
Abstract
In this paper, the author explores the relevance of indigenous training from a cross-cultural perspective. We start by examining the broader context of traditional Western psychology and its relevance in a multicultural society. A brief description of the indigenous paradigm is followed by a discussion of differences between Western and indigenous psychology, and a proposal of cultural eclecticism as a potential frame for their integration. Next, we discuss the South African context in relation to comparative-cultural aspects of medical and psychological services.
The author’s clinical experience informs her increased awareness of culturally inadequate service at the state hospital, developing curiosity about African indigenous healing, and subsequent encounters and collaboration with African traditional healers. Ultimately, the author develops culturally sensitive training that explores cultural biases and generates cross-cultural knowledge and competence.
In conclusion, the author advocates that in the area of globalisation and multicultural societies, psychological training and clinical practice, should include dialogue and facilitate collaboration between Western and indigenous knowledge, hopefully leading to a more holistic and culturally inclusive service to a population of different backgrounds. Such collaboration and integration of Western and indigenous knowledge may be a source of professional stimulation as well as a benefit to health-care consumers.
Keywords
Western and indigenous psychology in a global context
Having limited relevance to other cultures, Disregarding and undermining alternative cultural traditions, Misconstruing the realities of other people by exoticising or disregarding psychologies that are non-Western, and Identities and conceptual repertoires of non-Western individuals are rendered obsolete.
Gergen et al. (1996) propose a multicultural psychology that celebrates the rich multiplicity of indigenous conceptualisations along with varying means of acquiring knowledge. To realise such a psychology, they suggest new forms of dialogue must be sought while remaining aware of the following potential pitfalls of such dialogue:
A strong commitment to any particular epistemology and methodology would be unproductive; An entry to a new dialogue would require that no single paradigm of psychological inquiry would be granted pre-eminence; and An attempt to improve or enlighten the other would be patronising.
For a dialogue to be more productive, Gergen et al. (1996) suggest several ideas:
A context should be made available for others to appropriate selectively, as their local circumstances invite; Western science should develop more capacity for diversity and pluralism and tolerance for ambiguity and the unknown; Honouring different traditions, from Western psychology to those existing in other cultures; and Inviting humility by appreciating the limitations inherent in any paradigm.
In Africa, and particularly South Africa, the relevance of Western psychology becomes questionable when we consider 2015 statistics: 80.5% of the South African population is Black, and only 8.3% is White (Statistics of South Africa, 2015). However, in 2004, and 10 years into democracy, only 18% of the psychologists registered with the Health Professions Council of South Africa (HPCSA) were Black (Duncan et al., 2004).
Indigenous cultures and knowledge have been impacted both positively and negatively by globalisation. Yankuzo (2014) points out that over the last two decades, the negative impact of globalisation on local cultures refers to a loss of traditional values. On the other hand, the positive effect of globalisation occurred through the mutual exchange between global and local cultures, initiating an increased global interest in traditional cultures and indigenous knowledge (Ginsburg, 2002). Traditional indigenous cultures offer knowledge that may have global relevance, such as a deep respect for self, for other people and for all of nature (Solomon & Wane, 2005) as well as sustainability and balanced, harmonious living, grounded in a spiritual relationship, which has been lost in our modern society.
Southern African indigenous cosmology is a tradition in which the spiritual and healing worlds are interlinked. Despite differences in geographical location, urbanisation and tribal affiliation, there are certain basic themes in African cosmology (Buhrmann, 1984):
Human beings are viewed as part of a holistic system that includes relationships with elements of nature and the supernatural. Ancestors play a significant role in African society. Rituals aim to restore balance and harmony in terms of the beliefs and values of the culture of the tribe. Dreams are one of the primary means of communication between the living and the ancestors. Traditional healers have a non-dualistic understanding of mind–body functioning.
The World Health Organization (WHO, 2002) estimates that, at present, more than 80% of the world’s population relies on traditional healing modalities for primary health care and wellness. The number of traditional healers in Southern African countries is consistently higher than the number of Western medical practitioners. For example, in 1995, South Africa had 200,000 traditional healers, compared to 25,000 doctors. It is estimated that between 60% and 80% of South Africa’s Black population consult a traditional healer before going to a primary health care practitioner.
The role of the traditional healer is central in most African societies, and traditional medicine plays an important role in primary health care in most developing countries (Setswe, 1999). In South Africa, many traditional healers practise in rural settings, but a growing number practise in developed urban locations, such as Black townships. In African cosmology, wellness is derived from the cultural understanding of the role of family, the community and the spiritual world in which traditional healers perform complex roles as social mediators and mediums between the spirit world and the living (Buhrmann, 1984).
Training to become a traditional healer (or sangoma) can take from a few months to a few years (Peek, 1991). To become a traditional healer, a special ‘calling’ from the ancestors is required, which may come through dreams, significant and severe sickness or a near-death experience. Traditional mastery is usually a secret, and part of the knowledge that the healer will pass onto their apprentice. A variety of treatments are used; for example, rituals, prayer, burning of incense, dance, herbal medication (muti), animal sacrifices, blood-letting, induction of vomiting, steaming, enemas.
Several significant differences between Western and indigenous psychology have been described by different authors (Mazzocchi, 2006; Nakashima & Roué, 2002). They argue that Western science and psychology tend to see itself as an objective science using a scientific approach, preferring quantitative analysis, focusing on rational experiences, and using intellect as the primary way of understanding.
Western psychology considers consciousness limited to the brain and has shown little interest about non-ordinary states of consciousness. Western science and psychology tend to rely on methods that investigate processes in isolation.
On the other hand, indigenous psychology and healing utilise subjective experiences: history taking would include community and ancestry using a model of explanation that is complex and holistic. Transmission of knowledge is oral and visual, which makes this approach narrative and intuitive. Indigenous psychology views the human mind as not limited to the brain; it integrates dreams and other extrasensory experiences as well as non-ordinary states of consciousness. Indigenous psychology’s nature of understanding is of one-ness; further, it examines phenomena in cultural and ecological contexts, which leads to inclusivity.
The author agrees with Valsiner’s (2009) suggestion that considering opposites may lead to uniting within the same whole and new forms of synthesis. Table 1 shows the opposite poles of traditional Western and indigenous psychology as a speculative layout, but the process eventually moves towards collaborative and dialogical relations, creating the potential for integration.
The contrast between Western psychology and indigenous psychology.
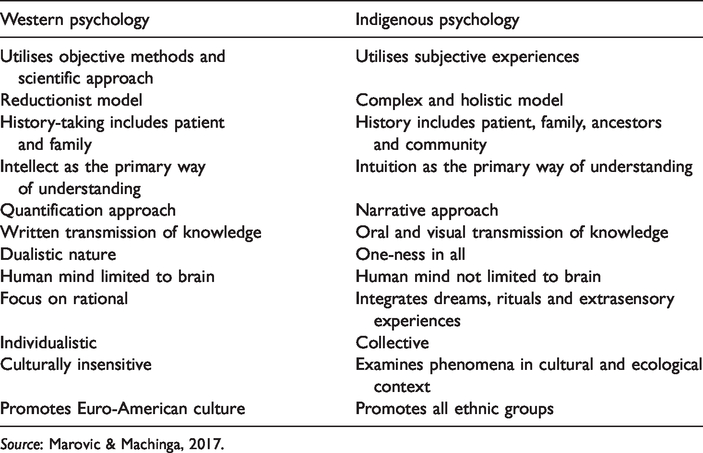
Source: Marovic & Machinga, 2017.
How to integrate Western and indigenous knowledge is an important question. Even though literature suggests that integration of indigenous knowledge is culturally relevant for health care and education, and for the development of environmentally harmonious healing practices, only a limited number of publications describe such integration (Pesek et al., 2006).
Craven et al. (2016) describe an integration of the Australian indigenous knowledge and positive psychology, which, according to them, leads to thriving. Their model of optimal human functioning, or thriving, proposes the interconnectedness of physical, educational, psychological and community aspects using principles of respect, relationships, reciprocity and responsibility.
In my clinical practice and training, I use eclecticism, more specifically technical and cultural eclecticism, as a preferred method of integration. Eclecticism is a conceptual approach that does not hold rigidly to a single paradigm but instead draws upon multiple theories and ideas to gain complementary insights into a particular situation. Technical eclecticism allows the therapist possibilities in selecting the best therapeutic method for the person and the problem (Lazarus et al., 1992). This route to integration is guided by empirical data on the efficacy of different methods. Technical eclecticism encourages the use of diverse strategies without being hindered by theoretical differences, but, in order to practice technical eclecticism, the therapist must develop competence in a number of different trainings and techniques.
In a similar fashion, cultural eclecticism refers to knowledge used from a particular cultural source that might not necessarily subscribe to the theories that spawned them. A culturally eclectic health service requires competence in diverse cultures to appropriately harmonise cultural knowledge with the culture of the person and the problem. For example, knowledge of the African indigenous paradigm might be useful when working with a person from an African background. In addition, African indigenous psychology may offer more hope to a patient in certain clinical situations. From the patient’s perspective, the African paradigm offers a positive view of the symptoms as potential of calling to become a healer, compared to the Western approach of getting a psychiatric diagnosis, the stigma associated with it, and a possible admission to a psychiatric institution.
Feedback from my clients of African origin suggests that they feel more comfortable with a therapist who has knowledge of the indigenous African system from which they come. African clients also comment on the fact that such knowledge shows that their therapist has interest in and respect for their culture. In addition, when clinically appropriate, I have discussed the African paradigm of calling to become a healer with non-African clients with mental health symptoms. For a client that does not believe in psychiatric treatment, it may open more positive possibilities than a psychiatric approach.
Ultimately, I suggest that developing cross-cultural competence helps to deepen the connection and the bond between therapist and client when the client is coming from a different cultural background to the therapist. Further, if we consider a patient-centred or family-centred model as the future of health care, cultural eclecticism may provide health care consumers with more treatment options and better care.
Valsiner's point (2019) that the potential future of cultural psychology depends on building models of dialogical relationships in otherwise socially asymmetric role relations holds the truth. Creating a platform for dialogues in asymmetric relationships such as between psychologists and indigenous healers would be a step towards re-positioning Western psychology into a dialogically equal relationship with indigenous psychology. Such a process reflects an important consideration; namely, that we need constructs that apply to all humans but retain cultural uniqueness (Yang & Lu, 2007). In addition, introducing indigenous knowledge into training may build an appreciation that indigenous (African or other local) knowledge has to offer to health care.
In the next part, the reader becomes acquainted with the South African context, cross-cultural challenges and a trial and error process that the author has faced in developing cross-cultural training that encourages dialogue and collaboration between psychologists and indigenous healers.
South African psychology in a global context
South Africa is culturally, linguistically and ethnically diverse, embracing many cultures, customs and 11 official languages (Berg, 2012). The concept ‘culture’ has carried multiple meanings in the South African context, having been associated with race, ethnic identity, Afrocentrism, historical tradition, material deprivation, poverty, and often that, which is not Western or Eurocentric (Eagle, 2005).
Since the National Party came to power in 1948, the apartheid ideology advocated total racial segregation, entrenching and expanding existing colonial segregation, and White minority domination. Hence, it is no surprise that South African psychology has been grappling with culture, ethnicity and diversity (Burke, 2006). Further, psychology academia was used for developing racial theories in compliance with the discriminatory social–political context, while membership in the South African Psychology Association (SAPA) was exclusively White (Burke, 2006).
In 1994, shortly before the birth of democracy in South Africa and the release of Nelson Mandela, the Psychological Society of South Africa (PsySSA) was formed. Although racial tensions are still present, this propelled a move in South African psychology towards the development of more diverse psychology, and the encouragement of local, Afrocentric and indigenous influences (Dawes, 1998). Van der Merwe (1996, p. 77) describes South Africans as ‘late-comers to the intellectual scene of multiculturalism, while at the same time perhaps forerunners in the experience of multi-culturality’.
The development of culturally appropriate services concerning indigenous cultures was virtually non-existent in South Africa and globally. At present, the leading country in that respect seems to be Australia. For example, The Australian Indigenous Psychologists Association (AIPE) has established and delivered an impressive 82 cultural competency workshops to 1125 non-indigenous mental health workers since 2010: www.indigenouspsychology.com.au/workshop/about-the-workshops/.
Psychology training in South Africa has significant British influence (Eagle, 2005). Mkabela (2005) and Dawes (1998) point out that South African formal education did not adequately refer to indigenous African education, and propose engaging with neglected African indigenous knowledge. Edwards (2011) suggests that indigenous constructs and knowledge may provide a fertile ground for future generations of psychologists, teachers, researchers and practitioners.
South African clinical psychology demonstrates relevant research related to the cultural relevance of psychological tests and health psychology (Johnston, 2015). However, there is a dire need for training in cultural sensitivity and the development of multicultural counselling competencies (Ngcobo, 2002). Cross-cultural encounters and training described as follows were the first of their kind approved by the Professional Board of Psychology for continuing professional development (CPD) purposes. CPD is the process by which health professionals keep updated to meet the needs of patients, the health service and their own professional development. CPD has been introduced as mandatory in South Africa across the health professions.
One of the issues relating to the cross-cultural barrier was a language problem. Hall (1966) advocates that people from different cultures not only speak different languages but also ‘inhabit different sensory worlds’ (p. 2). Most patients seen at the state hospital were African, and many were from rural areas. They spoke different African languages and – very occasionally – English. On the other hand, the majority of medical and psychology staff employed by the state hospital were White and English-speaking. It was common practice during medical and psychological interviews and assessments to ask one of the African nurses to translate. One can imagine that a lot was lost in translation.
An important cross-cultural issue my colleagues and I have faced was a discrepancy between how we, as Westerners, understood illness, causes and treatments, in contrast to the majority of Black patients. Most Western-trained clinicians had no knowledge of the African indigenous healing paradigm, which left us perplexed about patients’ perspectives. They would describe bewitching, ‘evil eyes’, unhappy ancestors or ‘calling’ to become a traditional healer as reasons for sickness.
The majority of staff had a belief that the treatment we offered is scientific while African is primitive. Because state patients had little education and grew up in poverty, a somewhat hierarchical position was taken by most of the staff. Patients were treated like children who do not have the ability to understand, hence no need to even attempt to explain medical advice. Instead, the expectation was that they should do what they were told. In retrospect, I wonder, how such a superior attitude was affecting the recovery of patients.
In the early 1990s, I had no exposure to African indigenous knowledge, and like most Western-trained health professionals, I considered it to be primitive magical thinking.
However, in 1995, a case I dealt with caused a shift towards curiosity about African indigenous healing. The paediatric department referred a nine-year-old Black African boy who had suffered from severe epileptic attacks since early childhood. Despite paediatric neurologists trying different medication, very little improvement was achieved. When I saw the family and discussed options moving forward, they shared with me that they are considering taking their son to a local African traditional healer.
Considering that our medical knowledge failed and we had little to offer going forward, I had no issue with the family seeking help elsewhere. To my surprise, a month later, the family arrived for their appointment looking cheerful and informed me that their son is much better. He had had only one epileptic attack in a month, which was a significant improvement compared to daily attacks in previous months. The electroencephalogram, a test that records the electrical signals of the brain, showed significant improvement, leaving our medical staff puzzled. The family asked me to keep quiet about my knowledge of the traditional treatment because of the medical staff’s potential prejudices. During follow-ups the next year, the boy remained well, with very few epileptic attacks in between.
In 2009, a close friend introduced me to a Black African professional woman who was also a practising traditional healer (see Figure 1). Our collaboration created a platform for the introduction of indigenous knowledge into training and initiating cross-cultural dialogue between psychologists and traditional healers.

Author and sangoma, at the sangoma’s sacred hut (ndumba).
Cross-cultural indigenous training
Indigenous cross-cultural competency training is defined as training that assists organisations and individuals to better understand indigenous histories and cultures. The indigenous training I developed was a CPD course; participants were a small group of 10 -12 White psychologists, and the majority were female. Most participants had limited knowledge of indigenous healing systems and no personal experiences with African traditional healers.
There are two relevant aspects of cross-cultural indigenous training: format of the training and its content.
Participatory training format: The training format used for cross-cultural training was participatory and experiential learning combined with group dialogue and personalised experiences. Numerous authors suggest such a format as the most constructive (Ahmed et al., 2011; Gudykunst et al., 1996).
Cross-cultural competence: Over several years, the training content evolved using Campinha-Bacote’s model (1998) of cultural competence as a process in which health care providers are becoming culturally competent rather than already being culturally competent. The training focused on five relevant constructs of cultural competence in health care:
1. Cultural desire was evidently demonstrated by participants’ motivation to attend training and to engage in the process of becoming culturally skillful.
2. Cultural encounters refers to the process that encourages the health care provider to engage in cross-cultural interactions with clients from culturally diverse backgrounds (in this training, the engagement was between Western health care providers and indigenous health care providers). Cultural encounters are relevant in enhancing cultural sensitivity and helping address cultural biases (Ngcobo, 2002).
The author proposes another relevant aspect to enhance such encounters:
Familiarity: Creating an element of familiarity, especially during the initial encounters, might be of importance. Otherwise, there is a possibility that the encounter might lead to a negative experience. For example, the choice of a typical traditional healer might be risky, as Western participants would have difficulty relating to a person who seems so different to them. On the other hand, the choice of a traditional healer who had a number of qualities that resonate with Western participants, such as professional appearance, academic education and corporate position, would increase the sense of familiarity.
3. Cultural knowledge refers to obtaining information about different aspects of culture. For example, the traditional healer presented the relevant concepts of African traditional healing (see Buhrmann, 1984, p. 6), and at that point, she also changed her appearance to traditional African healers’ clothes (Figure 2).

Traditional healer introducing African indigenous cosmology to a group of psychologists.
4. Cultural skills relate to learning how to assess the cultural data of patients. A cultural genogram (see further below) was used as a cultural assessment tool as well as work on self-of-the-therapist (Hardy & Laszloffy, 1995).
5. Cultural awareness is self-examination of own culture and biases. Participants used a cultural genogram to promote cultural awareness and gain a greater appreciation for how culture impacts their role as therapists and influences the lives of clients in treatment. Exploration of the cultural genogram helped participants clarify the influence that culture had on their family system and cultural identity. This also encouraged discussions on cultural stereotypes (Hardy & Laszloffy, 1995).
As discussed before, Western professionals held many biases towards indigenous knowledge, but other way was true too.
Indigenous communities’ bias: Indigenous healers grew up in oppression during the apartheid years; hence they had negative and suspicious views of Western medicine and psychology. The author’s experience suggests that continuous and open engagement with indigenous communities may help to address some of the fears and biases they may hold about Western knowledge. For example, in 2012, as a result of positive collaboration with traditional healers, I was the first White psychologist to be invited to present at the Annual Traditional Healers’ Conference in Mamelodi, a Black township. My first talk was on spirituality and mystical experiences in front of a large audience of indigenous healers. Initially, my talks were met with apprehension, but over a few years, the attitude changed to curiosity and an appreciation. As a result, I have been invited numerous times to the annual traditional healers’ conferences, and I have presented on a variety of subjects, from mental health disorders to stress management, mindfulness and quantum psychology (Figure 3).
The author at the Annual Traditional Healers’ Conference in Mamelodi.
The author proposes two other relevant concepts that may hold value for cross-cultural training:
Vulnerability is an essential element of human connection and including an aspect of vulnerability in cross-cultural training, may enhance cross-cultural awareness by initiating empathy and potentially lessening cultural biases. For example, I asked an indigenous healer to share her personal story – her ‘calling’ – which started with mental health problems and diagnosis. She told participants of a dream, in which the ancestors told her that she must start training as an African traditional healer. After successful completion of her training a year later, her symptoms of mental problems disappeared. During my presentations at the indigenous healers’ conferences, I also shared my struggle with cultural issues at the state hospital. It is the author’s experience that sharing vulnerability seems to engage participants on a more personal level, and may help to break down biases.
Breakdown of the typical classroom structure and the relevance of nature in cross-cultural training have been informed through many years of facilitating retreats for clients in the mountains near Johannesburg. The result of these retreats is positive feedback on how nature and open spaces promote shift and transformation of outdated mental and emotional patterns. Beautiful outdoor space and nature, instead of a classroom set-up, was used for a dialogue between psychologists and indigenous healers, with the idea that it would promote openness and curiosity (Figure 4).

Dialogue between indigenous healers and psychologists at Nirox Art Foundation Park at The Cradle of Humankind, South Africa.
Training feedback forms were anonymous, and the overall value and quality of the workshop were marked as very high. Below are some of the comments:
“Awesome! I learned a lot and can’t wait to learn more and expand on my journey as healer.” “Fantastic experience. Thank you for facilitating this space. Please do more on alternative and indigenous knowledge.” “Very different workshop. Would’ve liked more theoretical input on indigenous healing.” “Lovely experience! Thank you. Perhaps more examples of working with clients from different backgrounds and how to use this knowledge in clinical settings would be useful.” “The highlight for me was a talk by sangomas and dialogue with them. Would’ve liked more time for discussion and questions.”
Conclusion
The cross-cultural encounters, training experience and feedbacks discussed above confirm the value of developing cultural sensitivity and competence for clinicians. Some important points that should be considered for the future of clinical training in multicultural societies with indigenous populations are:
Cultural encounters create valuable experiences that may increase cultural sensitivity and competence. When encounters include a high level of difference to participants’ own culture, it might be useful to consider introducing elements that have some comforting aspects to participants’ own culture. Cultural eclecticism and knowledge of other cultures may increase clinicians’ ability to relate to clients from different cultures, as well as increase clients’ appreciation of a therapist who shows a desire to learn about a different culture. Training where clinicians are encouraged to share examples of cultural biases, difficult cases, failures and mistakes related to cultural aspects, may have a positive effect on clinicians’ cultural competence. Future clinical programmes, especially in countries that have indigenous populations, should create platforms for cross-cultural dialogues between Western and indigenous health care practitioners (an example: Western psychologists and African traditional healers). The introduction of such programmes would create a bridge between mainstream and indigenous psychology, and potentially shape mainstream psychology as culturally more applicable and sensitive. In order to develop an appreciation of indigenous (and other) cultures and prevent biases, consideration should be given to an early exposure to other cultures, and positive experience developed via cross-cultural programmes aimed not only at an academic level but as early as at preschool and primary school level. There is a need for qualitative and quantitative research that investigates the benefits of cross-cultural training and the relevance of indigenous psychology and training.
In respect of challenges, one global challenge is the increased number of economic and political immigrants moving from the African and Indian continents to the First World countries. Cultural biases, misunderstandings and racially and religiously motivated violence are becoming common aftermaths of such migrations. Therefore, platforms for dialogues and cultural bridges are going to be critical globally if we are to move forward in a participatory process. Further, clinical training that integrates indigenous and cross-cultural dimensions has more to offer in today’s multicultural societies.
Another global challenge is an ecological crisis, as well as crises of resources and sustainability issue. The author agrees with Nakashima et al. (2000) that indigenous knowledge and an understanding of plants and animals can potentially offer knowledge on how to live sustainably.
Finally, there is a challenge in appreciating the fact that during the training, both psychologists and indigenous participants have shown evidence of cultural biases. While efforts should certainly be focussed on sensitising Western clinicians towards indigenous knowledge and culture, it may be equally important to consider addressing biases that indigenous (and other) populations hold about Western knowledge, which they historically experienced as oppressive. In the author’s experience, collaboration between herself and indigenous healers led to the breakdown of some of their held biases towards Western psychology.
In conclusion, Western psychology needs to develop an awareness of the value that indigenous constructs and research methodology may offer. If we embrace the need for psychology that is culturally sensitive, then indigenous psychology becomes a relevant addition to understanding people in their cultural context and assisting the development of society-wide compassion towards other cultures. Indigenous cosmology and concepts such as relationality, multilevel interconnectivity, spirituality and ecological sacredness offer a unique contribution and ancient wisdom that may be vital for addressing some of the current global challenges.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.