
Abstract
Objectives
Successful partnership working has theoretically been linked to improvements in service delivery and is dependent on the strength of the partnership, trust, communication, professional roles and resource sharing. Empirical evidence to confirm the relationships between these factors and improved service provision, however, is lacking. Our aim was to assess the views of staff as to the conditions required for partnership working.
Methods
This study was a cross-sectional survey of 687 staff offering sexual health education, information or support to young people in the Healthy Respect intervention area in Scotland. Views of each variable were scored and structural equation modelling was used to assess the theoretical model.
Results
Responses were received from 284 (41%) staff. Greater strength of partnership was directly associated with increasing the number of referrals. Establishing professional roles between organizations was also associated with increasing the number of referrals. Strength of partnership was indirectly associated with working more effectively with young people and this relationship depended on clear communication, trust, established professional roles and shared resources. Effective partnership working depends on a number of interdependent relationships between organizations, which act synergistically to improve organizational outcomes.
Conclusions
Effective partnership working leads to improved service delivery though there is a need for better controlled studies which demonstrate the effect on health outcomes.
Introduction
Partnership working between organizations tends to be regarded as ‘a good thing’ in the quest to improve the health of the public.1,2 The literature describes the virtues of partnerships, including capability and capacity building, rationalization of resources, a reduction in duplication of effort, less organizational fragmentation, improved communication between agencies, and a better understanding and responsiveness to health needs.3–5 Whilst potential benefits are abundant, they are rarely assessed.1,2,6
Partnership working has been referred to as a terminological quagmire with no agreed definition. 3 Our definition is based on a substantial body of theoretical work from the health and organizational literature which describes the conditions that are necessary for successful partnership working as well as its key outcomes: trust, the consensus being that although it is possible to work jointly with little trust between partners, the most successful partnerships are based on considerable mutual trust;2,7–9 clear, consistent communication; commitment of each partner;9–13 intensity; intimacy (mutual confiding); reciprocity; and time. 14 The model we adopted is based on the hypothesis that effective partnerships should lead to better services and better outcomes for service users. 6
Most of the existing evidence refers to how partnerships function (the process) rather than the outcomes for staff, service users or other stakeholders.1,15,16 There are several challenges in assessing the contribution of partnership working to outcomes. 17 Visible changes in population level outcomes may take longer than the lifetime of many of the partnerships including improvements in health. Some authors argue that evaluating the effects of partnerships on population outcomes may not be prudent, given the minimal understanding of the mechanisms by which they operate.17,18
Our aim was to assess a theoretical model of the conditions associated with successful partnership working (trust, communication, strength of partnership, establishing professional roles between organizations, pooling resources) and the extent to which these were associated with two intermediate organizational outcomes namely, increasing referrals to specialist organizations and working more effectively with young people.
Methods
The research was conducted as part of an evaluation of the impact of a National Health Demonstration Project (Healthy Respect) in an area of Scotland, which aimed to improve the sexual health of young people. It encouraged partnerships between the three main service sectors, namely the National Health Service (NHS), local authorities and the voluntary sector. The partnerships were based on agreements between agencies rather than structural or legal changes between agencies. Healthy Respect was a complex intervention developed over eight years. It comprised theory-based school sex education linked to sexual health services which operated either in or near to schools. It also involved a communications strategy which included extensive media campaigns and branding. The programme was compared with other areas in Scotland where standard sex education was provided. This comprised mainly information giving with sexual health services less available and not linked to schools and no communication strategy or branding. 19
Study design
A cross-sectional survey was conducted with staff providing sexual health education, advice or services for people aged 10–18 years old in the area targeted by Healthy Respect. The survey, conducted in 2008 at the end of the demonstration period, invited 687 professionals to take part. Most (approximately 80%) were identified by the Healthy Respect team, and the remainder identified by the research team. Those contacted by the research team were identified through an independent search for organizations. A number of methods were used consisting of a search of information web-sites, Google searches, local knowledge and professional contacts. We contacted each organization and asked them to confirm whether they offered sexual health education, advice or services to young people. Once an organization confirmed they did so, they were contacted again, through a senior manager, and were asked to provide a list of staff who worked with young people. All were sent a self-completion questionnaire.
Measures and analytical approach
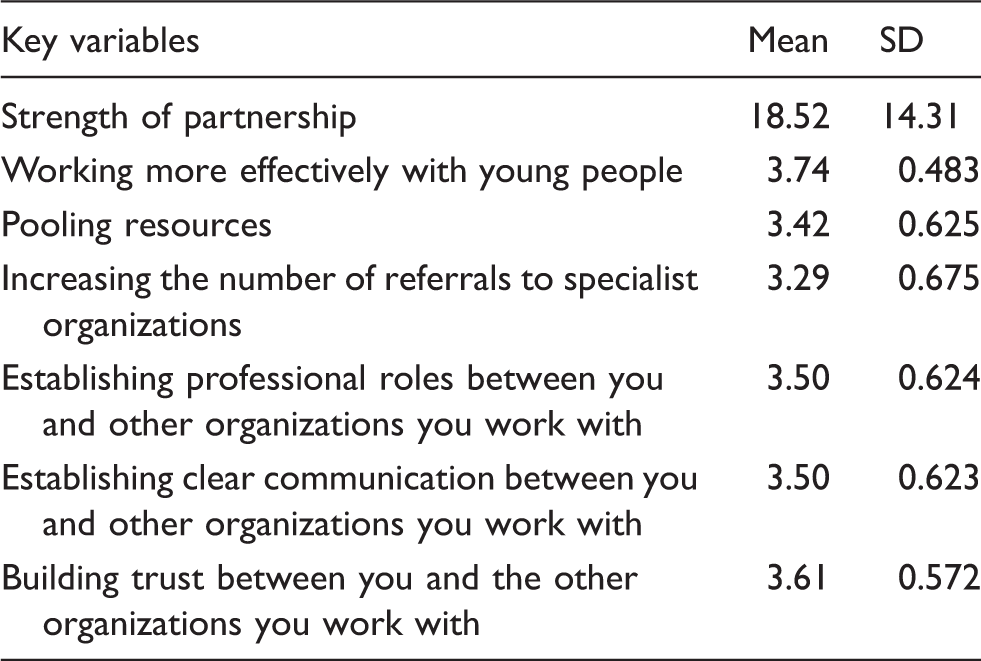
The questionnaire gathered data on the participants' links with other relevant organizations, the importance of these links and how these links affected partnership working in six areas: establishing clear communication; building trust; establishing professional roles; pooling resources; increasing the number of referrals; and working more effectively with young people. A Likert scale was used to measure the effects of partnership working (1 = Made it worse to 4 = Helped a lot). The strength of partnership working was determined by constructing a score from:
The frequency ( f ) of the contact they had with each organization (daily = 4, weekly = 3, monthly = 2 or less frequently = 1) The importance of the relationship (I) with each respondent (not important = 1, of little importance = 2, important = 3 or very important = 4).
The strength of Partnership score =
Structural equation modelling
Structural equation modelling (SEM) was used to test the relationship between all the variables (described above). SEM is a statistical modelling technique which combines factor analysis and regression or path analysis. 20 The relationships between the variables are represented by path coefficients. Structural equation models are visualized using a path diagram. As a means of examining the inter-related relations, path modelling20–23 was applied using AMOS 19. 24 In this modelling process, all links, including reciprocal links, were investigated and various sub models produced. These were compared on grounds of goodness of fit and of parsimony.
Results
Summary scores of key variables.
Pearson correlation coefficients of key variables.
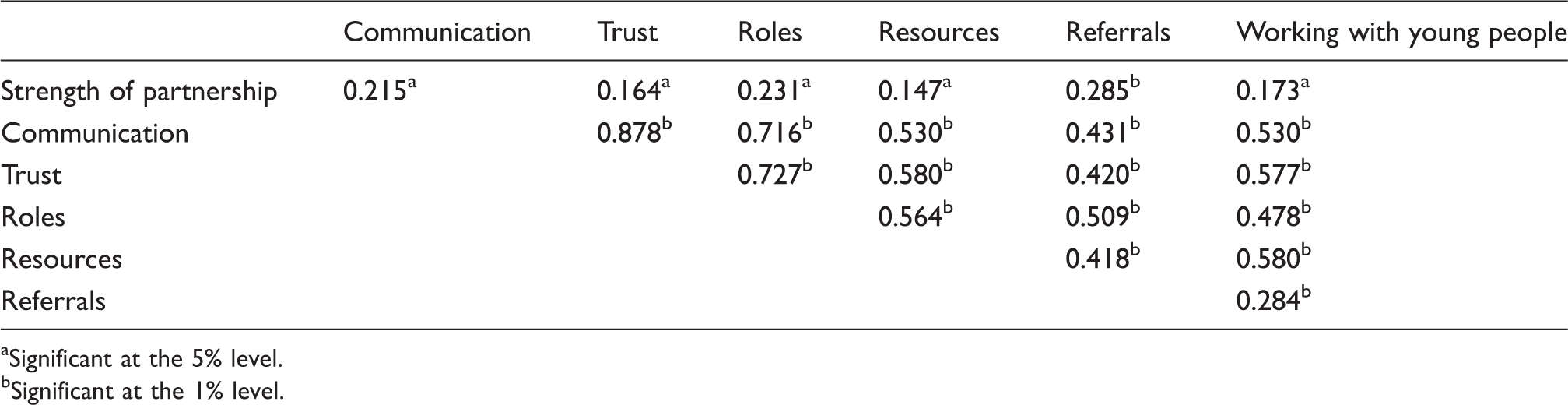
Significant at the 5% level.
Significant at the 1% level.
The final model is presented in Figure 1 in which, for clarity, only significant links are presented. Rectangles are the variables. The arrows indicate the direction of the paths and the figures on the arrows are the slope of the regression line between the variables. Figure 1 presents the standardized estimates of the coefficients and the absolute magnitude of these indicate the relative strength of the association between variables on the paths. The slope coefficients and their significances are displayed in Table 3.
Path model of effects on final outcomes. Regression weights of slope coefficients.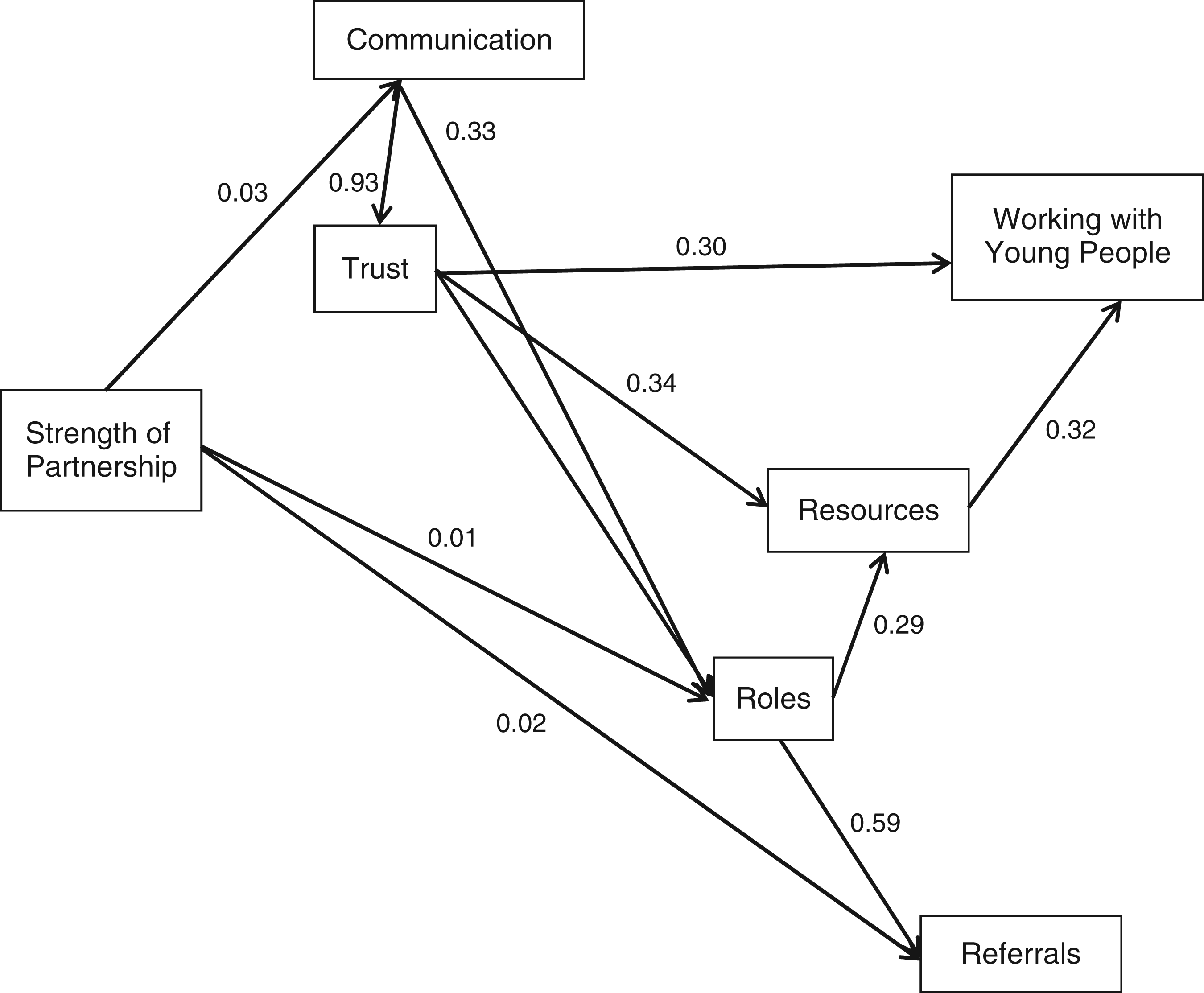

This model fitted well with a comparative fit index 25 (CFI) of 0.997, a CMIN/DF of 1.227 and an RMSEA of 0.028 compared to the independence model of 0.329. Greater strength of partnership was directly associated with increasing the number of referrals. It was not directly associated with working more effectively with young people. Strength of partnership was indirectly associated with working more effectively with young people and this relationship depended on clear communication, trust, established professional roles and shared resources. Strength of partnership did, however, have an indirect effect on working more effectively with young people by enhancing professional roles and communications which, via encouraging sharing of resources, became associated with more effective working with young people. Trust was a key component of the model and was integral to partnership working.
Discussion
Effective partnership working comprises a number of interdependent relationships between organizations which act synergistically to improve outcomes. For example, the strength of the partnership between staff in different organizations not only has a direct effect on referrals but it also requires improved communication, trust, established professionals' roles and shared resources to help staff work more effectively with young people. These findings support the theoretical hypothesis that effective partnership working leads to improved service delivery. 6
Although there is evidence that partnership working has led to improvements in service delivery in other areas of health care, in particular care for the elderly,26 this is the first time this has been assessed for sexual health services. However, we do not have proof of effect. For example, the outcomes were based on self-reports and these were not linked to objective measures such as records of referrals or sexual health outcomes. However, surveys conducted with young people as part of the wider evaluation of Healthy Respect indicated an increase in the use of sexual health services amongst those exposed to the intervention. 19 Improvement in the sexual health of boys compared to girls was also noted. 19
There was a 41% response rate to the survey. Although respondents represented staff from diverse organizations it is not known whether the responses were representative. This could have led to more optimistic results by excluding the views of those less committed to partnership working. There is also the need to design studies which compare partnership working with a control condition. This presents a significant challenge in terms of choosing a suitable comparator. Partnership working represents one approach to improving health care but whether it adds any additional benefit over other interventions such as financial incentives or legislation, is unclear.
As regards future research, quantitative studies could be enhanced by qualitative research into the context and mechanisms which underpin partnership working. For example, in-depth interviews with service providers and policy makers suggested that Healthy Respect was important in encouraging strategic partnerships and strengthening links between sexual health services and schools. 19 Thus, there is scope for research which substantiates the causal link between partnership working and improved outcomes for organizations and those who use their services. Studies also need to incorporate an economic component which examines the cost effectiveness of partnership working.
Footnotes
Funding
This study was funded by NHS Health, Scotland; the Wellcome Trust Clinical Research Facility, Edinburgh, UK; and the Centre for Integrated Healthcare Research Edinburgh, UK.
Acknowledgements
We are grateful to the funding organizations and to two reviewers for their support.