
Abstract
Background
Subacromial impingement syndrome poses a substantial socioeconomic burden, leading to significant consumption of healthcare. Health systems are calling for greater evidence of economic impacts of particular healthcare services. Telerehabilitation programmes have the potential to reduce costs and improve patient access as an alternative to traditional care. Cost analysis has been traditionally included in study protocols and results, although the reliability and research methodology have frequently been under debate. The aim of this study was to compare costs related to a telerehabilitation programme versus conventional physiotherapy following subacromial decompression surgery (ASD).
Methods
The study was embedded in a randomised controlled trial. The economic analysis was based on the perspective of the health sector and the human capital method. Only the costs associated with the provision of physiotherapy services were taken into account. Costs were measured during the intervention period between baseline and 12 weeks for both groups. Student’s t-test was used to compare independent variables between the two groups, with a 95% confidence interval for the estimates and real costs.
Results
The estimated total cost analysis shows a preliminary cost differential in favour of the telerehabilitation group, meaning that for each participant’s total intervention, telerehabilitation saves 29.8% of the costs. Real cost analysis, only for received treatments, shows a cost differential in favour of telerehabilitation, meaning that for each participant’s total intervention, telerehabilitation saves 22.15% of the costs incurred for conventional rehabilitation.
Conclusions
Our study provides direct and meaningful information about telerehabilitation opportunities and can be an essential component in further cost evaluations for different strategies after surgical procedures. This study demonstrates that there was a trend towards lower healthcare costs after ASD. Managers now have the responsibility to decide whether to implement telerehabilitation based on clinical and economic data.
Keywords
Introduction
Subacromial impingement syndrome poses a substantial socioeconomic burden. It has a reported prevalence between 70 and 200 per 1000 adults, leading to a significant consumption of healthcare resources and productive losses from employee absenteeism. 1 A socioeconomic study with a 6-month follow up of patients with shoulder pain estimated an average cost of 652€ per patient in healthcare, and the total cost was 4139€, counting the average economic loss associated with absenteeism. 2
Economic analysis is of central importance to telerehabilitation (TR) because the main rationales for its introduction have been to decrease the cost of delivering healthcare, make more efficient use of the health workforce, and improve timely and equitable access to services. 3 From that perspective, the fundamental goal of any health system is to maximise the level of health of the population it covers. 4 As the healthcare system experiences increasing demand and resource constraints, policy makers, investors and other stakeholders are calling for greater evidence of the health and economic impacts of particular healthcare services. 5 It is noteworthy that the role of health professionals in determining priorities is receiving much attention recently, as it is on the basic level where decisions are made about what kind of healthcare intervention is required, how it is done, and who applies it. 4
Physiotherapy (PT) cost analysis has been carried out in different post-surgical interventions, such as hip fractures, 6 knee replacement, 7 arthroscopic rotator cuff repair, 8 rehabilitation programmes for an implantable cardioverter-defibrillator, 9 and PT programmes after thoracoscopy. 10 Because TR programmes promise to reduce costs and improve patient access, as an alternative to traditional care, cost analysis has traditionally been included in study protocols and results.11–14 A recent research report funded by the APTA (American Physical Therapy Association) concludes that the quality of the literature regarding the cost-effectiveness of physical therapy is very good, although the magnitude of this body of literature is small. 5
TR is a term used to describe the provision of rehabilitation services at a distance using telecommunications technology as the service delivery medium. 15 The reliability of the cost estimates and varying research methodologies has been frequently under debate. 16 It is important to complement studies of TR effectiveness with economic and cost analysis.17,18
The present study was embedded in a large, randomised controlled trial (RCT) evaluating the non-inferiority of TR interventions compared with face-to-face therapy after arthroscopy for subacromial decompression (ASD). 19 The aim of this study was to compare costs related to TR programmes versus conventional PT following ASD.
Methods
The trial was registered at ClinicalTrials.gov (identifier: NCT02909920, 14 September 2016). This was a single-blind, prospective, randomised clinical trial in the rehabilitation service of the Hospital Costa del Sol in Spain. 20 The study was approved by the ethics committee, and written consent was obtained from all participants. The study includes adults between 18 and 65 years of age who were diagnosed with subacromial syndrome (shoulder impingement syndrome, SIS) according to the 10th revision of the International Classification of Diseases ICD-9 CM 726.10, 726.12, and 726.19. 20 The subjects underwent surgical procedure arthroscopically (subacromial decompression with partial acromioplasty, with or without coracoacromial release) or surgical codes related to SIS. 21 Furthermore, patients had to have lived in Spain during the intervention phase, have computer equipment with internet connection (including one of the following devices: personal computer, notebook, tablet or smartphone), and be able to access it frequently and have an existing email account. Exclusion criteria included patients who have had surgery on the shoulder before the first contact with this research, those whose interventions are not based on surgical codes recommended for SIS, and those who do not have full cognitive abilities to allow the use of new technological tools.
After the surgery, the patients were randomly assigned to either a TR group or traditional PT group using a computerised random number generator and opaque sealed numbered envelopes. We developed a TR system to provide services to patients who have undergone shoulder arthroscopy. Patients in the TR group received a customised exercises programme through a web application that allows the physiotherapist to generate videos, images, and parameters of each exercise programme and send them via email. The TR programme included videoconferencing and a self-workout video exercise. Subjects received 12-week (5 days/week) self-workout video exercises following the TR programme, as well as a supporting document called the Telerehabilitation Patient Manual (this document included an exercise tracking sheet to be used by patients in the TR group).
The PT group received face-to-face physical therapy (manual therapy, home exercise programmes and other PT techniques) in a 12-week programme (5 days/week). The primary outcome of the trial was the Constant–Murley score, which has subscales representing pain, daily life activities, range of motion and strength. During their participation in the project, all participants underwent four assessments: baseline, 4 weeks, 8 weeks and 12 weeks. Data were collected by a blinded evaluator.
This economic evaluation followed international guidelines for conducting a cost analysis alongside a randomised clinical trial. 22 Health economic evaluation is conducted to assist rational decisions in health politics. Economic evaluation provides information on the costs, outcomes, and efficiency of medical technologies and supports decisions on whether new technologies should be adopted in the healthcare system. 23 The basic approaches of health economic evaluation are cost-minimisation analysis, cost-effectiveness analysis, cost–utility analysis, and cost–benefit analysis. 23
Preliminary results about TR effectiveness after ASD have recently been published; 24 therefore, the least costly among alternative interventions was determined through a cost-minimisation analysis. 5
This economic analysis is based on the perspective of the health sector, which means that only health intervention costs will be considered, not costs relevant to the patient. Direct costs are essentially monetary transactions involving both health services and products for health. 25 Direct costs to health are considered directly related to the specific intervention evaluated and include costs of hospitalisation, treatment, professional fees, laboratory testing, rehabilitation, and medical equipment, among others. 4 In our study, only the costs associated with the provision of PT services were taken into account. 25 Costs were measured during the intervention period between baseline and 12 weeks for both groups.
In contrast with other studies that require highly complex technology platforms, software installation, and multidirectional cameras for clinical control connecting the physical therapist and the patient, 26 our intervention generated few obstacles, as it is available on any device that allows internet, and patients usually have a desktop, laptop, tablet or smartphone, allowing access from any location and different devices.
Costing
We used three steps for the costing procedure throughout this study:
Identification of relevant cost items (direct and indirect costs) Valuing the identified items (in €) Quantification of the use of the identified cost items.
Identification of relevant cost items (direct and indirect costs)
Costs were divided into categories: (1) costs related to the clinical aspects and (2) costs related to the technology. For each of these cost categories, direct costs were defined as essential for the delivery of the clinical intervention, and indirect costs as related to the intervention without being part of it. The cost evaluation was based on all registered actions related to PT services during the measured period. Relevant study items and cost items are described hereinafter.
Relevant items
Direct clinical time was defined as the duration of the interaction between physiotherapist and participant to deliver the intervention in both groups.
Indirect clinical time was defined as the time required to optimise the intervention (i.e. scheduling, file preparation, planning the treatment, writing the report and follow-up notes) without direct contact with the participant.
Direct technology costs were defined as the costs in € for acquiring the TR programme licence for patients in the TR group.
Indirect technology costs included the cost to provide information about and education for platform use, as well as technical assistance for internet and connection issues for the TR group.
Valuing the identified items (€)
The economic cost analysis in this study is based on the human capital method. The standard hourly salary in effect at the time of the study was applied to the time spent by the physiotherapists and technicians (11.03€/hour and 10.46€/hour, respectively) in both groups. We used economic references published by the official bulletin of the province of Málaga (Spain)27,28 at the time of the trial. A minimum annual cost of 19,847.64€ for physiotherapists and 18,827.49€ for computer technicians at a maximum of 1800 hours yearly was used to calculate the cost per hour. Costs were calculated in Euro (€) (1€ = 1.47 AUD; 1.17 USD).
Quantification of the use of the identified cost items
Usually, a physiotherapist serves two patients per hour with the characteristics of participants in this study, exclusively for the PT group. Therefore, 50% of the value for each item was considered. Thus, in a 12-week (5 days/week) programme, a minimum total cost of 331.2€ per patient was estimated (5.52€/treatment). For the indirect clinical cost, a minimum of 4 hours with the assessment points were considered accordingly, with an estimated cost of 44.12€ per patient.
In the TR group, two initial videoconference sessions (30 min/session) were included, with a total cost of 11.03€/hour per patient. Once a week the physiotherapist held a 30-minute control session that allowed adaptation of the programme and monitoring of developments. Therefore, a cost of 66.24€ was estimated for the 12 control sessions. For the indirect clinical cost, a minimum of 4 hours with the assessment points were estimated accordingly, with a cost of 44.12€ per patient. The licence to use the TR programme had a fixed cost of 100€ per patient, defined as the direct technology cost.
Quality rating
This study was assessed according to Chiou’s grading system of the quality of health economic analyses 29 with a value of 71 points, which is considered a good-quality study. 30 This system contains 16 weighted items developed by an expert committee; some items are applicable to research in general, such as the clarity of the study objective, use of reliable and valid health outcome measures, the methodology for data abstraction, use of statistical analysis, discussion of bias, justified conclusions, and disclosure of funding source. 3 Results of the quality health economic analysis (QHES) are shown in Supplemental material 1.
Statistical analysis
The central hypothesis of the study was tested by comparing costs in both groups. Student’s t-test was used to compare independent variables between the two groups with a 95% confidence interval.
Results
Breakdown of costs for telerehabilitation and traditional physiotherapy.
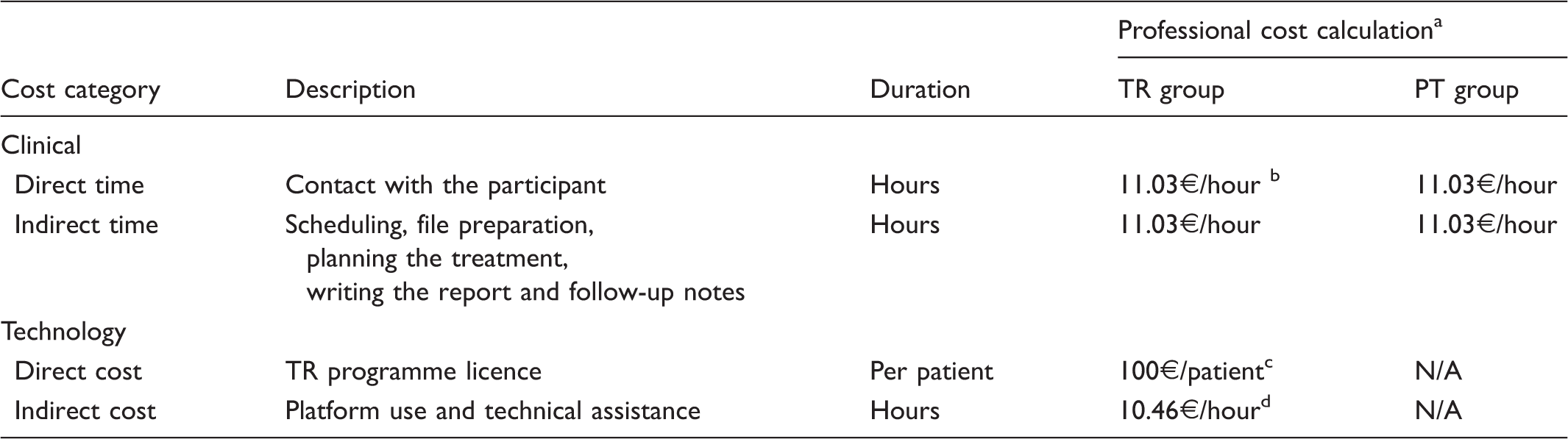
TR: telerehabilitation; PT: physiotherapy; N/A: not applicable.
All costs are in euros.
Physiotherapist’s hourly salary.
Cost for TR programme licence per patient.
Technician’s hourly salary.
Baseline characteristics of patients with shoulder impingement syndrome undergoing arthroscopy for subacromial decompression (n = 18).

SD: standard deviation; TR: telerehabilitation; PT: physiotherapy; SE: standard error.
Estimated and real costs (received and cancelled)
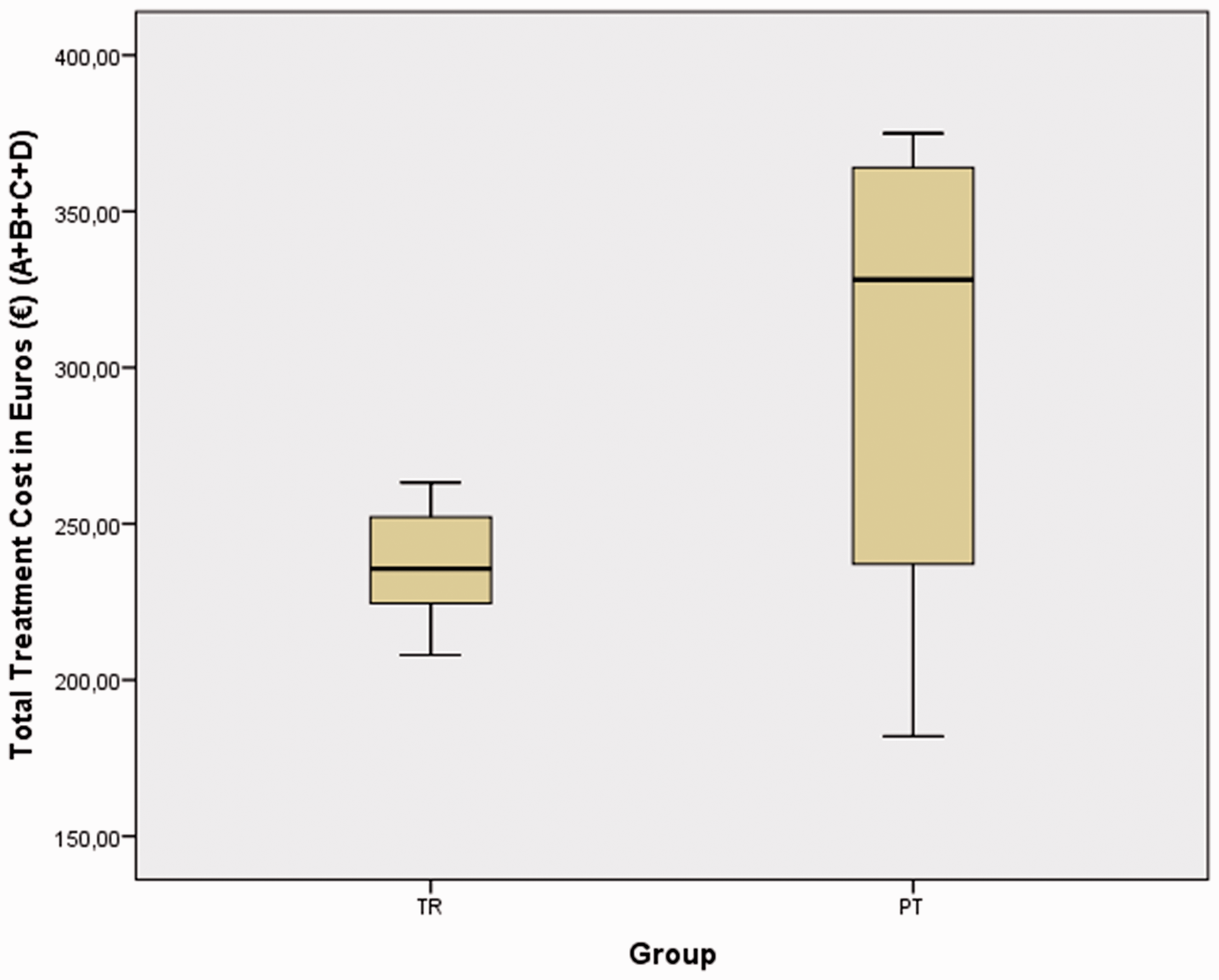
In the randomised trial, some participants from the TR group and PT group did not receive all scheduled treatments due to medical, technical or personal reasons. Because there are expenses associated with cancelled treatments, the estimated cost analysis took into account all planned costs, the cost of treatment given plus the cost of cancelled treatment. The estimated total cost analysis shows a preliminary cost differential in favour of the TR group (TR 263.17€ to PT 375.02€), meaning that for each participant’s total intervention, TR saves 29.8% of the costs incurred for conventional rehabilitation following ASD.
The total estimated cost for the TR group included two initial videoconferences (11.03€), 12 control session videoconferences (66.18€), four indirect clinical time sessions (44.12€), four technician hours (41.84€), and a licence-per-patient cost (100€), as was described in the quantification of use of the identified cost items. Real cost analysis for received treatments only shows a cost differential in favour of the TR group (236.97€ ± 8.55) compared with the PT group (304.42€ ± 22.10), meaning that for each participant’s total intervention, TR saves 22.15% of the costs incurred for conventional rehabilitation following ASD.
Discussion
The purpose of this study was to document costs for a TR programme versus traditional PT after ASD based on an RCT. To our knowledge, this is the first cost analysis of a TR programme involving the cost structure for this type of service in that group of patients. We included all subcosts related to the TR technology (programme licence and technical services).
Economic decision-making is based on a comparison of costs and effects. If an intervention is dominant (i.e. has greater effects and lower costs), then the decision is clear that the dominant treatment would be the preferred treatment. 31 Cost-analysis studies have been carried out in several pathologies and interventions.32–36 A long-term exercise training study in patients with stable chronic heart failure showed cost-effective results that prolong survival by an additional 1.82 years at a low cost of $1773 per life-year saved. 32 The ‘Active Project’, an RCT comparing the effectiveness of two different interventions demonstrated that lifestyle intervention was more cost-effective than a structured intervention. 33 In a Dutch study with 120 outpatients with ankylosing spondylitis, a cost-utility measurement using the EuroQol (EQ-5Dutility) was added to the effectiveness measurement, providing new knowledge regarding the usefulness of interventions. 34 In a study in children with juvenile idiopathic arthritis, the productivity costs of the parents was added in addition to the costs of health service resources; results showed no evidence to justify the costs specifically for use in this disease. 35 Finally, a study in patients with osteoarthritis of the hip and knee demonstrated no differences between groups with respect to any of the outcome measure improvements, as well as less cost in the behavioural intervention compared with usual care, but this difference was not significant. 36
Therefore, if the hypothesis that results of the TR intervention are not inferior to traditional therapy is confirmed throughout the RCT, it would be a key issue to justify implementation of TR. The cost analysis conducted in this trial supports the use of TR in cost-saving conditions. Our results show that delivering a TR programme is less expensive than providing the traditional PT service by at least 22–29% in patients following ASD.
Other interventions require software installations on specific devices, whereas our intervention is available on any commonly possessed, internet-enabled device (desktop, laptop, tablet and smartphone), allowing access from any location and different devices. This contrasts with other studies that require highly complex technology platforms, software installation, and multidirectional cameras for clinical control in order to connect the physical therapist and the patient. 27
At the time of the RCT, the TR licence cost per patient was calculated only for the trial. A substantial reduction in the TR licence cost (–30–50%) is expected when the platform is recruiting for larger populations, as has been informed by the provider. In addition, the reduced number of administered sessions compared with the estimated number in the PT group had a direct correlation in total cost difference. The PT group spent only 81% of the total estimated cost in contrast with the TR group that spent 90% of the total estimated cost. This result allows us to predict better budgets and cost estimates for PT interventions after surgical procedures.
If a TR programme has cost saving of at least 22–29%, this is a new way to increase the budget for rehabilitation services and cover a larger population. For example, a reduction of 29% in a 1 million/euro budget is 290.000€. This reduction could be optimised for new patients needing the best healthcare services. Innovative ways of managing rehabilitation budgets in patients after musculoskeletal surgery need robust research.
There are some limitations of this analysis. The follow-up period was a short time frame of 12 weeks; therefore, the long-term impact on costs, quality of life, and time off work cannot be estimated. This study does not consider previous physical therapy or conservative treatment costs in the results. It included only individuals who have internet-enabled devices and access to the internet; thus, we do not have information about costs to provide devices and access to the internet for people without resources. This study does not consider costs related to the patients, such as workers’ compensation, absenteeism, and travel costs. The limited number of subjects in the preliminary results of the RCT does not allow extrapolation of those economic parameters. Further economic studies could show whether TR can be applied to other categories of patients.
Real costs of telerehabilitation and traditional physiotherapy.

TR: telerehabilitation; PT: physiotherapy; SE: standard error.
Total cost is for real intervention, which includes only received treatments. Patient licence (100€) and technician assistance (41.84€) were included for the TR group. All costs are in euros.
Real total cost in both groups.
Footnotes
Acknowledgements
All authors have made significant contributions to this article. JMPB coordinated the project, contributed to the conception, design of the study and drafted the manuscript. RMV and FJBL were responsible for the methodological guidance, analysis and interpretation of data. All authors read and approved the final manuscript as submitted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMPB, the corresponding author, owns the commercial licence of web My-fisio (exercise prescription software) used as a telerehabilitation tool.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.