
Abstract
Introduction
Telepractice systems should be acceptable to users and meet end-user needs. Whilst the system requirements to conduct adult dysphagia assessments via telepractice are established, key differences exist between adult and paediatric swallowing assessments. This study was conducted to develop the system architecture required to conduct paediatric feeding assessments in patient homes via telepractice.
Methods
The study used a four-phase iterative design, informed by human-centred design principles. In Phase 1, two telepractice researchers and two paediatric feeding clinicians identified assessment tasks and explored potential system design solutions. Initial system testing was completed using clinical simulations (Phase 2). Live trials with 10 typically developing children were then conducted (Phase 3). Phase 4 involved user-centred feedback from clinicians and parents. Feedback from the development team, clinicians and parents was used to continuously refine the model.
Results
A combination of synchronous and asynchronous methods enabled all assessment components to be successfully completed. Clinician and parent feedback established the optimal technology (e.g. phone, tablet) and key camera positions necessary to optimise visual/auditory information for the online clinician. End-user feedback identified greater time efficiencies could be achieved through collecting some data (e.g. intra-oral pictures) via asynchronous methods prior to the session. Information sheets were deemed necessary to enhance the user experience. Clinicians and parents responded positively to the final system design.
Discussion
Modifications to standard videoconferencing were necessary to develop a clinically viable process for conducting paediatric feeding assessments in the home via telepractice. End-user feedback was integral to the design of the final model.
Introduction
The delivery of effective telepractice services requires systems designed to meet the needs of end-users. 1 Human-centred design principles aid the development of telepractice systems that are well-designed, user-friendly and acceptable to consumers.2,3 Within speech pathology, multiple examples of telepractice systems that incorporate additional add-ons and modifications necessary to meet assessment needs and enhance user experience have been reported, e.g. paediatric language/literacy assessments conducted via telepractice incorporate touch-screen technology to facilitate user interaction.4,5
Studies into the design and efficacy of synchronous telepractice models for the assessment of patients with swallowing disorders (dysphagia) has, to date, primarily focused on the adult population.6–14 Telepractice systems used for adult dysphagia assessments have undergone multiple testing iterations with a variety of patient groups to ensure that they meet the needs of users, tasks and environments. However, due to multiple differences between the assessment and treatment of adult versus paediatric swallowing disorders, transference of the adult telepractice assessment model to the paediatric population is limited.
Currently, there are few available studies describing the use of telepractice to provide paediatric feeding interventions,15–20 and only one known study has investigated the delivery of feeding assessments via telepractice, using an asynchronous assessment method. 21 Although the research team identified key technical factors that improved the reliability of their assessments (e.g. use of a trained assistant to position the camera), their research did not focus on user-acceptability or the design of systems. Previous research studies have recommended that further research is required to investigate how best to deliver synchronous feeding assessments via telepractice.16,21 Consequently, the aim of the current study was to develop and evaluate the system architecture required to conduct synchronous telepractice paediatric feeding assessments in patient homes.
Methods and results
A four-phase iterative process, integrating principles of human-centred design,2,3 was used to develop and evaluate the system (Figure 1). The study was conducted with ethical exemption from The University of Queensland.
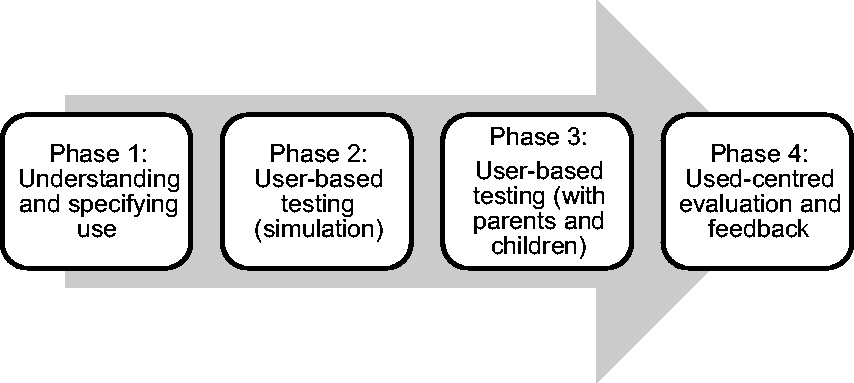
The four-phase iterative human-design process used to develop system architecture.
Phase 1: Understanding and specifying use
Phase 1 involved collaboration between four clinicians with diverse experiences (two experienced adult telepractice researchers; two experienced paediatric feeding clinicians). This design team identified the context of use, including identification of key users and stakeholders in the model, characteristics of users, goals and tasks required to be completed and the system environment. 2 It was identified that the audio-visual system needed to be sufficiently flexible to facilitate a range of tasks/observations including infant oral reflex examination, oral motor assessment, breastfeeding, bottle feeding, cup drinking and solid food trials, different seating/hold positions, infant/child posture/position for feeding, respiratory rate/colour change during feeding and parent–child interaction. As assessments were to be conducted in patient homes, it was identified that multiple forms of consumer-grade equipment (e.g. laptop, tablets) would need to be considered and trialled in planning. Specific consideration was given to the capacity of equipment to be positioned and re-positioned to capture the necessary visual/audio footage of the parent and child in specific situations (e.g. assessment of nipple attachment and suck-swallow-breath pattern during breastfeeding). Four main camera angles were proposed to enable capture of required visual information: a wide-angled front on view; a close-up front on view; a 45° camera angle; and a front-on long-shot. Specific assessment tasks, such as the infant oral reflex and non-nutritive suck assessment, are typically completed by a face-to-face clinician. 22 Consideration was given to how to complete these tasks in a telepractice environment, with modification so that the parent would complete these tasks under verbal instruction from the telepractice speech pathologist.
Phase 2: User-based testing (simulation)
Phase 2 involved multiple trials of the system in a range of simulated environments, with modifications made based on user feedback from the research team. Using infant mannequins, members of the team portrayed the online clinician and parent roles to undertake trials of all identified assessment tasks using a variety of devices (e.g. smart phone, laptop). Whilst these trials confirmed that the research team were able to achieve all assessment elements using any moveable device (e.g. laptop), a desktop computer was unsuitable for assessment needs due to difficulty repositioning the camera. Device cameras also needed to be positioned at a 45° angle from the child and feeder (Figure 2) as user testing identified that the child’s bottle or cup and/or the feeder’s hand obstructed clinician view if the camera was positioned front-on. A wearable breastfeeding simulator was utilised to conduct simulated breastfeeding trials. Feedback from trials with this device determined that a smart phone, due to its manoeuvrability, was the ideal device for this task. The phone, positioned approximately 10 cm above the mother’s shoulder, enabled visualisation of the mother’s breast and the infant’s mouth and detection of feeding sounds (Figure 3).
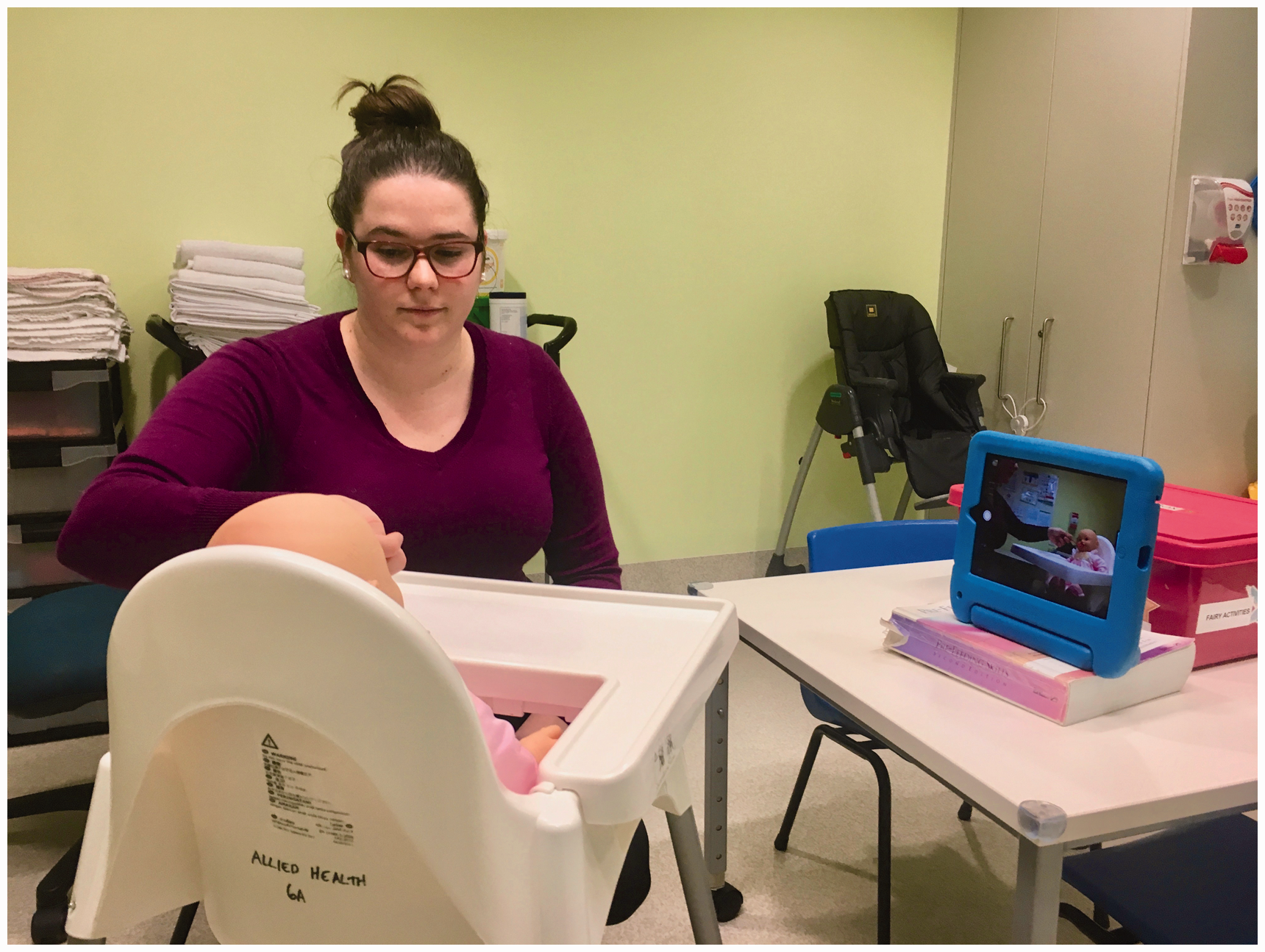
Simulation user-based testing enabling view of the parent and child to facilitate assessment of feeding and parent–child interaction.
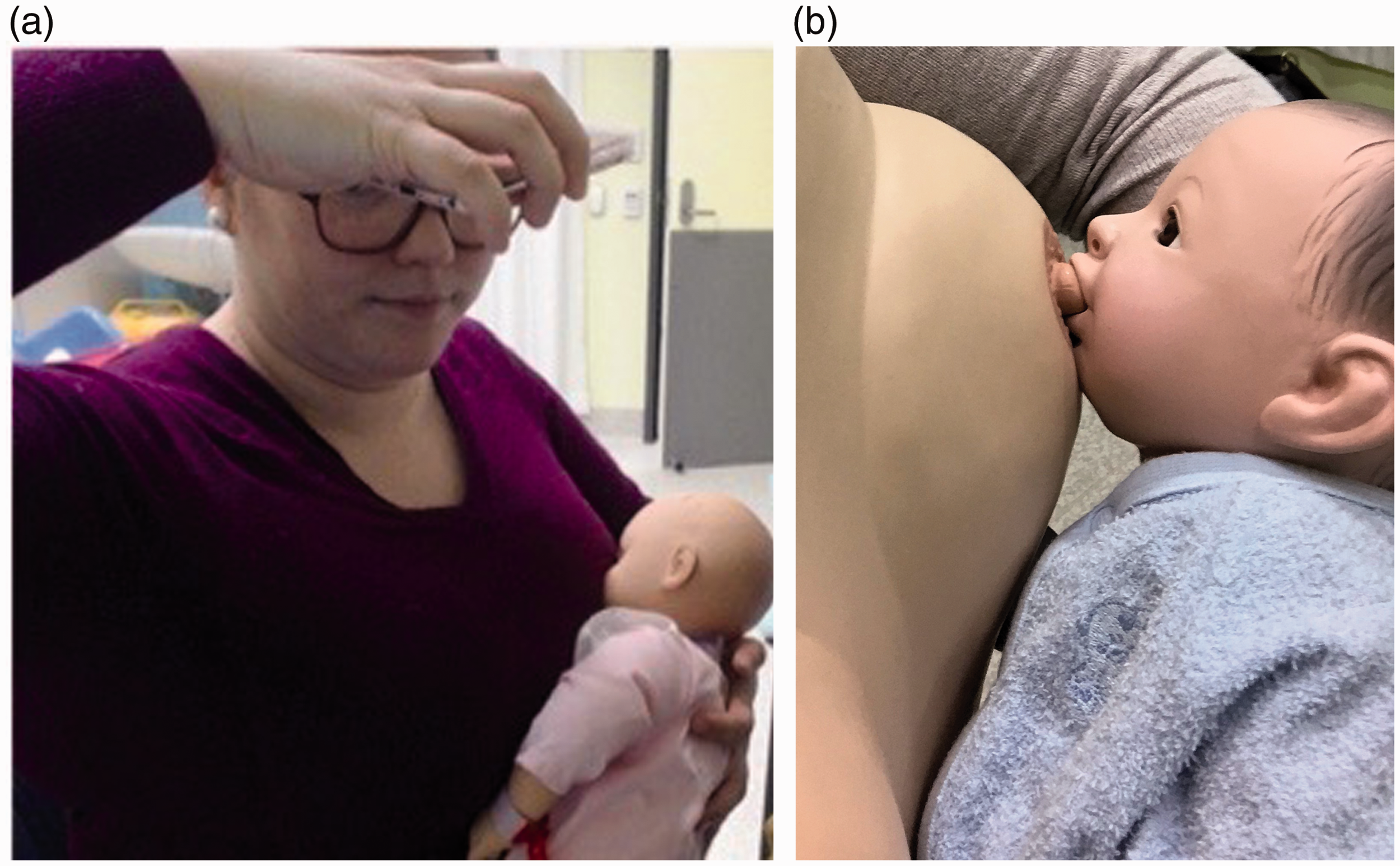
User-based testing with wearable breastfeeding simulator: (a) smart phone positioning above the mother's shoulder assisted and (b) visualisation of attachment and feeding/suckling.
In preparation for Phase 3, telepractice fact sheets were drafted to help improve user experience: one for breast/bottle-feeding infants and one for older children. These fact sheets were intended to improve the usability of the telepractice system for parents, including information regarding technical and set-up requirements (e.g. device video/audio capabilities, providing preferred toys and food/fluid); device connection; optimising lighting and sound; troubleshooting technical difficulties; and plan for medical emergency support (if required).
Phase 3: User-based testing (with parents and children)
Phase 3 involved user-based testing with ten typically developing children (aged 1 month to 6 years) and their mothers (n = 8). Synchronous telepractice feeding assessments were conducted in participant homes, led by an experienced paediatric speech pathologist located in a hospital facility. Participants utilised a variety of personal devices (Table 1), whilst the telepractice clinician used a desktop computer with a Logitech 1080p HD Pro webcam and Jabra SPEAK 410 MS speaker. Videoconferencing calls were made via a secure web-based platform provided by the health service (free to participants) with dual image layout and a bandwidth of >0.4 Mbps.
Phase 3 participant information.

Nine telepractice appointments were successfully conducted using the procedures confirmed from feedback during Phases 1 and 2 (Figure 4). One appointment could not be completed due to patient-end internet connectivity issues that were unable to be resolved. Of those assessments completed, all parents of infants successfully conducted the infant oral reflex and non-nutritive suck assessment following the online clinician’s instruction.

User-based testing with typically developing children enabling assessment of a) infant oral reflex exam, b) chewable solids and c) purees.
User feedback was used after each session to enhance the design. After the first two assessments it became clear that parents were taking a long time, and experiencing difficulty capturing images for assessment of positioning and the intra-oral examination during the appointment, with some images inadequate for clinical decision making. For subsequent appointments, modifications to the telepractice fact sheets included instructions for the parent on how to collect images of the child’s usual feeding position and oral cavity, to send to the telepractice clinician prior to an appointment.
Phase 4: Used-centred evaluation and feedback
Although feedback was sought from the research team, clinicians and parents throughout the design process, further verbal feedback was sought from all parents immediately following their telepractice appointment. Feedback from the research team identified that the final system design (incorporating both synchronous and asynchronous telepractice aspects) effectively met clinician need. It was reported that the designed telepractice system provided little disruption to clinical workflow, and that the use of asynchronous images was beneficial to improve the diagnostic accuracy of assessment tasks such as intra-oral examination due to reduced image quality during synchronous assessment.
All parents also provided positive feedback about their experience. They reported that the telepractice session was easy to complete and that they only occasionally experienced minor technical issues (e.g. initial connection difficulties, occasional audio drop-out). Parents liked that the clinician was available immediately via the phone to assist with troubleshooting. The parents also stated the fact sheet provided prior to the telepractice appointment assisted them in preparing for the assessment and setting up the equipment. The simple instructions and visual examples provided on the fact sheets assisted their preparation for the session, particularly planning positioning of their child at home in relation to the device camera to optimise image quality.
Most parents of infants reported that the telepractice clinician’s verbal instruction and modelling of the infant oral reflex exam was sufficient for them to complete the required tasks. One parent identified that providing access to video examples of these reflexes being elicited may have also been beneficial for her to complete the assessment tasks. During breastfeeding assessments, two mothers reported that they were able to hold the camera independently, and two others had their partner hold the camera. All participants agreed that having someone else to hold the camera was, or would have been, beneficial for their appointment, and would be crucial for mothers of children with breastfeeding difficulties. Mother’s reported that they would not have been able to manage any attachment/re-attachment difficulties whilst holding the camera themselves. One mother who trialled using a tablet device for the breastfeeding assessment reported this was difficult to hold and position.
Recommendations
On the basis of information gathered in all four phases, final equipment and system positioning recommendations were established (Table 2).
Assessment components and camera angles/modifications identified through human-centred design approach.

Discussion
An efficient telepractice system needs to be appropriately designed, integrating feedback from users and testing in ‘real world’ scenarios.2,3 The four-phase iterative human-centred design process utilised in this research study engaged both clinicians and parents to help design and develop a viable telepractice system. Through this process, it was identified that the integration of both synchronous and asynchronous assessment elements was required to optimise the feeding evaluation. The need for both telepractice methods was identified through a combination of user feedback regarding usability and clinician identification of required diagnostic image quality. The combination of these telepractice elements is not uncommon in speech pathology,6,14,23,24 with store-and-forward typically used when high quality diagnostic images are required.25,26
User-based testing also revealed that the patient-end device needed to be flexible and easily moveable. This is similar to previous research highlighting that paediatric telepractice platforms should be as flexible as possible to enable assessment in a variety of environments.25,26 Trials identified that some components of the feeding assessment (i.e. assessment of breastfeeding) required specific technology (smart phone) to improve assessment feasibility. This was highlighted further during the breastfeeding assessments, with mothers reporting difficulty completing breastfeeding assessments with larger devices. Such smaller devices are more often available within a family home; therefore their suitability was considered a positive outcome for the future uptake of this telepractice model. Clark et al. reported that the majority of families accessing their telepractice-enhanced paediatric feeding service used tablets or smart phones to link into consultations. 17
Finally, parents reported that the provision of information prior to the appointment was useful to prepare for the practical and technological expectations of the assessment. Session-specific factsheets ensured that parents had all necessary equipment ready for the appointment (e.g. toys, food) and were familiar with key camera positions. Then during the assessment, when the telepractice clinician required the parent to move to a different camera angle or position, they could refer directly to images on the fact sheet. Previous research by Bloomfield et al. reported the provision of information when enrolling parents in feeding intervention via telepractice. 18 Malandraki et al. also reported sending an email the day prior to their telepractice sessions to inform the parent what materials they needed to prepare. 16 They hypothesised that involving the family in the preparation of appointment materials and intervention tasks improved task saliency, specificity and generalization due to the natural intervention environment and incidental parent training.
In conclusion, the current iterative study design enabled development of a telepractice system that was acceptable to users and enabled completion of typical paediatric feeding assessments within the home. This has laid the foundation for the stages of further research to be conducted by this team, which will involve systematically investigating the reliability of this new model of care and both parent and clinician perceptions of the model when integrated into clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Children’s Hospital Foundation (grant number 50235).