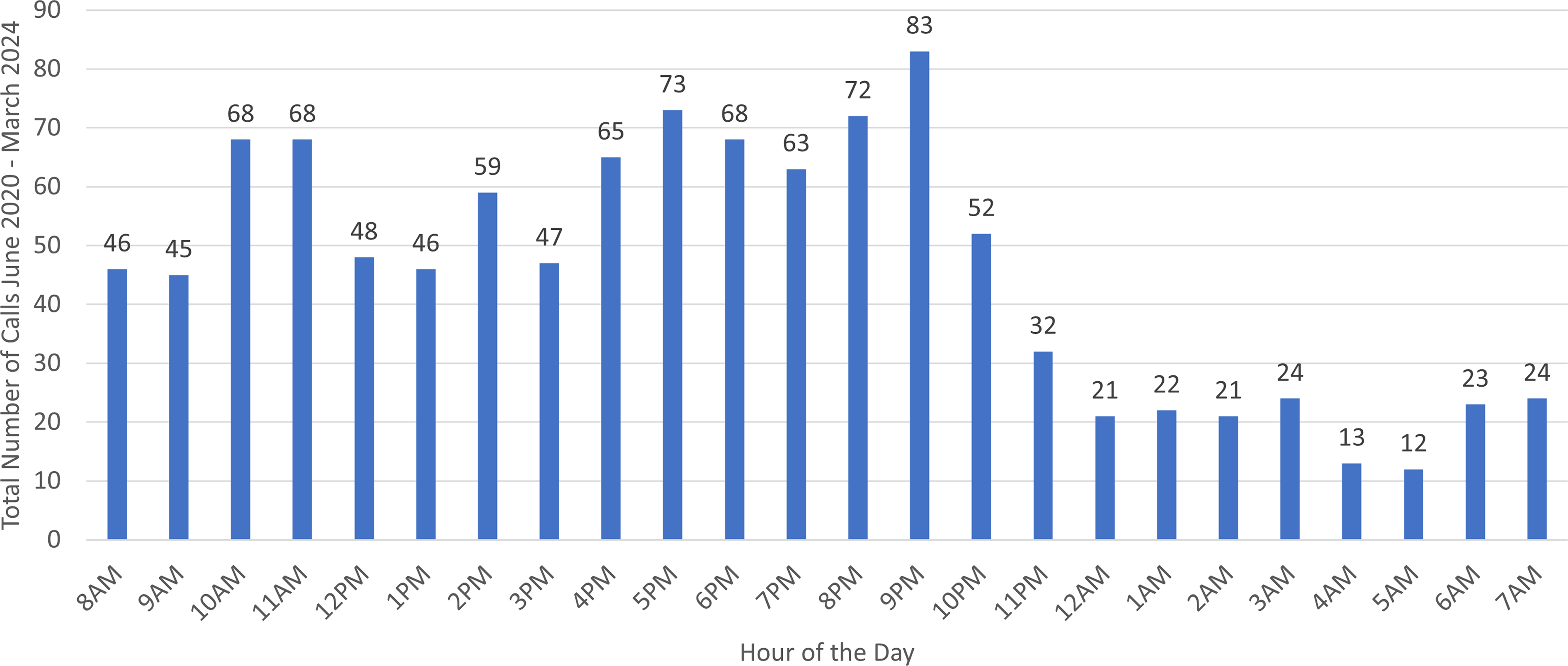
Total call volume by hour of the day (N = 1095). Calls occurring from 12:00 AM to 11:59 PM were counted for that day.
The average number of calls that occurred on any given weekday (Monday through Friday) was 0.82 calls per day and 1.025 for any weekend days (Saturday and Sunday).
Average number of calls per month peaked in April, was lowest in May, and climbed into another peak in December (Fig. 4). Care planning calls exhibit a relatively lower but consistent call volume, whereas calls for pain and symptom management, update on status, and family support appear to fluctuate as per the total call volume trends (Fig. 4). Average monthly call volume was lower in 2020 and 2021 (13 and 11 calls, respectively) and increased annually to 35 per month in 2022, 32 in 2023, and 41 in 2024.
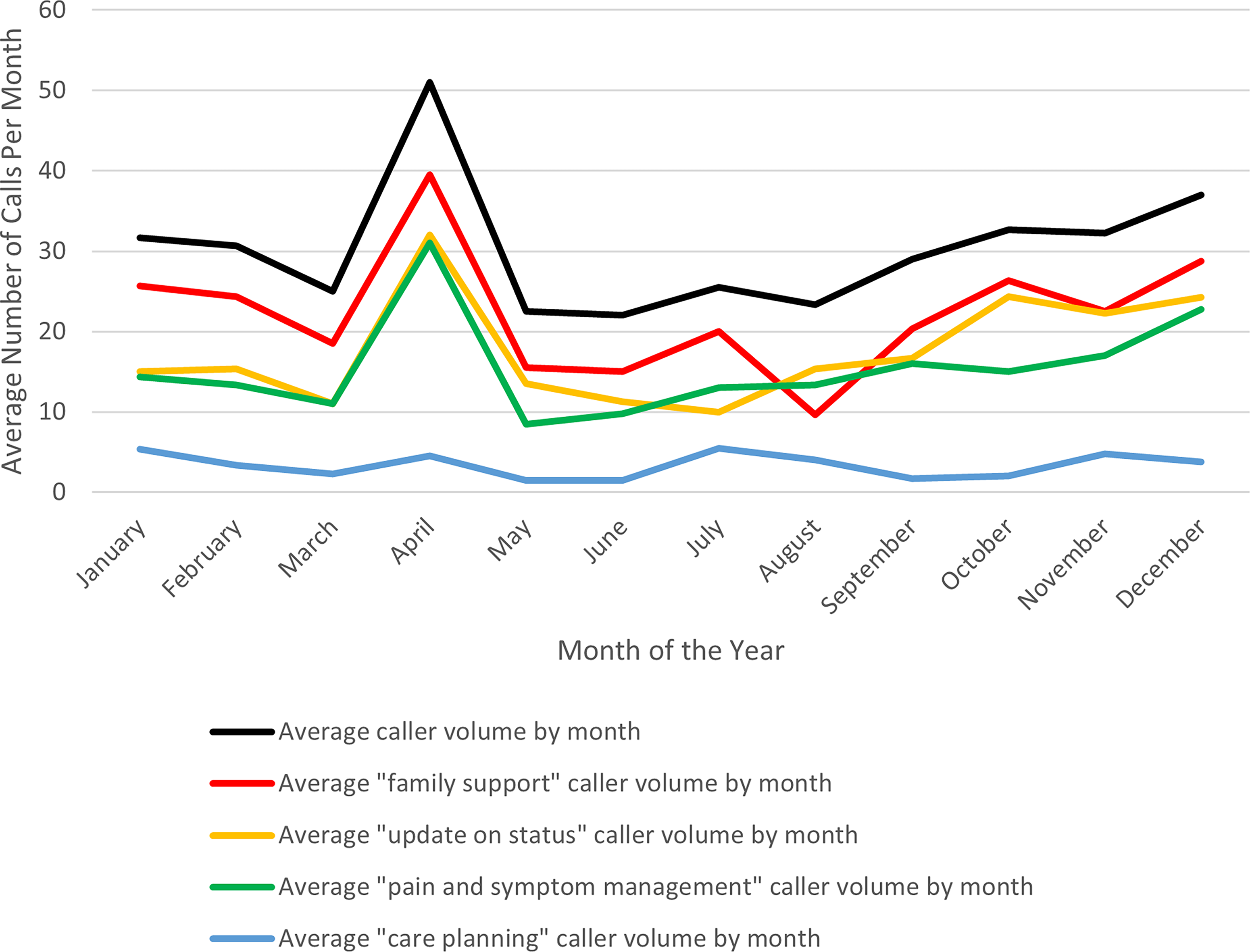
Average number of calls by month of the year, in total, and by reason.
Family feedback survey
Between April and June 2024, 42 families utilized the 24-Hour Line. We contacted 40 families with an invitation to complete the survey, and 13 families responded, yielding a participation rate of 32.5%. Call reasons are classified differently in the survey than nurse-reported call logs to facilitate caregiver interpretation and distinguish calls about medical equipment from calls about medication. Families reported calling most frequently for symptom management (12/13; 92.3%), followed by decision-making support (10/13; 76.9%), medical equipment (8/13; 61.5%), family support (3/13; 23.1%), and medication (1/13; 7.7%).
Families were asked to rate how helpful the service was. No respondents stated the service was “Not Helpful,” 1 found it “Helpful,” and 12 found it “Very Helpful.” If the 24-Hour Line was unavailable, 11 (84.6%) families would have consulted the emergency department (Supplementary Table S8). In open-response comments, caregivers appreciated reaching nurses and clinicians who were familiar with them and their child and found reassurance during emergencies or onset of unfamiliar symptoms. Families noted the competency and relevance of 24-Hour Line advice for their child’s complex care as opposed to alternatives, such as urgent care. Reported issues included repeating information when calls are answered by a personal care assistant or receptionist before being transferred to nursing and desire for clinical support that accommodates families in regional areas, as opposed to the Lower Mainland.
Discussion
Increased evidence on pediatric palliative telephone nurse lines with after-hours availability can inform implementation and improvement of similar services by other PPC providers in Canada and internationally. This study examined caller characteristics and usage patterns for a 24-hour pediatric palliative nurse line in Canada. Results suggest this service provides support for caregivers of children with various complex care needs and can be a valuable addition to a PPC program.
Caregivers of children 15 years or older called significantly less frequently. Most of these children live with oncological disorders (Supplementary Table S9) and may have ongoing connections with the oncology team and enhanced community care team, who already provide surveillance and care planning for anticipatory needs. Adolescents with cancer may also be reluctant to call the 24-Hour Line for fear of judgment and stressing caregivers, overwhelm of medical information, and despair about disease progression. 25 Caregivers may also have become more equipped to care for adolescents who have lived with their disease longer.
Children younger than 1 year whose caregivers called the service represented a disproportionate 21.6% of callers compared to 11.8% of the CPCH program. Our program supports newly discharged infants from the NICU with life-limiting illnesses. Anecdotally, nurses have reported receiving more calls about infants shortly after discharge; however, this age group does not exhibit a significantly higher call rate. Caregivers of newborns transitioning from hospitalization to home often require extra educational and psychosocial support, and it could be that families rely on the service upon discharge, then call volume decreases after they adapt to caring for their newborns.26,27
Children with metabolic or CNS conditions had significantly higher call rates than other diagnostic groups, which may be due to their medical complexity and shifting health baseline. These families may also have engaged more with inpatient services at CPCH, such as hospice admission and respite stays, resulting in higher familiarity with the staff and the service, thus increasing utilization.
Families from Interior Health exhibited a significantly higher call rate; however, children in Northern Health, who would be farther on average from the hospice, did not call more often, despite potential advantages of telenursing in reducing safety risks, discomfort for children, and psychosocial and financial caregiver burden during farther travel to in-person visits. 28 The Northern Health Authority serves a smaller, sparser rural population. Rural families may be less aware of or willing to use telehealth services 29 due to lower utilization of hospice care and familiarity with CPCH clinicians. It is possible families in Northern Health prefer consulting clinicians within their community who have become clinically familiar with their child and have adopted more versatile practice capacities as demanded in rural health care. 30 Further investigation on resources available and where care is utilized relative to where families reside in each health authority can build understanding of these call patterns.
Nurses reported “family support” as the leading call reason. Similar services evaluated in the literature also observed that daily care and psychological support were valuable to caregivers.14,15 Those services also identified “communication” 15 and “information” 14 as prominent reasons for calling, which may coincide with “update on status” as the next leading reason for calling the CPCH service. While the survey and call log samples are not suited for comparison, surveyed caregivers reported “symptom management” rather than “family support” as their leading call reason. The discrepancy in call reason could be because symptoms prompt caregivers to call, and nurses recognize the distress as a need for reassurance, thus labeling the call “family support.” Future qualitative explorations could inquire what this divergence reveals about communication dynamics among nurses and families and differing perceptions of care needs.
Increased call volume on weekends is likely due to other services being offline or unavailable. Monthly call volume fluctuations may be attributed to seasonal outbreaks of respiratory illness. Children discharged home in March after hospitalizations during flu/cold seasons may have required increased support upon returning home, which could contextualize the increasing call volumes in April. These temporal patterns are comparable to available research on the 811-health information line in Nova Scotia, Canada. 31 which also peaked in late spring and winter months and evening hours and remained steadily low at night. 31 We expect annual call volume to increase with expansions to the program and outreach and quality improvements to the 24-Hour Line that provide more accessible, reassuring, and timely support to families navigating serious illnesses in childhood.
Limitations
Phone call tracking relied on nurses recording information on paper call logs at the nursing station, which were scanned into a PDF archive, which introduced opportunities for missing data. The purposive survey sample represents a minor portion of families in the data collection period, and results may provide skewed feedback due to self-selection bias. While the survey period is brief, it aims to capture how helpful caregivers found the service and suggestions for improvement rather than seasonal variations and long-term evolution in caregiver experiences. This project aims to reflect perceptions and needs specific to the CPCH 24-Hour Clinical Care Line for quality improvement and may have limited generalizability of findings to other PPC settings, including in international contexts with varied health care infrastructures.
Future directions
Interestingly, most surveyed caregivers would have utilized emergency care if the CPCH 24-Hour Line were not available. Future directions can utilize prospective designs to investigate medical records and emergency department visits to examine patient outcomes after calling the 24-Hour Line, and whether this service helps families avoid unnecessary hospitalization and supports care goals. Further qualitative exploration of caregiver burden, well-being, and capacity may detail the relational value of the service.
Conclusion
Findings on the impact and value of the 24-Hour Clinical Care Line in the Canuck Place Children’s Hospice program are promising and endorsed by families. PPC nurses answer calls across a range of age, diagnostic, and geographic demographics on the program, but especially for children under 1 and children with CNS and metabolic conditions. Caregivers call at various times to seek reassurance and care advice, including updates on status, pain and symptom management, and care planning. Some families develop longitudinal relationships with nursing staff and call the 24-Hour Line repeatedly for support throughout a child’s life.
Clinical Palliative Care Program
Program description
Canuck Place is a major provider of PPC for children with serious and life-threatening illnesses in British Columbia and the Yukon. It is the first freestanding hospice in North America, opened in 1995. The PPC program provides pain and symptom management, family support, care coordination, end-of-life care and bereavement support by an interprofessional care team. As part of this service, Canuck Place offers both community care and outreach services, as well as a centralized 24-Hour Telephone Line available to all families on the program.
Canuck Place Children’s Hospice has two hospice locations, in Abbotsford and Vancouver, with 8 family suites and 10 patient beds in total across the 2 sites. Care is provided free to families as payment sources for the operating budget, which includes philanthropy and government funding from the Ministry of Health, Province of BC.
Team staffing
The community care team of our palliative program comprises the following team members:
Nurse Practitioner (1.5 FTE) and Clinical Response Registered Nurses (3.5 FTE). The hospice is staffed with 3 palliative care nurses on the inpatient unit who also answer the 24-Hour Line after normal business hours. Counsellors are available Monday-Friday during daytime hours and on-call on most weekends. One MD is on call 24/7 for the hospice and is also available to respond to calls on the 24-Hour Line when needed after hours.
Program availability
PPC is provided in-hospice, in-hospital, virtually via telephone and telehealth, and in the patient’s home. Inpatient services include respite, pain and symptom management, and end-of-life care. Outpatient services include in-person consultations at the tertiary pediatric hospital and virtual visits for local community hospitals. Community care services include home and community visits, in addition to the above. The Community Care team is available 7 days a week for regular day hours and on-call during periods of urgent patient response needs, as assessed by the team. Canuck Place utilizes a Zones of Health© framework, comfort-directed goals of care and desire to stay in their home community to determine appropriateness for the Enhanced Community Care program and needs that would benefit from increased support in the home community.
Patient volume and interactions
The average daily census across the two sites is 6.8 children; however, only the main hospice location in the city of Vancouver answers the 24-Hour Line calls. There are typically four to six children staying in the house as inpatients at this site at any given time. The average number of new referrals to the program per year is 200, with approximately 920 children in the program across all the services. Overall, about 350 children accessed medical consults, counseling, or recreation therapy or had an admission yearly, along with 268 families who accessed the bereavement services.
Authors’ Contributions
C.v.B.: Conceptualization and writing—review and editing. S.L.: Conceptualization, methodology, and investigation (survey design). C.Z.: Investigation (data entry), writing—original draft, visualization, and methodology. J.Z.: Formal data analysis, contribution to writing—original draft. G.A.: Conceptualization, methodology, writing—original draft, and project administration.
Supplemental Material
sj-docx-1-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-1-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-2-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-2-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-3-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-3-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-4-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-4-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-5-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-5-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-6-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-6-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-7-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-7-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-8-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-8-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Supplemental Material
sj-docx-9-plm-10.1177_10966218261460532 — Supplemental material for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line
Supplemental material, sj-docx-9-plm-10.1177_10966218261460532 for Help Is a Phone Call Away: A 24-Hour Nurse-Led Pediatric Hospice Clinical Care Line by Camara van Breemen, Stephanie Liversidge, Christina Zeng, Jason Zheng, and Gail Andrews
Footnotes
Acknowledgments
The authors would like to thank Dr. Louise Lund, PhD, for provisioning data; Nadine Lusney, RN, MSN, for assisting in survey development and distribution; and Dr. Hal Siden, MD, MHSc, FRCPC, for his guidance and critiques.
Author Disclosure Statements
The authors declare no conflicts of interest.
Funding Information
This quality improvement project was funded by the Canuck Place Children’s Hospice Research Initiative and a summary student bursary from the British Columbia Children’s Hospital Research Initiative.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.