
Abstract
Although women are the focal point of abortion care, a woman’s male partner may accompany her to the abortion appointment. Using Connell’s “hierarchy of masculinities” framework, this study examines how male partners negotiate their identity and role in an unfamiliar setting while their female partners undergo an abortion. Twenty-seven in-depth interviews with male partners of women obtaining abortions at a community-based and a university-based abortion clinic were conducted. The interviews reflected the tension male partners felt while attempting to maintain characteristics of hegemonic masculinity (e.g., dominance, stoicism, ambition, and fatherhood) in an environment where their female partner’s needs were prioritized. Some male partners expressed distress about their inexperience with the process and procedure as well as their inability to participate or better care for their partners. Others negotiated alternative definitions of masculinity, emphasizing a duty and/or desire to provide support during his female partner’s pregnancy decision-making and abortion experience.
Nearly one million abortions are performed in the United States annually (Jones and Jerman 2017a). As close to 25 percent of women will have had an abortion by the age of forty-five (Jones and Jerman 2017b), abortion care is appropriately centered on the experience of women. However, more than 80 percent of women report informing their male partner about their abortions (Major et al. 1997) and up to half of all abortions are attended by male partners (defined in this study as the man involved in a pregnancy; Jones, Moore, and Frohwirth 2011). Despite the substantial number of men who may be involved in abortions, whether during the decision-making process or the actual abortion procedure, men’s experiences are not well described.
Previous accounts of male partner involvement in abortion provide conflicting, one-dimensional images of men’s abortion-related attitudes and behaviors. In some cases, the male partner takes on an antagonistic role, engaging in coercive behaviors (Park et al. 2016) or intimate partner violence (Coker 2007; Moore, Frohwirth, and Miller 2010) as a means of controlling his female partner’s discordant pregnancy beliefs, which could be to either continue the pregnancy or obtain an abortion. Other studies describe men endorsing feelings of failure and loss when their female partner opts to end a pregnancy that he would have chosen to continue (Holmes 2004; Johnson and Williams 2005). Nevertheless, other research shows that most men support their female partner’s decision to have an abortion, regardless of whether he would prefer she continue the pregnancy (Jones, Moore, and Frohwirth 2011; Shostak and McLouth 1984; Kero and Lalos 2004). These examples neither adequately represent the variety of ways in which men perceive themselves, particularly in a space dedicated to women, nor do they explain how men might reconcile their perceived role in the setting of discordant pregnancy desires with their female partner. To date, no study has explored men’s identity as men at the time of an abortion. The current study thus uses the lens of masculinity to better characterize men’s abortion-related attitudes and behaviors at the time of their female partner’s abortion.
Theoretical Framework: Hierarchy of Masculinities
To better understand the variation in male partners’ accounts of their experience with abortion, we considered the influence of masculinity. Masculinity, as described by Connell (2005), refers to a socially constructed role or identity, typically enacted by men to distinguish their behaviors and beliefs from other men as well as to maintain dominance over women. Masculine characteristics commonly include strength, stoicism, and ambition (Diamond 2002; Connell 2005, R. W.Connell 2009; Connell and Messerschmidt 2005) in contrast to feminine characteristics such as sensitivity, deference, and compassion (hooks 2004). The descriptor “being a man” thus refers to enacting a masculine, gendered identity. The beliefs and behaviors that make up one’s identity are taught, learned, performed, validated, and reinforced by an individual’s external environment (e.g., family, school, and the media), where variations within or deviations from one’s expected gender may have social consequences (Bandura 1977; Connell 1996b).
According to Connell’s (2005) masculinities theory, the spectrum of masculine beliefs and behaviors can be divided into four configurations according to an individual’s ability to achieve social and cultural power: (1) hegemonic, (2) complicit, (3) marginalized, and (4) subordinate. Hegemonic masculinity refers to the dominant, socially expected male identity that prioritizes status over women and other men. While being able to behave according to the standards of hegemonic masculinity is idealized by most men, achieving dominance is not always possible or desirable. In order to adapt to contexts where hegemonic masculinity cannot be embodied, these men compromise and position themselves within one of the other three configurations of masculinity (Connell and Messerschmidt 2005).
Men exhibiting a complicit form of masculinity, despite not being able to achieve dominance themselves, will still identify with hegemonic men and ideals. Thus, complicit men may still attempt to distance themselves from women and men whom they consider lower in the hierarchy of masculinity. Marginalized men perceive themselves to be unable to meet the expectations of hegemonic masculinity and unable to be accepted by hegemonic and complicit men. Therefore, marginalized men commonly identify as victims. Subordinate men, regardless of their own ability or opportunities, are prevented from enacting and embodying hegemonic masculinity. Examples of subordinate men may include some racial and sexual minorities as well as men of low socioeconomic status and mobility who experience discrimination (Connell 1996a; Whitehead and Barrett 2001). While hegemonic masculinity is the archetype sought by complicit and marginalized masculinities, those in the subordinate group may have a different appraisal of dominance. That is, subordinate masculinity describes the beliefs and behaviors of certain men as perceived by those subscribing to hegemonic masculinity ideals.
When men do not perceive their identity as part of a hierarchy, acceptance and compromise within are eschewed. As seen with the historical subordination and liberation of lesbian, gay, bisexual, transgender, and queer masculinity (Connell and Messerschmidt 2005), men are able to challenge hegemonic gender structures and expectations. Some masculinity scholars suggest that Connell’s hierarchy overlooks these beliefs and behaviors subsequently called as “oppositional,” “compulsive,” “compensatory,” or “protest” masculinities (Pyke 1996; Majors and Billson 1992; Connell and Messerschmidt 2005). While these labels suggest contentious identities, some of these men may intentionally and comfortably exist outside established standards of hegemonic masculinity by acknowledging their own vulnerability (hooks 2004), showing caretaking behaviors (Hanlon 2009), and expressing emotions usually associated with femininity, such as affection (Barrow 2015) and anxiety (Dolan and Coe 2011). Such behaviors and beliefs that challenge hierarchal masculinities can also be categorized as “reformed masculinities.”
Reproduction and Masculinities
Reproductive health and related behaviors present a unique set of circumstances with conflicting expectations of hegemonic masculine identity (Connell 2005). For example, hegemonic masculinity promotes male risk-taking behavior, such as condom avoidance (Noar and Morokoff 2002), sexual performance, and virility (Daugherty 2014), with human reproduction, contraception, and pregnancy prevention generally considered to be within the female domain. However, ascribing to these hegemonic ideals can result in unintended pregnancies (Courtenay 2000; Schofield et al. 2000) that can threaten alternate hegemonic ideals about becoming fathers and raising children (Marcell, Raine, and Eyre 2003). Men aiming for dominance within reproductive health may also view biological children as an opportunity to gain immortality (Throsby and Gill 2004) as well as respond to expectations that they will be present, competent fathers, act as the head of the household (Weber 2012), and care for their female partner throughout her pregnancy and during childbirth (Reich 2008; Johnson 2002).
The abortion setting provides a window into how men negotiate the discordant expectations of hegemonic masculinity made evident by an unintended pregnancy. A few studies from Latin America analyzed the relationship between masculinity and abortion, evaluating men’s dichotic perspective on reproduction and sexual behavior as well as their conflicting desires for children and for their female partner’s well-being (Salcedo Fidalgo 1999; Vigoya and Navia 2012). In the United States, Reich (2008) published “a masculinist discourse of abortion,” based on in-depth interviews with twenty men whose female partners had an abortion. These men described how these experiences confronted their masculine identity, particularly their desire to be competent fathers. Men who supported abortion did so primarily to delay parenting so that they could later provide the social and financial resources needed to be a father, or in some cases, in order to find a more suitable mother for “his child” (Reich 2008). This study was limited, however, by its inclusion of men whose abortion experience took place up to thirty years before their interview. We hypothesized that more variation in the masculine narrative would emerge among men interviewed at the time of their female partner’s abortion. We thus explored how these men experienced their partner’s abortion and how they reconciled the abortion with their masculine identity, guided by the aforementioned hierarchy of masculinities framework (Table 1).
The Hierarchy of Masculinities Framework and Its Relation to the Abortion Context.
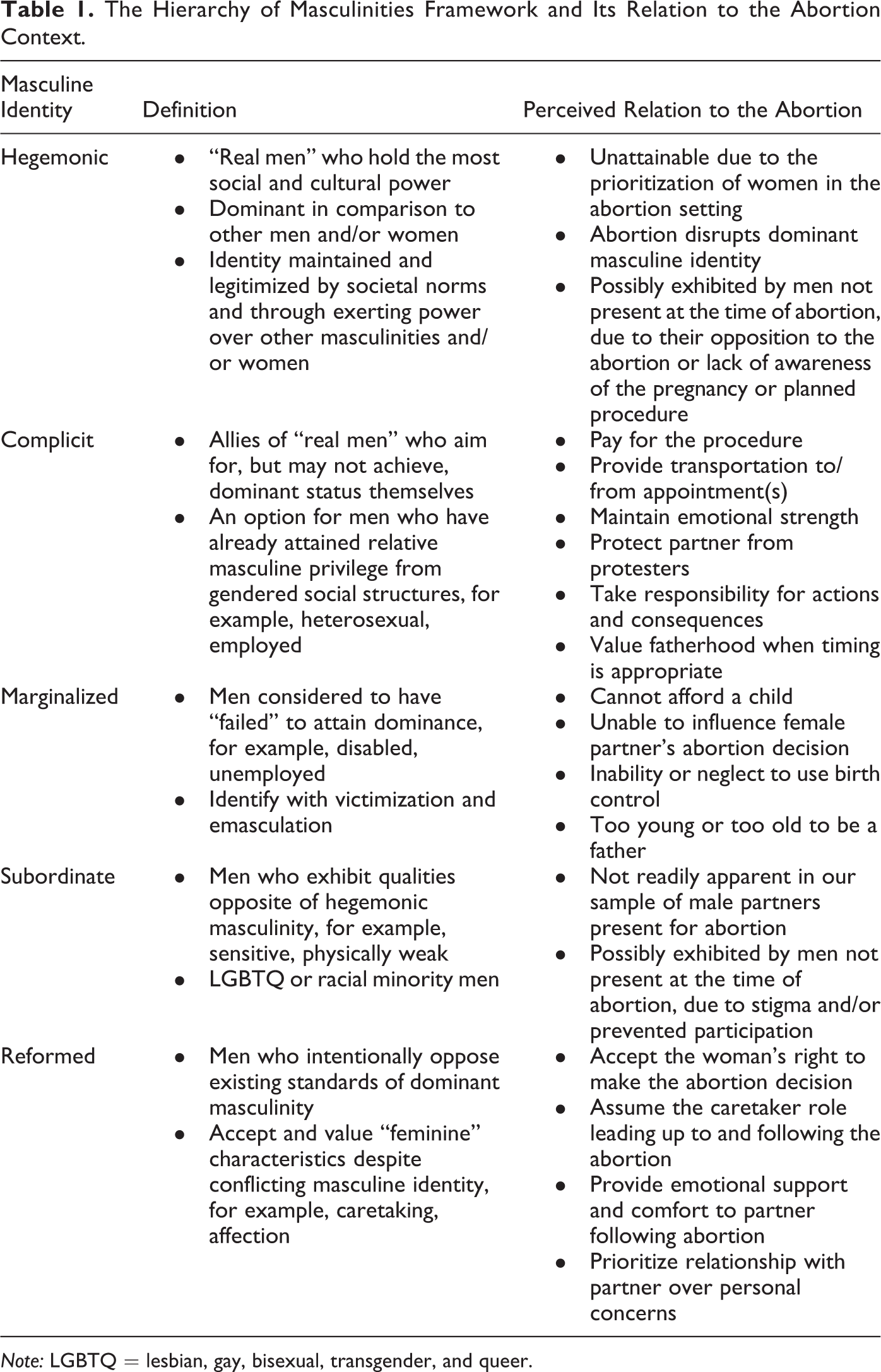
Note: LGBTQ = lesbian, gay, bisexual, transgender, and queer.
Method
Recruitment
We conducted in-depth interviews between April and August 2015 with male partners of women obtaining abortions at a community-based and a university-based abortion clinic in a metropolitan, Midwestern US city. We approached all abortion patients and asked each woman whether she would allow her male partner to be approached for research if he was on-site. Male partners were contacted once women gave consent for their inclusion. Male partners, defined as men who were recognized by women to be involved in the pregnancy, were eligible if: (1) they were at least eighteen years of age, (2) English-speaking, and (3) if the abortion was not motivated by a fetal anomaly, maternal medical condition, or intimate partner violence/sexual abuse. We applied purposive sampling in order to achieve diversity in both age and race/ethnicity. The number of interviews was determined by thematic saturation. If an in-person interview was not possible, a telephone interview was offered within four weeks of the procedure. Male partners received a US$50 gift card following their interview.
In-depth Interviews
All interviews were conducted by an Asian American, male physician-researcher in his thirties. Interviews were conducted in-person in a private room at each facility or via telephone. Immediately prior to the interview, all research participants completed a brief survey of their demographic, socioeconomic, sexual relationship, and reproductive characteristics. In-depth interviews followed a semi-structured guide. The interview guide consisted of open-ended questions that covered the male partner’s chronologic experience and expectations for involvement throughout the abortion, starting with his learning of the pregnancy through the female partner’s receipt of the abortion and recovery. Specific questions included the man’s role in the decision to have an abortion, his involvement in care at the clinic, and his need for personal support. Interviews were audio-recorded and transcribed by an outside transcription company. Interviews lasted between twenty and seventy-five minutes. At the end of the interview, all men were offered contact information for a free, national, All-Options pregnancy support talkline with experience in providing abortion-related counseling.
Data Analysis
After reviewing interview transcripts and memos, we developed a codebook that included both deductive codes (those based on the interview guide) and inductive codes (those emerging directly from the data). All transcripts were independently coded by two members of the research team using Atlas.ti version 7.5.10 (1993–2017). Interrater reliability coefficients identified systematic differences in coding and the need for arbitration. Disagreements were resolved through discussion and the judgment of a third coder. All codes were consolidated and categorized into matrices. Emergent themes were analyzed using a thematic content approach (Green and Thorogood 2013), and additional memos were drafted to summarize patterns across themes. All memos, matrices, and elicited themes were set against Connell’s hierarchy of masculinities framework (Table 1) to draw associations between men’s narratives and each configuration of masculine identity (hegemonic, complicit, and marginalized, with the addition of reformed masculinities) as previously described. We excluded “subordinate” masculinities that did not explicitly apply to our sample or emerge from the discussions.
Results
We completed twenty-seven interviews with male partners who were present at the time of their female partner’s abortion between April and August 2015. The average age of interviewed male partners was twenty-eight years old. Many of the men (eleven of the twenty-seven, 40 percent) identified as non-Hispanic black; eight men were non-Hispanic white, three men were Hispanic/Latino, and the remainder identified as “other race/ethnicity.” Illustrative quotes from their interviews are arranged in the following section according to an evolved hierarchy of masculinities framework.
Hegemonic Masculinity
Interviewed male partners struggled with their prioritization of two opposing hegemonic ideals juxtaposed at the time of abortion—manhood and fatherhood. Fatherhood is a highly desired end goal within hegemonic masculinity; additionally, being a breadwinner and establishing oneself within one’s community or society are central to “being a man.” Abortion stands in direct opposition to men’s opportunity and/or ability to fulfill these roles. One male partner described the pressures to achieve fatherhood against his inability to be in a stable relationship with his female partner and provide for a future family, resulting in discordant views surrounding the decision to have the abortion up to the time of the procedure: I don’t have any kids, and I wasn’t ready for kids. I practically always wanted to be married and established before I had any kids, which that’s not the case. My first thought and option was to get an abortion, but I did change my mind at the last minute. She went on with it. It bothered me…At the end, I didn’t want her to even have [the abortion]. (thirty-seven years, other race, abortion undesired) When we got there, I spent most of the time trying to convince her not to have it…after checking in at the front desk we had a seat, sitting next to each other. I leaned over towards her. I was being quiet so I wouldn’t be heard by the other guests. I was trying to convince her not to have the abortion. (thirty-seven years, other race, abortion undesired) For her to take [decision-making] power from away from me, or to take any power away from me, made the balance uneven…That’s where the problem came from, especially when it’s a monumental decision like this…for her to tilt the scales of power so drastically in her favor…It was just a telling sign and it’s something we’re very careful to avoid since, when it comes to our relationship. (twenty-four years, white, abortion desired)
Complicit Masculinity
The majority of interviews were with men whose narratives were congruent with complicit masculinities. While they could not attain their desired status, these men could remain “complicit” with ideals of hegemonic masculinity and negotiate an acceptable identity, adopting behaviors that still distanced themselves from their female partners as well as from other men whom they perceived as less masculine. A hallmark of hegemonic masculinity is competition and the comparison of oneself not only to women but also to other men. This was noted during an interview with a twenty-seven-year-old African American male who did not want his partner to have an abortion and wondered aloud about other men in the waiting room. He asked, “Are these guys the fathers of these kids? Why wouldn’t they want to keep them?”
For some men, being actively involved and engaged in the abortion experience was a point of pride that separated them from a stereotype of young men who avoid their roles in pregnancy and reproduction: A lot of young men aren’t mature about situations like these. They don’t know that it’s important for them and it would mean a lot for them to be there…I was there from beginning to end. That’s just how I am. A lot of guys, they’re not like that. They’ll make excuses or they don’t want to be around or they try to skip out on paying for the abortion. (twenty-four years, African American, abortion indifferent) I just knew that, “OK, you just give me the price, I will take care of it.”…Like I said, I had to be logical with it and reason with myself. She doesn’t have a job, she doesn’t want to go around, she doesn’t want to talk to her father—because he’s not really the type she can go and talk to—she don’t ask him for anything, she doesn’t want to tell her mama or anything, so I just be the man. She’s my girl; she’s going to be my wife one day. I just took that man role. “I’ll just take care of it. Don’t worry about it.” (thirty-two years, African American, abortion undesired) I didn’t want her to think I was having second thoughts or uncomfortable or doubting the decision or anything like that…I felt I couldn’t show anything but strength to her. I didn’t want her to think I was scared or uncomfortable or anything like that…I just simply wanted her to know that I was confident and strong for her, so that if she needed somebody in turn to I could be that for her. (twenty-four years, white, abortion desired) Personally, I think that some guys, you have to know as a man that if something like this happens and you do it then you have to be responsible for it. You can’t leave someone in the dust. (twenty-three years, Hispanic, abortion desired) I come from a family where my dad had to work for everything he had. It felt like I couldn’t let him down and all his hard work he put in for me and my two siblings for school. For me to just do something irresponsible and basically put us in a tougher financial hole, I couldn’t do that to him…Even though I was irresponsible, I was responsible enough to fix it. I guess I don’t know. I just don’t want to let them down. (twenty-two years, white, abortion undesired)
One man expressed this desire to delay fatherhood until he was prepared to assume the role of head of his household. When he first learned about his partner’s pregnancy, he immediately thought about whether the child would bear his resemblance, how “creating something” was powerful and how having a child would be an opportunity for him to assume the role of a father figure. Despite this opportunity, however, this man was in agreement with his female partner’s decision to have the abortion so that he could better prepare himself and become more like his partner’s father, and thus gain her respect: When I talk to her about it, she looks up to her dad a lot. She brags about how she loves that her dad was always there for her family. I feel that’s the kind of person she’s looking for, and so I want to take on that role and do whatever I need to do for her. (twenty-three years, Hispanic, abortion desired) I want my child to know their actual father is there for them through their entire life, whether they wanted to be there or not…Just because I feel like if I have a child, like I’m going to do anything to make sure that it is OK and happy and living a healthy good life…(nineteen years, white, abortion desired)
Marginalized Masculinity
Marginalized masculinity was exemplified by male partners who, because of their internalization of hegemonic standards of masculinity, were isolated from other men given their perceived inability to enact their gender. Whether due to age, socioeconomic status, or relationship quality, these interviews exhibited themes of weakness (physical, emotional, and/or financial), emasculation, and victimization. A fundamental loss of power due to an inability to support a pregnancy or influence his partner’s decision compromised these men’s ability to “be a man.” Unlike men who accepted a complicit status, these men’s discomfort with their marginalized position was evident when speaking about the hegemonic traits they desired but could not have. As one man said, he felt marginalized financially: If I had at least more money, if I was actually financially ready, yes, I would have went totally against it. “No, no we are just going to have it,” straight and forward, but I’m not actually financially staged for it. It was out of the question. (eighteen years, Hispanic, abortion undesired) Her and her doctor came up with these odds, and I was presented the facts. Basically, they made that decision, I just had to agree. Wasn’t really much I could say or do about it, right, without looking like a monster. (thirty-seven years, other race, abortion indifferent) Me as a man, I feel like I could have been more forceful in the situation, and stood my ground, and said, “No. This is what we gonna do. If we’ve got to struggle, I’m going to get up out of here and do what’s necessary for us to raise this child.” But I didn’t, so that kicked me in my ass. (twenty-four years, African American, abortion undesired)
Reformed Masculinity
Not all men identified with the drive to become fathers and to maintain dominance over others, as dictated by hegemonic masculinity and appraised by complicit and marginalized masculinities. Some men instead reevaluated their perceptions of what might be ideal masculine qualities in the abortion context, adopting a “reformed masculinity.” Male partners who identified with reformed traits described their abortion experiences deferentially, ceding power in decision-making and reconsidering the drive for dominance in a setting focused on a woman’s experience. Thus, accepting their lesser status, although in opposition to hegemonic values, elevated the value of providing social support to their female partner.
Male partners who prioritized providing emotional support described how this aspect of reformed masculinity defined their role in their partner’s decision to have an abortion. A twenty-four-year-old African American man summarized his discussion with his partner: “Whatever you agree upon, I agree with you.” Reformed identities and behaviors were also evident among male partners who described pregnancy as physical—appraising how women carry and deliver pregnancies. Therefore, to consider their own emotional needs would be “selfish,” leading these men to settle into their role as a “team player” and a “supporter” in both the emotional and physical aspects of the abortion process: It’s really hard. Like I said, there’s nothing you can do unless you just put yourself in her shoes. (thirty-two years, African American, abortion undesired) The role of the man should be, no matter how he feels about it, no matter if he’s broke, don’t care what the situation is, the role of the man is supposed to be behind the woman 100 percent in the decision, whether she wants the child or not. (twenty-one years, African American, abortion indifferent)
By accompanying the patient to the appointment, some male partners were able to provide support as well as comfort and encourage their partners during what they perceived to be a stressful time, even if they themselves did not fully understand or participate in the procedure. As one man explained: I think she needed somebody to be able to be there for her to get home, which I didn’t know, all I knew was that she wanted me to be here, because she said that I needed to be here and that I needed to get up here. So that’s just what I did, I didn’t ask any questions, I just said, “OK give me some time and I will be up there as fast as I can.” (nineteen years, white, abortion desired) I financed the whole [abortion procedure], even though I didn’t care about the money aspect. I definitely showed her that I loved her and that it all wasn’t in vain. And that we obviously would stay together forever. And that this wasn’t just “let’s do this and then let me get rid of you” kind of thing. I obviously love the girl with all my heart. I’m not going to bail…(twenty-two years, white, abortion undesired)
Discussion
This study describes the range of masculinities that emerge among male partners in the abortion context. Power is central to these competing masculinities, and its perceived importance may influence how men negotiate their masculine identity. The abortion experience confronts men’s power in multiple ways—from the inability to provide for a child, which may contribute to women’s decision to have an abortion, to being relegated to the clinic waiting room. With their ability to fulfill a hegemonic ideal and “be a man” compromised, some men may feel marginalized or have to negotiate a complicit masculinity. Yet for others, the restructuring of power in the abortion context reveals a reformed masculinity predicated on partnership and the provision of support. The emergence of these masculinities in settings where men’s gendered status has shifted is consistent with observations in other reproductive health contexts including pregnancy confirmation (Draper 2002), attendance during childbirth (Dolan and Coe 2011), and in the treatment of erectile dysfunction and male infertility (Inhorn and Wentzell 2011).
Hegemonic ideals of manhood were prominent throughout our interviews, with male partners articulating a need to be seen as responsible, financially able, and emotionally strong potential fathers. Unable to assume or reprise the role of an ideal father, these men negotiated their identity in order to maintain prominence within the abortion context; nearly all of the interviewed men did so by expressing a desire to provide support to his female partner. While partner support may seem inconsistent with hegemonic masculine ideals, certain support narratives correspond well with complicit masculinities when they underscored men’s position and power as financial providers, gatekeepers, and heads of households who needed to facilitate or support his partner’s abortion. For some men, this negotiation took the form of paying for the procedure, driving her to the appointment, and organizing aftercare.
Where power or privilege compared to his female partner was not emphasized, some male partners maintained complicit masculinity by embracing a “growth” narrative that pressured them to become strong, unemotional, and worthy of the respect of others. In this way, these male partners distinguished themselves from “lesser” men who were not present at the clinic and whom they perceived not to be “real men” who took responsibility for their actions.
Not all men were able to negotiate their hegemonic expectations with their role in the abortion setting and thus articulated marginalized masculinity. These men reflected on their abortion experience with confusion, anger, disappointment, and regret, particularly when their partners had greater power in decision-making and the logistics of the abortion process. By failing to negotiate their masculine identity in the abortion experience, these men remained marginalized in the hierarchy of “real men.”
Whereas previous explorations of men’s abortion experiences described sentiments of loss, grief, helplessness, and victimization (Coyle and Rue 2015), our interviews with male partners at the time of an abortion provide a broader perspective, recognizing the willingness of some male partners to cede decision-making power to women and find value in the provision of support. Their reformed masculinity accepted traditionally feminine characteristics such as caretaking and affection. These men also described a desire to prioritize their relationship with their partner over personal concerns.
Our study has a number of limitations. First, an in-depth investigation into masculinity was not a primary aim of this study but rather one that emerged from the data. Further, the findings from this study cannot be extended to all male partners of abortion patients. Our sample included only those men who accompanied their female partner, which may represent support for the partner and a desire or ability to be present at the clinic. We excluded partners who were not present and the partners for whom women did not give consent for an interview. These men may have had different views about their role in the pregnancy, abortion, and relationship with the female patient. They may have also exhibited different narratives of masculinity than those explored here.
Implications
Restrictive policies that exclude men from the clinical components of abortion exist and are enforced to protect legal precedent for women’s autonomy at the time of abortion (US District Court 1993; U S Supreme Court 1976). Although some abortion scholars suggested clinic policy and structure reforms to include male partners more than three decades ago (Shostak and McLouth 1984), considering these services is no less controversial today. The political and social climate that continues to restrict women’s access to abortion validates abortion providers’ and advocates’ fears that involving male partners would compromise the safety and reproductive autonomy of female patients. While men should never be the first priority at the time of an abortion, opportunities may be developed to alleviate isolation and oppositions held by male partners who may be experiencing an unfamiliar interaction with abortion procedures and processes that can challenge their masculinity. In addition, neglecting the men who present in the abortion setting may inadvertently overlook potential allies who, through their own experience with abortion, become greater advocates and supporters for women’s health.
The decision to terminate a pregnancy and the time spent at the abortion clinic with his partner may lead a man to consider his role in conceiving a pregnancy and its ramifications on their relationship, both topics about which men are often reticent to discuss without prompting by professionals (Same et al. 2014). However, clinicians and educators have limited prior opportunities to introduce abortion education and awareness to men who seek sexual and reproductive health care most often for sexually transmitted infection and pregnancy preventative services (Same et al. 2014). These clinical encounters could be a first resource to address men’s internalized masculine expectations about their involvement in women’s reproductive health care (Draper 2002), particularly with regard to changing gender norms and sexual behaviors (Seal and Ehrhardt 2003), and thus better equip men to understand their identity and role during a possible unintended pregnancy and abortion.
Implementing further gender-informed health care at an abortion appointment, if the male partner attends, could present another point of contact to address the influence of masculinity, including discussing health concerns in the context of the sexual relationship with their female partner (e.g., contraception use and responsibility; Fennell 2011; Schofield et al. 2000). Including male partners in the abortion visit is not without precedent; male involvement has been positively associated with women’s well-being and their assessment of their abortion experience (Altshuler et al. 2016; Kimport, Foster, and Weitz 2011). Previous interventions have shown the favorability of couples counseling at an abortion appointment (Becker, Bazant, and Meyers 2008), suggesting an acceptable way to mitigate the uneven division of abortion-related emotional labor, a burden primarily shouldered by women (Kimport, Foster, and Weitz 2011).
Furthermore, by considering the perspectives of male partners, there is the opportunity to explore how the abortion experience may support, challenge, and/or reconstruct definitions of masculinity; considering how these variations in masculinities shape men’s beliefs and behaviors in the abortion setting may ultimately help to guide men to provide aftercare for their partners (Altshuler et al. 2016). While patient-centered care rightfully supports the primacy of women in the abortion setting, abortion-providing facilities may want to consider fostering men to be allies and caretaking partners for patients. Clinicians and staff caring for women at the time of abortion may want to be sensitive to how masculinity is internalized and performed by male partners and how gender role conflict influences women’s abortion experience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: During the conduct of this research, Dr. Nguyen served on the medical advisory board of the Female Health Company, the products and services of which are unrelated to this research. None of the other authors have a conflict of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the Fellowship in Family Planning Research Fund.