
Abstract
Introduction
Under certain circumstances, e-consultations can substitute for a face-to-face consultation. A basic requirement for a successful e-consultation is that the e-consultant has access to important medical history and exam findings along with laboratory and imaging results. Knowing just what information the specialist needs to complete an e-consultation is a major challenge. This paper examines differences between specialties in their need for past information from laboratory, imaging and clinical notes.
Methods
This is a retrospective study of patients who had an internal e-consultation performed at an academic medical centre. We reviewed a random sample of e-consultations that occurred in the first half of 2013 for the indication for the e-consultation and whether the e-consultant reviewed data in the medical record that was older than one year to perform the e-consultation.
Results
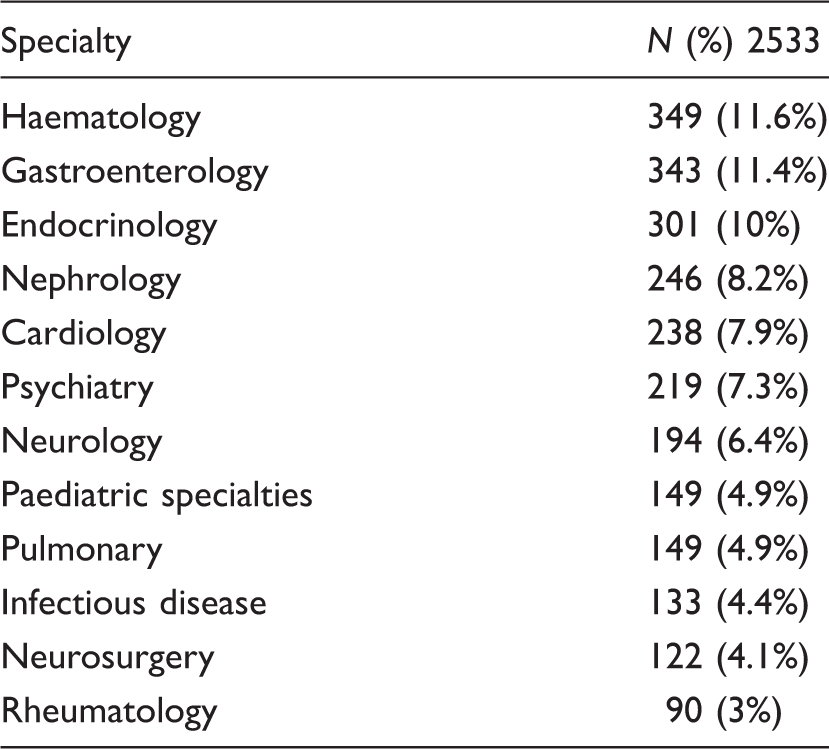
Out of 3008 total e-consultations we reviewed 360 (12%) randomly selected e-consultations from 12 specialties. Questions on management (35.8%), image results (27.2%) and laboratory results (25%) were the three most common indications for e-consultation. E-consultants reviewed medical records in existence more than one year prior to the e-consultation 146 (40.6%) of the time with e-consultants in the specialties of endocrinology, haematology and rheumatology, reviewing records older than one year more than half the time. Labs (20.3%), office notes (20%) and imaging (17.8%) were the types of medical data older than one year that were reviewed the most frequently overall.
Discussion
Management questions appear to be the most common reason for e-consultation. E-consultants frequently reviewed historical medical data that is older than one year at the time of the e-consultation, especially in endocrinology, haematology and rheumatology specialties. Practices engaging in e-consultations that require transfer of data may want to include longer time frames of historical information for those specialties.
Introduction
E-consultations are electronic consultations between health care providers. 1 These can take the form of real time (synchronous) e-consultations using video or asynchronous (‘store and forward’) e-consultations. E-consultations can be between providers in the same medical system (i.e. an ‘internal’ e-consultation) or between providers in different medical systems. E-consultations have been used to improve access to care when geographical or resource barriers exist.2,3 Studies show patients, referring providers and specialist consultants find the e-consultation process satisfactory with providers citing improved timeliness of care, convenience, improved communication and improved access as primary benefits of e-consultations.4-7 E-consultations have been found to decrease the need for face to face consultations 8 with various factors suggested as contributing to the need for subsequent face to face specialty consultation including clinical complexity of the question 9 and how the question is formulated by the referring clinician. 10
Our institution began offering internal asynchronous e-consultations in 2008. Originally available as a request from a generalist to a specialist, the process was liberalized to allow specialist to specialist e-consultations in 2011. Described in more detail in previous publications, 11 most e-consultations are requested by a provider by being entered into an electronic ordering system. Patient care coordinators then arrange for the e-consultation to be performed, monitor for its completion and notify the referring provider once completed. The entire process is performed through the same ordering system that is used in face to face consultation requests, making the process convenient for the referring provider. E-consultations are transcribed and entered into the patient’s electronic medical record (EMR) for the requesting provider’s review. With these internal e-consultations, both the requesting provider and the e-consultant share and have access to the same EMR. Thus any information available to the referring provider is also available to the e-consultant to review without any additional work flow processes. Additionally, as the EMR is the same that is used for all patient care it is familiar to the e-consultant and information should not be difficult to locate in the record for the e-consulting specialist. This process meets the criterion recommended by Zanaboni and Wootton in 2012 that for telemedicine options to be sustainable they should be ‘adopted into everyday practice’. 12
In 2003, Wootton et al. described various potential pitfalls of e-consultations including the possibility of the request not being received, not being allocated for reply or that the requester may not know what data the consultant needs to perform the e-consultation. 1 Internal e-consultations can reveal how much information e-consultants are actually accessing to perform the e-consultation. For healthcare systems without a shared EMR, there is a significant burden to copy and send medical records for the e-consultant to review, but with internal e-consultations, the entire medical record is available to the e-consultant. By examining what data these e-consultants are actually using when they have ready access to all patient data, we can get a better idea of what patient data should be sent when there is no system interoperability.
In this retrospective study, we reviewed internal e-consultations for differences among specialties in the indication for e-consultation and types of data reviewed that were over one year old.
Methods
Setting
The study took place at the Rochester campus of the Mayo clinic, a large multispecialty group in the United States with 4400 physicians and scientists overall and with 2200 physicians and scientists at the Rochester campus.
Data collection and review
We retrospectively identified all internal e-consultations that occurred between 1 January 2013 and 30 June 2013. Twenty-six e-consulting specialties were represented. For further analysis we selected 12 specialties with the highest number of e-consultations. For those 12 specialties we used a stratified random sampling method (by specialty) to obtain e-consultations from each specialty for manual review. We obtained random samples of 40 e-consultations from specialties with large e-consultation numbers and random samples of 20 e-consultations from specialties with lower e-consultation numbers. Both authors independently manually reviewed the randomized e-consultation samples for content.
E-consultation content coding
Categories were coded dichotomously as being either present or absent. Discrepancies in coding were reviewed and agreement by consensus was reached.
We reviewed e-consultations for:
The indication for the e-consultation; Evidence for review of medical records older than one year by the e-consultant; Evidence for insufficient data to adequately perform the e-consultation.
Indication for the e-consultation
E-consultations were reviewed and coded dichotomously (present or absent) for the following indications:
Management – assistance in management of a medical condition; Image – interpretation or further evaluation of image results; Lab result(s) – interpretation or recommendations for further evaluation of lab result(s); Diagnosis – assistance in diagnosis; Test selection – question(s) on what specific test to perform next for evaluation; Test timing – question(s) on when to perform follow-up tests (for example when to perform follow-up colonoscopy after a positive colonoscopy); Medication questions – questions on medication(s); Procedure – questions regarding procedure results; Preoperative concern(s) – questions on pre-operative evaluation or concerns; Physical exam finding – questions on physical exam finding(s).
Evidence for extended electronic medical record review
The e-consultation note was reviewed for any indication that the e-consulting specialist reviewed the patient’s EMR for data that was in existence more than one year prior to the e-consultation. If there was evidence in the e-consultation note that the e-consultant reviewed data from greater than one year from the date of the e-consultation request, the specific type of data reviewed was categorized. Greater than one year medical record review categories were: lab data, office notes, imaging reports, medications, procedure reports, pathology reports and/or hospital notes.
E-consultations could code for more than one category for indication and type of extended record review performed (if review was performed).
Evidence for insufficient data to adequately perform the e-consultation
The e-consultation note was reviewed for statement(s) by the e-consultant that desired or necessary information was not available that would be helpful for the e-consultation. For those e-consultations where insufficient information was present we then reviewed the type of information that was requested.
Study data were collected and managed using REDCap electronic data capture tools hosted at our institution. 13 Statistical analysis and randomization of samples was performed using JMP Pro 11.0.0 (SAS Institute Inc., Cary, NC, USA). The study was reviewed and approved by the Mayo Clinic Institutional Review Board.
Results
Number of total e-consultations for each of the 12 specialties reviewed.
Indication for e-consultation by specialty.
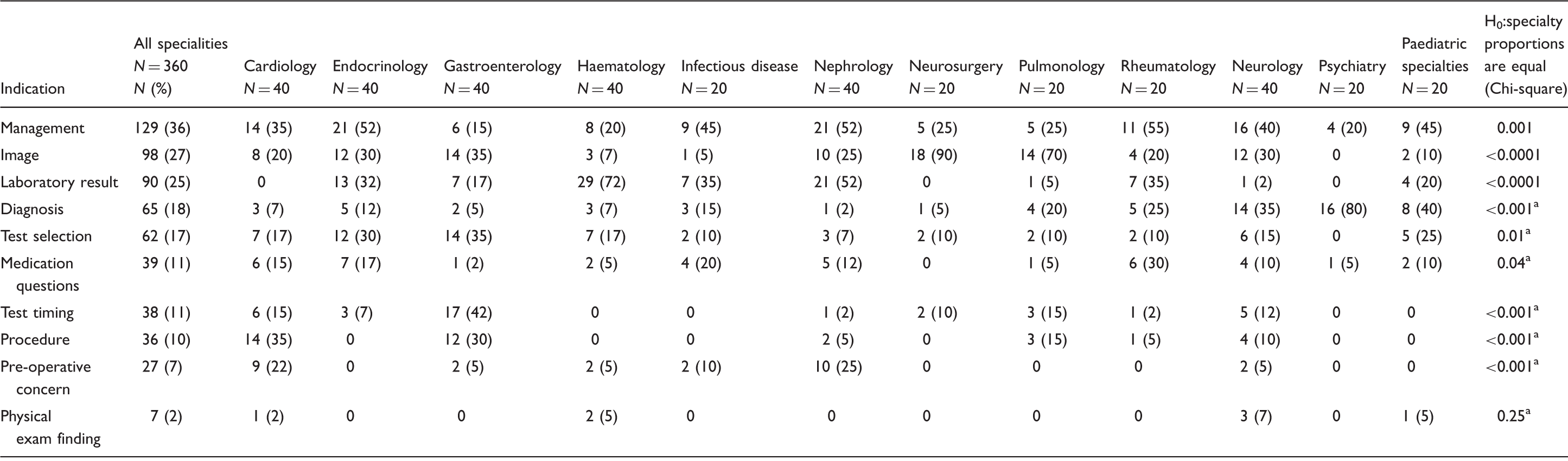
20% of cells have expected count less than 5; Chi-square may be suspect.
E-consultant specialist review of patient records for data older than one year by specialty type and data review type.
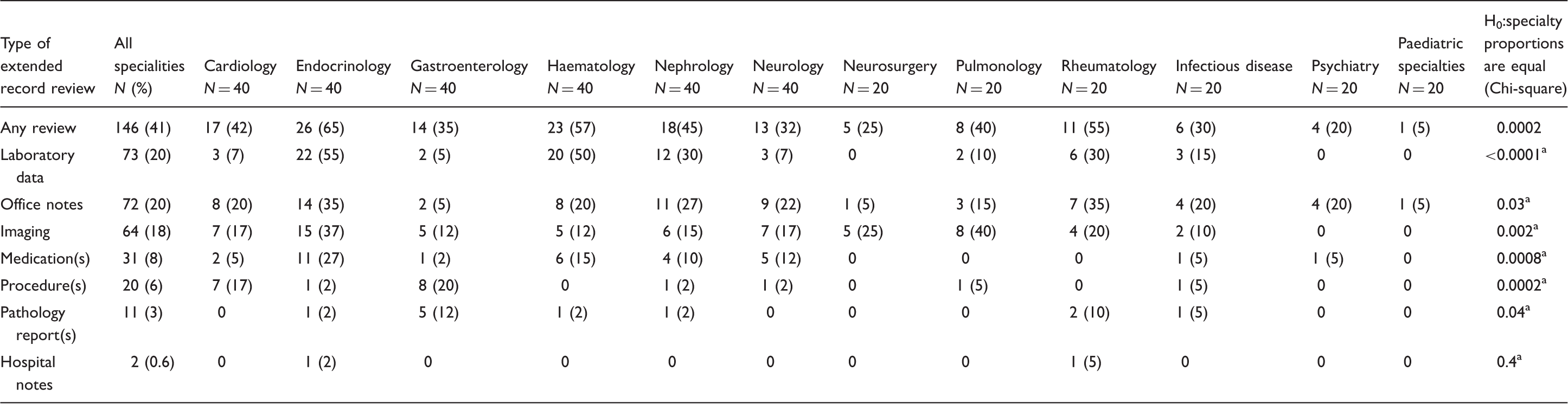
20% of cells have expected count less than 5; Chi-square may be suspect.
Indication from e-consultant of insufficient information available.
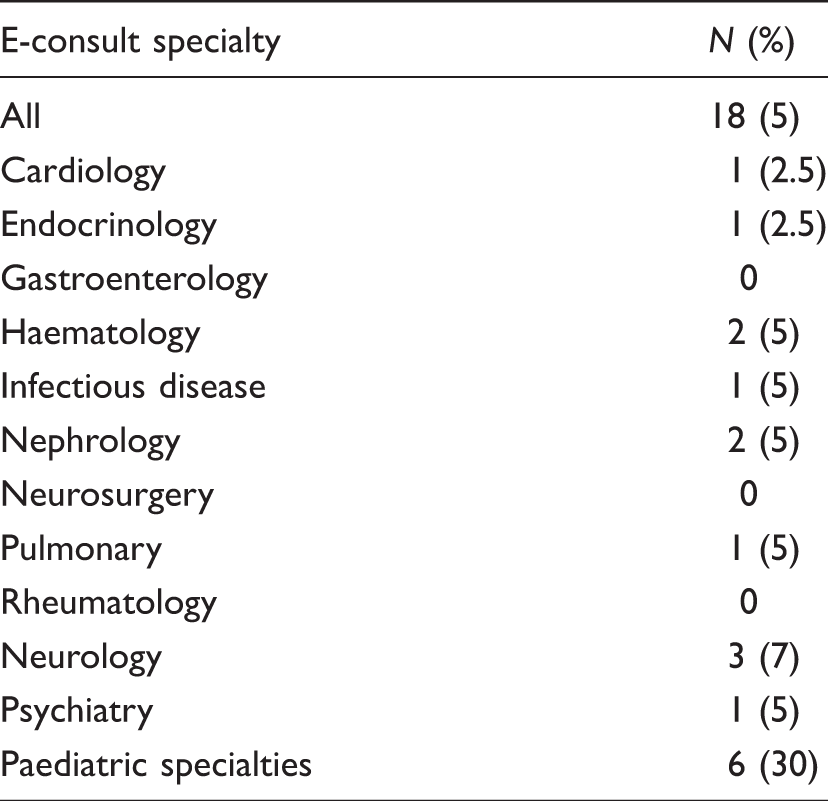
Insufficient data to perform the e-consultation was noted in 18 (5%) of the e-consultations reviewed (Table 4). Of the 18 e-consultations that were noted to have insufficient data 11 of these noted that important historical information in the history portion of the referring note was not available while five noted that historical records (for pathology and lab results) from outside medical institutions should be requested and two noted that physical exam findings were necessary to complete the e-consultation.
Discussion
In our system, where the e-consultant had all of the medical information available that was available to the referring provider, we saw a very low incidence of e-consultations citing inadequate information. Of these, the majority were due to inadequate information in the history from the referring provider though a few were from lack of outside records. We saw e-consultants respond to this scenario in three ways. Some e-consultants took a direct approach with a collegial call or message to the referring provider to obtain the necessary information. Others took a less direct approach to the perceived lack of information by requesting in the e-consultation note that the referring provider resubmit an e-consultation after obtaining the needed information or recommending that a face to face consultation be ordered. Additionally, some e-consultants provided conditional recommendations such as ‘if physical exam finding “a” is present then I recommend test 1, 2, 3 be performed. If “a” is absent then no further evaluation should be needed’. While this approach is quite scalable when occurring 5% of the time, it may be more problematic in a situation of inter-institutional e-consultations if not all medical data available to the referring provider are available to the e-consultant. Della Mea describes the two ways in which information can be transmitted for telemedicine: either in toto or by sampling (where the sender reviews the data and sends what is deemed relevant). 14 Wootton et al. have described concerns that e-consultations could be negatively impacted if the referring provider does not know what data the e-consultant needs to complete the e-consultation. 1 For systems that use the sampling method likely the most recent records (such as the lab or image that prompts a question) would be sent for review. Wootton et al. considered adequate relevant information sent with the e-consultation request to be a quality indicator for e-consultations. 15 Our study can help institutions start to hone in on the correct amounts and type of data to send along with an e-consultation request so that the e-consultant gets adequate information to complete the e-consultation. One of the strengths of our study was that the internal e-consultation represents an ‘idealized’ e-consultation system where there are minimal data barriers and any data that were available to the referring provider were available to the e-consultant without the need for special processes to transmit the information. This allowed us the opportunity to assess what historical data could be useful for completion of an e-consultation. By reviewing when, how often (and in what specialties) year old or older medical data were reviewed by the e-consultant, we were able to gain insight on what data may be necessary to complete the e-consultation. Our study suggests that older historical data may be quite valuable in certain specialties. For practices implementing e-consultations without a shared EMR, this study is a first step in examining what e-consultants are really looking at to make their recommendations. Our finding that endocrinologists, haematologists and rheumatologists are examining information greater than one year old more than half of the time can help healthcare systems prioritize what they copy and send to e-consultants with a referral request. Additionally, although the specialties of neurosurgery and pulmonology reviewed older medical data less frequently than the above specialities, they appeared to primarily review older imaging studies. Review of medications used, pathology reports and procedure notes older than one year occurred infrequently with the exception of the specialties of cardiology (procedure notes), gastroenterology (procedure and pathology reports) and endocrinology (medication review). E-consultants in paediatric specialties almost never reviewed older medical records. Review of hospital notes for time periods greater than one year prior to the e-consultation was also extremely rare for all specialties. This information suggests specifically what older data for what specialties to include when actually transferring data for an e-consultation. For systems without data interoperability, templates on which information to send for specific indications to specific specialties could be developed. To satisfy the specialists’ need for information, future studies will need to better define what subset of patient information should be sent and how far back in medical records to review. Our study is a step in that process to show the importance of historical medical data for e-consultants.
We only found two occasions in which the e-consultant determined that physical findings were necessary to complete the e-consultation. The retrospective design did not allow us to determine whether the e-consultant would have been satisfied with a more specific or more detailed exam done by the referring provider or if a specialist physical exam was absolutely necessary. Either way, lack of a ‘hands on’ physical examination by a specialist does not appear to be a barrier in the vast majority of these e-consultations.
Limitations of our study include that our methodology only collected information that was specifically reported in e-consultants’ notes. E-consultants may have reviewed older medical data without commenting on it in their notes. Thus it is possible that we have underestimated how often the older record review was occurring. Additionally, our methodology does not allow us to distinguish whether the review of medical data more than one year old was absolutely necessary for the e-consultant to complete the e-consultation or if the e-consultation could have been satisfactorily rendered without that review.
Conclusions
Management questions appear to be the most common reason for e-consultation. A sizable percentage of the time (40%) e-consultants are reviewing historical medical data that is older than one year at the time of the e-consultation, especially in endocrinology, haematology and rheumatology specialities. For this reason, providing historical records older than one year may facilitate e-consultations in these specialties particularly. For endocrinology, haematology and rheumatology e-consultations, historical lab data would be most helpful to include while historical images would be most useful for pulmonary and neurosurgery e-consultations.
Footnotes
Acknowledgements
Author contributions: JLP contributed to study design, acquisition of data, statistical analysis and drafting of the manuscript. FN contributed to study design, acquisition of data and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.