
Abstract
Objective
To investigate whether previous drug prescriptions by, or exposure to, specialists influence general practitioners’ prescribing (using the example of inhibitors of the renin-angiotensin system).
Methods
Drug prescriptions in GP and specialist care, hospital records and outpatient visits in the Emilia-Romagna region (northern Italy) were linked to assess, among patients who in 2013 had been prescribed Angiotensin Converting Enzyme (ACE)-inhibitors or Angiotensin Receptor Blocker (ARBs) in general practice for the first time, whether those who had been previously prescribed these drugs by specialists (or have been recently exposed to cardiovascular, diabetes or nephrology specialists) were more likely to be prescribed an ARB or a patented ACE-inhibitor/ARB.
Results
A cohort of 88,926 patients was identified of whom 52,666 had not been exposed to specialists. Of these patients, 77.6% were initially prescribed ACE-inhibitors and 87.2% a non-patented drug. Higher prescription of ACE-inhibitors (82.0%) and of non-patented drugs (95.8%) in general practice were observed in the 10,243 the patients who had already been prescribed these drugs by a specialist compared to unexposed patients (p < 0.001 in both cases) and in the 14,648 patients exposed to specialists in the 90 days preceding the first prescription in general practice (79.0% and 89.6%, respectively, p < 0.001 in both cases).
Conclusions
Exposure to specialists was not associated with higher prescription of ARBs and of patented drugs in this Region of Italy. The hypothesis of prescribing induction by specialists is not supported by these data. This kind of analysis can provide help inform local prescribing agreements.
Introduction
Drug prescribing in general practice can be influenced by several factors. Information on drug effectiveness and safety should be the basis of therapeutic decision-making. Information is mostly provided by pharmaceutical companies and supported by drug representatives, 1 promotional initiatives, 2 sponsored publications, 3 clinical opinion leaders, 4 scientific publications and web sources. Less frequently, drug information is actively promoted by health authorities supported by evidence-based documents, educational activities and outreach visits.5,6
Using available information, general practitioners (GPs) may decide on their own which drugs to prescribe, depending on clinical assessments. However, sometimes they may rely on decisions taken by specialist colleagues and adopt prescriptions that they did not initially decide on. This may be used to justify high rates of prescription of newer and relatively expensive drugs, 7 not adequately supported by evidence but promoted by drug companies.
Angiotensin Converting Enzyme (ACE) inhibitors and Angiotensin Receptor Blockers (ARB) are drugs that inhibit the renin-angiotensin system. They provide an example of a prescribing choice that may be influenced by factors other than clinical evidence. These drugs share similar indications and are similar in terms of effectiveness and safety in patients with hypertension, heart failure, diabetes or renal disease. However, ACE-inhibitors were introduced earlier, have been studied more extensively, are cheaper and their use is supported by longer clinical experience than ARBs, so that clinical guidelines often suggest them as first choice. Preference should be given to ARBs in those patients not tolerating ACE-inhibitors, especially those who experience cough though this circumstance does not happen frequently with 2–3% withdrawal rates due to this reason. 8
Few studies had addressed the issue of specialist-induced prescribing.9–12 Analyses are lacking as to which drug doctors preferentially choose among alternative, well-established and clinically relevant treatments. In Italy, there are 14 ACE-inhibitors (out of 16 ever developed) and seven ARBs (out of 9) available not including their combinations with other drugs. This study aimed at testing the hypothesis that specialists can influence the prescription of ARBs (instead of ACE-inhibitors) and of patented drugs of those two classes (instead of older but still reliable non patented drugs) in general practice in Emilia-Romagna, a region in northern Italy.
Methods
Residents of the Emilia-Romagna Region (population 4.4 m) who were prescribed ACE-inhibitors (ATC codes C09A and C09B) and ARBs (ATC codes C09C and C09D) by a GP during 2013 were selected. Those who had already been prescribed these classes of drugs during 2012 were excluded in order to focus on patients newly prescribed these drugs in general practice. GPs can prescribe up to two drugs on each prescription and each prescription can be used within one month. The first GP prescription of ACE-inhibitors or ARBs in 2013 was linked with the most recent specialists’ prescription of these drugs before the first GP prescription, and with the last hospitalization or outpatient visit in NHS or NHS-accredited facilities which resulted in a diagnosis of either diabetes, cardiovascular or renal disease if it occurred within the preceeding 90 days and did not result in a specialist prescribing a ACE inhibitor or ARB. Figure 1 shows the patient flow and exposures.
Flow of patients prescribed ACE inhibitors or ARBs in general practice in Emilia-Romagna in 2013, according to previous use and to exposure to specialists.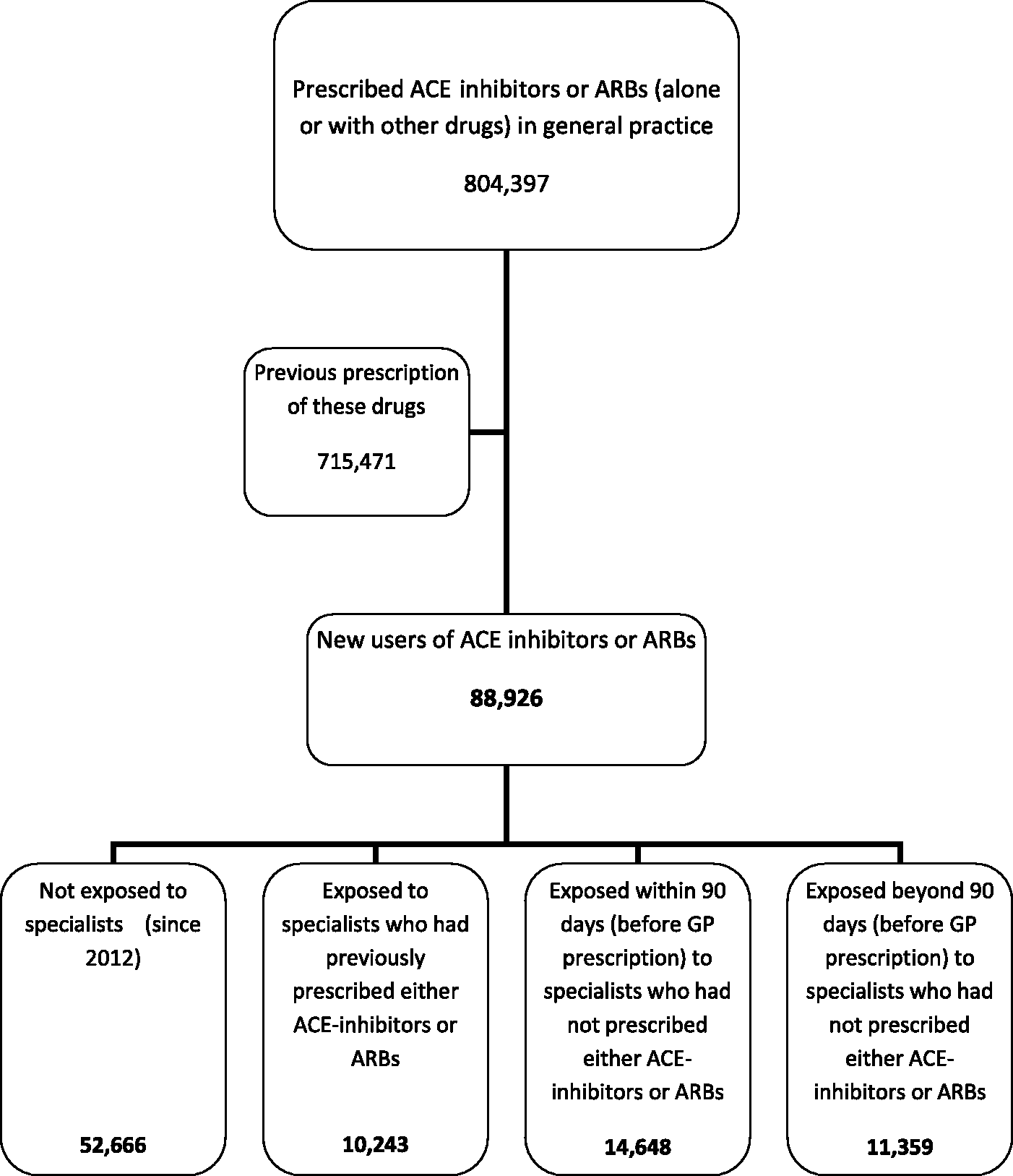
Chi-squared tests were used to evaluate whether patients with such exposures were firstly prescribed ARBs and non-patented drugs (excluding those which went off-patent during 2013) in general practice more often than unexposed patients. Sensitivity analyses were performed by varying the time since exposure to non-prescribing specialists by considering 30, 60 and more than 90 days. Data were extracted from regional administrative databases of outpatient drug prescriptions, hospital records and outpatient visits. ICD-9 codes of hospital discharge diagnoses and of outpatient visits were used to identify relevant exposure to specialists (Appendix 1, available online). STATA statistical software ® (version 12) was used for data analysis.
Results
Percentage of GPs’ first prescription of ACE inhibitors or ARBs in first-time users in 2013, according to type of exposure to specialists.
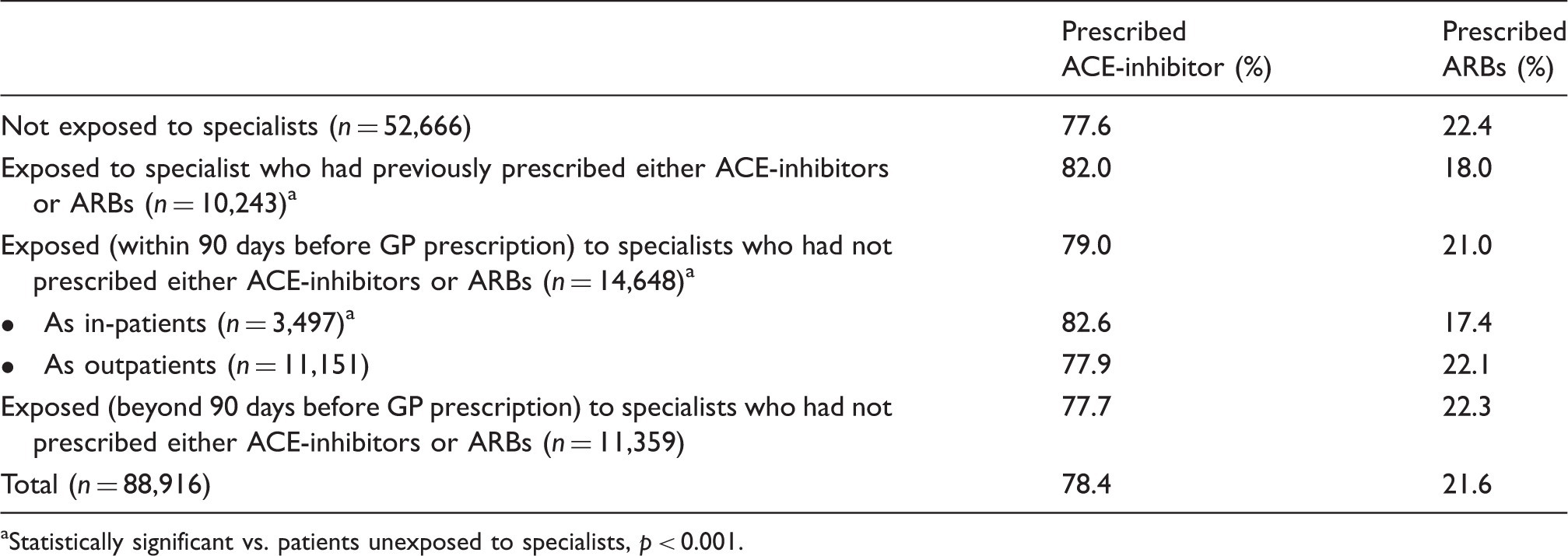
Statistically significant vs. patients unexposed to specialists, p < 0.001.
Concordance between last specialists’ prescription of ACE-inhibitors and ARBs and subsequent prescription by GPs.

Percentage of GPs’ first prescription of non-patented ACE inhibitors or ARBs in first-time users in 2013, according to type of exposure to specialists.

Statistically significant vs. patients unexposed to specialists, p < 0.001.
Statistically significant vs. patients unexposed to specialists, p = 0.015.
Sensitivity analyses by time since exposure to non-prescribing specialists show that all the prescribing patterns observed were similar using 30, 60 and more than 90 days.
Discussion
Main findings
In general practice, prescription of ARBs and of patented drugs is not influenced by specialists. In contrast, patients who had already been prescribed these drugs by a specialist, or who had seen a specialist as inpatients within 90 days before receiving their first prescription by a GP, were more likely to be prescribed an ACE-inhibitor or an off-patent drug. The latter circumstance may be related to the prevalence of older drugs in hospital formularies, whereas no difference is observed for the prescription of ACE-inhibitors in the case of exposure to outpatient specialists. In case of previous specialist prescriptions, concordance of about 95% was observed with subsequent prescriptions by GPs. Among the few GPs who did not continue specialists’ prescriptions, 3.2% more did not follow on ARBs compared to those not following on ACE-inhibitors, suggesting that GPs who expressed disagreement tended to show a higher compliance with clinical practice guidelines.
A few small studies have addressed the specialist-induction issue in drug prescribing with conflicting results. This is not surprising, as drug prescribing can be strongly influenced by the characteristics of health systems, local prescribing habits and drug policies, organization of health services, classes of drugs considered and their evidence-base and timing of the evaluation.
Strengths and limitations
The strength of this study is the large number of prescriptions analysed, much greater than in previous studies, and the use of new prescriptions which should reflect prescribing behaviour by general practitioners. However, the results specifically relate to incident prescriptions of ACE inhibitors and ARBs, and may not be generalizable to other clinical areas. Our results could be influenced by local factors, which may also limit their generalizability to other geographical areas and health systems. Some other specific limitations should be acknowledged. First, not all visits to specialists taking place outside the NHS could be retrieved. Then, we presumed patients with no prescription in 2012 were new recipients of the drugs, but some of these patients may have used those drugs previously, although the non-use window was quite wide (from a minimum of 12 to a maximum of 24 months, depending on timing of the first prescription). This should have limited that risk considerably. As for subsequent prescriptions, we did not follow up beyond the first ones. Finally, a record-linkage study using administrative data cannot provide information on health status or other specific determinants of prescribing but can probably suffice in rejecting the hypothesis of specialist induction that – if present – should have been clearly visible in these data.
Implications
In general, the incident prescription of ACE-inhibitors and off-patent drugs of these classes in general practice in Emilia-Romagna is consistent with the recommendations of clinical guidelines: ramipril is by and large the most prescribed drug of these classes and, among ARBs, valsartan is the preferred one. It is reassuring that the most commonly prescribed drugs reflect the research evidence which influenced the recommendations in local prescribing agreements. 13 On the other hand, new prescriptions of ARBs and of patented drugs may have been influenced by drug representatives. Prescribing improvements are possible using evidence-based policy documents developed by key stakeholders within multidisciplinary groups. 13 It should be noted that, in 2013 there were about 6.4 million prescriptions of either ACE-inhibitors or ARBs in Emilia-Romagna. Since the average cost of a prescription was 10 euros for ACE-inhibitors and 25 euros for ARBs (including associations with diuretics or calcium antagonists), each 1% shift from ARBs to ACE-inhibitors could bring savings for about 1 million euros.
Conclusion
These data do not support the hypothesis that GP prescribing of ARBs and off-patent drugs is initiated by specialists. We do not know whether the opposite pattern emerging from our data means that specialists’ prescribing is closer to guidelines recommendations, or simply that it is somehow influenced by local formularies where established drugs are highly represented especially within hospitals. It is also possible that GPs may be sensitive to drug promotion, maybe because they mostly work alone and infrequently share drug information and prescribing responsibility with their colleagues. 14
Appropriate drug prescribing is key for the sustainability of health systems, in general practice as well as in hospital and outpatient facilities. In order to promote it, a mix of strategies should be considered, such as providing information independent from drug companies through NHS led, collaborative efforts involving both GPs and specialists, avoiding top-down approaches,5,6 using prescribing audit and feedback, 15 and using disincentives to inappropriate prescription. 16 GPs and specialists should collaborate and actively promote sensible drug policies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.