
Abstract
This study examined the effects of teaching the reframing of negative statements through self-management and video-feedback on social conversation in adults with autism spectrum disorder (ASD). A multiple baseline design across five participants showed that, following intervention, all were able to increase their positive and neutral statements while decreasing negative statements, with generalization to peers in new settings. In addition, four of the five participants’ affect and interest improved following the intervention, and three were rated as more socially desirable. Furthermore, post-treatment improvements were noted on standardized measures of depression, anxiety, and hopelessness. Results are discussed in terms of improving general social communicative interactions and quality of life in adults with ASD.
Introduction
Impairments in social communication in individuals with autism spectrum disorder (ASD) can interfere with social interactions, friendships, and intimate relationships (Howlin, 2000). Research suggests that even when children progress well with the acquisition of age-appropriate language structures, they can continue to have difficulties developing social relationships with peers as they grow older (Bauminger & Kasari, 2000; Howlin, 2000; Strain & Schwartz, 2001). Furthermore, a growing body of literature suggests that up to 65% of individuals with ASD develop co-morbid disorders of depression and anxiety, which are frequently caused by their difficulties with interpersonal communication skills and challenges with social relationships (L. K. Koegel, Detar, Fox, & Koegel, 2014; Van Bergeijk, Klin, & Volkmar, 2008). As well, individuals with ASD often demonstrate higher levels of negative emotions and difficulty with emotion regulation (Samson, Huber, & Gross, 2012). These increased levels of expressed negativity may affect their ability to develop and maintain friendships. It is, therefore, important to develop intervention procedures to reduce negative statements for adults on the autism spectrum that exhibit high levels of this behavior during social conversation.
A number of techniques have emerged in the literature as effective interventions for social conversation, including reframing, video-feedback, and self-management (Müller, Schuler, & Yates, 2008). Reframing, or the re-stating of negative statements to focus on their positive qualities, has been shown to improve mental health components such as gratitude and depression, as well as relationship outcomes such as relationship satisfaction and relationship maintenance (Lambert, Fincham, & Stillman, 2012). Reframing interventions have been empirically validated as beneficial treatments for a range of psychological conditions, including social anxiety (Goldin et al., 2012), posttraumatic stress disorder (Moore, Varra, Michael, & Simpson, 2010), and depression and anxiety in parents of children with ASD (Benson, 2010). However, the effectiveness of a reframing intervention in adults with ASD has yet to be investigated.
Another promising area that has emerged for young adults with ASD is that of video-based interventions. Video-feedback is a relatively new type of intervention, which includes viewing video clips and evaluating one’s own previous performance. In general, video-based interventions have proven to be successful with individuals with ASD to increase positive behaviors across a range of areas, including sharing, greetings, labeling, eye gaze, response latency, and socialization (Ayres & Langone, 2005; Bellini & Akullian, 2007). Recent literature suggests that video-modeling interventions may lead to faster and greater acquisition of the target behavior than in-vivo modeling, particularly in individuals with ASD who prefer watching videos more than social interaction (Charlop-Christy, Le, & Freeman, 2000; McCoy & Hermansen, 2007). In addition, those diagnosed with ASD may be particularly receptive to video-modeling interventions, due to their reported strength in visual perception (Ayres & Langone, 2005; Grandin, 1995; Rayner, Denholm, & Sigafoos, 2009) and the interventionist’s ability to manipulate the control of attention on the relevant cue (addressing overselectivity) embedded in the video-modeling framework (Bellini & Akullian, 2007; Charlop-Christy et al., 2000).
Another procedure shown to be effective in ameliorating social communication impairments in individuals with ASD is the teaching of conversational skills through self-management (Boettcher, 2004; L. K. Koegel, Koegel, Hurley, & Frea, 1992). Self-management creates the opportunity for individuals to evaluate, record, and be reinforced for their appropriate behavior. This procedure can also improve generalization and maintenance of targeted social areas (Hughes et al., 2012; Koegel, Koegel, & Parks, 1995). Self-management has provided promise for individuals with ASD to self-regulate their own behaviors rather than relying on others for prompts or other external interventions (Lee, Simpson, & Shogren, 2007; McDougall, 1998). In addition, it has been shown to increase responsiveness during social conversation with generalization to natural community settings in the absence of an interventionist (L. K. Koegel et al., 1992) and to increase the variety of expressive language utterances during social conversation (Barlow, Wright, Sheasby, Turner, & Hainsworth, 2002).
Therefore, based on these effective interventions, the proposed study addressed the following research questions:
Method
Participants and Setting
Five adults between 20 and 37 years of age participated in this study. All were referred to the University Autism Center by the California State Department of Rehabilitation for vocational and behavior intervention, specifically for difficulty with socialization. Each participant met the following criteria: (a) had a diagnosis of ASD according to the specified criteria in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) from an outside agency and confirmed by our center as either autism or Social Communication Disorder, (b) spoke in full, syntactically correct sentences, (c) had IQ scores within average range, and (d) exhibited negative statements during at least 25% of intervals during conversational probes. Specific participant characteristics are listed below.
Participant 1
Mary was a 37-year-old Caucasian woman. She worked as a staff member at a department store and simultaneously pursued an online degree related to electronic health records. Mary lived with her parents and spent the majority of her free time alone in her bedroom either studying for her courses or looking up topics of interest on the Internet. She reported not having any close friends and did not participate in any social activities. She noted having difficulty maintaining conversation with peers and reported feeling depressed due to her challenges initiating and maintaining friendships.
Participant 2
Angela was a 37-year-old Caucasian woman. She had previously completed her academic studies at a local community college and had worked in several administrative assistant positions but was fired due to emotion regulation difficulties in the workplace. She engaged in once-weekly activities with other individuals with disabilities organized by a social skills group with counselors present. Angela did not spend time with typical peers, nor did she report attending any other activities.
Participant 3
Daniel was a 22-year-old Asian American man. He was in the process of finishing his senior year at a 4-year university and lived independently in on-campus housing with several roommates. He maintained an overall grade point average (GPA) of above 3.0, and in his free time, engaged in solitary activities including playing video games and watching Anime movies online. As part of his ongoing intervention, he attended a weekly on-campus club (an Anime club) on Friday nights with the support of an undergraduate peer. He did not engage in any additional social activities.
Participant 4
David was a 20-year-old Caucasian man. He was a senior studying sociology at a 4-year university but dropped out due to social and academic difficulties. At the time of the study, he was enrolled in courses at a community college studying video game design, with a GPA of 4.0. He lived at home with his parents and reported having few friends. Although he participated in the school’s computer science club and tennis, he did not spend time with peers outside of these formal activities. In addition, he noted having difficulty maintaining conversation with peers.
Participant 5
Sam was a 23-year-old Caucasian man. At the time of the study, he was studying geology at a local community college but was on academic probation for failing to meet a minimum 2.5 GPA. He lived at home with his parents and reported having a few friends he met through structured activities but to whom he never initiated or engaged with during informal social events. Furthermore, he reported being only somewhat satisfied with his college experience and having difficulty interacting with peers.
Intervention sessions were conducted in the university campus in a clinic room at the Autism Center. Clinic rooms were decorated like a living room with chairs, sofas, and pictures. A small video camera was placed on top of a table to record sessions. Generalization probes were recorded in mainstream areas of campus, such as in common outside areas and at campus and community restaurants and cafés.
Experimental Design and Procedures
Data were collected in the context of a multiple baseline design across participants (Kratochwill et al., 2010). The number of baseline points was systematically staggered for 4, 6, 8, 10, and 12 weeks, respectively, for the five participants.
Baseline
Prior to the start of intervention, baseline conversational probes were collected for each participant. These probes consisted of weekly, 10-min videotaped conversations with a similarly aged adult. During baseline, no instructions were provided regarding the conversation. Rather, participants were simply asked to chat and get to know each other. No feedback was provided during these probes. In addition, during the last session of the baseline period prior to the start of intervention, each participant completed the following standardized self-reports to assess general emotional functioning: the Beck Depression Inventory (BDI-II; Beck, Steer, & Brown, 1996), the Beck Anxiety Inventory (BAI; Beck, Epstein, Brown, & Steer, 1988), and the Beck Hopelessness Scale (BHS; Beck, Weissman, Lester, & Trexler, 1974).
Intervention
Intervention sessions began 1 week after the final baseline session for each participant, as participants were seen on a weekly basis. All intervention sessions were conducted by graduate students, who had at least 3 years of experience working with individuals with ASD. The first session of the intervention phase began with a description of the importance of reframing and the undesirable impact that negative statements may have on peers, co-workers, or potential employers. Next, the clinician would model both negative statements and reframed statements, and then check for understanding by briefly role-playing possible scenarios that would call for reframing. For example, the clinician would explain that “I can’t wait to be done with my boring school year” was a negative statement and would coach the client that this statement could be reframed as “I am looking forward to summer.” This initial brief training lasted approximately 10 to 15 min for each participant.
Each subsequent intervention session consisted of a video-feedback portion followed by a practice conversation. The video-feedback portion consisted of four systematic steps: (a) The clinician played the video clip and paused it after the conversational partner asked a question or provided a pause for the participant to speak, (b) the clinician asked the participant to generate three appropriate responses (i.e., responses that were not negative) and explain why they were positive or neutral. If the participant was unable to provide a positive or neutral response, the clinician assisted the participant by helping to identify positive and neutral responses, and then discussed why the response was positive or neutral. Next, (c) the clinician continued to play the tape to review the participant’s actual response, and then asked the participant to evaluate if that response was positive, neutral, or negative. If the response was negative, the clinician asked the participant to reframe it into a positive or neutral statement, and (d) the clinician praised the participant’s correct reframing into positive and negative statements. Video-feedback lasted about 20 min, with approximately six responses played and discussed per session.
Following each video-feedback portion of the session, the participant engaged in a 10-min videotaped conversation with the clinician. During this conversation, the participant was instructed to self-manage by making a checkmark on their sheet for each minute that they reframed a negative statement into a positive or neutral statement during the conversation. Participants, therefore, self-monitored their use of reframing on a minute-by-minute basis during each conversation.
The video-feedback portion of the intervention was faded and the practice portion alone was used once the participant was able to independently identify at least three appropriate uses of reframing for each opportunity shown that needed improvement, and the percentage of time with negative statements was 10% or lower during conversation probes. The exit criterion for intervention was engaging in negative statements during 10% or less of the time for five consecutive conversational probes, including at least one generalization probe in a non-clinical setting. Intervention, therefore, lasted a total of 4 weeks for Participants 1 to 3, and a total of 8 weeks for Participant 4, who continued with additional intervention to meet the exit criterion. Alternative exit criterion was indication of participant satisfaction and their expression of no longer needing further services, as was the case with Participant 5.
Generalization and follow-up
To assess for generalization of positive and neutral statements during conversations with similar-age typical peers in community settings, an approximately 10-min generalization conversation probe was collected throughout the baseline, intervention, and during follow-up. During generalization probes, the participants had a conversation outside of the clinical setting (see above) with a typical peer that was naïve to the purpose of the study. Typical peers selected for such conversations included similarly aged clinic staff and research assistants who were neither involved in nor informed about the purpose of the study. Settings of generalization probes were all away from the clinic and not within the rooms or building where intervention sessions took place, and included mainstream areas of campus, such as in common outside park areas and at campus and community restaurants and cafés. Generalization probes did not take place on the same day as an intervention session, but rather 1 week following intervention.
In addition, a 10-min follow-up conversation probe was conducted 2 months after ending intervention with typical peers and in the natural environment. An additional follow-up conversational probe was collected for Participant 2 who demonstrated an increased number of negative statements during the 2-month follow-up probe to assess whether the higher number of negative statements was consistent following the completion of intervention.
Dependent Measures
Data were collected on four dependent measures based on coding of videotaped probes during baseline and intervention. Coding was implemented by undergraduate research assistants naïve to the purpose of the study. Data were collected on (a) negative statements during social conversation, (b) positive/neutral statements during social conversation each week, (c) affect and interest during conversation, and (d) social desirability. In addition, we collected social validation measures through three self-report questionnaires relating to emotional functioning. Each area is defined below.
Negative statements
Data were collected on negative statements made by the participant during the weekly 10-min conversation probes. Negative statements were defined as utterances made by the participant that reflected sadness, anger, or anxiety. Examples of these negative statements are listed in Table 1. On rare occasion, participants would make statements that were in response to the conversational partner’s misfortune. These were not counted as negative statements. For example, if the conversational partner said “I was sick over the weekend” and the participant responded with “oh, that’s awful,” this statement was not coded as negative because it indicated the pro-social behavior of empathizing with another person. Interval scoring was used to measure the amount of negative statements. For each 30-s interval in the conversation, a plus (+) was recorded if there was a negative statement in the interval, and a minus (−) was recorded if there were no negative statements made by the participant. The percentage of intervals with negative statements for the 10-min probe was then calculated.
Examples of Negative Statements and Their Reframed Replacement Statements.

Positive and neutral statements
Positive statements were defined as utterances made by the participant that reflected happiness or excitement in the content of speech, independent of affect. Neutral statements were defined as utterances made by the participant that reflected an absence of negative or positive content of speech, independent of affect. Positive and neutral statements were merged into a single dependent variable, in defining the use of reframing as making positive or neutral statements in place of and with the exclusion of negative statements. Using the same interval scoring method as mentioned above, overall percentage of time during the probe in which positive and neutral statements were made while excluding negative statements was calculated.
Affect and conversational interest
A 6-point rating scale adapted from Dunlap and Koegel (1980) was used to assess affect/interest in conversation. This measure was used to assess any collateral changes in affect/interest as a result of reframing negative statements during conversation. Ratings for affect/interest included low affect/interest (0–1) defined as appears discontent with the ongoing activities, does not seem to be enjoying him/herself; medium affect/interest (2–3) defined as does not appear to be decidedly happy or particularly unhappy, may smile or frown occasionally, but overall seems rather neutral in this situation; and high affect/interest (4–5) defined as smiles, laughs appropriately, seems to be enjoying self. Each 1-min interval was given a global score throughout the 10-min probe. The average affect/interest rating was calculated by summing the total scores and dividing by the number of intervals.
Social desirability
A social desirability Likert-type scale was adapted from Dunlap and Koegel (1980) to assess the social validity of the intervention. Specifically, we attempted to determine to what extent similarly aged individuals would like to interact with the participants. Three general categories focused on whether they would be desirable, neutral (somewhat desirable), or undesirable as a conversational partner. To assess for general social desirability following intervention, coders naïve to the purpose of the study were given instructions to provide general ratings of the participant as a conversational partner, keeping in mind how much they would want to have a conversation with them. A 6-point rating scale was developed for the coders to rate the participants as very undesirable as a social conversational partner (0–1), somewhat desirable as a conversational partner (2–3), and very desirable as a conversational partner (4–5). This rating was completed when watching one video selected randomly from each participant’s collection of baseline videos, intervention videos, as well as the follow-up video.
General emotional functioning
In addition to the behavioral measures described above, three standardized assessments were given to the participants to assess depressive and anxiety symptoms at baseline (pre-intervention), following the completion of intervention (post-intervention), and at follow-up. These tests were administered far enough apart to be consistent with the Beck testing protocols.
BDI-II
The BDI-II consists of 21 multiple-choice items and is designed to measure the severity of depression in adolescents and adults aged 13 and older. The inventory is composed of self-report items relating to symptoms of depression such as hopelessness and irritability, cognitions such as guilt or feelings of being punished, as well as physical symptoms such as fatigue, appetite, changes in sleeping patterns, and lack of interest in sexual activity. Individuals are asked to respond to each question based on the previous 2-week time period. The BDI-II is widely used as an indicator of the severity of depression, and numerous studies provide evidence for its reliability and validity across different populations and cultural groups (Beck, Steer, Ball, & Ranieri, 1996; Whisman, Perez, & Ramel, 2000). It has also been used in numerous treatment outcome studies.
BAI
The BAI consists of 21 self-report items and is used to assess anxiety levels in adolescents and adults between ages of 17 and 80. The test is a quick screening tool to identify anxiety in two domains that are descriptive of subjective somatic or panic-related anxiety symptoms. The inventory asks individuals about how they have been feeling in the last week as measured by common symptoms of anxiety, such as numbness and tingling, sweating (not due to heat), and fear of the worst happening. Each question has four possible answer choices of not at all, mildly, moderately, and severely. Reliability (e.g., internal, test–retest) and validity (e.g., concurrent, criterion) have been reported for the BAI (Fydrich, Dowdall, & Chambless, 1992; Kabacoff, Segal, Hersen, & Van Hasselt, 1997).
BHS
The BHS consists of 20 self-report items and is used to measure major hopelessness for individuals aged 13 and older. More specifically, this questionnaire was designed to measure three major aspects of hopelessness, including feelings about the future, loss of motivation, and expectations. Respondents mark true or false to each item. The BHS measures the extent of the individual’s negative attitudes or pessimism about the future. Norms are available and reliability and validity data have been reported for the measure (Beck et al., 1974; Steed, 2001).
Data Recorders and Reliability
Reliability for negative and positive/neutral statements was obtained by having two naïve undergraduate research assistants independently code the intervals that contained (a) negative statements or (b) positive/neutral statements during the 10-min videotaped probes. These were presented in random order to control for experimenter bias and observer drift. Reliability was calculated for 25% of the probes, which were randomly selected, using a computer-generated program, from baseline and treatment. Percentage of agreement between observers was calculated by dividing the number of agreements by the sum of agreements plus disagreements and multiplying by 100 (Bailey & Burch, 2002). The percentage agreement for negative statements was 85% (range = 70%–100%), and for positive/neutral statements, percentage was 91% (range = 75%–100%).
Reliability for the categorical measure of affect/interest was calculated using Cohen’s weighted kappa coefficient. Because this measure takes into account agreement by chance but allows for incorporation of scaled degrees of disagreement, it is considered a robust measure of inter-observer agreement for categorical data (Cohen, 1968, 1988). Agreement for affect/interest was scored as both raters coding within the same range (low, neutral, or high). Cohen’s weighted kappa coefficient for affect was .32, indicating fair agreement.
Reliability was scored for the standardized self-report measures by having a second observer compute the scores on 31% (4 of the 13 assessments), again using a computer-generated randomization of the protocols. Reliability was 100% for the BDI-II, 100% for the BAI, and 96% for the BHS.
Results
The first question asked in this study was whether the use of a reframing intervention incorporating video-feedback and self-management would decrease the percentage of intervals that participants with ASD engaged in negative statements. The results of this question are shown in Figure 1. As can be seen, all five participants made multiple negative statements during baseline.

Negative comments in conversation probes.
For example, Participant 1, Mary, made negative statements during social conversation at an average of 40% of the 30-s intervals during baseline. When intervention began, she immediately decreased her negative statements to an average of 10% of 30-s intervals with negative statements during intervention. During the last generalization probe, as well as the follow-up probe, she did not make any negative statements. Participant 2 had rapid decreases in the percent of intervals with negative statements with some increase at the 2-month follow-up with a peer. Therefore, a second follow-up point was collected that was again at a lower level than baseline points. The remaining three participants showed higher percentages of intervals with negative statements in baseline and decreased levels during intervention. The generalization and follow-up probes for Participants 3, 4, and 5 showed lower percentages of intervals with negative statements when they interacted with new peers in novel settings.
The second question asked in this study was whether the use of a reframing intervention incorporating video-feedback and self-management would increase the percentage of time intervals with only positive and neutral statements during social conversation (without any negative statements). The results of this question are shown in Figure 2. All five participants showed improvements in the number of intervals with only positive and neutral statements. For example, Participant 1 engaged in only positive and neutral statements during approximately 42% of the intervals. In contrast, during intervention, she engaged in positive and neutral statements at an average of 90% of the intervals. Similarly, during baseline, Participants 2, 3, 4, and 5 engaged in positive and neutral statements at an average of 63.5%, 70%, 63.6%, and 55.4% of the time, respectively. However, after the start of intervention, their positive and neutral statements increased to 97%, 98%, 84.8%, and 87.5% of intervals, respectively. Furthermore, during generalization and follow-up, three of the four participants improved on their percentages of positive and neutral statements and Participant 2 showed improved generalization on the second follow-up probe.
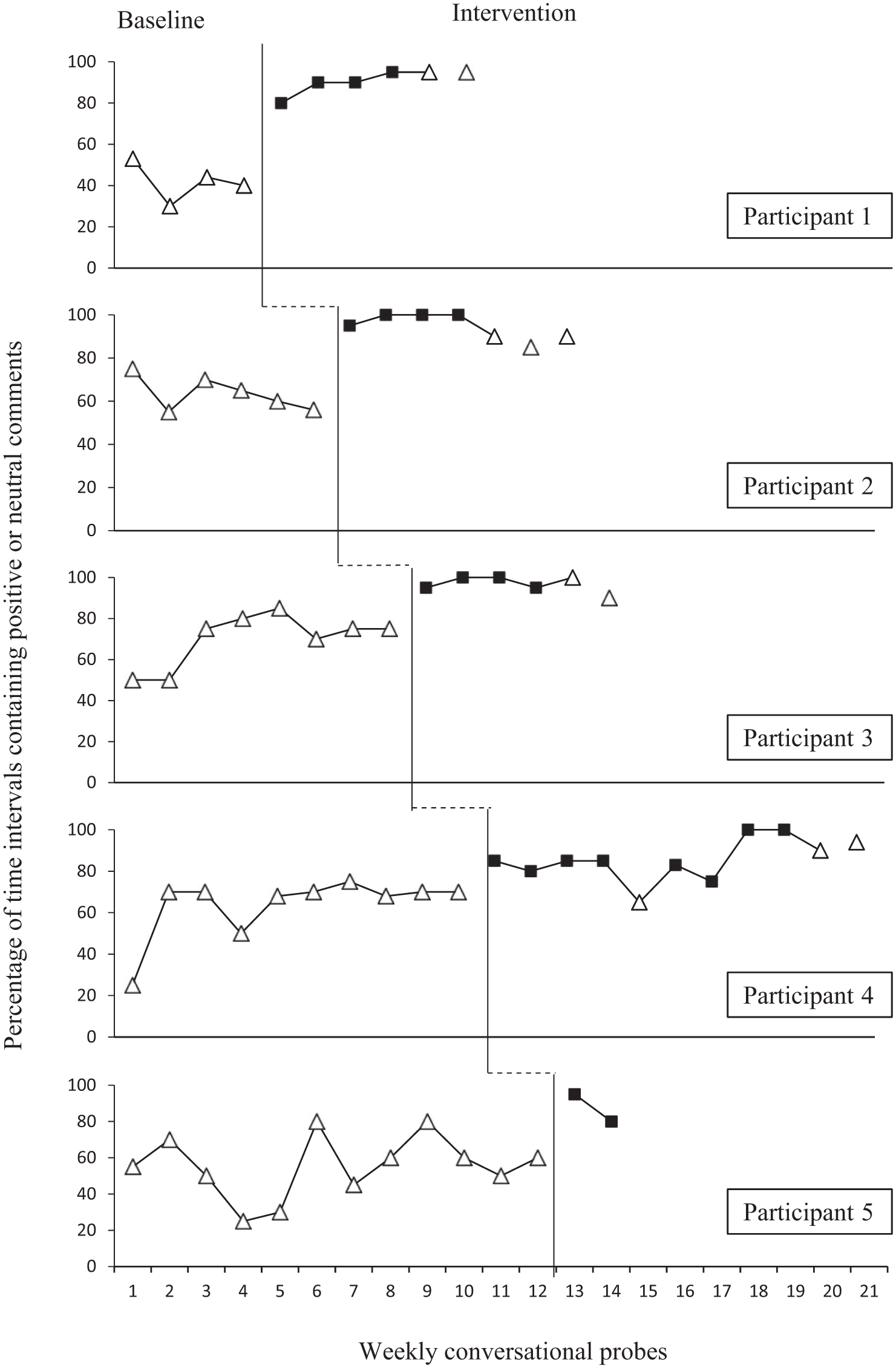
Positive and neutral comments in conversation probes.
The third question asked in this study was whether the reframing intervention would produce collateral gains in affect/interest and social desirability during social conversation. The results of this question are shown in Table 2. Four of the five participants showed improvements in their affect/interest scores following the baseline probes. These gains continued to improve at follow-up. Specifically, Participant 1’s affect/interest averaged 2.3 during the baseline session probes and then improved to 3.1 during the intervention session probes, which was above the low/neutral range. Furthermore, her affect/interest continued to improve at her follow-up probe to 3.3, which was above the neutral range. Participant 2’s average affect/interest score improved from 2.3 during her baseline session probes to 2.5 during her intervention session probes and continued to improve to an average of 3.4 during her two follow-up probes, which was above the low/neutral range. Participant 3’s affect/interest remained fairly stable throughout the study in the above the neutral range with average scores of 3.5 and 3 during the baseline and intervention session probes, respectively, and 3.3 during his follow-up probe. Participant 4 improved from 1.9 during his baseline probes to 2.4 during the intervention probes, with his final follow-up probe at 3.1. Thus, he exhibited low affect/interest during baseline, improved to neutral affect during the intervention probes, then further improved to the above neutral range at his follow-up probe. Participant 5’s affect/interest improved from the 2.3 during the baseline probes (in the mid-neutral range) to 3 during the intervention probes, which was in the high-neutral range.
Social Desirability and Affect/Interest Ratings During Baseline, Intervention, and Follow-Up Sessions.

Note. BL = baseline; INT = intervention.
Unavailable data.
In regard to scored social desirability, raters scored three of the five participants as being more socially desirable following intervention, and two remained the same. Specifically, Participants 2, 4, and 5 were rated as more desirable socially, following the intervention. That is, all improved by 1 to 2 points following the intervention. Participant 3 was rated as a highly desirable conversational partner during baseline and remained that way following intervention and at follow-up.
The final questions asked in this study were whether collateral gains on standardized measures of depression, anxiety, and hopelessness would occur after implementation of the intervention. The results of this question are shown in Table 3. Four of the five participants were available to complete the testing at baseline, following intervention, and at follow-up. On the BDI-II, three of the four participants improved their measures of depression. That is, Participants 1, 3, and 4 reported lower levels of depressive symptoms following intervention, and Participant 2 reported a lower level of depressive symptoms at post-intervention, but this did not maintain at follow-up. Three of the four participants who completed all of the measures (pre, post, and follow-up) improved in their reported level of depression but remained in the same general range, indicating they had minimal to moderate depressive symptoms. Participant 2 moved from minimal symptoms at baseline to no symptoms following intervention and at follow-up. Participant 4 reported minimal symptoms at baseline and post-intervention and then moved to moderate range at follow-up. In regard to the BAI, three of the four participants (Participants 1, 2, and 4) reported lower levels of anxiety following intervention and continued to report lower levels of anxious symptoms at follow-up. Participant 3 reported no anxious symptoms throughout the entirety of the study. Participant 1 moved from severe symptoms at baseline to moderate symptoms at post and follow-up. Participant 2 moved from the mild range at baseline and post-intervention to the minimal range at follow-up. Finally, Participant 4 moved from minimal reported symptoms at baseline to no anxious symptoms at post and follow-up.
Scores on the BDI-II, the BAI, and the BHS During Baseline, Intervention, and Follow-Up Sessions.
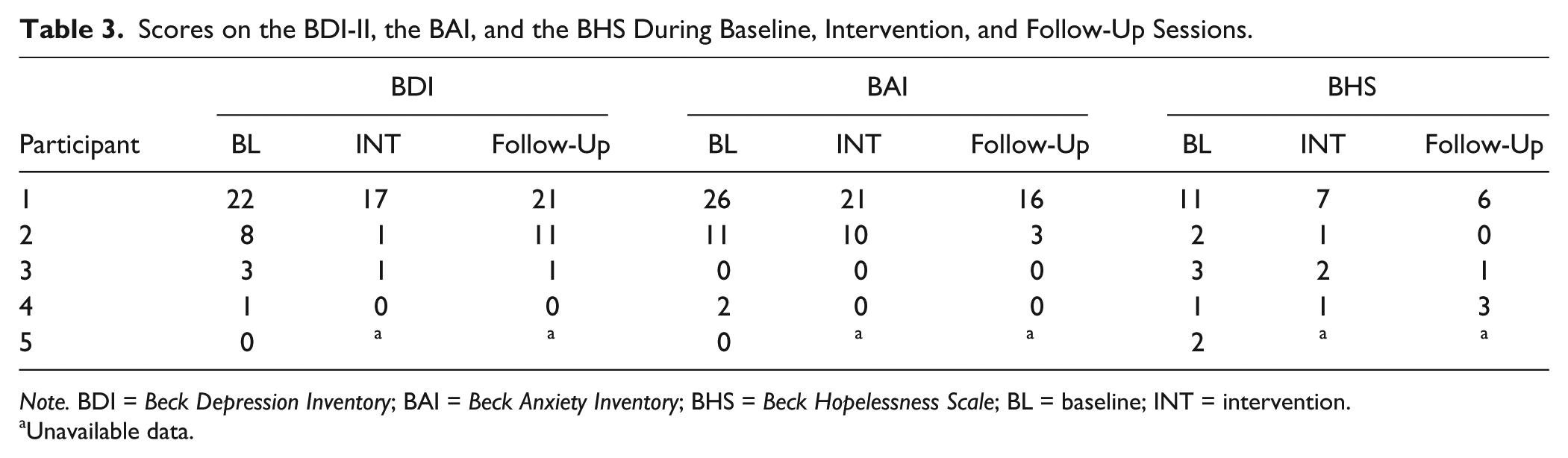
Note. BDI = Beck Depression Inventory; BAI = Beck Anxiety Inventory; BHS = Beck Hopelessness Scale; BL = baseline; INT = intervention.
Unavailable data.
In regard to hopelessness symptoms measured on the BHS, three of the four participants (Participants 1, 2, and 3) reported improvements in feelings of hopelessness, and Participant 4 reported the same level of hopelessness symptoms at baseline and post-intervention with no maintenance at follow-up. Participant 1 moved from moderate symptoms at baseline to minimal hopelessness symptoms at post-intervention and follow-up. Participant 2 reported minimal symptoms at baseline and post-intervention and no hopelessness symptoms at follow-up. Participants 3 and 4 remained in the mild range throughout the study. It should be noted that Participant 5 stated that he felt pleased with what he had learned during the intervention sessions and that he no longer needed additional intervention. The clinician continued to call him for several weeks prior to his regularly scheduled appointments, but he continuously expressed satisfaction with his treatment gains and reported that he did not feel that he needed additional intervention sessions.
Discussion
The main purpose of this study was to assess whether social conversation could be improved in adults who were observed to make repeated negative statements while engaging in social conversation. Despite the frequent psychosocial difficulties in this population, very few studies have focused on areas such as social conversation with adults, a skill that is essential for meaningful relationships (Gantman, Kapp, Orenski, & Laugeson, 2012; Howlin & Yates, 1999). The few studies that have targeted this population have shown general overall improvement in social functioning, after interventions that have focused on specific skills such as question-asking (Detar, 2013) as well as treatment in the context of peer groups (Gantman et al., 2012; Mesibov, 1984) and during inclusion with typical peers (R. Koegel, Kim, Koegel, & Schwartzman, 2013). This study also resulted in improvements in social conversation with positive generalized improvements for several participants in a variety of areas. It may be proposed that although such an intervention does not address all social difficulties faced by adults on the spectrum, it holds promise for improving the crucial conversational behavior of reframing as well as positively affecting the general emotional well-being of those actively practicing reframing.
The first theoretical question one might ask is why social conversation can be so challenging in this population. Many theories suggest that pragmatic deficits in autism may relate to an inability to relate to how they are perceived by their communicative partners (Baron-Cohen, 1989). The participants in this study reported very few social contacts at baseline but did not appear to adjust their conversations to decrease negative statements that may have interfered with social relationships. This behavior of repeatedly making negative statements may have been related to this difficulty in attending to their partners’ social cues indicating that their excessive negativity made them less desirable conversational partners.
This is supported by the fact that the reframing intervention was not only effective in reducing negative statements, but also concomitant improvements such as social desirability in three out of the five participants occurred. In fact, according to the qualitative descriptions depicted by the Likert-type scale utilized, Participant 2 increased from being rated as a very undesirable conversational partner to a somewhat desirable conversational partner, and Participant 5 increased from being rated as a somewhat desirable conversational partner to a very desirable conversational partner. Such a demonstrated ability to decrease negative statements in conversation holds promise for communicative partners’ social perception of individuals with ASD. These social perceptions may improve areas such as the initiating and maintaining of meaningful social relationships for this population, corresponding with previous findings illustrating the strong association between increased reframing abilities and improved quality of relationships with others (Lambert, 2010).
Moreover, collateral improvements were also seen in self-report measures related to depression, anxiety, and hopelessness for four out of the five participants following intervention, corroborating previous findings with other populations demonstrating that an increased general ability to use reframing of individuals’ life perspectives may have widespread implications for various areas such as decreased depressive symptoms according to the BDI-II (Kraft, Claiborn, & Dowd, 1985) and the Center for Epidemiologic Studies Depression Scale (CESD) as well as positive coping abilities following traumatic events (Moore et al., 2010). Given that reframing has also been shown to improve test performance for those with test-related anxiety (Kass & Fish, 1991) as well as increased coping skills and performance-related satisfaction in individuals with reported high levels of perfectionism and self-criticism (Stoeber & Janssen, 2011), it may be of interest in future studies to further explore perception of self as well as performance scores following reframing interventions in this population. Thus, selecting specific targets such as reframing for intervention may be helpful in overall quality of life gains for some individuals on the autism spectrum.
A second issue relates to the total amount of talking time in which the participants engaged. Given that the participants were provided with feedback on their negative statements, it is possible that the participants engaged in less talking, thereby artificially lowering their percentages of negative statements. Analysis of the data suggests the number of intervals with talking remained fairly stable across all conditions at above 90%. Therefore, the participants maintained a high level of conversation, while emitting fewer negative statements and more positive and neutral statements following intervention. Thus, we are optimistic that the participants enjoyed the social interactions, because they were able to continue being socially engaged at post-intervention and follow-up while benefitting from the feedback regarding reframing their comments during social conversation.
There are some limitations to the present study. First, we used a combination of interventions and the relative effectiveness of each of the interventions was not assessed. Future research assessing the relative effectiveness of the components may be fruitful. Second, the implementation of interval recording for the coding of negative, positive, and neutral comments may be considered as a limitation due to its inability to capture the frequency or intensity of negative, positive, or neutral commenting. Furthermore, although we collected generalization measures with similarly aged peers, we did not assess whether the intervention resulted in increases in the number of friends the participants were able to make after their social conversation improved. Research in this area would be important. Finally, the study was conducted over a short period of time, with the relatively short period of 4 weeks between administration of the BDI, BAI, and BHS before and after treatment for most participants. Longitudinal data to assess if gains maintained or continued to improve may prove to be informative.
In summary, the intervention used in this study did not provide all types of supports needed by the participants with ASD; however, for a brief intervention (mode = 4 weeks), we saw some progress. That is, all participants were able to improve the quality of their conversations by decreasing their negative statements and increasing their positive and neutral statements during social interactions. In addition, collateral gains were evident in the areas of social desirability, affect/interest, and self-report of general emotional functioning. Although a multi-component intervention is important and necessary for adults with ASD if communicative competence is the goal, these individuals’ social lives were significantly negatively affected because of their repeated and frequent negative comments. Therefore, this research suggests that such programs may be helpful in improving social conversation and overall quality of life in individuals with ASD who demonstrate these symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Autism Speaks (Grant/Award No. SB140159).