
Abstract
Objective
Emergency Department (ED) patient volumes are unpredictable, which can result in service delays and patients leaving without care. We initiated a programme of emergency physician (EP) telepresence in the ED with the objectives of assessing feasibility, safety, patient and provider acceptance, and throughput time.
Methods
This was a prospective convenience study. Patients presenting to the ED during operation of the study who were planned for placement in the waiting room were considered for enrolment. A faculty EP conducted patient evaluations via telepresence with confirmatory evaluation by the onsite faculty EP prior to disposition. Patient care was either taken to completion by the telemedicine EP or initiated and handed off to the onsite team. Measures included patient demographics, triage class (ESI 1–5), throughput time and a single question satisfaction survey (rating 1–5, 5 most favourable) completed by patients, registered nurses and EPs. Patients were called within 3 days and the electronic health record reviewed at 7 days looking for unscheduled visits and adverse events.
Results
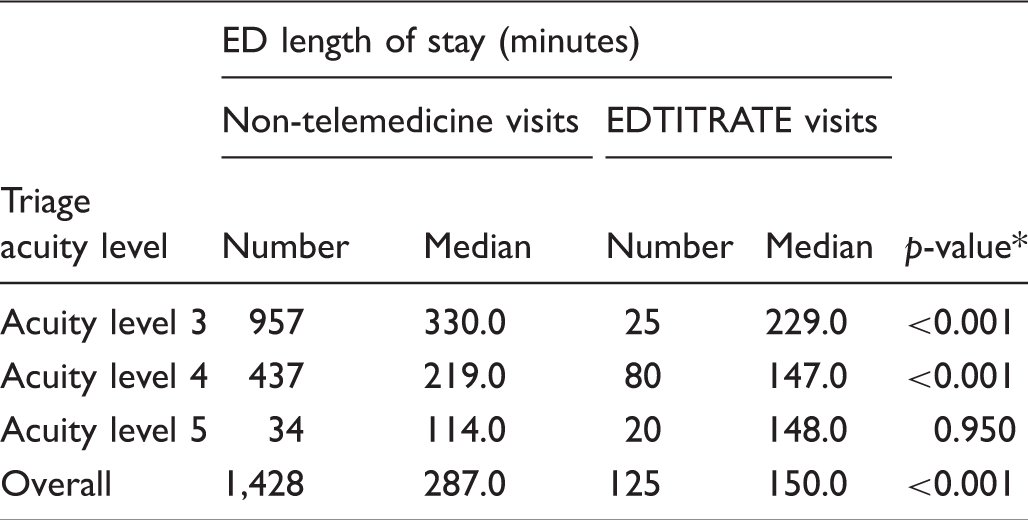
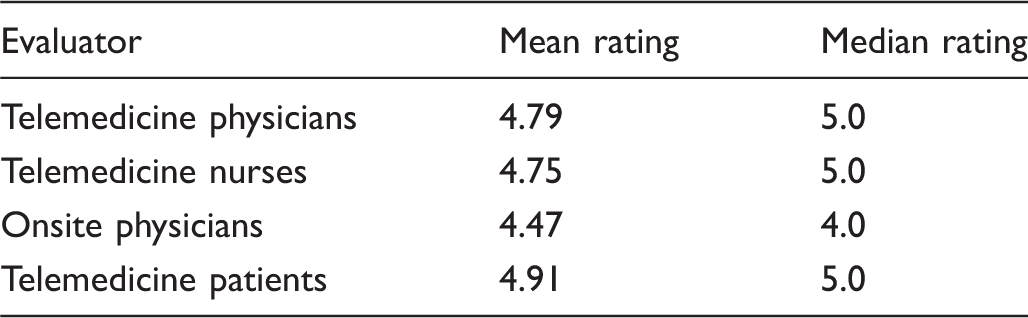
In total, 130 patients were enrolled. Mean triage class was 3.9 with a median throughput of 150 minutes (IQR = 116.5, 206). Non-telemedicine patients during the same time period with similar triage classes had a median throughput of 287 minutes (IQR = 199, 408). Mean satisfaction scores were: patient 4.91, nurse 4.75, onsite EP 4.47 and telemedicine EP 4.79. There was one potential misdiagnosis and no adverse events.
Conclusion
Patient evaluation by EP via telepresence is feasible, safe, readily accepted by patients and providers and associated with reduced throughput time.
Introduction
Emergency Department (ED) attendance has been increasing steadily over the past two decades from 95 million in 1997 to 130 million in 2010.1,2 This increase has occurred in the setting of fewer EDs and a reduction in the number of hospitals and inpatient beds.3,4 These factors contribute to progressive problems with ED overcrowding. Overcrowding has been associated with prolonged waits, reduced patient satisfaction, increased mortality and increased likelihood of patients leaving before medical evaluation.1,5–7 ED and emergency groups have long recognized these problems and have implemented programs to mitigate the impact. One approach has included placement of physicians in the triage area during periods of anticipated maximal demand to both initiate evaluation and to treat and release patients with minor problems.8–10 In addition, many EDs have physicians available for backup to be called in during periods of high demand or surge. While these approaches work, they can be costly and inefficient. When a physician is scheduled to work a triage shift, but the anticipated need does not materialize, the result is economic inefficiency. In the case of calls for backup, physicians on site tend to be inherently reluctant to initiate the process, and even when done promptly response can be delayed. The backup physician has to respond to the call, deal with whatever they may be involved in, and then travel variable distances to come in. Time is also consumed on the back end with travelling home. The reluctance to activate a backup physician is even greater when it happens more than once in a single day.
Exploring innovative approaches to address the combined issues of increasing ED utilization and unpredictable daily and intra-day patterns of patient arrival is urgently needed. Placing an emergency medicine (EM) physician in triage via telepresence offers the opportunity to provide physician staffing immediately when the need arises. This “just-in-time” approach can glean the benefit of a physician at triage in a more responsive and cost-effective manner. Furthermore, remote response via a telemedicine link should reduce the reluctance to initiate a call for assistance and makes secondary activations within a single day less onerous for the off-site provider.
In this study we aimed to initiate a pilot program of EM physician telepresence in the ED with the objectives of assessing feasibility, safety, patient and provider acceptance and impact on patient throughput.
Methods
Study design
We conducted a prospective convenience study of an innovative pilot of physician telepresence in an academic ED with the acronym EDTITRATE (Emergency Department Telemedicine Initiative To Rapidly Accommodate in Times of Emergency).
Site and patient selection
The study was conducted at an urban comprehensive academic ED staffed 24 hours a day by one or more board-certified emergency physicians along with 2–4 EM residents, a variable number of residents rotating from other specialties and medical students. Nurse practitioners or physician assistants are not utilized. Patients were enrolled on a voluntary basis after signing a standardized facility telemedicine consent and a second consent specific to the EDTITRATE pilot study. Any patient presenting during hours of the pilot study operation that was suitable for placement in the waiting room was considered eligible for enrolment in the pilot. Patients appropriate for waiting room placement were approached by the telemedicine nurse and given the option to participate in the study, at which time the consent was reviewed with both the telemedicine nurse as well as the remote physician. There was no advertising of this study. The telemedicine nurse was the only nurse involved in the care of these patients. Children, non-English speakers, patients in custody and those unable to provide informed consent were excluded from study enrolment.
Intervention
The program utilized the Globalmed i8500™ (GlobalMedia Group, LLC headquartered in Scottsdale, AZ, USA) telemedicine cart. The device provides for two-way high-quality audio as well as a high-resolution camera that is controlled by the remote practitioner and can be manipulated up and down and side to side, with zoom in and out features allowing for optimal viewing angles. This model is equipped with a PC, two monitors, a fibre optic light source and three peripherals: a high-resolution hand-held camera, a fibre optic otoscope and stethoscope. The peripherals are managed by the onsite telemedicine nurse. The remote physician connects with the onsite system using a PC or lap top via Cisco Jabber TelepresenceR software (Cisco Systems Inc., San Jose, CA, USA). This Jabber software is available to us via an institutional license and provides for high-definition, HIPAA-secure two-way communication between the remote physician and the exam room in which the telemedicine cart is placed. Anyone present in the private exam room can see and converse with the remote physician. A group of seven emergency physicians volunteered to share a call schedule for the project. Four telemedicine-trained onsite emergency nurses scheduled to fill administrative shifts were available to convert to a telemedicine role during times of need. Only one nurse was necessary for any particular telemedicine patient. Telemedicine was considered for activation on weekdays between 12 pm and 7 pm when the ED was impacted with patients backing up into the waiting area. The telemedicine nurse made the decision to activate after assuring the on-call physician was available and could establish a reliable connection to the telemedicine cart. All exams were conducted in one of several ED rooms wired to accept the telemedicine cart. The physician conducted an appropriate history and visual exam, with portions of the physical exam performed by the nurse under the direction and visual monitoring by the telemedicine physician. Nurses had standardized training in basic telemedicine physical exam skills in order to make the process seamless. All orders, physician and nurse documentation was placed into the ED electronic health record (EHR). Telemedicine patients were identified on the EHR status screen which included the assigned nurse and telemedicine physician. Test results and imaging studies could be reviewed remotely by the telemedicine physician. All telemedicine staff (nurses and physicians) are licensed and credentialed at the University of California San Diego Health System.
Two primary scenarios could occur in the telemedicine patient encounter. Patient care could be completed by the telemedicine team, or care could be initiated and the patient returned to the waiting room to be assumed by the onsite medical team when an exam room became available. Prior to disposition or at the time of handoff, a report was given to the onsite emergency attending physician. The onsite attending physician performed an evaluation, the extent of which was at their discretion. All telemedicine patients were required to be seen by the onsite physician. The onsite physician either formally assumed care of the patient or placed a confirmatory note in the medical record if the patient was ready for discharge or admission. Data regarding onsite physician performance times were not tracked, but the throughput figure in the results below is inclusive of any delay that may have occurred in the onsite physician completing their evaluation. Prescriptions for discharged patients could be written with the assistance of an onsite physician or transmitted electronically to a pharmacy by the telemedicine physician using the “e-prescribe” function of the EHR.
Data collection and processing
Study variables included patient demographics, chief complaint, triage category (Emergency Severity Index (ESI), 1–5 classification system employed in which level 1 is the highest acuity and level 5 is the least acute), throughput time (triage to left the ED), disposition (admit, discharge), discharge diagnosis, a patient numerical satisfaction assessment score (1–5, 1: dissatisfied, would not agree to telemedicine again, 5: very satisfied, would recommend telemedicine to other patients), a provider (telemedicine physician, onsite nurse and onsite physician) numerical assessment score (1: dissatisfied, would not continue telemedicine, 5: very satisfied, would recommend telemedicine). This survey tool was developed internally for this project and was not a simple Likert Scale. Attempts were made to call all patients within 3 days of being seen to check on their status. This phone call was made by the remote physician who participated in the care during the encounter. The EHR was reviewed at 7 days post disposition to determine if unexpected return visits or adverse events had occurred.
Throughput time was reported as medians with interquartile ranges (IQR) for EDTITRATE and non-telemedicine patients. Median values comparing discharged EDTITRATE and non-telemedicine patients by triage category was performed employing Non-Parametric Mann–Whitney U tests.
This study was approved by the UC San Diego Human Research Protection Program.
Results
ED length of stay – discharged patients.
Patient and provider assessment scores.
Discussion
The Oregon health insurance experiment increased Medicaid coverage for uninsured low-income adults. This is a state-coordinated effort to insure lower-income members of the population. A study of its effects indicated it was associated with a significant increase in ED utilization. 11 If a similar impact occurs as a result of the Patient Protection and Affordability Act (Obamacare), the rise in ED use seen over the last several decades is likely to continue or even accelerate. This creates an urgency to explore new and innovative means of managing ED patients. Traditional attempts to optimize staffing levels with need are based upon trends that are created by plotting patient flow on an annual basis. These fairly smooth curves belie the highly variable daily and intra-day arrival of patients and their disease complexity. As a consequence, it is not unusual to be either short staffed or overstaffed at any time of the day or week. Telemedicine offers an opportunity to respond to these unpredictable variations in a rapid and potentially cost-effective manner by better matching service needs with provider availability.
Telemedicine has been widely deployed in a variety of settings; however, its use in the ED has been more limited and generally focused on providing consultation for specialty services. 12 Provision of psychiatric consultation via telemedicine in an ED setting was found to be as effective as face-to-face specialty evaluations. 13 Critical care consultations on children in rural EDs were found to improve care as compared with telephone only or no consultation. 14 Several reports support the effectiveness of telemedicine for acute stroke assessment to determine safe and timely administration of tissue plasminogen activator in EDs without onsite neurologic specialty support.15–18
A review of the literature uncovered two reports of physician telepresence in an ED triage area. One was a paediatric ED which found physician telepresence to be equivalent or superior to nurse triage in several categories of evaluation. 19 A limited pilot by Traub et al. included 36 patients and supported the safety and patient acceptance of physician telepresence in an ED triage area. 20
The results from this pilot study demonstrate the safety of emergency physician telepresence in the ED along with very favourable ratings by patients and providers which is in line with prior reports. This is the first study to demonstrate a significant reduction in throughput time for patients managed with emergency physician telepresence as an alternative to traditional care when the ED is impacted. Billing of all telemedicine patients was done by the onsite physician as this is currently a requirement for billing purposes. This study and others in telemedicine happening concurrently would be sources of future policy change considerations to more broadly cover telemedicine services. As a result of this pilot study, ED Telemedicine was very favourably viewed by the department and the health system and overall deemed a success. As we were planning to make this part of usual ED care, new opportunities for growth of the program arose thus we decided to put the process on hold temporarily. Our next iteration of EDTITRATE will be to include two additional clinical sites. We are also expanding our base of physicians and operationalizing ED Telemedicine in order to cover several sites at the same time.
One aspect of the telemedicine experience for the patient that was not considered prior to initiation of the program and is worthy of comment is the opportunity for the patient to see what the telemedicine physician sees during the examination. This includes views of oral cavity, pharynx, external ear canal, tympanic membrane and skin findings on portions of the body not otherwise visible to the patient. These are all features that are not generally available during a conventional exam and were repeatedly commented upon by patients. This patient-centred feature involves them in their care in a unique manner, which may have contributed to the highly favourable ratings in some cases.
There was one potential misdiagnosis, the patient that returned and was subsequently diagnosed with possible mastoiditis. The nature of emergency medicine is such that diagnoses are occasionally missed and in many cases a process evolves over time such that the signs and symptoms of a disease are not apparent on an initial visit. This was likely the circumstance in this case because this patient was seen and examined by the onsite physician prior to discharge on the index visit.
The objective of this study was to establish feasibility and safety as well as patient and provider acceptance and impact on throughput. These objectives were all met. Before EDTITRATE can be more generally recommended two additional factors need to be analyzed. Telemedicine needs to be tested in other sites, both academic and community ED settings, to assure exportability. More importantly, the cost effectiveness of this approach to staff augmentation in an “as needed” basis needs to be established. The convenience design of the EDTITRATE pilot did not allow for this evaluation.
Limitations
There are several limitations to this study. The highly favourable patient ratings may have been biased by the enrolment process, which was voluntary and without a randomized comparator group. That being said, the level of patient acceptance was very high and is consistent with the findings in other reports. The throughput times for telemedicine patients was reduced more than 50% when compared with the non-telemedicine patients seen during the same time frame with the same triage categories. However, because this was a convenience study at a single institution, similar reduction in throughput during other times of the day and at other ED settings may not be found. Naturally, adding a provider will create more efficient processes; but, this study aims to allow that provider to be remote and activated only when deemed necessary. A potential limitation is related to connectivity. The physicians had to have internet access on either a desktop or laptop, though location was not a factor as one provider cared for several patients from out of state. There were no reported issues of failed connectivity or hardware malfunctions.
Conclusion
Based upon the limited data in this pilot project, emergency physician telepresence in the ED is potentially safe, though larger studies would need to validate safety; it is viewed favourably by patients and providers who participated in the process, and may reduce throughput time for patients seen by this method as opposed to otherwise waiting. Emergency medicine evaluations and efficiency models can be complex and thus further studies in more diverse ED settings with larger patient groups as well as comparison with other staffing methods are necessary to assess broader application of this approach and to assess its cost effectiveness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant Support: For calendar year 2013, innovation grant support to Dr. Vaishal Tolia from the UCOP (University of California Office of the President) CHQI (Center for Health Quality and Innovation).