
Abstract
Background and aim
Deploy and evaluate a gastroenterology (GI) electronic consultation (e-consult) program. E-consults are a promising approach to enhance provider communication, facilitate timely specialty advice and may replace some outpatient visits.
Study
As part of our health system’s efforts to provide more cost-effective care under risk-based contracts, we implemented an e-consult program where referring providers submit patient-specific clinical questions electronically via an electronic referral system. A GI consultant then reviews the patient’s record and provides a written recommendation back to the referring physician. For our program evaluation, we conducted chart reviews of each e-consult to understand how the program was being used and surveyed the participating providers and consultants.
Results
From September 2015 to March 2016, we received 144 e-consults, with most questions concerning GI symptoms or abnormal hepatology labs. Only 36% of e-consults recommended an in-person GI consult or procedure. In our survey of participating providers, referring providers strongly agreed that the GI e-consults promoted good patient care (88%) and were satisfied with the program (84%). The majority of GI consultants felt strongly that e-consults were useful for referring providers and their patients, but that current reimbursement and time allotted were not adequate.
Conclusions
We report on the implementation of a GI e-consult program within an ACO, showing that many clinical questions could be answered using this mechanism. E-consults in gastroenterology have the potential to reduce unnecessary visits and/or procedures for patients who can be managed by their primary provider, potentially increasing access for other patients.
Introduction
Electronic consultations (e-consults) are a promising approach to enhance provider communication, facilitate timely specialty advice and may replace some outpatient visits. E-consults are defined as “an asynchronous consultative communication between providers occurring within a shared EHR or secure Web-based platform”. 1 As demand for consultant services continues to rise, thereby increasing wait days for specialty care appointments, specialty providers such as gastroenterologists (GI) should look for novel ways to help expedite and improve patient’s access to care.2,3 At the same time, large comprehensive electronic health records (EHRs) are becoming widespread and allow consultants to review a significant amount of information and address many specific questions without an in-person consultation. 4 Unlike “curbside consults”, e-consults provide structure and reimbursement for the consultant. 5 Several specialties have demonstrated the feasibility of e-consults including rheumatology, cardiology, vascular medicine, diabetes and endocrinology.6–11 Patients and providers in GI may benefit from e-consults, as the need for an in-person consult, procedure, radiograph, or additional testing may be addressed without seeing the patient in the office.
Programs such as e-consults allow for increased communication and education between providers, as well as expedite care for patients who do not require in-person specialty consults. While e-consults are provider-to-provider interactions, patients may also benefit from their use. The 2014 Merritt Hawkins Physician Appointment Wait Times and Medicaid and Medicare Acceptance Rates Physician Survey found that the average wait time for a specialty care appointment was 18.5 days across 15 metropolitan markets. 12 While this report did not include GI practitioners, demand for specialty services, including GI, has been steadily climbing.3,13
The emergence of accountable care organisations (ACOs) in the United States has created new incentives to reduce the unsustainable growth in utilisation and spending. 14 Our institution comprises both an academic medical centre, as well as community health centres, all of which are part of an integrated healthcare network whose providers use a shared electronic medical record system. Our institution also participates, as an ACO, in multiple risk contracts with both private and government payers and is therefore incentivised to provide more effective, coordinated care while reducing costs utilising population health management tools such as e-consult.14,15 As new value-based payment systems are being developed as part of the Medicare Access and CHIP Reauthorization Act (MACRA), specialty providers should be proactive regarding the implementation of innovative care delivery methods, whether or not they belong to an ACO. To our knowledge, there are few publications regarding utilisation and implementation of a gastroenterology-based e-consult program. We therefore describe our initial experience with a gastroenterology e-consult program at an academic medical centre.
Materials and methods
Study population
The Massachusetts General Hospital (MGH) is a large tertiary academic medical centre and teaching hospital, with multiple primary care practices and community health centres located throughout eastern Massachusetts. The Division of Gastroenterology at MGH performs more than 27,000 procedures and 25,000 consults annually, with 38 staff physicians, eight nurse practitioners and 16 fellows practising in our hospital-based location, as well as three community-based ambulatory centres. As experienced nationally, patients experience lengthy delays ahead of being seen in the office, as we do not have enough gastroenterologists or physical space to expeditiously meet demand for our services. 13 Of these 62 providers who were part of our division at the time of program deployment, six attending physicians initially participated as GI “e-consultants”.
GI E-consult program
Our GI e-consult program was launched in September 2015. Referring providers submit questions on any GI topic, along with a brief patient history, via our internal referral system. These requests are routed to a single GI physician lead who performs an initial review for appropriateness and then forwards appropriate e-consult requests to subspecialty GI providers for consultation. Criteria for deferral of an e-consult request include: (1) need for an in-person encounter; (2) not enough clinical information in the electronic record; and (3) complexity of patient and/or clinical question.
The GI e-consultant providers then respond to the appropriate e-consult requests by reviewing the patient’s most recent visit and/or testing. The consultant responds to the e-consult request with a brief note in the medical record detailing their recommendations for management and guidance for next step, including when it is appropriate to refer for an in-person consult. The referring provider then communicates with the patient and arranges any necessary testing or follow-up. The consultant is directly paid a flat fee ($52) per e-consult from internal funds from the hospital’s physician organisation, which is currently paid separately from salary. Patients may have been aware that an e-consult was requested but generally had no direct contact with the consultant, and there was no charge assessed to the patient or their insurance.
Our GI program was the fourth specialty e-consult program launched at our institution, which was announced to referring providers in our hospital via newsletters, email bulletins and staff meetings.
Data collection and analysis
We collected data from the first six months of the GI e-consult program (September 2015 to March 2016). We conducted a review of the requests submitted, e-consults performed, as well as the recommendations made. We collected data on the types of referring providers who sent e-consult requests, as well as basic demographic data on the patients for whom the e-consult was requested. All e-consult requests and related notes were reviewed by a gastroenterologist. This physician reviewer then assigned clinical categories to each of the e-consult requests which were classified by GI subspecialty. We also collected data on whether in-person GI follow-up (in-person consult and/or procedure) was recommended as a result of the e-consult request. For patients who had an e-consult, the patient’s medical record was reviewed by the physician reviewer to determine whether they ultimately had an in-person GI consult or procedure within the 90 days following the e-consult. Lastly, we reviewed the medical record of all patients with e-consult requests to look for emergency department or urgent care visits within 30 days of the e-consult request to assess whether there were any adverse events related to the e-consult subject.
Six months after introducing this service, we surveyed both the referring providers and GI e-consultants about the program’s value, its impact on patient care, and usability according to a Likert scale (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree). We based our survey questions (Appendices 1 and 2) on those utilised by prior e-consult studies at our institution. Our surveys were developed in an internal research computing tool, which provides a secure web application for building and managing online surveys and databases. Participation was voluntary and all survey responses were kept anonymous.
As this work was performed primarily as an implementation review of a new operational program, it was exempt from review by our institutional review board.
Results
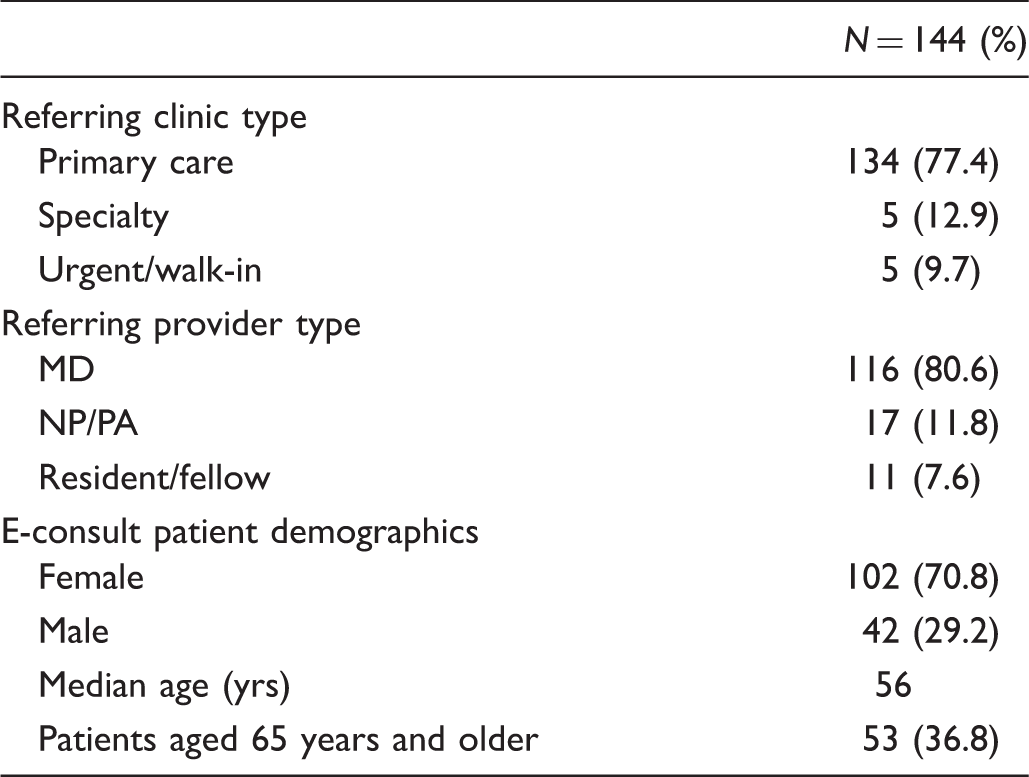
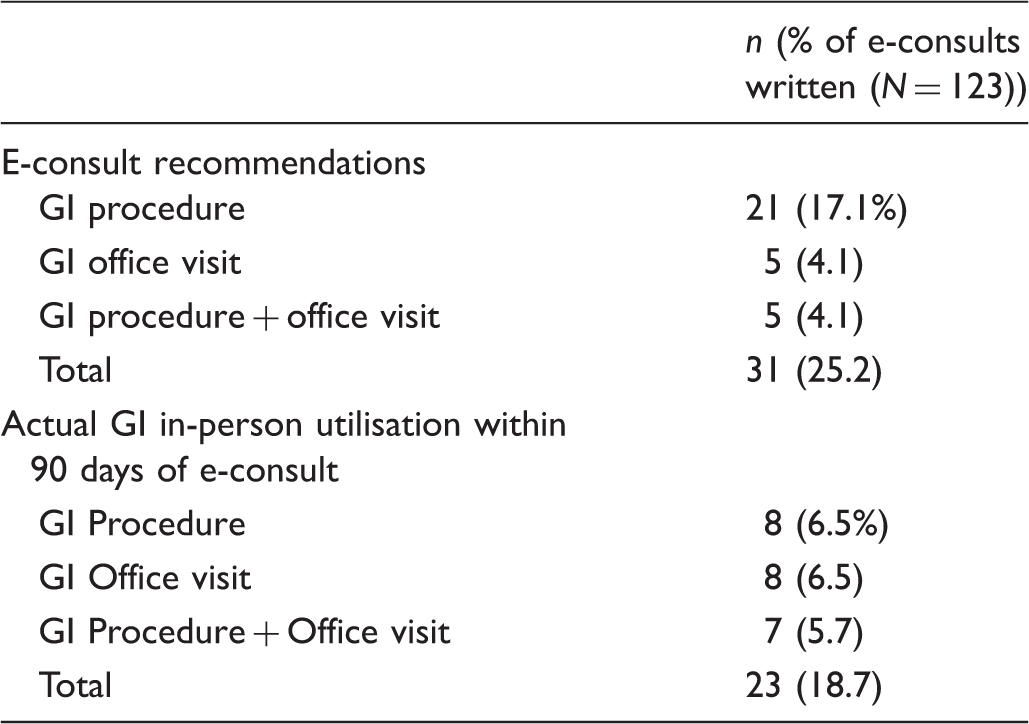
From September 2015 to March 2016, referring providers made 144 e-consult requests, which were triaged by our e-consult physician lead (Figure 1). Twenty-one (21) of these requests were deferred as not appropriate for e-consult and converted to a traditional consult or procedure. The triaging GI e-consultant typically deferred requests if a patient required an in-person work-up, if there was insufficient information in the electronic medical record to answer the clinical question, or if the question(s) being asked were unclear or too complex to answer without an in-person visit. The remaining 123 e-consult requests were answered by our GI e-consultants, returning recommendations within two business days in 97.9% of the cases. Our study team reviewed all 123 e-consult notes and found that only one quarter of these notes recommended a GI procedure (21), a traditional in-person consult (five), or both (five) as next steps (Figure 1). The remaining 64% e-consults did not recommend a GI procedure and/or traditional in-person consult but rather gave recommendations such as reassurance, communication of guidelines and indications for further testing.
Flow diagram of gastroenterology e-consult requests (Sep 2015–Mar 2016).
GI e-consult requests.
GI e-consult question categories.
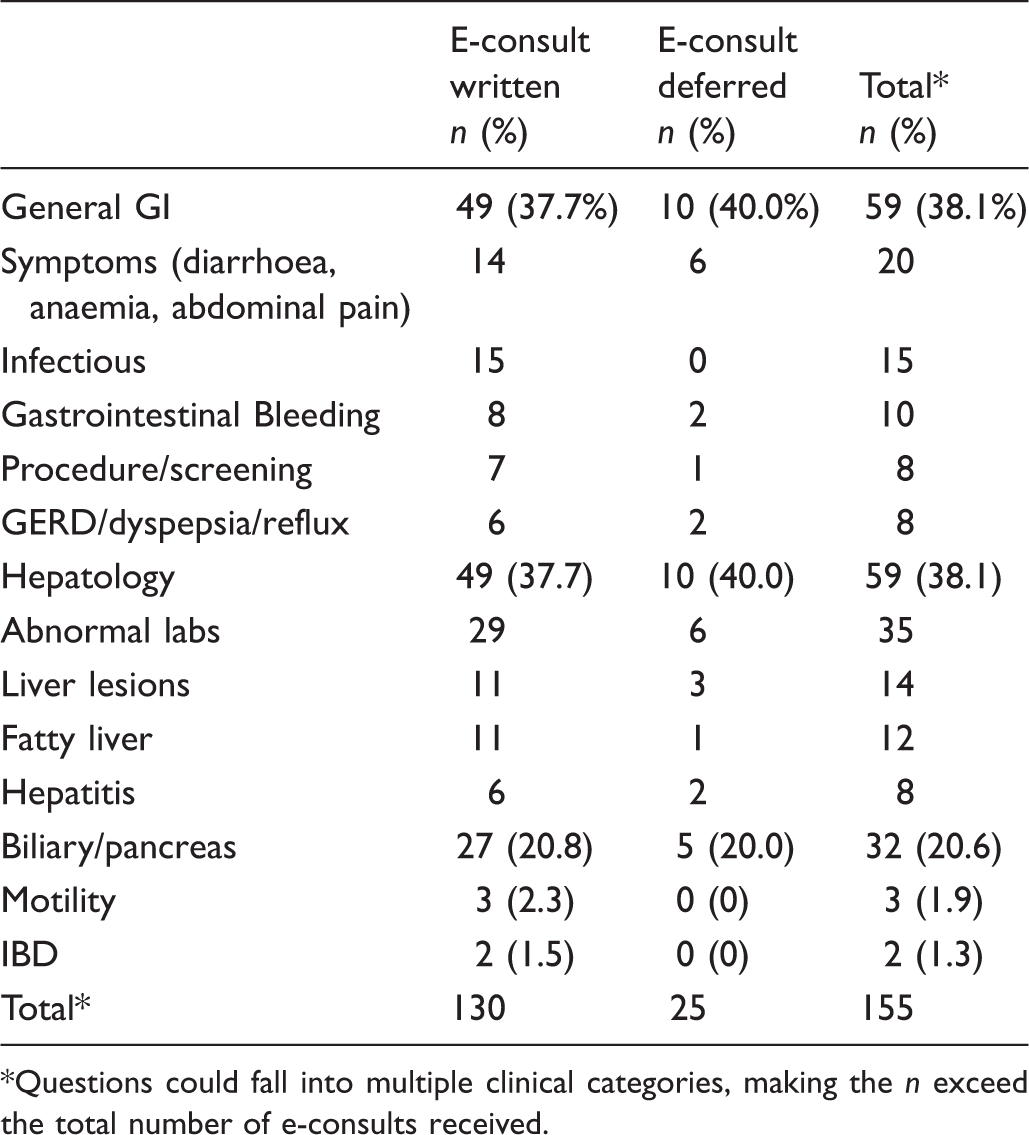
Questions could fall into multiple clinical categories, making the n exceed the total number of e-consults received.
GI e-consult outcomes.
We invited all 85 referring providers who submitted GI e-consults during the first six months of the program to participate in a survey and received 32 responses (response rate of 38%) (Figure 2). Referring providers strongly agreed that the GI e-consult program promoted good patient care (88%) and were satisfied with the service (84%). Responses were more divided regarding whether e-consults helped prevent additional testing such as labs and imaging (52% Strongly Agreed). In addition, there was not strong agreement as to whether use of e-consults avoided an in-person GI consult and/or procedure (60%). Most referring providers, however, did strongly agree that the e-consult recommendations they received from GI were clear/easy to understand (78%), and strongly agreed that they would use or recommend the GI e-consult program in the future (84%).
Referring provider survey responses (n = 32). GI Consultant survey responses (n = 6).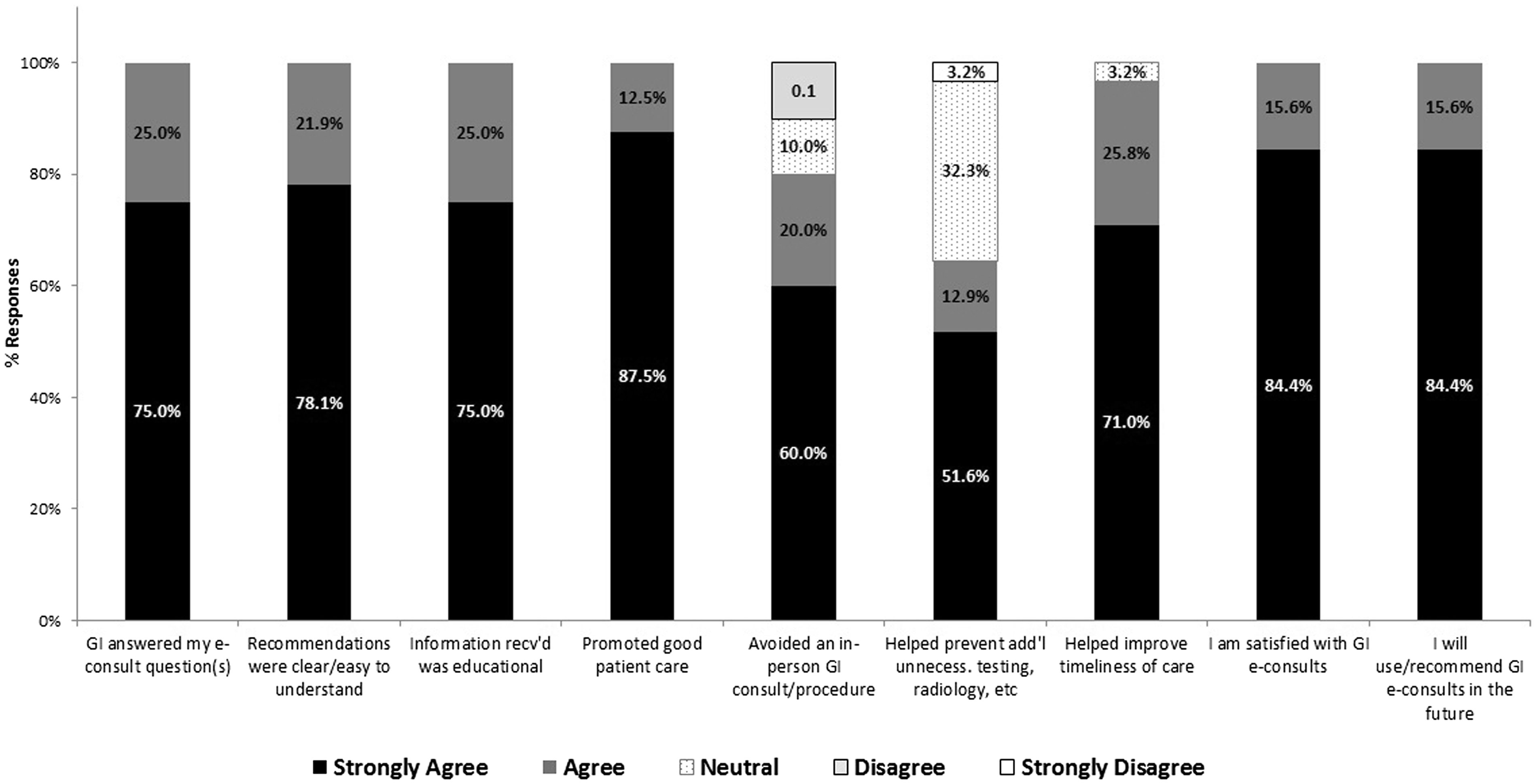
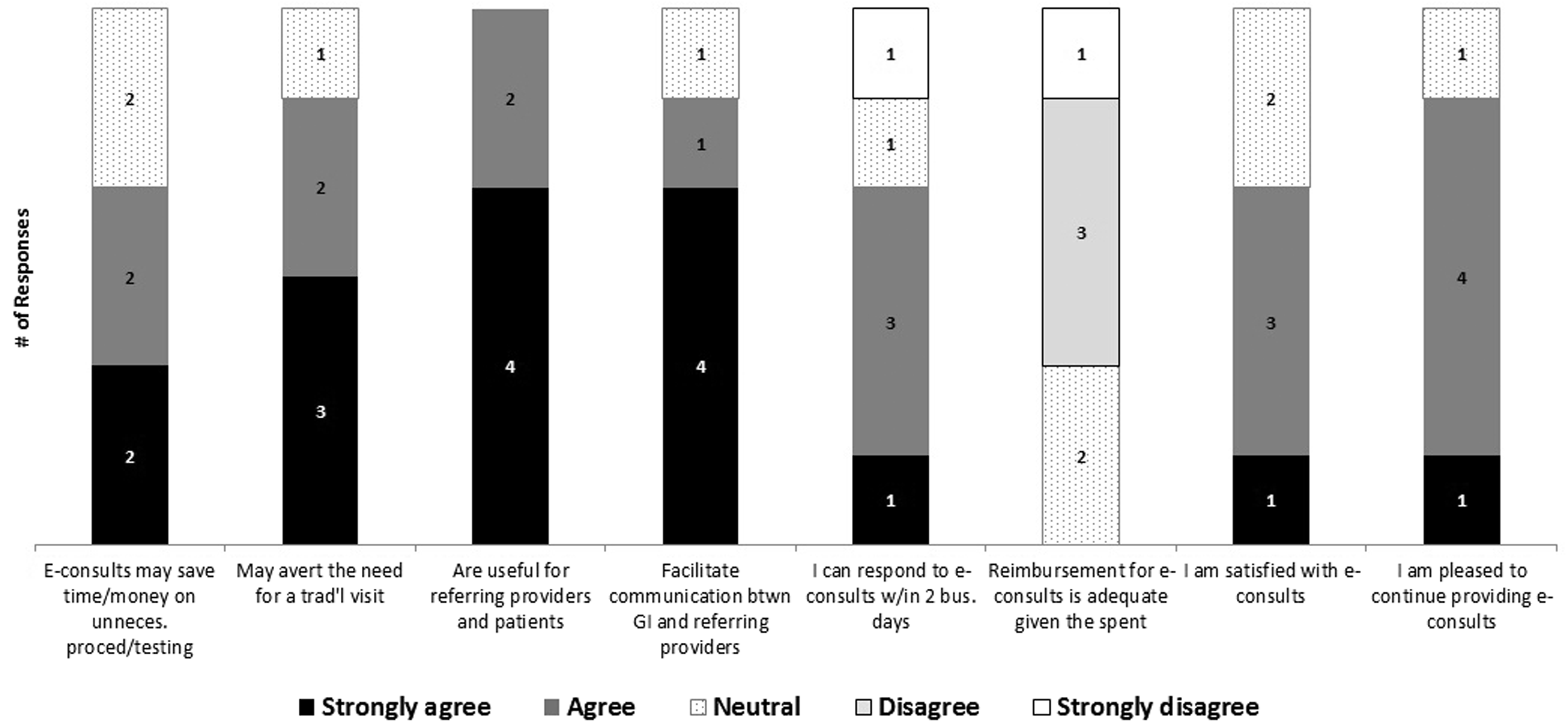
We received survey responses from all six GI consultants in our program, who agreed that e-consults were useful for referring providers and their patients (6/6 Strongly Agree or Agree), and 5/6 Strongly Agree or Agree that e-consults facilitate communication between GI and referring providers (Table 3). Five out of six GI consultants cited a busy workload as the main barrier to providing timely e-consults. While most of the GI consultants agreed they were pleased to continue participating in the e-consult program (5/6), none of the consultants agreed that the reimbursement for this activity was adequate given the time spent (reported as 15–30+ minutes per e-consult) (Figure 3).
Discussion
E-consults are emerging as a central tactic to both improve outpatient access to consultant expertise and to avoid unnecessary patient visits and procedures.16–18 In this study, we have demonstrated both satisfaction and feasibility of a GI e-consult program within a large ACO with a comprehensive integrated EHR. Our initial experience with GI e-consults demonstrated that many GI queries could be answered using this provider-to-provider mechanism, with GI providing expert guidance and recommendations as a safe and effective mechanism within a short timeframe. These new models for generalist–consultant information exchange have shown promise in some fields including rheumatology. Rheumatology eReferrals resulted in pre-consultation exchange of information between generalists and consultants that enabled management and resolution of the clinical question without ever requiring a traditional visit. 6 Our study demonstrated that 75% of GI e-consult requests did not require any further procedures or traditional visits. In addition, we demonstrated that primary care providers found e-consults to be educational, timely, and improved the patient’s quality of clinical care.
By utilising existing referral or clinical communication software tools, e-consult programs do not usually require much capital to implement. However, e-consults are not universally revenue generators, as payers are only beginning to embrace reimbursement for telemedicine, first focusing on patient-facing activities such as virtual or electronic visits. Currently, clinicians are often reimbursed internally; for example the Mayo Clinic provides salary support and visit credit for the provider’s role in e-consults.15,19 Our physician organisation provides a flat fee ($52 per e-consult) to participating consultants as reimbursement for their time. A similar study at our institution previously demonstrated that this fee is substantially lower than the cost of a new patient ambulatory visit; however the program is ideally designed for clinical questions that can be answered in a shorter amount of time (15 minutes or less) than a full new patient visit. 8 In addition, this service has the potential to save patients loss of work, copays and parking as they avoid traditional visits and potentially unnecessary testing.20–22
As EHRs continue to become more prevalent, telemedicine programs, such as e-consults, provide an opportunity for specialists to reach patients and providers outside of their local health systems through use of secure online portals, such as Epic’s Care Everywhere functionality. As demonstrated by the Extension for Community Health Outcomes (ECHO) program, telemedicine also has the potential to increase access to subspecialty services and consultation for patients and primary providers in rural and underserved areas, particularly for difficult-to-manage chronic diseases such as chronic hepatitis and inflammatory bowel diseases.22–24 The Mayo Clinic has also utilised telemedicine programs, including e-consults, to help expand its market share in specialty medicine nationally and internationally via their Affiliated Care Network. 24
Our GI providers felt that they generally spent more than 15 minutes per e-consult and that the current reimbursement was not adequate given the time they required. Despite a shared EHR, identifying the relevant information from accumulated notes and test results can be challenging as noted by other institutions. 25 However, previously un-reimbursed activities such as “curbside consults” can now be directed to the e-consult pathway for proper triage, documentation and physician reimbursement. 5 As administrative burden remains high for physicians, finding ways to reimburse for and incorporate non-traditional clinical and administrative activities remains important, and e-consults may provide a structured mechanism to do this. Programs such as e-consults also help triage of consult requests, by allowing more follow-up to be conducted electronically in stable patients, as well helping Primary Care Physicians manage lower-acuity patients longer, thereby freeing up consult blocks for new patients and patients with more complex needs.22,24 For practices that perform open access endoscopy, e-consult programs may also a provide a feedback method for referring providers to promote appropriate referral of costly endoscopic procedures.
Our findings should be interpreted in the setting of important limitations. First, as a study conducted within a single academic centre, it is difficult to extrapolate these findings to other populations and care settings. Second, we did not track these patients beyond 90 days to determine their health status, and if they eventually saw a gastroenterologist in the traditional face-to-face environment beyond three months. In addition, we could only capture information that occurred within our EHR and additional utilisation occurring outside of our ACO cannot be excluded. While program satisfaction among referring providers and consultants was high in the population surveyed, limitations include small sample size and low response rate from referring providers. We have demonstrated preliminary results of an e-consult program and expect that this can be expanded as broader adoption of e-consults in gastroenterology grows. We received e-consults from only about one third of our primary care providers and believe that there is an opportunity for growth as early adoption of the program becomes more ingrained in clinical practice. However, continued monitoring of volume and long-term clinical outcomes is essential in order to further validate the effectiveness of this strategy for providing gastroenterology care.
Conclusions
Programs such as e-consults are an important part of the patient-centred medical neighbourhood, improving multidisciplinary care coordination as an effective mechanism for primary care-specialty consultant communication.15,26 We have demonstrated that gastroenterology e-consults can be a safe and effective option for the delivery of gastroenterology outpatient care. For primary care providers, placing an e-consult is generally easy and convenient. 27 Both of our surveys demonstrated that providers appreciate e-consults as both an educational opportunity for referring providers and an innovative way to help improve provider communication, which can become fragmented in large institutions and health systems. 4
E-consult programs can also alleviate pressure on limited health system resources by improving access to specialty care at a relatively low cost. GI providers may also benefit from e-consults, as participation may reduce the burden of unnecessary visits for patients who can be managed by their primary provider, thereby increasing subspecialty access for other patients. As we look to expand such programs, specialty consultants need to participate in their design and evaluation to ensure that the expectations, resources and remuneration for these activities are aligned with overall objectives. The enhanced communication between primary care physicians and gastroenterologists will be especially valuable as the selection and timing of expensive diagnostic tests and pharmacological therapies come under greater scrutiny.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Wasfy was supported by a career development award from the National Institutes of Health through Harvard Catalyst (KL2 TR001100).