
Abstract
Discrete-trial functional analysis (DTFA) is an experimental method for determining the variables maintaining problem behavior in the context of natural routines. Functional communication training (FCT) is an effective method for replacing problem behavior, once identified, with a functionally equivalent response. We implemented these procedures in the natural environment for three individuals with developmental disabilities who resided in a residential treatment facility. Study 1 results show that the DTFA procedures experimentally validated the function of each participant’s problem behavior after completing a functional assessment using informal and descriptive methods. Study 2 results reveal that FCT was successful at replacing problem behavior with an alternative communication behavior that served the same function. A unique feature of this study was the use of behavioral indication (i.e., observable behavior signaling momentary motivation) as a cue for determining when to deliver the FCT intervention.
Keywords
Problem behavior may be the biggest barrier to social and community inclusion (Reichle, 1990). Effective approaches that reduce problem behavior while increasing socially acceptable means of communication can offer an individual better choices and opportunities that promote normalization, potentially leading to an improved quality of life for the individual and related care providers (Carr et al., 2002). One specific communication method that has proven fruitful for achieving this goal is functional communication training (FCT; Carr et al., 1994). FCT replaces problem behavior with socially acceptable behavior that serves the same function (Carr & Durand, 1985). This procedure begins with an assessment to determine the function of problem behavior, followed by the instruction of a new functionally equivalent communication form. For FCT to be successful, the assessment procedures must produce accurate and valid information about the function of the behavior, and instruction must replace problem behavior with a new functionally equivalent behavior.
The first step of FCT is to conduct a functional assessment, which often consists of interviews, ratings scales, and observations to develop hypotheses about factors that reliably predict and maintain problem behavior (O’Neill et al., 1997). In situations where these assessment procedures do not produce a clear hypothesis about the function of problem behavior, a functional analysis (FA) may be warranted. An FA consists of the systematic and experimental manipulation of antecedent and consequent factors to determine the relationship between environmental events and the probability of problem behavior (Iwata, Dorsey, Slifer, & Bauman, 1994). For decades, this procedure has been considered the gold standard for determining the function of problem behavior regardless of the individual’s disability (Hanley, Iwata, & McCord, 2003; Iwata, Pace, et al., 1994).
Despite the methodological rigor of a traditional FA, it has several potential shortcomings. First, analogue FAs may not accurately identify the function of behavior because the conditions in contrived settings could differ in small, but important, ways from those in the natural environment (Tiger, Fisher, Toussaint, & Kodak, 2009). Second, it is common to reinforce the occurrence of problem behavior on a continuous schedule of reinforcement (CRF) during an FA. A CRF may differ from the schedule operating in the natural environment and, thus, may inadvertently lead to the acquisition of problem behavior (Van Camp, Lerman, & Kelley, 2001). Third, standard FAs often require additional training and resources and can be time-consuming, negating its feasibility in many applied settings (LaRue et al., 2010).
Because of these limitations, researchers have sought alternative methods of conducting FAs (Derby et al., 1992; Northup, Wacker, Sasso, & Steege, 1991), particularly those that can be easily implemented in natural settings (Wallace & Knights, 2003). One experimental procedure that has the potential to address some of the limitations of traditional, analogue FA is discrete-trial functional analysis (DTFA, Sigafoos & Saggers, 1995). With a DTFA, antecedents and consequences are systematically manipulated just as they are in a traditional FA, but trials are embedded throughout the day in participants’ natural routines. The results of the embedded trials for each condition are then summed and the percentage of times that the individual engaged in problem behavior across trials within each condition is calculated. DTFA procedures involve less training, less time, and fewer resources than typical FA procedures, but still permit an assessment of the function of problem behavior in everyday settings in systematically and methodologically rigorous ways. As a result, caregivers can more easily participate in the assessment process and DTFA procedures may increase ecological validity.
Recent research has compared traditional FA procedures with DTFA methods (also known as trial-based FA) to assess the validity of this new procedure. So far, results of these studies have been promising (Bloom, Iwata, Fritz, Roscoe, & Carreau, 2011; LaRue et al., 2010). However, Bloom et al. (2011) used therapists who were unfamiliar to the participants to increase procedural integrity. The use of unfamiliar care providers might have led to results that did not accurately capture an individual’s motivation with the care providers whom they are most likely to encounter on a daily basis (English & Anderson, 2004; Huete & Kurtz, 2010; Ringdahl & Sellers, 2000). LaRue et al. (2010) found that classroom teachers who used DTFA identified the function of problem behavior for four of five participants in far less time than is typically required for traditional FAs. Although both of these studies evaluated DTFA, neither included nor evaluated a corresponding intervention.
After the function of the problem behavior has been identified, the next step in FCT is to teach a replacement communication behavior. Instruction usually consists of prompting and reinforcing the replacement behavior on a dense schedule of reinforcement while placing problem behavior on extinction. A critical aspect of instruction is timing to ensure that the replacement behavior is acquired under the same stimulus conditions as those that evoked the functionally equivalent problem behavior. One way to time instruction is to capitalize on an individual’s behavioral indication of deprivation to signify the presence of stimulus conditions that reflect the motivation for reinforcement. Behavioral indication consists of subtle, observable behaviors that occur immediately prior to problem behavior and indicate momentary states of motivation (Drasgow, Halle, Ostrosky, & Harbers, 1996). Delivering instruction when motivation is prepotent may facilitate the transfer of internal stimulus control of the problem behavior to the replacement behavior (Drasgow, Halle, & Sigafoos, 1999). Moreover, behavioral indication of satiation can be used to identify times when instruction should be discontinued or withheld (Lang et al., 2010). Although a FA may be essential to developing FCT interventions, current FA methodologies may not be a practical method in naturalistic contexts (Carr et al., 1999). Developing FA methodologies that are practitioner-friendly represents an important contribution to the field because of their potential to improve the lives of individuals with disabilities who have problem behavior.
The purpose of our study was to examine DTFA and the corresponding FCT intervention procedures resulting from the DTFA that were implemented in natural classroom routines to enhance the communication repertoire of three individuals with autism and other developmental disabilities. In Study 1, we sought to assess the utility of DTFA procedures for determining the function of problem behavior by embedding trials in each participant’s natural routines. In Study 2, we implemented FCT based on the DTFA results from Study 1 in an effort to decrease rates of problem behavior by teaching participants more efficient, socially acceptable forms of communication when they were highly motivated.
Method
Participants and Setting
Three students were nominated for the study by a team of facility administrators because prior attempts to determine the function of their problem behavior or to teach them alternative communication strategies were unsuccessful. A review of each participant’s records revealed that various behavioral interventions had been implemented with all of them in an attempt to decrease their rates of problem behavior. Examples of interventions reported to have been used with participants included extinction, differential reinforcement of other and alternative behavior (e.g., token economy system or FCT), timeout, restraint, and medication. These procedures were part of each participant’s comprehensive behavior plan. However, we could not verify the accuracy or fidelity of intervention implementation for any of the participants.
Ivan was a 9-year-old, nonverbal, Caucasian male diagnosed with autism and profound intellectual disability. His problem behavior included throwing objects, aggression, and pica. Staff reported that in the past they had used prompting and reinforcement strategies in an attempt to implement FCT with Ivan. They had selected a gestural modality of communication. Data indicated that he had not acquired the targeted replacement communication behavior despite extensive instruction.
Thomas was a 10-year-old, nonverbal, Caucasian male diagnosed with autism and profound intellectual disability. He followed a few one-step commands and required physical prompts to complete daily living tasks. Thomas’s problem behavior included aggression, self-injurious behavior (SIB), elopement, fecal smearing, pica, and property destruction. Records showed that physicians were concerned that Thomas’s consistent and forceful head slapping placed him in danger of detaching his retinas. Staff reported that in the past they had used prompting and reinforcement strategies in an attempt to teach both verbal and gestural modalities of communication. Despite extensive instruction, data indicated that Thomas had not acquired the targeted communication behaviors.
Billy was a 15-year-old Caucasian male diagnosed with autism, severe intellectual disability, depressive disorder–not otherwise specified, and psychotic disorder–not otherwise specified. Although he had a verbal vocabulary of more than 100 words, most of his communication was nonfunctional and consisted of delayed echolalia. Specifically, many of his statements involved cursing, racial slurs, or sexual statements. His problem behavior included aggression, inappropriate touching of others’ genitals, and cursing or sexual statements. Staff reported that in the past they had attempted to implement FCT with Billy. Their protocols emphasized using prompting and reinforcement to teach him to communicate by using a verbal modality or picture communication cards. Data indicated that Billy had not yet acquired the targeted communication behaviors.
The studies were conducted at a southeastern U.S. residential treatment facility that served more than 30 students, ages 7 to 21, with developmental disabilities and a history of challenging behavior. Only the school building was used as a setting for these two studies, except for generalization trials, when multiple other areas were included. The school consisted of eight classrooms with four students and one behavior staff member (BSM) assigned to each room. BSMs, who were required to have at least a high school education, managed the day-to-day activities and behavior problems of the students. They were informed about the purposes of the study, the specific children from their classes who would be participating, and that their participation in the study was voluntary; all BSMs agreed to participate.
Study 1: Functional Assessment and Analysis
The purpose of this study was to identify the functions of the problem behavior for each participant. The assessment began with a review of the documentation of each of the participant’s prior psychological evaluations, intake records, and behavioral data that had been collected regarding his or her most frequent, severe, and challenging behaviors. We completed the Functional Analysis Screening Tool (Iwata & DeLeon, 2005) and the Motivation Assessment Scale (Durand & Crimmins, 1988) with the BSMs. We also conducted approximately 5 hr of direct observation for each participant across multiple settings (i.e., classroom, lunchroom, and playground) using the A-B-C method (Bijou, Peterson, & Ault, 1968). Data from these observations were used to identify participant’s problem behaviors and to refine or revise hypotheses about the environmental stimuli maintaining problem behavior to design the DTFA conditions.
Procedures
DTFA
Sessions were conducted in each participant’s classroom with his peers and staff members present. We matched the protocol for the DTFA as closely as possible to the methods and routines used by BSMs with the participants in the natural environment by creating a schedule to approximate the times participants were typically exposed to snacks, deprived of attention, given academic tasks, or allowed to have free time with access to reinforcers. All participants had one session under each relevant condition in the morning (9:00 a.m.–11:45 a.m.) and one session in the afternoon (1:00 p.m.–3:05 p.m.). This method was used to avoid the massed trial, analogue format that is typical of a standard FA. Sessions were separated by at least 30 min and were videotaped.
Prior to conducting the DTFA, BSMs were trained to implement protocol procedures using modeling and role-playing with performance feedback. Criterion consisted of 100% implementation fidelity for five consecutive role-play sessions. BSMs or the first author were randomly assigned to complete an equal number of DTFA sessions. From here on, the term therapist will refer to either BSMs or the first author.
Initially, 10 DTFA sessions, each consisting of an assessment and reinforcement trial, were conducted for each participant in the specific conditions where a hypothesized function had been developed from the prior data collection. The assessment trial consisted of specific antecedent conditions being arranged and ended contingent upon problem behavior, a communication response, or time expiring (duration varied based on participant). At the end of the assessment trial, the reinforcer trial began. The reinforcer trial consisted of the consequence (i.e., attention, food, or removal of the task) being presented continuously for 1 to 3 min, depending on the function being assessed. The reinforcer trials served as a control condition for that specific context and time, to enhance the probability that the prior problem behavior occurred specifically for the reinforcer that was now available. Condition procedures are described below.
Tangible-edible
The assessment trial started when the therapist placed a small amount of food on the table in sight but out of the participant’s reach for up to 1 min. Assessment trials were 1 min in duration because staff members reported that this was how long food would typically be in the environment before it was delivered. If during this trial (a) the participant engaged in problem behavior, (b) the participant engaged in an acceptable communicative behavior (e.g., “food please”), or (c) time expired (1 min), the reinforcer trial began. During the reinforcer trial, the therapist ignored all instances of problem behavior and continued to provide noncontingent access to food for 1 min.
Attention
The assessment trial (up to 3 min) started when the therapist began looking at a magazine or completing written work. Assessment trials were 3 min because it was hypothesized to be an appropriate amount of time for creating a state of deprivation, based on staff members’ reports of how long students would be required to go without any attention in the classroom. If during this trial (a) the participant engaged in problem behavior, (b) the participant engaged in a communicative behavior (e.g., “talk to me”), or (c) time expired, the reinforcer trial began. During the reinforcer trial, the therapist provided physical (e.g., pat on the back) and verbal attention (e.g., “I really like your shirt”) for 1 min, and ignored all problem behavior.
Escape
The assessment trial (up to 3 min) began when the therapist placed an academic task in front of the participant and instructed him to do his work (e.g., put the clothespins in the basket or choose a specific picture from a group of pictures). Assessment trials were 3 min because staff members reported this to be the average amount of time that Ivan would be required to work on a task if he was consistently prompted by his BSMs. If during this trial (a) the participant engaged in problem behavior, (b) the participant engaged in a communicative behavior directly related to the reinforcer (“break”), or (c) time expired, the therapist immediately said “We are finished” and removed all academic materials; this started the reinforcer period. During the reinforcer trial, the therapist read a magazine or completed written work and ignored all problem behavior; no demands were presented during this time.
Control
The assessment and reinforcer trials of the control condition were both 1 min in duration. For both trials, the therapist provided the participant with noncontingent access to hypothesized reinforcers that were being evaluated for maintaining problem behavior. This condition was an exact replication of the procedures that we used in the reinforcer trials during other DTFA conditions.
Response measurement
For each DTFA trial (assessment and reinforcer), behavior was coded as (a) problem behavior, (b) communicative response, or (c) neither a nor b. Only the first targeted behavior observed during each assessment and reinforcer trial was recorded because of the severity of each participant’s problem behavior. At the conclusion of the DTFA, the number of trials with problem behavior was summed, divided by the total number of trials for a condition, and multiplied by 100. Only problem behavior was graphed for the purposes of the DTFA.
Ivan’s problem behaviors included food stealing (taking a food item that is in sight and out of reach but has not been given to him), disruption (throwing or pushing away objects and turning away from the therapist, or repeatedly stomping feet on the ground), and aggression (forceful hitting, kicking, pushing, and pinching or throwing objects at others). Thomas’ problem behaviors included self-injury (forceful striking, rubbing, poking, or banging of head, or biting himself), food stealing (taking a food item that is in sight and out of reach but has not been given to him), and aggression (forceful hitting, kicking, pushing, pinching, or throwing objects at others). Billy’s problem behaviors included cursing/sexual statements with or without physical behavior (grabbing groin, butt, or chest) and aggression (forceful hitting, kicking, pushing, and grabbing or bumping into another person).
Interobserver agreement
Trained undergraduate and graduate students in the psychology and education departments collected reliability data independently of the primary observer. Reliability was conducted on 30% of sessions for each relevant condition that was assessed for each participant. Sessions consisted of assessment and reinforcer trials. Each trial was scored as an agreement or disagreement for the occurrence of problem behavior, communication form, or expiration of time. Then the total number of agreements was divided by the total number of agreements plus disagreements and multiplied by 100. Reliability for all topographies of each participant’s behavior for assessment and reinforcer trials across all conditions was 100%.
Results
Figure 1 displays the percentage of assessment and reinforcer trials during which each participant emitted problem behavior in each condition. Ivan stole the tangible-edible (food) during 100% of the assessment trials but only engaged in problem behavior during 10% of the reinforcer trials where he had unrestricted access to the edible. In the escape condition, Ivan displayed problem behavior more frequently during the assessment trials (60%) when academic demands were placed on him than during the reinforcer trials (20%) when academic demands were removed.
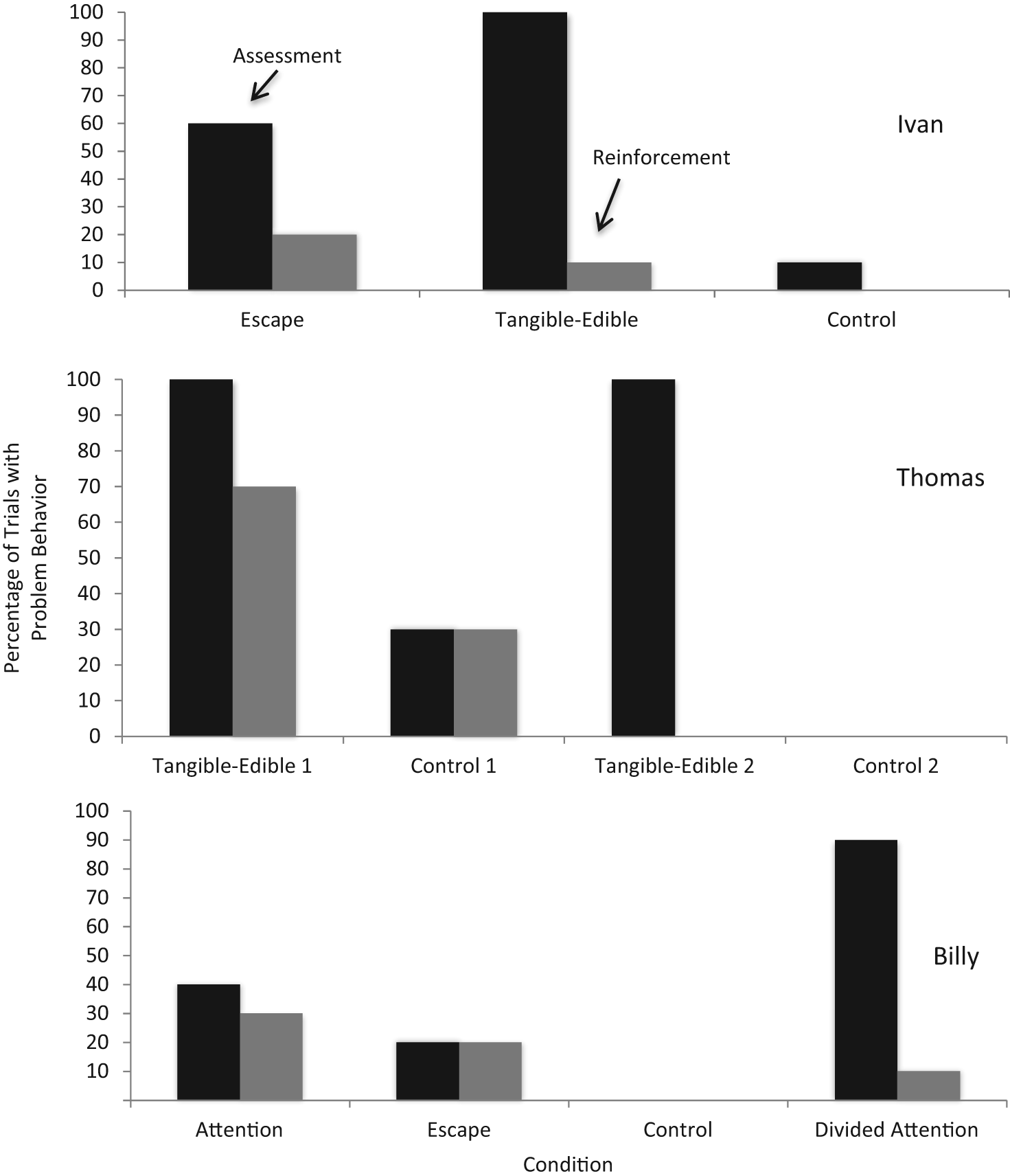
Distribution of function across DTFA trials for Ivan, Thomas, and Billy.
During the first set of tangible-edible assessment trials (i.e., tangible-edible 1), Thomas’ primary form of problem behavior was food stealing (90%). However, he also displayed high rates of SIB, specifically head slapping, during trials where he had access to food (70%) approximately 5 to 10 s after beginning to consume his edible. In addition, Thomas engaged in head slapping during the assessment and reinforcer trials in the control condition (30% each) even though he was given noncontingent access to the reinforcer. Because Thomas’ data were not clearly differentiated, 10 additional tangible-edible and control condition sessions (i.e., tangible-edible 2 and control 2, respectively) were conducted with him wearing a helmet to assess whether he was engaging in problem behavior as a form of sensory reinforcement. During these sessions, he did not emit SIB during any of the reinforcement trials of the tangible-edible 2 conditions nor any problem behavior during the control 2 trials. To comply with the facility’s policy, the staff used the helmet with Thomas as they deemed necessary. No further sessions were conducted to evaluate if head slapping was maintained by automatic reinforcement.
The initial DTFA analysis revealed undifferentiated results for Billy in the attention (40% on assessment and 30% on reinforcer trials) and escape conditions (20% on both assessment and reinforcer trials). A review of the DTFA videos revealed that Billy engaged in problem behavior during escape sessions only when he was not receiving physical and verbal attention. Based on these observations, we revised the protocol to assess whether Billy engaged in problem behavior (to obtain attention) within 20 s of an adult entering the room and beginning a conversation with the therapist while Billy was sitting at a table by himself with access to leisure items (i.e., a divided attention condition). Results from a second set of DTFA trials confirmed this hypothesis: Billy was more likely to engage in problem behavior during the assessment trials (90%) than during the reinforcement trials (10%).
Study 2: FCT
The purpose of the FCT study was to teach each participant a new communication form that served the same function as his problem behavior.
Response Definitions
Table 1 presents each participant’s problem behaviors, functions identified by DTFA, communication responses selected for FCT, and number of days to criterion for each participant. Ivan’s target replacement communication responses were to sign “eat” (raising open palm of hand with fingers fully extended to mouth, with at least one finger covering mouth) and to sign “break” (placing arms across chest with open hands touching the opposite shoulder). We reinforced this single topography for signing “eat” throughout the remainder of the study.
Target Problem Behaviors, Function, and Functional Communication Response for Each Participant.
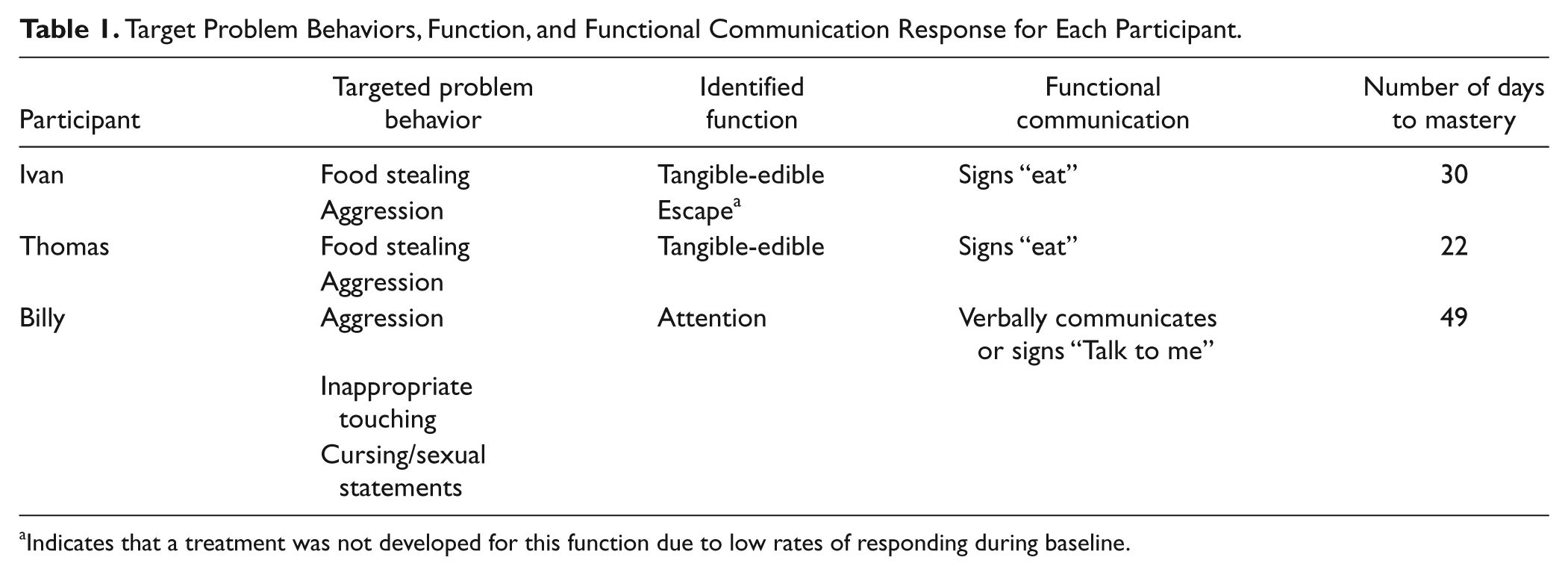
Indicates that a treatment was not developed for this function due to low rates of responding during baseline.
Thomas’ initial replacement communication response was to sign “eat” (raising open palm of hand with fingers fully extended to mouth, and at least one finger covering mouth). Beginning with Session 18, we changed his communication response because he was forcefully striking his chin while completing the aforementioned sign. The new response was to sign “eat” by having any portion of his right palm in contact with his left fist. Thomas’ communication form was altered again at Session 24 due to his failure to physically form the response; his new communication response was to tap both hands together in a fist formation in the center of his body. As the topography of a correct replacement response changed, so did the operational definition for recording purposes.
Billy’s initial replacement communication response was to communicate, “talk to me.” The operational definition of this behavior was Billy either (a) vocally said “talk to me,” (b) raised his hand toward head with fingers spread apart, and touched his chin with index his finger, or (c) did both (a) and (b). Due to inconsistency of responding, we changed his communication response at session 32 to be either (a) vocally said “talk to me,” “talk,” or a similar variation (b) placed one or both palms forward with palms facing upwards and elbows within 8 inches of his body or (c) did both (a) and (b). As the topography of a correct replacement response changed, so did the definition for recording purposes.
Response Measurement
Communicative responses and problem behavior were measured on a response-per-opportunity basis. Each time the antecedent condition was presented, it was considered a trial or an opportunity for the participant to respond with (a) a problem behavior, (b) therapist-prompted responses, (c) an independent emission of the replacement behaviors, or (d) no targeted response. Thus, during each intervention trial, a participant could be recorded as responding incorrectly by emitting problem behavior, by receiving a prompt from the therapist, or by not responding. Conversely, participants could respond correctly by emitting the replacement behavior independently.
Experimental Design
We used a multiple baseline design across three participants to assess the effects of FCT on participant responding. Phases consisted of baseline, FCT intervention, and maintenance.
Baseline
Baseline sessions consisted of 8 to 10 trials that were distributed throughout the day and embedded within the participant’s natural classroom routine. Trials for each participant were separated by at least 10 min, and no more than three trials occurred in 1 hr for any participant. We recorded the first target behavior and terminated the trial at that point because the participants were unlikely to emit the new communication form that had not yet been taught, and it would be unethical to allow their behavior to escalate to more severe forms in their response class.
Tangible-edible
The trial began when the therapist placed an edible on the table within sight of the participant but out of reach. The food remained in sight until the participant (a) engaged in a problem behavior, (b) signed “eat,” or (c) 1 min elapsed. If the participant emitted problem behavior or signed “eat,” food was provided. If time elapsed, the therapist removed the food from the participant’s sight.
Escape
The trial began when the therapist placed an academic task in front of the participant and delivered a prompt (e.g., put the clothespins in the basket or choose a specific item among the pictures). If the participant (a) engaged in problem behavior, (b) signed “break,” or (c) 3 min expired, the therapist immediately said “We are finished” and removed all academic materials, thus ending the trial.
Divided attention
The therapist began a conversation with another care provider. If the participant (a) engaged in problem behavior or (b) communicated (i.e., signed or spoke) “talk to me,” the therapist provided physical and verbal attention contingently for approximately 10 to 20 s. After attention was provided, the trial ended. However, if time expired (i.e., one min) before the participant engaged in either problem behavior or the replacement communication form, the trial ended and the therapist exited the room.
Intervention
For intervention trials, we recorded the first target behavior the participants emitted to prevent chaining of new forms of behavior to old forms. Data from each session (8–10 trials) were graphed as the percentage of trials in which problem behavior or the replacement behavior was emitted. If the participant’s data did not reveal an increasing trend or had high levels of variability when acquiring the replacement behavior, then the therapist used a massed-trial format (i.e., 10–15 trials run consecutively within 10 min) to foster acquisition.
Intervention protocol
During the intervention phase, the therapist was near the participant while a BSM continued with the scheduled activity. General procedures consisted of presenting the antecedent condition or the presumed motivating stimulus, issuing a prompt if necessary for the participant to perform the replacement behavior (i.e., model the sign for “eat” or say “talk to me”), and delivering a consequence based on the participant’s response.
During intervention sessions, the therapist conducted a variable number of trials (8–10) with each participant, based on the participant’s current motivation for the reinforcer (Drasgow et al., 1996; Lang et al., 2010). Motivation was identified by observing each participant’s behavioral indication or lack thereof (i.e., observable behaviors that reflect an internal state of deprivation or satiation, such as reaching for food or tugging at the therapist’s sleeve), and if they interacted with the reinforcer once contacting it (i.e., ate the food or interacted with the therapist). We used these behaviors or their absence to determine whether to continue with trials or to wait to conduct the trial at a later time. That is, the behavioral indication was used to determine when the next trial occurred.
To instruct participants in their new communication form, the therapist initially used a 0-s constant time delay physical prompting procedure with differential reinforcement depending on the participant’s response. The therapist prompted the new communication form in the presence of the presumed motivating stimulus and reinforced occurrences of the targeted replacement behavior on a fixed ratio (FR) 1 schedule (i.e., each response emitted received reinforcement). After three consecutive trials in which the participant performed the response with the prompt, the therapist inserted a 2-s delay. The purpose of this delay was to provide the participant the opportunity to produce the response independently in the presence of the natural discriminative stimulus (e.g., presence of food) and to transfer control of responding from the instructor to the natural cue (Halle, 1987). If the participant engaged in problem behavior, the reinforcer was removed, and approximately 15 s later, the therapist presented the antecedent, delivered a controlling prompt to ensure a correct response, and provided the reinforcer.
Maintenance
After a participant met the intervention criterion for mastery (i.e., at least 90% for three consecutive sessions) he entered the maintenance phase. During the maintenance phase, BSMs conducted one to two trials 3 times per week. Thus, during maintenance, a data point, which consisted of 10 combined trials, was accumulated approximately every 10 days.
Generalization
To assess if Ivan and Thomas spontaneously used the new communication form in different settings and with different care providers than those involved in training, the first author collected 10 additional data points by filming from an unobtrusive location (e.g., out of the participant’s sight) within 2 weeks after completing the FCT maintenance phase. To do this, the first author remained out of sight while setting up the video equipment, during the filming, and when leaving discreetly after completing filming to avoid any reactivity effects due to his presence. During generalization trials, the antecedent was present (e.g., food) within the participant’s normal routine but exclusive of the training setting; the participant’s behavior was recorded and the natural consequence was delivered (i.e., the participant was given the food contingent on use of the new form). Only BSMs who were not involved in intervention were used as therapists during the generalization sessions.
Social validity procedures
We administered a social validity questionnaire (available from the first author) at the completion of the study to the BSMs who participated. This form was given to them specifically because they worked with the participants on a daily basis and would be responsible for maintaining the replacement behavior at the termination of the study. The questionnaire focused on assessing the fit of the study procedures with their everyday routines and with their satisfaction with the outcomes.
Interobserver agreement
Reliability was conducted for 30% of the trials in each phase. For each trial, the scores of the independent observer (graduate or undergraduate student) and the therapist were compared. Each trial was scored as an agreement or disagreement for prompted or independent replacement form or for problem behavior. For each participant, response option, and phase, the total number of agreements was divided by the total number of agreements plus disagreements and that quotient was multiplied by 100. During baseline, agreement on trials for Ivan was 100% (13/13) for food stealing. During FCT, it was 100% (34/34) for prompted communication, 96% (51/53) for independent communication, and 100% (5/5) for nonoccurrence of target problem behaviors. During maintenance, it was 93% (14/15) for independent communication, and 86% for nonoccurrence of target problem behaviors (6/7). For Thomas, interobserver agreement (IOA) during baseline was 100% (26/26) for food stealing. During FCT, it was 93% (28/30) for prompted communication of Sign 1 and 100% for prompted communication of Sign 2 (42/42) and Sign 3 (30/30), respectively. IOA for communicating independently for Sign 1 was 80% (4/5), and for Sign 3 was 90% (50/55). Sign 2 was not evaluated due to its low rate of occurrence and the quick change in signs due to safety concerns (discussed above and below). During maintenance, it was 100% for independent communication (9/9) and the nonoccurrence of target problem behaviors (2/2). During generalization, reliability was calculated using the same methods described above. The IOA for generalization trials was 100% (3/3) for both Ivan and Thomas.
During baseline with Billy, IOA for cursing/sexual statements was 100% (3/3), inappropriate touching was 100% (23/23), aggression was 85% (6/7), and no target behaviors was 100% (12/12). During FCT with Billy, IOA for communicating vocally or with Sign 1 was 100% for prompted communication (35/35), independent communications (2/2), cursing/sexual statements (2/2), inappropriate touching (1/1), aggression (5/5), and for no target behavior (4/4). Agreement on communicating vocally or with Sign 2 during FCT for cursing/sexual statements was 100% (2/2), for inappropriate touching was 90% (9/10), for aggression was 80% (4/5), for prompts to communicate was 92% (161/174), for communicating independently was 90% (26/29), and for no target behavior was 94% (17/18). No maintenance or generalization data were gathered for Billy because the study ended.
Results
Figure 2 presents the FCT results for Ivan, Thomas, and Billy. During the baseline phase, all participants displayed high rates (100% of trials) of problem behavior with zero occurrences of the new communication form. When intervention was implemented, all participants eventually acquired the new form with a corresponding decline in problem behavior. Of note, there were two distinctly different patterns of acquisition of the new communication among the participants. For example, Ivan’s data show that he acquired the new communication form quickly as evidenced by a steady, increasing trend in his responding after the first several intervention sessions. Thomas’s data replicate this pattern beginning with Session 24, when a communication form that did not promote SIB and that required less effort (i.e., Sign 3) was identified. Specifically, his prior two communication targets were altered because he struck his chin with force during the first sign we selected, and he struggled to form each hand into topographically different shapes in the center of his body for the second sign.

Multiple baseline depicting results of treatment across participants.
In contrast to Ivan and Thomas, Billy required many more trials to acquire a new communication form. In our effort to address this situation, we altered his new form on one occasion due to low rates of independent responding, and a decrease in problem behavior, despite emitting behavioral indication for attention. Thus, Billy was not using problem behavior or the alternative communication response to obtain attention. It was possible that he had learned to sit and wait to be prompted by the examiner (i.e., prompt dependence), as opposed to independently emitting the new communication form. For this reason, the topography of his communication form was adjusted to promote learning a new form without interference from prior instruction.
Maintenance
During the maintenance phase, both Ivan and Thomas continued to sign “eat,” and had zero occurrences of problem behavior when food was present. Maintenance data were not collected on Billy’s communication forms because the first author had to report for an out-of-state internship, ending any further data collection.
Generalization
Ivan and Thomas independently signed “eat” in a variety of settings with multiple adults who were not involved with intervention. Specifically, both participants had 10 separate opportunities to respond when food was present in their environment. For all 10 opportunities, both participants signed “eat” with different care providers in a variety of areas (i.e., in different classrooms, a hallway, lunchroom, office, house, and on a playground) other than those in which they were trained.
Social validity
At the end of the study, we gave BSMs who participated in the study a social validity questionnaire focusing on study procedures and consumer satisfaction. Three of the four BSMs surveyed made positive statements about the study and their experiences. For example, three BSMs commented they had lower levels of stress and that the participants benefitted from the study. They also commented that because each participant was better able to independently communicate his needs, they displayed less problem behavior. In addition, these BSMs commented that they were likely to implement similar procedures in the future with guidance by collaborating with the behavioral consultants in the facility.
The fourth BSM provided answers that varied from the other three. She reported that her stress levels had not been reduced during the study and that the participant still exhibited too much problem behavior. This BSM did comment that she appreciated the efforts and hard work of the people who attempted to teach the participant, but that the participant did not learn because he was not willing to participate appropriately. The comments from the fourth BSM were difficult for us to interpret because they differed from our data, which revealed that the participants had acquired the new communication form and no longer emitted problem behavior to obtain reinforcers in training and generalization contexts.
Discussion
Results from the first study suggest that DTFA permitted the identification of function for each participant’s problem behavior. Results from the second study reveal that FCT effectively replaced problem behavior with an alternative communication form that served the same function. There are several novel features and noteworthy aspects of our study that warrant discussion.
First, DTFA appears to be an effective empirical strategy for identifying the function of problem behavior in naturally occurring settings. Building upon prior research on trial-based FA (Bloom et al., 2011; LaRue et al., 2010; Sigafoos & Saggers, 1995), we required fewer trials for each condition to identify the function of each participant’s problem behavior than are typically conducted in a FA. The additional flexibility and brevity of the DTFA allowed us to adjust the trials as necessary to quickly determine the function of Thomas’s and Billy’s problem behavior after the initial trials did not result in clear differentiation. By distributing fewer trials across natural routines instead of rapid implementation across several sessions in analogue contexts, we avoided the criticism that typical FA procedures may not reflect extant contingencies that exist in the natural environment.
One reason we may have obtained clear results so quickly in our DTFA is because of the relevant information collected from the informal and descriptive assessments. These initial assessments allowed us to design the DTFA conditions in an ecologically valid manner. Thus, the DTFA procedure can be used as an alternative to a traditional FA but should be used in conjunction with nonexperimental methods when the latter produce less than clear and compelling hypotheses. This combination of descriptive assessments and DTFA will allow experimental confirmation of the hypothesized function of the problem behavior, increasing the likelihood of an appropriately designed corresponding intervention.
Second, care providers learned to conduct DTFA trials readily and rapidly. With multiple staff participating, the effectiveness of the FA is enhanced because clients can be assessed in a variety of environments where they exhibit problem behavior and this may lead to better differentiated results that are obtained more quickly (Ringdahl & Sellers, 2000). Furthermore, having multiple staff implement the procedure provides more robust results that are not confined to a single care provider. Future research should focus on increasing the external validity of DTFA by replicating the procedures used in this study with additional care providers in multiple settings (parents at home or in the community, teachers at school, etc.). Of course, problem behavior is specific to context and the results may vary by implementer and setting.
After completing the DTFA, interventions were implemented with each participant in an effort to reduce rates of problem behavior by teaching a replacement response. Results from each participant’s data reveal that the FCT intervention was successful at teaching a socially acceptable communication form. Furthermore, the pattern of acquisition of the replacement form and of the reduction of problem behavior offers evidence of their functional equivalence. Although the data support the effectiveness of the intervention, similarities and differences among each participant’s acquisition data warrant elaboration. For example, Thomas’s data suggest that he performed the initial “eat” sign independently after Session 15; however, he forcefully struck his chin when communicating. To prevent self-injury, we altered his replacement form (so the topography of the newly taught form was incompatible with the topography of face-hitting) to signing “eat” in front of his body using two different hand shapes. The data reveal that Thomas required consistent prompting to perform this new sign (Sessions 18–23) because he was having difficulty forming his hands in two nonidentical shapes in the center of his body. This problem is common among individuals with developmental disabilities (Cermak, Quintero, & Cohen, 1980; Stremel-Campbell, Cantrell, & Halle, 1977). For this reason, his target sign was modified a second time. Thomas’s data reflect that he quickly acquired this third sign, approximating Ivan’s pattern of acquisition.
To determine the timing of instructional delivery during the intervention trials with Billy, the therapist capitalized on Billy’s behavioral indication. Billy’s behavioral indication consisted of looking in the therapist’s direction or orienting his body in the direction of the therapist when he or she entered the room. We changed the topography of Billy’s communication response because our analysis revealed it may be too complex. However, further review of the tapes collected during Sessions 17 through 31 revealed that Billy began waiting for the prompt instead of initiating the replacement response, although he had very few instances of problem behavior. We determined that by immediately providing prompts when behavioral indication was first noted, we may have inadvertently strengthened a behavior chain: therapist enters → Billy looks and orients → therapist provides “physical and verbal prompts” that reinforce his looking and orienting. Thus, prior to emitting the new replacement form, Billy had already been reinforced by physical contact and verbal interaction (i.e., therapist’s prompt). We addressed this issue by increasing the duration of delay between Billy’s behavioral indicators and the therapist’s prompt. During FCT, researchers and practitioners are often concerned that behavioral indication, or precursor behavior, and problem behavior may become chained to the new replacement behavior. We urge researchers and practitioners to be aware that relying on behavioral indication to determine the timing of intervention delivery will likely preempt problem behavior, but this procedure may also result in adventitious reinforcement and subsequent strengthening of behavioral indication.
Two of the three participants required modifications to their initial replacement communication form before reaching criterion. The necessity for modifications might have been due to a number of factors that are related to success when teaching a novel communication form that is functionally equivalent to problem behavior (Halle, Bambara, & Reichle, 2005). For example, relative to the problem behavior, the new communication form ought to require less effort, have a shorter duration between the emission of the communication form and the delivery of reinforcement, and have a denser schedule of reinforcement (Horner & Day, 1991). In addition, it may be necessary to have problem behavior on extinction to reduce its competitive edge when compared with the replacement form. Future research should focus on using additional assessments to identify new forms that will compete favorably with existing forms to foster rapid acquisition of replacement communication.
In this study, we provide evidence suggesting that teaching an alternative form of communication when each participant displayed behavioral indication (Drasgow & Halle, 1995; Lang et al., 2010) of high levels of motivation to access a reinforcer may facilitate maintenance of the skill, discriminated responding, transfer of stimulus control, and increased generalization. Evidence for each participant’s internal state serving as a discriminative stimulus for requests was provided through several observations. Ivan and Thomas were taught the “eat” sign only on those occasions when they emitted behavioral indication, so we were relatively certain that the reinforcing value of food was prepotent. For example, we waited until they looked at the food and began to raise their arms, and then prompted them to sign “eat.” Although we used the same approach with Billy (i.e., we waited until he stared at the therapist for at least 2 s or mumbled while looking in the therapist’s direction), his data show that he required many more trials to acquire the request “talk.” This relatively slower acquisition may be attributable to the topographies of the problem behaviors involved. Ivan and Thomas had one specific topography (i.e., food stealing) that they emitted to access food, and the behavior could be easily molded physically to produce the replacement communication form. In contrast, Billy had a larger repertoire of problem behavior that he emitted for attention and the behaviors (i.e., cursing/sexual statements and forceful aggression) were not as easy to redirect or prevent.
We did not specifically program for generalization by conducting the FCT in multiple settings or with multiple care providers. However, generalized responding occurred when each participant’s motivational state served as the discriminative stimulus. The generalization data collected for Ivan and Thomas reveal they emitted their new communication form with other care providers and in settings other than those in which they were trained.
One limitation of this study pertains to maintenance and generalization data. They were collected shortly after FCT ended and, thus, may not be predictive of how well the communication form would endure over longer periods of time. Although the gathering of long-term follow-up data is not a novel recommendation, future research in this area should emphasize evaluating variables that are sensitive predictors of performance over time. Also, of even greater importance is the investigation of reasons why communication forms are not maintained over time (e.g., difficult for others to recognize, care provider finds communication form annoying or stigmatizing). Despite these limitations, the results of the current study suggest that the DTFA is an effective procedure for identifying the functions of an individual’s problem behavior in their natural environment. In addition, by focusing more closely on motivating operations in the natural environment at the precise point that FCT instruction is delivered, individuals with severe problem behavior can be taught to communicate in socially acceptable ways while preserving the existing function of their problem behavior. DFTA and FCT are an effective combination to enhance the independence of individuals with severe disabilities and problem behavior, and to improve the quality of life for them and for their care providers.
Footnotes
Acknowledgements
We wish to give extensive thanks to the staff at the facility that participated in this study, particularly for their endless dedication for improving the lives of the individuals with whom they work. Also, thanks to the students who participated and allowed us to learn from them throughout this study.
Authors’ Note
The project was completed as a portion of the first author’s dissertation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.