
Abstract
Objective
We aimed to assess use of and interest in mobile health (mHealth) technology and in-person services for diabetes self-care in vulnerable populations.
Methods
We delivered a self-administered cross-sectional survey. Participants were recruited at two primary care practices (P1 and P2) with P1 located in a medically underserved area and P2 in an affluent suburb. Two-sample t-tests and chi-square tests were used with p < 0.05 significant. In addition, a secondary analysis was performed to analyse differences in use and interest in mHealth by age.
Results
Of 75 eligible patients, 60 completed the survey (80% response rate). P1 patients had significantly higher interest in three of five categories of in-person diabetes support services, one of four categories of health-related text messages (TM), and three of eight categories of mHealth applications (p < 0.05). Smartphone users reported higher interest in TM (p = 0.004) and mHealth applications for diabetes self-care (p = 0.004). Younger patients were more likely to have a smartphone (p < 0.006), use the Internet (p < 0.0012), use smartphone applications (p < 0.0004), and to be interested in using applications to manage their diabetes (p < 0.004).
Discussion
This study shows substantial patient interest in TM and mHealth applications for diabetes self-care and suggests that patients in underserved areas may have particularly high interest in using mHealth solutions in primary care. Younger patients and smartphone users were more likely to be interested in using applications to manage their diabetes. As more patients use smartphones, interest in using mHealth to support patient self-care and strengthen primary care infrastructure will continue to grow.
Introduction
Over 28 million Americans currently have diabetes,1,2 and their adherence with medications and recommended lifestyle changes is often poor. 3 Recent population-based estimates indicate that less than 40% of type 2 diabetics have “good” adherence to their medication regimens, 3 and even fewer adhere to other recommended diabetes self-care behaviours such as physical activity, weight loss, and smoking cessation. 4 New approaches are needed to improve patient engagement in diabetes self-care to prevent long-term complications. Mobile health (mHealth) solutions including health-related text messages (TM) and mHealth applications (Apps) have been proposed as important emerging technologies to assist in patient self-care.4–6 Early evidence from several studies supports effectiveness for health-related TM7–10 and mHealth Apps11–13 in improving diabetes self-care behaviours. 4 On average over 83% of Americans report owning a cell phone, and the use of cell phones for more than simply making calls continues to grow. 14
Although interest is growing in using mHealth tools to improve diabetes self-care in vulnerable populations, major feasibility issues remain unanswered. First, only a few studies have documented interest in mHealth in vulnerable groups,15,16 and the current study explored what patients wanted in a mHealth programme. Likewise, implementation feasibility and effectiveness in primary care practice settings is unclear. 17 One recent study demonstrated that even though patients prefer entering their personal diabetes health data using mobile rather than web-based technology, their engagement diminishes over time. 18 Another recent survey showed that physicians were willing to incorporate mHealth tools into their practices, provided they showed value and were not too cumbersome. 19 Furthermore, a major study is underway in three countries investigating whether clinical outcomes for diabetics are improved using health-related TM for diabetes self-care. 20
The current research assesses use of and interest in mHealth tools in vulnerable populations in order to help determine the feasibility of encouraging vulnerable patients to use mHealth technology more broadly to assist in diabetes self-management. In particular, we sought to assess diabetic patients’ current cell phone, smartphone, and mHealth usage practices, and their interest in using mHealth tools to help them take charge of their own chronic illness. Furthermore, we hoped to document vulnerable patients’ use of and interest in various types of health-related TM and mHealth Apps in the primary care setting, and patient use of and interest in in-person diabetes support services. We particularly wanted to know whether use of and interest in mHealth and in-person services varied according to smartphone use and/or according to practice location and predominant population served. We hypothesized that smartphone users would be much more interested in mHealth Apps, and that interest in health-related TM and mHealth Apps would be significantly lower among patients seen in a practice serving a medically underserved area.
Methods
The current investigation employs a self-administered cross-sectional survey of patients with diabetes assessing their use of and interest in both mHealth and in-person support services for diabetes self-care.
Setting and participants
In order to contrast use of and interest in mHealth and in-person support services for diabetes self-management in diverse populations in the Southern United States, two representative primary care practices in West Tennessee were selected: one general internal medicine practice serving a majority African-American medically underserved community (Practice 1), and a second general internal medicine and endocrinology practice serving a majority white and more affluent suburban community (Practice 2). The Whitehaven, Tennessee community in which Practice 1 is located is primarily African-American (96.0%) and has a median income of $37,016, with about 45.4% of residents having completed at least 1 year of college, and about 35% having not completed high school. 21 Nearly 28% of individuals live below the poverty level, with 37.4% single-mother households. 22 This region is a medically underserved area and a primary care shortage area according to the Health Resources and Services Administration. 23 In contrast, the Germantown, Tennessee community in which Practice 2 is located is primarily white (86.6%) and has a median income of $126,196, with about 83.6% of residents having completed at least 1 year of college, and only about 2.2% having not completed high school. 21 These disparate populations were targeted in order to investigate whether use of and interest in in-person and mHealth diabetes support services differed among people from neighbourhoods with diverse geographic, racial, and socioeconomic characteristics.
The subject population included all adult diabetes patients seen in the participating practices for an outpatient visit for a representative 1-week period in July and August 2013. All survey participants met the following inclusion criteria: they were between 18 and 90 years of age and carried a physician-confirmed diagnosis of either type 1 or 2 diabetes. Patients with significant cognitive impairment or inability to communicate their responses to survey questions as determined by their physician or family members were excluded.
Survey development
The survey instrument was designed to collect general demographic data and to investigate use of and interest in mHealth and in-person support services for diabetes self-care. The survey instrument was developed using standardized questions from several sources including the Behavioral Risk Factor Surveillance System (BRFSS), 24 National Health Interview Survey, 25 and several peer-reviewed articles.26,27 Questions regarding diabetes diagnosis and treatment were derived from BRFSS. 24 Questions regarding use of and interest in mHealth for diabetes self-care were adapted from the De Reuver et al. cell phone and mobile application survey, 26 and all employed a 5-point Likert scale. Diabetes communications experts assisted in refining the survey content in an iterative fashion both before and after pilot testing the draft survey instrument with adult diabetic patients in the Memphis area.
Survey administration
A medical student explained the role and scope of the survey to each eligible participant during a routine primary care visit. Patients were left to complete the survey as they waited on their physician. A written consent statement was included at the beginning of each survey and consent for participation was indicated by completion of the self-administered survey. Surveys were generally self-administered but for patients who desired assistance, either a companion of the patient or a medical student read the survey aloud and collected the patient’s responses. Each survey was individually numbered in order to track participation, and incomplete surveys were collected to assess response rate.
Analysis
Frequencies were enumerated for patient characteristics and responses by practice site and smartphone ownership. Two-sample t-tests and chi-square tests for contingency tables were employed to identify differences between practices and between smartphone users and non-users, with p < 0.05 considered significant. In addition, we conducted a post-hoc secondary analysis to assess the impact of age on use and interest in mHealth opportunities, comparing those <65 years of age vs. those ≥65 using the chi-square test and controlling for practice.
Results
Participant characteristics stratified by practice site.*

Column percentages only include valid responses.
The total of column percentages for medication regimen surpass 100% because many patients were on both oral hypoglycaemic agents and insulin.
Participant use of technology, cellular phones, and smartphones.*
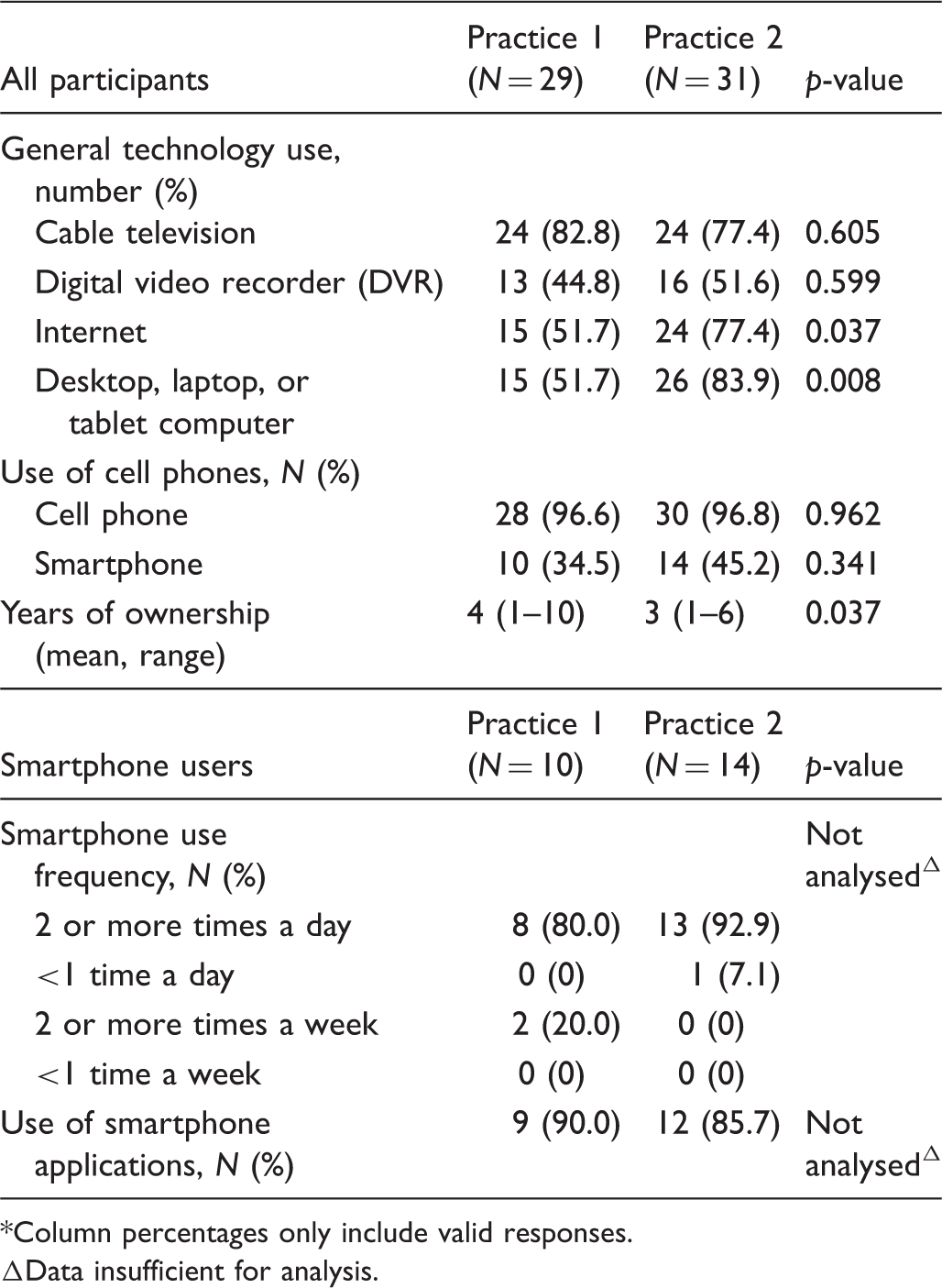
Column percentages only include valid responses.
Data insufficient for analysis.
Participant interest in mHealth and in-person diabetes support services.
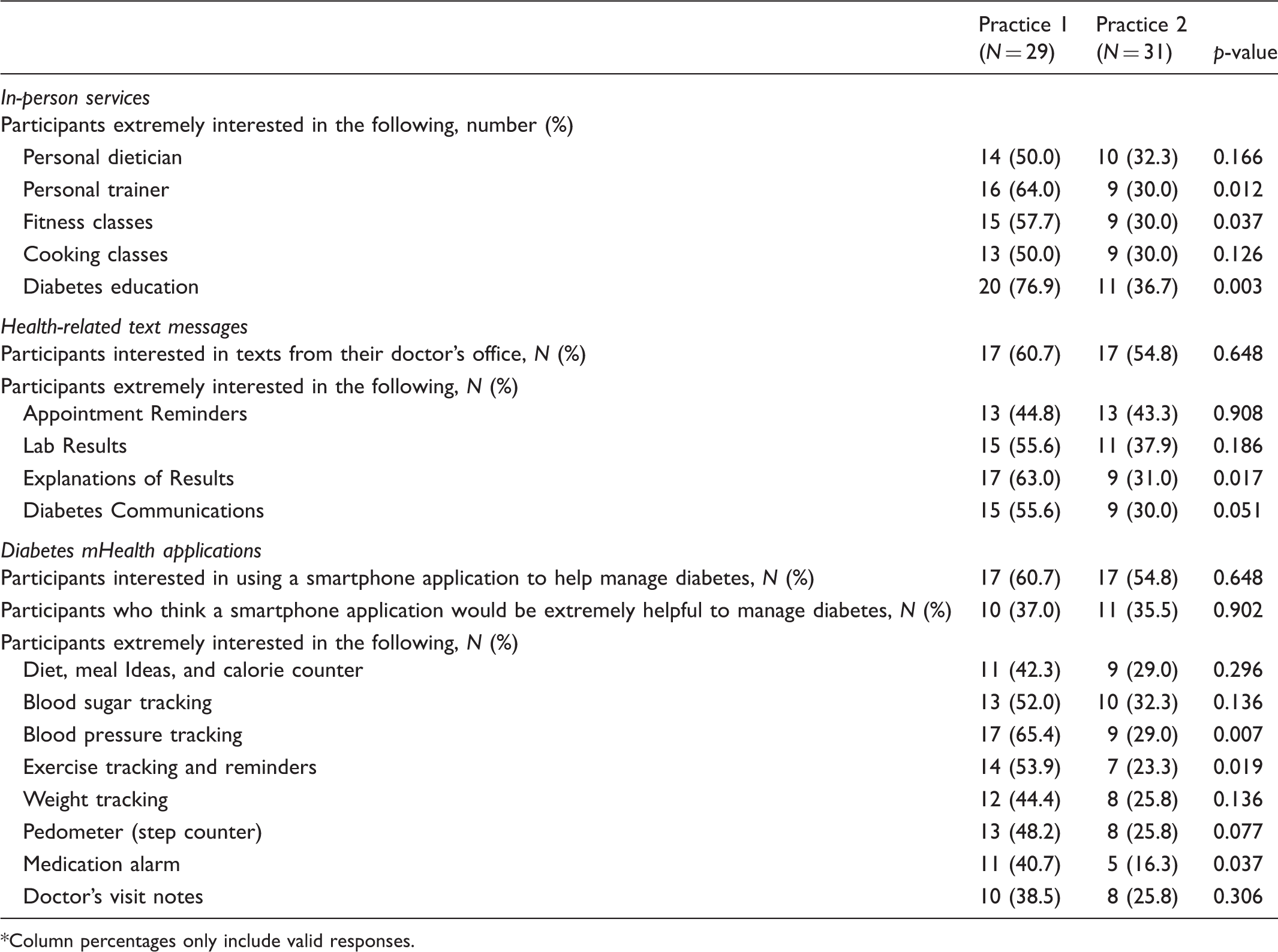
Column percentages only include valid responses.
The majority of respondents in both practices reported high levels of interest in health-related TM, with interest in Practice 1 (Table 3) showing a non-significant trend toward greater interest. Overall 56.7% of respondents reported interest in receiving health-related TM from their doctor’s office. The majority of the Practice 1 patients were extremely interested in almost every category of health-related TM assessed. Practice 1 patients had significantly greater interest in TM providing “explanation of results”, with 63.0% being extremely interested as compared with only 31.0% in Practice 2. However, for the remaining categories of health-related TM including “lab results”, “appointment reminders”, and “DM communications” differences in levels of interest at the two practices did not differ significantly.
The majority of respondents in both practices reported high levels of interest in mHealth Apps, but, once again, interest was not significantly higher in Practice 1 (Table 3). The percentage of respondents interested in using a smartphone application to help manage diabetes was slightly higher in Practice 1 (60.7% in Practice 1 vs. 54.8% in Practice 2). Similarly, 37.0% of respondents in Practice 1 versus 35.5% in Practice 2 reported that a diabetes smartphone application would be extremely helpful in managing diabetes. When response categories were collapsed (data not shown), we found that 51.9% of respondents in Practice 1 versus 54.8% in Practice 2 reported that a diabetes smartphone application would be either very or extremely helpful in managing diabetes. None of these differences were statistically significant.
As shown in Table 3, the majority of Practice 1 patients were extremely interested in mHealth Apps related to blood sugar, blood pressure, and exercise tracking, with significantly greater interest found for mHealth Apps providing “blood pressure tracking”, “exercise tracking and reminders”, and a “medication alarm”. The greater interest in mHealth Apps seen in Practice 1 was particularly surprising given the lower rates of smartphone use, Internet use, and computer ownership among patients in that practice.
Overall, interest in health-related TM and mHealth Apps was higher in smartphone users. Most smartphone users reported using Apps on their devices in Practice 1 (90.0%) and in Practice 2 (85.7%). We found that 79.2% of all smartphone users reported interest in receiving health-related TM from their doctor’s office vs. 41.7% of non-users (p = 0.004). Similarly, 79.2% of all smartphone users reported being interested in mHealth Apps to help manage diabetes versus 41.7% of non-users (p = 0.004). The percentage of patients either very or extremely interested in using a smartphone to help manage their diabetes was also slightly higher among those who owned smartphones (58.3%) versus those with regular cellphones (48.5%), but this difference was not significant (p = 0.4622, data not shown).
Secondary analysis to assess the effect of age on use and interest in mHealth demonstrated that younger patients in both practices were significantly more likely to have a smartphone (p < 0.006). There were no differences by age in interest in in-person diabetes support services. Controlling for practice, we found that younger patients were more likely to use the Internet (p < 0.0012), were more likely to have ever used mobile applications on a smartphone (p < 0.0004), and were more interested in using a smartphone application to help them manage their diabetes (p < 0.004). However, there was no difference in interest in assistance with using mHealth Apps and no differences in interest in specific types of diabetes mHealth Apps by age. Controlling for practice, more young patients were interested in receiving TM from their doctors’ offices (p < 0.0002) and thought a diabetes App would be extremely helpful (p < 0.05). However, high percentages of patients in both age groups were interested in receiving TM, with 100% of younger patients in P1 and 79% in P2 interested versus 42% of older patients in P1 and 33% in P2.
Discussion and conclusions
Discussion
This mHealth diabetes management survey was designed to assess patients current use and interest in mHealth technology and in-person intervention for diabetes self-management, and we were particularly interested to learn whether minority patients in medically underserved areas used and/or were interested in using mHealth. As expected, we found that smartphone users were more interested in health-related TM and mHealth Apps. But even though we hypothesized that interest in health-related TM and mHealth Apps would be significantly lower among patients seen in a practice serving a predominantly minority population, instead, we found that there was a higher degree of interest in mHealth in the patient population with less access to technology.
Little prior research documents interest in mHealth in vulnerable populations, and the feasibility of implementing mHealth solutions in primary care practice settings remains unclear. 17 But this study suggests that mHealth is a feasible modality for assisting vulnerable populations in taking charge of their own chronic illnesses. Furthermore, the study indicates that vulnerable patients are interested in both in-person and mHealth diabetes support services in the primary care setting. The current research suggests that low-cost health-related TM may be particularly suitable for dissemination in primary care practice settings given its ease of use by those with cell phones and smartphones alike, widespread patient interest in diverse populations, and low cost. The fact that patients with lower income and socioeconomic status want this information is promising. This work suggests that young patients are poised to take advantage of mHealth services in much higher numbers, but both younger and older patients showed interest. Future studies are needed to assess the impact of health-related TM and mHealth Apps for low-income minority populations and to assess whether mHealth tools help these populations track and measure change in the control of their diabetes.
The patients in Practice 1 also showed a significantly greater interest for in-person diabetes management, which may indicate that these patients may be lacking access to other important tools that they need to help manage their condition. This desire for more resources is consistent with the lower socioeconomic status of patients in this community, and indicates a need to combine the mHealth components of any self-management scheme with in-person support to afford patients the greatest possible chance for success.
The generalizability of this study is limited by its use of convenience samples from representative practices in two diverse communities rather than a regionally or nationally representative sample. However, there is no a priori reason to suspect that attitudes and practices related to mHealth in the surveyed populations would substantially differ from those in the population at large. It is possible that diabetic patients seen in the two participating practices were not representative of diabetic patients in the community at large. Indeed, the patients surveyed were likely more engaged in diabetes self-care than the average for each community. The respondents in the practice in the medically underserved area had higher levels of education than those in the community served by that practice, but the characteristics of the patient populations surveyed were otherwise generally similar to those for the communities from which they were drawn. The samples surveyed in this cross-sectional study are likely to represent the diabetic patients actually being seen in each community in medical clinics.
Conclusions
Unequal access to preventive and chronic disease care support services and mHealth tools may impact the ability of medically underserved populations to participate in effective preventive and chronic disease self-care. Equipping financially disadvantaged people with tools for disease prevention and chronic disease self-management may yield immediate payoffs though improved health and decreased overall healthcare expenditures. This study has important implications for primary care practices with limited resources to meet patient needs.
The results of this study suggest that mHealth interventions may be particularly suitable for younger patients, smartphone users, and patients in medically underserved areas. The data further suggest that there is high demand for both mHealth and in-person diabetes self-care support in primary care settings in medically underserved communities. The addition of a distance-based intervention, which does not require clinician time, is low cost, can be readily disseminated to large numbers of patients, may be a particularly effective population-based approach for educating patients about their disease.
Further studies should replicate the findings of this study and should assess the potential reasons for the differences seen in use of and interest in mHealth for diabetes self-care.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Ruth Weinstock, M.D. of the SUNY Upstate Medical University and Maggie Debon, Ph.D. of the University of Tennessee Health Science Center with survey and study design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.