
Abstract
Background
Diarrheal diseases remain a significant public health concern in urban, resource-limited settings, including Burao City, Somaliland, where socio-demographic factors and household environmental conditions contribute to disease prevalence. This study aimed to assess household sanitation conditions, environmental exposure pathways, and associated risk factors for diarrheal diseases in this urban context.
Methods
A community-based cross-sectional study was conducted from June to August 2025 in Burao City, Somaliland, involving 422 households selected through multistage sampling. Data were collected using structured questionnaires and direct environmental observations to evaluate sanitation infrastructure, hygiene facilities, waste management, and environmental contamination. The occurrence of household diarrheal disease within the previous two weeks was recorded. Bivariate and multivariate logistic regression analyses were used to identify factors independently associated with diarrheal disease.
Results
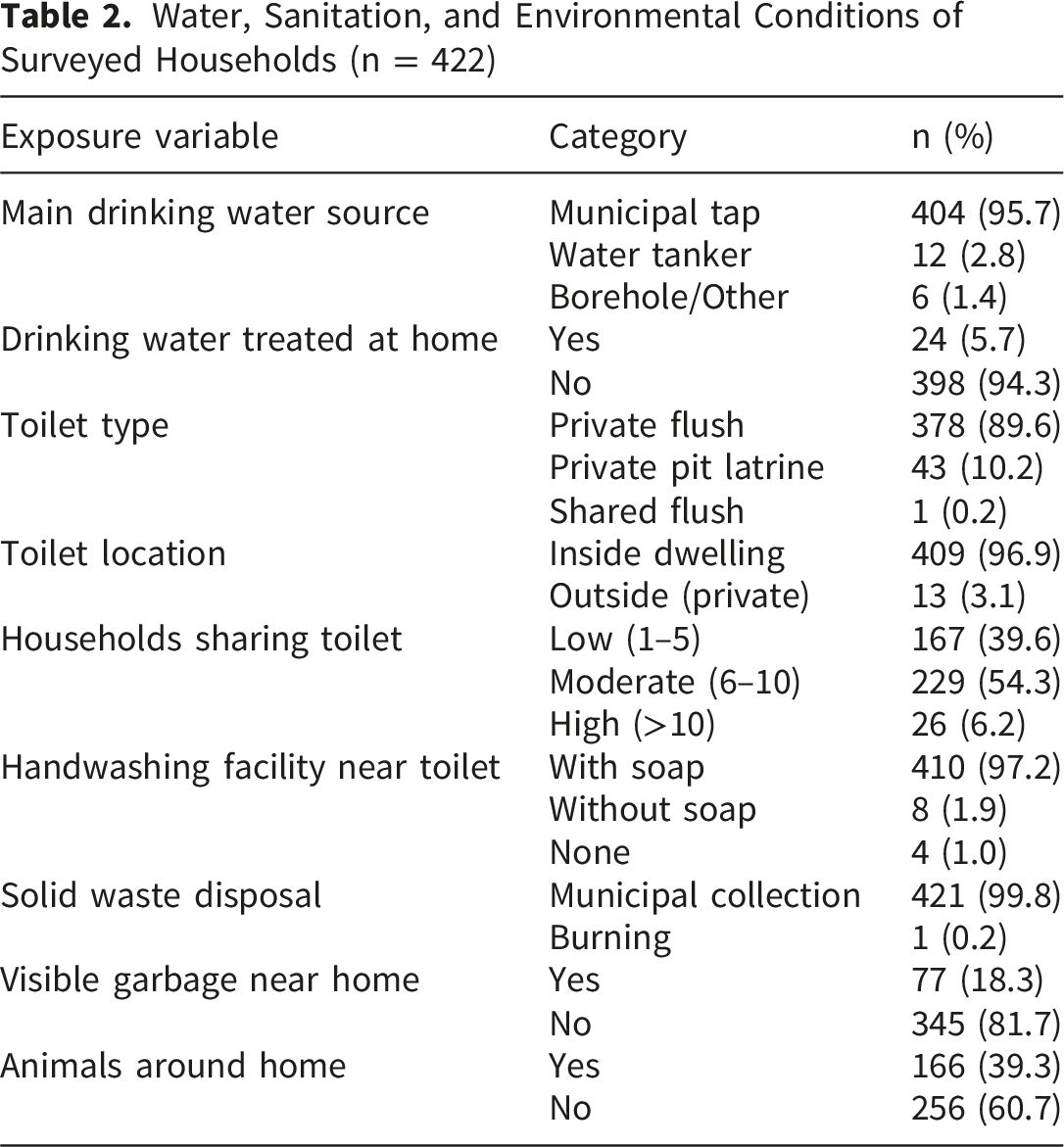
The two-week household diarrheal prevalence was 7.1% (95% CI, 5.0–10.0%). Most households used municipal tap water (95.7%) and had private flush toilets (89.6%), with high availability of handwashing facilities (97.2%). The absence of soap at handwashing stations was the strongest independent predictor of diarrheal disease (adjusted odds ratio [aOR] = 8.51; 95% CI: 1.93–37.52; p < 0.005). Visible garbage near households (aOR = 4.56; 95% CI: 2.12–9.83; p < 0.001) and the presence of domestic animals in living areas (aOR = 2.47; 95% CI: 1.16–5.28; p = 0.019) were also significantly associated with increased diarrheal risk. Additionally, households with three or more children under five years (aOR = 5.05; 95% CI: 1.06–24.17; p = 0.043) and respondents lacking formal education (aOR = 5.70; 95% CI: 1.80–18.02; p = 0.003) had higher odds of diarrhea.
Conclusion
Diarrheal disease in Burao City is strongly associated with modifiable household and environmental factors, particularly the absence of soap at handwashing facilities and environmental contamination. Integrated interventions focusing on sustained hygiene resource availability, improved waste management, safer human–animal interactions, and targeted health education for vulnerable populations are critical for reducing diarrheal morbidity in this urban, resource-constrained context.
Keywords
Key Summary Points
❖ Diarrheal disease remains a significant public health challenge in urban, resource-limited settings like Burao City, Somaliland, driven by sociodemographic and inadequate household sanitation conditions. ❖ This study aimed to assess associated household risk factors for diarrheal disease in Burao City. ❖ The diarrheal prevalence was 7.1%, with key risk factors including absence of soap at handwashing facilities, visible garbage near households, presence of domestic animals, multiple young children, and low educational attainment of respondents. ❖ The findings highlight that ensuring sustained availability of hygiene resources, improving waste management, promoting safer human–animal interactions, and targeted health education are critical to reducing diarrheal diseases in this urban setting.
A graphical abstract summarizing the household sanitation conditions, environmental exposure pathways, and key risk factors associated with diarrheal disease in Burao City is presented in Figure 1. Graphical abstract summarizing household sanitation conditions, environmental exposure pathways, and key risk factors associated with diarrheal disease in Burao City, Somaliland
Integrated context-specific interventions addressing these modifiable factors can significantly improve community health and resilience in rapidly urbanizing, resource-constrained environments.
Background
Diarrheal disease remains a major environmental health concern and is closely linked to exposure to biological hazards arising from inadequate household sanitation and contaminated environments.1,2Fecal–oral transmission of enteric pathogens occurs through multiple exposure pathways, including unsafe sanitation facilities, contaminated household surfaces, wastewater, and improper solid-waste management.3,4 In urban settings with limited sanitation infrastructure, these environmental exposures continue to drive preventable diarrheal morbidity and mortality, contributing significantly to the global disease burden.5,6
The World Health Organization (WHO) and UNICEF Joint Monitoring Programme (JMP) for Water Supply, Sanitation and Hygiene provides standardized indicators to monitor global progress toward safely managed drinking water, sanitation, and hygiene services at the household level, aligned with Sustainable Development Goals (SDG) 3 (Good Health and Well-being) and SDG 6 (Clean Water and Sanitation).7,8 Safely managed drinking water refers to an improved water source located on premises, available when needed, and free from contamination. 9 Safely managed sanitation involves the use of improved sanitation facilities that are not shared and where excreta are safely disposed of or treated.9,10 Household hygiene coverage is assessed by the availability of handwashing facilities with soap and water.3,11 In Somaliland, national data on WASH coverage remain limited, but available estimates suggest substantial gaps in safely managed water and sanitation services, especially in urban areas experiencing rapid population growth, such as Burao City. 12 While municipal tap water access is widespread, challenges persist in ensuring consistent water quality and hygiene resource availability. Similarly, sanitation infrastructure coverage is uneven, with many households relying on unimproved or shared facilities, and hygiene practices such as handwashing with soap are often inconsistent. These WASH deficiencies contribute to the ongoing burden of diarrheal diseases and highlight the urgent need for context-specific assessments and interventions in urban Somaliland.
Household sanitation conditions play a central role in shaping environmental exposure pathways for diarrheal diseases. 13 The use of unimproved or poorly maintained latrines, shared sanitation facilities, unsafe disposal of human excreta, and lack of functional handwashing facilities facilitate fecal contamination in domestic environments. 14 Environmental contamination surrounding households, such as visible fecal matter, stagnant wastewater, and accumulated refuse, can sustain pathogen persistence and increase exposure risk, even when basic sanitation facilities are present. 15 These risks are amplified in densely populated urban areas, where close spatial proximity among sanitation facilities, water sources, and living spaces enhances transmission potential. 16
Urbanization in sub-Saharan Africa has intensified sanitation-and environmental health risks. 17 Rapid population growth, informal settlement expansion, and limited municipal service capacity have resulted in heterogeneous sanitation conditions and inadequate waste management in many cities. 18 Such environments disproportionately expose vulnerable populations, particularly young children, to repeated contact with enteric pathogens through contaminated soil, water, and household surfaces. 19 Therefore, identifying specific sanitation conditions and environmental exposure pathways is essential for targeted risk assessment and effective intervention planning. 20
In Somaliland, evidence on sanitation-related environmental exposure and diarrheal diseases remains limited, particularly in urban contexts. Burao City has experienced substantial population growth driven by internal displacement and rural-to-urban migration, which has placed increased pressure on sanitation infrastructure and environmental services. Many households rely on unimproved sanitation facilities, lack appropriate handwashing infrastructure, and are exposed to poorly managed wastewater and solid waste within their residential compounds. However, systematic assessments linking household sanitation conditions and environmental contamination to diarrheal outcomes in this setting are limited.
Previous studies in this region have largely emphasized water sources or self-reported hygiene behaviors, with less attention to observable sanitation conditions and environmental contamination as direct exposure pathways.21-24 Reliance on self-reported data alone may underestimate true exposure risks, as environmental hazards are often unevenly distributed within household compounds and neighborhoods. Integrating household survey data with structured environmental assessments provides a more comprehensive and objective characterization of sanitation-related exposure relevant to diarrheal disease transmission.
This study examined household sanitation conditions and environmental exposure pathways for diarrheal diseases in Burao City, Somaliland, using a household survey complemented by direct environmental observations. By assessing sanitation infrastructure, hygiene facilities, waste management practices, and environmental contamination within household compounds, this study aimed to identify key exposure pathways associated with household-level diarrhea. The findings support evidence-based sanitation interventions and inform urban environmental health policies in resource-constrained settings.
Methods
Study Aim, Design, and Setting
This community-based cross-sectional study aimed to assess household sanitation conditions, environmental exposure pathways, and associated risk factors for diarrheal diseases among residents of Burao City, Somaliland. Data collection was conducted from June 1 to August 31, 2025. A three-month study period was selected to capture representative household sanitation conditions and environmental exposures during a typical seasonal timeframe, allowing for comprehensive data collection while ensuring logistical feasibility. Burao, the capital of the Togdheer Region, is a rapidly growing urban center with heterogeneous access to improved water and sanitation services.
Study Population and Eligibility
The target population comprised all households in Burao. A household was defined as a group of people living in the same dwelling and sharing meals. Eligible households had resided in the selected neighborhoods for at least six months and had an adult (≥18 years) respondent available at the time of the survey. Household diarrheal disease was operationally defined following the World Health Organization (WHO) criteria as the occurrence of diarrhea passage of three or more loose or watery stools within a 24-hour period among any household member during the two weeks preceding the survey (binary yes/no). 10 Households without a competent respondent, those that declined participation, and those that were temporarily unoccupied were excluded. Within each selected household, one eligible adult respondent (≥18 years) who had lived in the household for at least six months was identified and invited to participate in this study. If more than one eligible individual was present, one respondent was randomly selected using a simple lottery method.
Sample Size and Sampling Procedure
The sample size was calculated using the single population proportion formula, assuming a 50% prevalence of sanitation-related diarrheal outcomes. This conservative estimate was chosen because of the lack of precise household-level diarrheal prevalence data in Burao City across all age groups, ensuring an adequate sample size for detecting associations. Regional studies report higher diarrhea prevalence among children under five years of age (e.g., 16.5% in internally displaced populations in Hargeisa and approximately 19.8% nationally in Somalia); however, these child-specific estimates may not reflect overall household prevalence.21,22 A 95% confidence level and a 5% margin of error were applied. Accounting for a 10% non-response rate yielded a final sample size of 422 households. The catchment area for this study comprised all major administrative zones within the formally defined boundaries of Burao City, the capital of Somaliland’s Togdheer Region. These administrative zones represent the official city limits used by municipal authorities. A multistage sampling technique was employed. From these zones, neighborhoods were randomly selected as clusters using simple random sampling methods. Within each selected neighborhood, a comprehensive household listing was obtained or constructed to serve as a household sampling frame. Households were systematically selected using a fixed sampling interval determined by dividing the total number of households in the neighborhood by the required sample size for each cluster. The first household was randomly selected within the interval, and subsequent households were selected by adding to the interval.
Data Collection Instruments and Procedures
Data were collected using a structured questionnaire adapted from previously published studies,3,6,11,25-27 a pretested questionnaire, and an observational checklist, all of which were modified to suit the local context of Burao. The questionnaire was originally developed in English, translated into Somali, and back-translated to ensure conceptual and linguistic accuracy. Prior to the main survey, the questionnaire was pilot-tested on 20 adult respondents from a neighborhood not included in the main sample to assess clarity, relevance, and reliability. Feedback from the pilot study led to minor adjustments in wording and format to enhance comprehension. The questionnaire included sections on sociodemographic information, drinking water sources and treatment practices, sanitation facility characteristics, handwashing practices, solid waste disposal, presence of domestic animals, and recent occurrence of diarrheal and skin infections. Trained enumerators administered the tools, and supervisors conducted daily reviews to ensure completeness and quality. Enumerators received two days of training on study objectives, ethical conduct, interview techniques, and observational procedures. Observers also documented sanitation conditions at the household level, including toilet type and location, availability of handwashing facilities near toilets, and visible garbage within compounds. The questionnaire captured household drinking water treatment practices, including boiling, filtration, chlorination, and other methods, and household water treatment was defined as any reported practice of treating drinking water at home prior to consumption.
Variables
❖ Socio-demographic: respondent’s sex, education level, household size category, and number of children under five. ❖ Water and sanitation: main drinking water source, household water treatment status (defined as any household-level water treatment practice, such as boiling, filtration, or chlorination), toilet type and location, and number of households sharing the toilet. ❖ Hygiene and environment: availability of handwashing facilities with soap near toilets, solid waste disposal patterns, visible garbage near the household, presence of animals around the home.
Data Management and Statistical Analysis
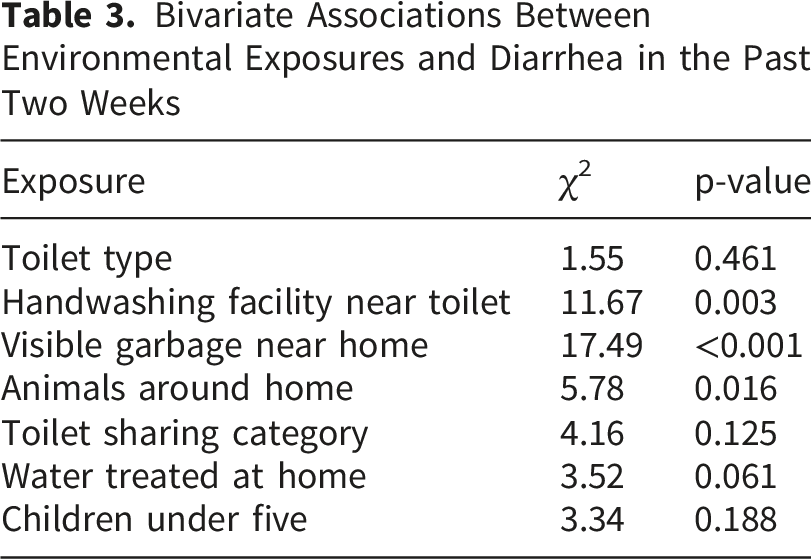
Data were entered and cleaned using Stata version 17. Descriptive statistics (frequencies and percentages) were calculated for all variables. Bivariate associations between diarrheal diseases and sanitation exposure were assessed using Pearson’s chi-square test. Variables with p < 0.20 in the bivariate analysis were included in the multivariable logistic regression to examine independent associations with diarrheal disease. Logistic regression was selected as the appropriate method to model the binary outcome variable and to adjust for potential confounding factors, allowing estimation of adjusted odds ratios (AOR) with 95% confidence intervals (CI).28-30 Statistical significance was set at p < 0.05. Model fit was evaluated using the Pearson goodness-of-fittest.
Result
Socio-Demographic Characteristics of Study Households
Socio-Demographic Characteristics of Households in Burao City, Somaliland (n = 422)

Household Water, Sanitation, and Environmental Conditions
Water, Sanitation, and Environmental Conditions of Surveyed Households (n = 422)
Prevalence of Diarrheal Disease
The overall prevalence of diarrheal diseases among household members in the two weeks preceding the survey was 7.1% (95% CI: 5.0–10.0) (Figure 2). Overall prevalence of diarrheal disease among household members in Burao City, Somaliland
Bivariate Associations Between Environmental Exposures and Recent Diarrhea
Bivariate Associations Between Environmental Exposures and Diarrhea in the Past Two Weeks
Multivariable Analysis of Environmental and Household Factors Associated With Diarrhea
Multivariable Logistic Regression of Factors Associated With Diarrhea in the Past Two Weeks (n = 417)

Discussion
This study provides important insights into household- and environment-related determinants of diarrheal diseases in Burao City, Somaliland, a rapidly urbanizing and resource-constrained setting. The overall two-week household diarrheal prevalence of 7.1% highlights a persistent public health burden, despite relatively high reported access to improved water sources and sanitation facilities. Several modifiable exposure pathways were identified, including the absence of soap at household handwashing stations, presence of domestic animals in close proximity to households, visible environmental waste, low educational attainment of respondents, and a higher number of young children within households. Collectively, these findings underscore the need for integrated hygiene, environmental sanitation, and health education interventions in similar urban contexts.
The two-week diarrheal prevalence was 7.1% (95% CI: 5.0–10.0) among households in Burao, representing a significant public health concern in the region. Although comparative data from urban Somaliland are scarce, this study establishes a critical baseline for future monitoring and intervention efforts. Prior research focusing on children under five in Somaliland and Somalia has reported notably higher prevalence rates, such as 16.5% among internally displaced populations in Hargeisa and approximately 19.8% nationally.15,16 Our study’s inclusion of all age groups at the household level likely accounts for the lower overall prevalence compared to child-specific estimates; nevertheless, the burden remains considerable. Similar urban, resource-limited settings in sub-Saharan Africa have shown a range of diarrheal prevalence rates: 24.1% in the informal settlements of Nairobi, Kenya, 10 11% in peri-urban Ethiopia, 31 and 54.7% in slum areas of Accra, Ghana. 32 These variations reflect differences in sanitation infrastructure, hygiene practices, population density, and socioeconomic conditions across different contexts. This comparison emphasizes the ongoing challenge of diarrheal disease in rapidly urbanizing environments with diverse sanitation and environmental exposures, underscoring the need for tailored, context-specific interventions to effectively address its multifactorial causes.
The exceptionally strong association between the absence of soap at handwashing stations and diarrheal diseases represents one of the most critical findings of this study. Despite the high availability of handwashing facilities (97.2%), households lacking soap had markedly higher odds of diarrhea. These findings highlight that the mere presence of infrastructure is insufficient; rather, consistent access to essential hygiene materials is fundamental for disease prevention. Similar studies in comparable urban, resource-limited settings have reported strong protective effects of handwashing with soap against diarrheal morbidity, reinforcing the global evidence base for this intervention.33-36 However, the wide confidence intervals around our estimate reflect the relatively small number of households without soap (n=8), indicating some uncertainty in the precise magnitude of the association. Therefore, while the direction and significance of the effect are clear, caution is warranted in interpreting the exact strength of this relationship. In the context of Burao City, ensuring sustained soap availability remains a highly impactful and feasible public health strategy.
The presence of domestic animals in the immediate household environment was independently associated with an increased risk of diarrheal disease. This finding indicates a potential zoonotic and environmental transmission pathway, particularly in settings where humans and animals share living spaces or courtyards. Animal feces can contaminate household environments, water sources, and children’s play areas, facilitating the fecal–oral transmission of enteric pathogens. Similar associations have been documented in other low-resource urban and peri-urban settings, where close human–animal interactions elevate the risk of enteric infections, especially among young children.37-39 Studies in peri-urban Kenya and Ethiopia have reported an increased diarrheal risk linked to domestic animal exposure, highlighting the zoonotic transmission pathway in crowded living environments.40,41 Additionally, research in informal settlements in sub-Saharan Africa has emphasized how shared living spaces between humans and animals contribute to environmental contamination and pathogen persistence. 42 This body of evidence underscores the relevance of a One Health-informed approach, which emphasizes safer animal husbandry practices, improved separation of animal and human living areas, and enhanced environmental hygiene to reduce diarrheal morbidity in vulnerable populations.
Furthermore, the importance of Water, Sanitation, and Hygiene (WASH) programs cannot be overstated in combating diarrheal diseases. WASH interventions, including access to safely managed drinking water, improved sanitation facilities, and promotion of consistent hand hygiene practices, are fundamental components of effective diarrheal disease prevention strategies. Our findings, especially the strong association between the absence of soap and increased diarrheal risk, reinforce the critical role of WASH programs in ensuring functional hygiene infrastructure and behavior change. Integrating WASH initiatives with One Health approaches can provide a comprehensive framework addressing both environmental and zoonotic transmission pathways, thereby maximizing health benefits in urban, resource-limited settings like Burao City.
The association between visible garbage near households and diarrheal diseases further implicates environmental contamination as a key driver of disease transmission. In this study, households with visible garbage had 4.56 times higher odds of diarrheal disease (aOR = 4.56; 95% CI: 2.12–9.83), highlighting a substantial increase in risk. Accumulated solid waste creates favorable conditions for disease vectors and provides surfaces on which enteric pathogens can persist and spread through direct contact, particularly in children. 43 Similar studies in urban settings have reported comparable findings; for example, research in Ethiopia found that inadequate solid waste disposal was associated with a 3.8-fold increase in diarrhea risk, 44 while a study in Uganda reported a 4.2-fold higher odds of diarrheal morbidity linked to poor waste management. 45 In rapidly urbanizing cities such as Burao, where municipal waste collection services may be inconsistent or insufficient, visible garbage reflects broader systemic challenges in solid waste management. These quantitative parallels reinforce the need for comprehensive environmental sanitation strategies that extend beyond latrine coverage to address waste management as a critical component of diarrheal disease prevention.37,41
Households with three or more children under five years of age were also at a significantly higher risk of diarrheal disease. This observation is consistent with studies from other resource-limited settings42-45 and may be attributed to increased fecal load within the household, crowding, and difficulties in maintaining optimal hygiene amid intensive caregiving demands. Young children are particularly susceptible to enteric infections and may act as reservoirs for pathogens, thereby amplifying intra-household transmissions. 46 These findings suggest that child-focused hygiene promotion and caregiver support interventions are essential components of diarrheal disease prevention.
Lower educational attainment among respondents was independently associated with a higher odds of diarrhea, highlighting the role of health literacy and socioeconomic determinants in shaping hygiene behaviors. Education influences awareness of disease transmission pathways, adoption of preventive practices, and effective utilization of sanitation. This association is well documented in the literature47-50 and suggests that tailored health education interventions designed to be culturally appropriate and accessible to low-literacy populations could substantially reduce diarrheal risk.
A key strength of this study is its community-based design and the integration of structured household surveys with direct environmental observations. This approach allowed for a more objective assessment of sanitation and environmental exposure, reducing reliance on self-reported behaviors alone. The use of multivariate logistic regression, adjusted for potential confounders, further strengthens the validity of the identified associations.
This study has several limitations that should be acknowledged. The cross-sectional design limits causal inference, and temporal relationships between exposure and outcome cannot be definitively established. Although the sample size was adequate for detecting major associations, smaller effects may have been undetected. Residual confounding from unmeasured factors, such as household income, hygiene behaviors, or child feeding practices, may have influenced the findings. Although environmental observations, such as visible garbage and the presence of animals, were systematically assessed, some degree of observer subjectivity may remain. Some exposure categories contained relatively small numbers of households, particularly those without soap at handwashing facilities and households with three or more children under five, which contributed to wide confidence intervals and reduced precision of certain adjusted odds ratio estimates in the multivariate logistic regression analysis. Although the overall sample size was adequate for the primary study objectives, sparse observations in these subgroups may have affected the stability and precision of the estimates for less frequent exposures. This limitation should be considered when interpreting the strength of associations for these variables.
The public health implications of these findings are significant and require further investigation. Interventions in Burao City should move beyond infrastructure provision to ensure the functional availability of hygiene resources, particularly consistent access to soap and water for handwashing. Strengthening solid waste management systems, promoting safer human–animal interactions, and delivering targeted health education to less-educated households and families with multiple young children are critical measures. Community-based hygiene promotion, integrated with municipal sanitation services and One Health–oriented strategies, could significantly reduce the burden of diarrheal diseases in urban settings similar to this one.
Future research should employ longitudinal designs to clarify causal pathways and assess the effectiveness of integrated interventions that combine soap provision, improved waste management, and safer animal husbandry practices. Further exploration of the behavioral and socioeconomic barriers to sustained hygiene practices would also inform the design of more effective and context-specific public health programs in rapidly urbanizing regions of Somaliland.
Conclusions
This study highlights the significant burden of diarrheal diseases in Burao City, Somaliland, and emphasizes the critical role of household sanitation and environmental factors in disease transmission. The absence of soap at handwashing facilities, visible garbage near households, presence of multiple young children, and low educational attainment among household heads were identified as key preventable risk factors. These findings underscore the urgent need for integrated public health interventions that ensure functional hygiene resources, improve solid waste management, promote safer human–animal interactions, and target vulnerable populations through tailored health education and child-focused support. Addressing these modifiable factors through context-specific, multifaceted strategies is essential to reduce diarrheal morbidity in rapidly urbanizing, resource-limited settings such as Burao City, thereby improving overall community health and resilience.
Footnotes
Acknowledgements
We would like to thank the University of Burao School of Postgraduate Studies and Research Ethical Review Board for approving the ethical clearance and all the data collectors and supervisors who participated in this study. Finally, we thank the study participants, without whom this study would not have been possible.
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the School of Postgraduate Studies and Research at the University of Burao, Somaliland (reference number: SPGSR/UoB/29/25) prior to its implementation.
Consent to Participate
All participants were informed about the study’s purpose, procedures, potential risks, and benefits, and were assured of confidentiality and their right to withdraw at any time without penalty. Written informed consent was obtained from all literate participants prior to data collection. For illiterate participants, the consent form was read aloud in Somali by trained research assistants, and verbal consent was obtained in the presence of an independent witness who also signed the consent form to confirm the participant’s agreement. Independent witnesses were selected by the research assistants from community members unaffiliated with the study team and without any vested interest in the research. No participants aged <16 years were enrolled in the study. However, in accordance with ethical guidelines, if a participant was under 16 years of age, informed consent was obtained from their parent or legal guardian before participation. All study procedures involving human participants were conducted in accordance with the ethical standards of the institutional and national research committees and the 1964 Declaration of Helsinki and its subsequent amendments.
Author contributions
DKY served as the principal and corresponding author of this study. DKY designed the studyj, analyzed the data, interpreted the results, drafted the manuscript, and critically reviewed and approved the final version of the manuscript. MAH contributed to the study design, data collection, analysis, and interpretation of the results, and manuscript review. All authors reviewed the manuscript, agreed on the target journal for submission, and accepted responsibility for all aspects of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used in this study are not publicly accessible because of privacy concerns. However, interested parties may contact the corresponding author to request access to the data supporting the findings presented herein. These requests were evaluated on a case-by-case basis.