
Abstract
Objectives
New and emerging health technologies (innovation outputs) do not always reflect conditions representing the greatest disease burden. We examine the role of research and development (R&D) funding in this relationship, considering whether areas with fewer innovative outputs receive an appropriate share of funding relative to their disease burden.
Methods
We report a retrospective observational study, comparing burden of disease with R&D funding and innovation output. UK disability-adjusted life years (DALYs) and deaths came from the World Health Organization (WHO) 2004 Global Burden of Disease estimates; funding estimates from the UK Clinical Research Collaboration’s 2006 Health Research Analysis; and innovation output was estimated by the number of new and emerging technologies reported by the National Institute for Health Research (NIHR) Horizon Scanning Centre between 2000 and 2009.
Results
Disease areas representing the biggest burden were generally associated with the most funding and innovation output; cancer, neuropsychiatric conditions and cardiovascular disease together comprised approximately two-thirds of DALYs, funding and reported technologies. Compared with DALYs, funding and technologies were disproportionately high for cancer, and technologies alone were disproportionately high for musculoskeletal conditions and endocrine/metabolic diseases. Neuropsychiatric conditions had comparatively few technologies compared to both DALYs and funding. The relationship between DALYs and innovation output appeared to be mediated by R&D funding.
Conclusions
The relationship between burden of disease and new and emerging health technologies for different disease areas is partly dependent on the associated level of R&D funding (input). Discrepancies among key groups may reflect differential focus of research funding across disease areas.
Introduction
Conditions representing the greatest disease burden in the population are not always reflected in the number of health technologies marketed or in the development pipeline. We have previously reported that innovation is disproportionately strong in cancer and non-ischaemic heart disease, and disproportionally weak in mental health when compared to disease burden. 1 This study aims to explore these findings further by examining the role of research and development (R&D) funding in the relationship between burden of disease and innovation.
Sir David Cooksey’s review of UK health research funding (2006) recommended that health research priorities and allocation of public funding should be informed by the impact of diseases on the population and economy. 2 The World Health Organization (WHO) Global Burden of Disease study3,4 reported deaths and disability-adjusted life years (DALYs) for 192 states to provide a global account of mortality and loss of health by cause. In high- to middle-income countries, including the UK, cardiovascular diseases and cancers accounted for the greatest proportion of deaths, with neuropsychiatric and sense organ disorders accounting for around one-third of years lived with disability. This is, to an extent, reflected in UK health care policy. The Cancer Reform Strategy (2007) 5 and Dementia Strategy (2009) 6 indicate a focus on these particular areas, which were also among the WHO’s priority medicine needs in terms of innovation. 7
However, although cancer, cardiovascular disease and neuropsychiatric conditions together attract the most R&D funding, 8 there are discrepancies within these wider disease groups that suggest funding is not being allocated according to need. The UK Clinical Research Collaboration (UKCRC) 8 reported that in 2004/2005 cancer received a disproportionately high level of governmental and charity R&D funding relative to its burden, with blood system disorders, cardiovascular diseases, stroke and mental health being comparatively underfunded; their more recent analysis indicated similar patterns for 2009/2010. 9 This is supported by another UK study showing that R&D for dementia and stroke are severely underfunded compared with cancer and coronary heart disease. 10 In the United States, burden of disease is a weak predictor of funding by the National Institutes for Health, with DALYs explaining just a third of the variance in funding. HIV/AIDS received the most funding in relation to its burden, and depression received the least. 11 Innovative outputs from research generally follow a similar trend; a disproportionately high number of health technologies (including drugs, devices, diagnostic products, procedures, programmes and settings) are developed for cancer relative to its burden, and a disproportionately low number for neuropsychiatric conditions. 1 This is also the case for medicinal products approved for use in the European Union; between 1995 and 2009 infectious/parasitic diseases and blood/endocrine disorders were among the most over-represented groups, and cardiovascular disease among the most under-represented, relative to population disease burden. 12
This study examines whether differences in R&D funding across disease areas can explain the apparently weak association between innovation and burden of disease using new and emerging health technologies reported by the National Institute for Health Research Horizon Scanning Centre (NIHR HSC) in England as a measure of innovation output. 1 The NIHR HSC informs key policy- and decision-makers in the National Health Service (NHS) about health technologies that may be important for patients or health service provision in the near future.1,13
Methods
Measures
Burden of disease was defined as deaths and DALYs for the UK, taken from the WHO 2004 Global Burden of Disease estimates. Research funding estimates for 2004/05 were taken from the UKCRC’s 2006 Health Research Analysis. 8 This used data from the 11 largest government and charitable organisations funding health-related research in the UK, including the Health Departments of the UK devolved nations, four research councils, and the three largest medical research charities. Innovation output was measured by the number of new and emerging technologies reported by the NIHR HSC between 2000 and 2009. 1
Classification of disease groups
Diseases were grouped according to the second level of the four-stage hierarchy used in the WHO Global Burden of Disease studies.3,4 This comprises 21 broad groups, including malignant neoplasms and cardiovascular disease. For the purpose of comparison, we grouped these further into the 14 health categories used in the UKCRC analysis. For example, ‘unintentional injuries’ and ‘intentional injuries’ were combined in a single ‘injuries’ category.
Assigning reported technologies to disease groups
Of all the technologies reported by the NIHR HSC between 2000 and 2009, 77% were drugs, 9% devices, 8% diagnostics, 3% procedures, and <1% programmes. The remainder were unspecified. We assigned technologies to health categories according to their associated indications (e.g. ‘vaccine for herpes zoster’). The ICD-10 and Annex 3 of the Global Burden of Disease 2004 Update were used for reference. Technologies whose indications could not be linked to specific diseases (e.g. contraception, smoking cessation and general wound care) were not coded. Technologies with more than one indication received separate codes for each health category. 1
Statistical analysis
We used the steps proposed by Baron and Kenny (1996) 14 to determine whether there was a mediating effect of R&D spend on the relationship between burden of disease and reported technologies. Firstly, Pearson’s bivariate correlation coefficients (r) were calculated for each combination of independent variable (burden of disease: DALYs/deaths) and dependent variables (technologies and R&D funding) (SPSS Statistics v19.0, IBM). Fisher’s z transformation was used to calculate 95% confidence intervals for each value of r. Secondly, regression analysis was conducted using DALYs as the sole predictor of reported technologies, and thirdly, the regression analysis was repeated using both DALYs and R&D funding as predictors of reported technologies in the same model.
Results
Descriptive statistics
Of the 549 unique technologies reported by the NIHR HSC, 18 (3.3%) could not be coded and were therefore excluded. This left 531 unique technologies with 540 individual indications.
Three main categories (cancer, neuropsychiatric conditions and cardiovascular disease) combined made up approximately 60% of DALYs, R&D funding and reported technologies, and over 70% of deaths (Figures 1 and 2; Table 1). Compared with DALYs, R&D funding and the number of technologies were disproportionately high for cancer, whereas neuropsychiatric conditions had comparatively few technologies despite representing the most DALYs and ranking second for funding. Musculoskeletal conditions and endocrine/metabolic diseases had relatively high numbers of technologies compared with DALYs and R&D funding. Infection and cardiovascular disease ranked similarly for R&D funding, despite the latter ranking much higher for DALYs and technologies. Respiratory conditions and injuries had low R&D funding and numbers of technologies relative to DALYs.
Proportion of all UK DALYs, R&D funding and reported technologies by health category (10 leading DALY causes). DALY: disability-adjusted life year; WHO: World Health Organization; R&D: research and development; UKCRC: UK Clinical Research Collaboration; NIHR HSC: National Institute for Health Research Horizon Scanning Centre. Proportion of all UK deaths, R&D funding and reported technologies by health category (10 leading death causes). WHO: World Health Organization; R&D: research and development; UKCRC: UK Clinical Research Collaboration; NIHR HSC: National Institute for Health Research Horizon Scanning Centre. Health categories ranked by proportion of all reported technologies (number, %), with associated rankings for DALYs (‘000 s, %), deaths (‘000 s, %) and R&D funding (%). Notes: DALYs: disability-adjusted life years; R&D: research and development. Permission to display % of funding only; data on actual funding used in calculations.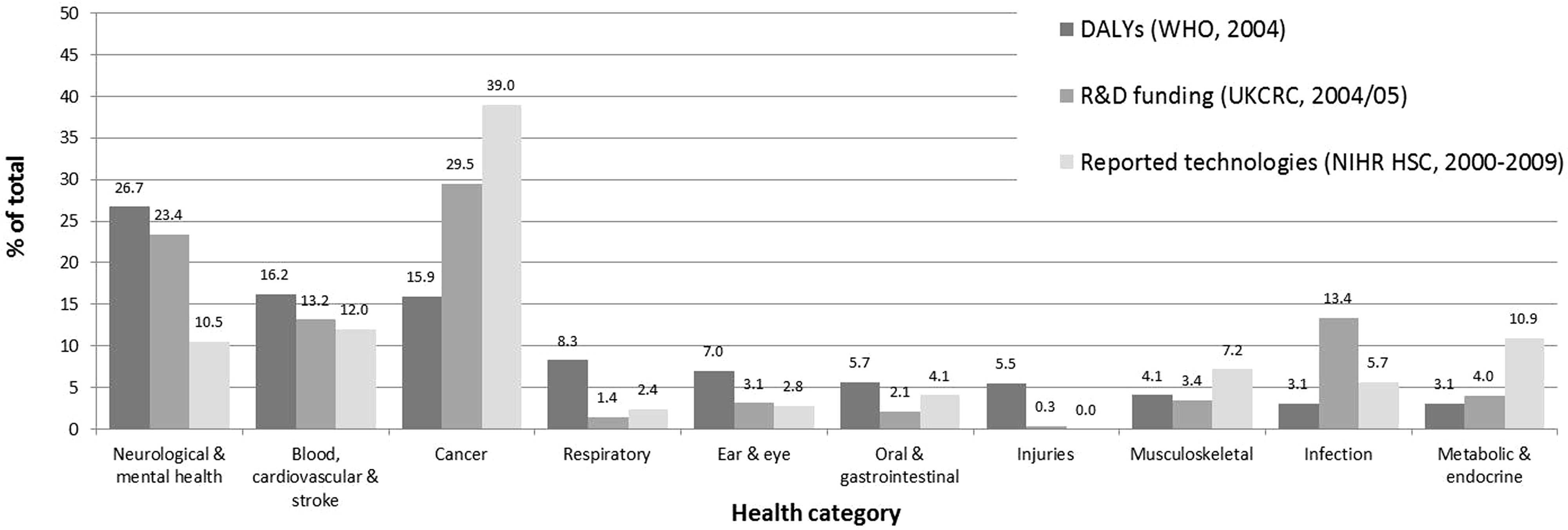


Relationships between burden of disease, innovation output and R&D funding
Summary of bivariate Pearson’s correlation coefficients comparing burden of disease, R&D funding and innovative output measures (N = 14 for all analyses).
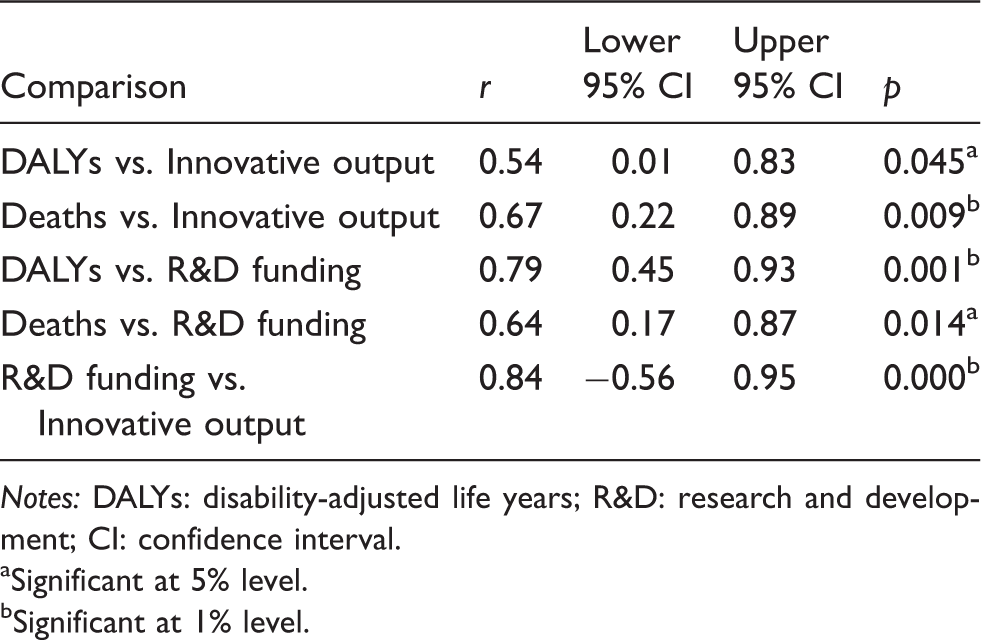
Notes: DALYs: disability-adjusted life years; R&D: research and development; CI: confidence interval.
Significant at 5% level.
Significant at 1% level.
While there was a significant positive association between R&D funding and reported technologies (Figure 3), the three health categories accounting for the biggest share of disease burden, funding and technologies (cancer; blood, cardiovascular and stroke; and neurological and mental health) were clearly preponderant. Removing these categories removed the apparent association (r = 0.45, n = 11, p > 0.05, 95% confidence interval (CI) −0.20 to 0.83).
Correlation between R&D funding and reported technologies (expressed as percentages of total values). R&D: research and development.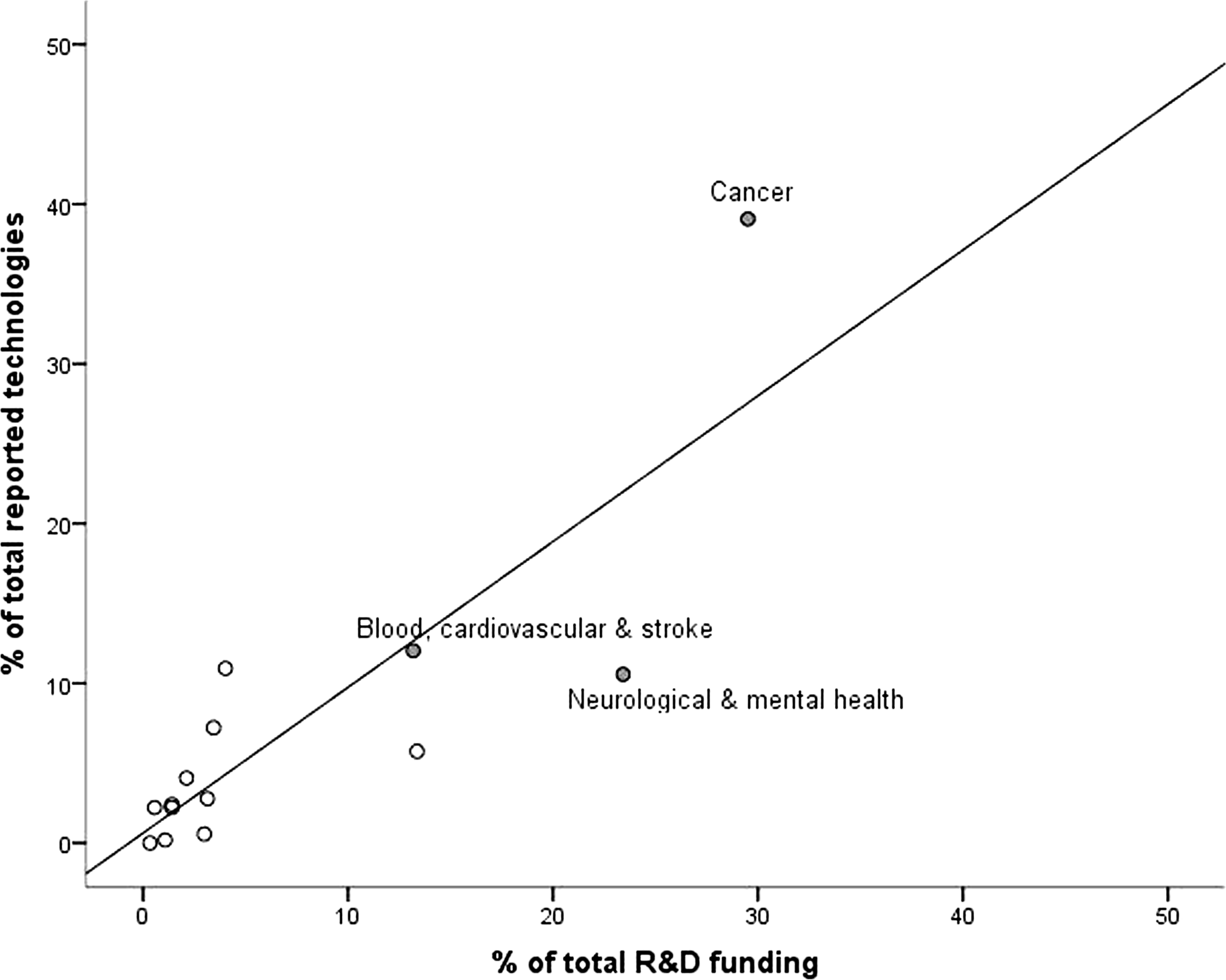
R&D funding as a mediator of the relationship between burden of disease and innovation output
Summary of regression analyses using burden of disease measures and R&D funding as predictors of reported technologies. (N = 14 for all analyses).

Notes: DALYs: disability-adjusted life years; R&D: research and development.
Significant at 5% level.
Significant at 1% level.
Discussion
The funding available for R&D is positively associated with both burden of disease and innovative output in the UK, and appears to mediate the relationship between burden of disease and innovative output. Spending and new and emerging health technologies reported by the NIHR HSC were disproportionately high for cancer compared with blood, cardiovascular disease and stroke, which represented the most deaths; and neurological and mental health conditions, which represented the most DALYs. Overall, deaths were a stronger predictor of reported technologies, whereas DALYs were a stronger predictor of funding.
The findings extend our previous research, which showed only a weak association between burden of disease and new and emerging health technologies among 17 developed countries. 1 One possible explanation for the discrepancy between health categories in relative funding and innovative output is that there is a differential focus of R&D funding across disease areas. Comparison with the UKCRC’s analysis 4 suggests that there is more innovative output in areas with higher spending on activities relating to treatment development and evaluation; detection and diagnosis; and disease management, rather than earlier stages of the research pathway (i.e. underpinning and aetiology). This may partly explain why neurological and mental health conditions account for a much lower proportion of technologies than would be expected according to funding levels, as less is understood about the pathophysiology of neurological diseases such as dementia. 15 The majority of R&D funding for this health category relates to underpinning and aetiology, 4 and it would be unreasonable to expect this to directly generate practical therapies within the timeframe of these data.
The main caveat is in the coarseness of the disease classification system. 1 Whilst the cause category hierarchy is an effective tool for grouping diseases, there are limitations where non-communicable conditions constitute the main burden. Many causes within this category represent high morbidity and mortality and would benefit from further subdivision. Separating the UKCRC’s data on neuropsychiatric conditions into neurological and mental health conditions reveals disproportionately low funding in mental health compared with the related burden, 16 and disaggregating the main categories into more specific causes decreases the degree of association between burden of disease and innovative output. 1 It is acknowledged that horizon scanning output does not represent all new and emerging health technologies over the study period, although it is a robust and relevant measure given the unit’s systematic approach to the identification and filtration of technologies, and its focus on those likely to impact on the NHS. 13 These technologies are also predominantly tangible innovations, i.e. drugs, devices and diagnostics rather than programmes and prevention, which may partly explain why cancer has far more associated technologies than neuropsychiatric conditions 1 despite both having high levels of R&D funding.
Timing is another important issue in interpreting these results. The time lag between basic research and translation into clinical practice has been estimated to be as long as 17 years; 17 though our dataset includes technologies that are still some years away from widespread adoption, technologies identified at later stages (e.g. post-launch or following appraisal by decision-makers) might show a different pattern. Furthermore, some caution is necessary in considering the role of funding in relation to innovation output. Firstly, commercially funded R&D may be focused on different points of the innovation pathway and different technology types and outputs to public funded R&D; industry involvement is likely to follow publicly funded basic research, and also influences downstream public research into models of care and service delivery. Secondly, the UKCRC analysis using 2004/2005 data provides the earliest overview of R&D funding across all disease areas, and is too recent to enable direct comparisons with innovation outputs from the last decade. However, comparisons with data from 1998/1999 1 8 suggest that it is a reasonable proxy for earlier trends, as the pattern of R&D spending in the UK for the three categories accounting for the most reported technologies in the present study (cancer, cardiovascular disease and neuropsychiatric conditions) has remained broadly similar.
These results accord with current policy emphasis on cancer 5 and dementia. 6 Although neuropsychiatric conditions have lower R&D funding than cancer, they still account for a high proportion of overall available monies. The importance of reducing inequalities in health also places emphasis on developing treatments for patient groups that are poorly represented, and ensuring that they have access to the same quality of health care. For example, the European Union legislative framework for orphan medicines exists to stimulate commercial R&D into drugs for rare conditions, 19 and potentially increase innovative outputs for these conditions. This may help to explain why metabolic and endocrine conditions are ranked quite highly in terms of funding and technologies relative to their associated burden. These findings might also inform future policy by highlighting areas that could benefit from increased R&D focus. It must be noted, however, that burden of disease is just one metric of need within health services, and reducing burden is just one factor in prioritising health service research. Broader impacts such as the economic benefits of research (as included in Buxton and Hanney’s 20 payback framework) may be as significant as direct gains in population health; the potential value of research is not a simple function of clinical need. 21
In conclusion, although there are generally more new health technologies for conditions representing a larger proportion of overall disease burden and R&D funding, and the relationship between burden of disease and innovative output appears to be mediated by the amount of funding or input, this is unlikely to be a straightforward cause-and-effect relationship. More funding does not necessarily translate to more innovation output, but instead may be concentrated into the earlier stages of the R&D pathway. The relationship between public and commercial R&D funding may also explain some of the apparent discrepancies between disease groups. Further analysis taking into account specific causes within wider groups would help show the extent to which innovation represents input and need. Future research should focus on developments within specific disease areas and retrospective comparisons with burden of disease, funding sources and R&D activity to clarify the main factors in defining and addressing unmet need.
Footnotes
Acknowledgement
We thank Dr Ian Viney from the MRC for providing the data on R&D funding for the analysis.
Conflict of interest
All authors declare that they have no competing interests.
Funding
The study was undertaken as part of the research programme of the National Institute for Health Research Horizon Scanning Centre (NIHR HSC). The NIHR Horizon Scanning Centre is funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.