
Abstract
This mixed methods study examined the phenomenon of nonsuicidal self-injury (NSSI) of adolescents in Singapore. The researchers analyzed quantitative data to understand the functions of NSSI, the relationship of parental invalidation to NSSI, and the association between academic stress and parental invalidation. In addition, the researchers employed semi-structured qualitative interviews to provide supportive qualitative data. The participants were outpatients at the Child Guidance Clinic, Singapore, between the ages of 13 to 19 years old. Researchers compared 30 participants who engage in NSSI with 30 participants who do not engage in NSSI. The emotional regulation function was the most commonly endorsed function for NSSI. Adolescents who engage in NSSI have statistically significant (p < .01) higher mean parental invalidation scores than those who do not engage in NSSI. There is also a moderate, positive correlation between the level of parental invalidation and the level of academic stress for Singaporean adolescents. The researchers discuss the implications of this study for mental health professionals.
Nonsuicidal self-injury (NSSI) is an increasingly important public health issue (Conterio & Lader, 1998; Klonsky, Oltmanns, & Turkheimer, 2003; Nock & Prinstein, 2004). Adolescents appear to be particularly at risk for NSSI. Studies of adolescents in the community have suggested rates between 14–15% (Ross & Heath, 2002) to a high of 39% of adolescents who reported self-mutilating within the previous 12 months (Lloyd, 1997). The prevalence of NSSI among adolescents in psychiatric inpatient settings is an alarming 82.4% (Nock & Prinstein, 2004). While these findings are based on the adolescent population in the United States, a review of literature on NSSI in other countries, including New Zealand (Conner, Langley, Tomaszewski, & Conwell, 2003) and Scandinavia (Lundh, Karim, & Quilish, 2007), suggests that NSSI is a growing worldwide problem. This problem extends even to Singapore, where clinical observations suggest an increase in the incidences of adolescent NSSI. An examination of the mental health statistics in Singapore (Lee, Fung, Teo, Chan, & Cai, 2003) and the current stressors facing the adolescent population (Ho & Yip, 2003) further suggest the potential pervasiveness of NSSI among Singaporean adolescents.
Nonsuicidal self-injury is defined as “purposely inflicting injury that results in immediate tissue damage, done without suicidal intent, and not socially sanctioned within one’s culture, nor for display” (Nixon & Heath, 2009, p. 4). NSSI is dangerous not only because of the physical damage that can be inflicted but because it can result in unintentional death (Kehrberg, 1997). Moreover, NSSI affects interpersonal relationships as well as the therapeutic relationship. NSSI often interferes with therapy (Favazza, 1989), and clients who self-injure often provoke strong negative responses from treatment professionals (Linehan, 1993; McDonald, O’Brien, & Jackson, 2007). The impact of NSSI upon both the individual and the therapist underscores the importance of understanding NSSI in order to increase the effectiveness of intervention and prevention programs.
Research has yet to examine NSSI in Singapore. Fundamental knowledge regarding NSSI in this population, such as prevalence rates, risk factors, and functions of NSSI, is presently unknown. Yet mental health professionals in the West, especially in the United States, have been concerned with the phenomenon of NSSI for decades and have conducted a great deal of research on NSSI. Amongst the areas studied are the relationship between various psychological correlates and NSSI. Psychological correlates studied include dissociation (Saxe, Chawla, & van der Kolk, 2002), alexithymia (Paivio & McCulloch, 2004; Zlotnick et al., 1996) as well as anger, aggressiveness, loneliness, emotional reactivity, and hopelessness (Darche, 1990; Guertin, Lloyd-Richardson, Spirito, Donaldson, & Boergers, 2001). Research also focused on the relationship between suicidal behavior and NSSI (Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006) and even the role of the internet in NSSI behavior (Whitlock, Powers & Eckenrode, 2006). Since an understanding of both the functions and the risk factors of NSSI is important for effective treatment and prevention (Gratz, 2003), this preliminary study of NSSI in Singapore had a dual focus.
In an exhaustive meta-analysis, Klonsky (2007) identified seven possible functions of NSSI: affect regulation; antidissociation; antisuicide; interpersonal boundaries; interpersonal influence; self-punishment; and sensation seeking. Although NSSI can serve other functions, research across samples consistently point to emotional regulation as the primary function. However, whether the primary function of NSSI is similar for Singaporean adolescents is not known. The first question the researchers of this study attempted to answer was, “What is the function of NSSI in the adolescent population in Singapore?”
An understanding of functions of NSSI will enable clinicians to tailor their interventions, and knowledge of risk factors will aid in the identification of adolescents who are at increased risk of NSSI. The literature indicates that the most extensively studied risk factors for NSSI involve childhood trauma, and includes physical and sexual abuse (Gratz, Conrad, & Roemer, 2002; van der Kolk, Perry, & Herman, 1991; Zlotnick et al., 1996), neglect, (van der Kolk et al., 1991), and separation and loss (Carroll, Schaffer, Spensley, & Abramowitz, 1980; Gratz et al., 2002). However, a significant limitation of these studies on trauma is the way different forms of childhood abuse have been “compartmentalized” (Briere & Runtz, 1990, as cited in Mountford, Corstorphine, Tomlinson, & Waller, 2007). This compartmentalization results in limited awareness of how different forms of abuse may interact with each other and overlooks other forms of passive abuse such as parental indifference to the child’s emotional needs (Rorty, Yager, & Rossotto, 1994). Furthermore, it should be noted that, increasingly, many adolescents who engage in NSSI reported no history of physical or sexual abuse (Walsh, 2006).
In their review of risk factors for NSSI, Gratz et al. (2002) noted that, even for individuals without a history of childhood abuse, factors of neglect, separation, or the quality of the attachment relationship with parents may contribute to the development of NSSI. Gratz et al. found that insecure paternal attachment was a significant predictor for NSSI behavior among female college students. Linehan (1993) suggested the possibility of environmental factors (i.e., an invalidating environment interacting with an individual’s vulnerability), contributing to emotional dysregulation, which may culminate in NSSI as a coping strategy. According to Linehan, an invalidating environment is one in which emotions are not validated, and communication of emotions is “punished, and/or trivialized” (1993, p. 49). The invalidating environment contributes to problems with emotional regulation by failing to teach the child how to label and moderate feelings, tolerate distress, or trust his or her emotional responses as legitimate interpretations of events (Linehan, 1993). In addition, such restrictive environments tend to reinforce only the extreme affective responses. This view finds support in the work of Fruzzetti, Shenk and Hoffman (2005) who suggest that parental behaviors transact with the child’s own behavior resulting in chronic and pervasive emotional dysregulation and the possible development of self invalidating behavior such as NSSI.
In their study of eating disorders, Mountford et al. (2007) focused on the role of passive abuse and utilized the concept of the invalidating environment (Linehan, 1993) as a way to understand the development of eating disorders. They found a relationship between the degree of invalidation and level of eating pathology, and an association between an invalidating environment and difficulties in distress tolerance (Mountford et al., 2007). The researchers in this study proposed that it may similarly be possible to account for NSSI amongst adolescents who do not report any history of overt abuse with the concept of an invalidating environment (Linehan, 1993). Therefore the second question this study explored was whether there was a difference in the degree of parental invalidation among Singapore adolescents who engaged in NSSI when compared to those who did not engage in NSSI.
There is little empirical research regarding the psychological construct of an invalidating environment or the factors that may contribute to an invalidating environment. However, in their extensive and nuanced discussion of invalidation, Fruzzetti et al. (2005) postulated a transactional model to understand the role of individual differences and environmental factors in the development of borderline personality disorder. This seems to be in line with the literature which suggests possible environmental factors, such as school and work stress, and the psychological unavailability of parents as contributing to an invalidating environment (Linehan, 1993; Walsh, 2006). A study of the stressors experienced by adolescents in Singapore would suggest that expectations of parents and high self-expectations are sources of academic stress and a possible factor for NSSI in the Singapore adolescent population. Reports indicate that both parents and students often rate the Singapore school system as a highly stressful system. In a Singapore Press Holdings survey (Mathi, 2000), 33% of 1,742 children aged 10 to 12 reported having thoughts that life is not worth living. Further, about 50% of these young people cited failing an examination and not scoring high marks as their greatest fear. Interestingly, youth rated a parent or guardian dying as their second greatest fear. This is significant because similar surveys conducted in other countries tend to show that the number one fear of a similar population is that of parents or guardians dying (Mathi, 2000). Similarly, in a National Youth Survey conducted in Singapore, 56% of the respondents chose “studies” as the top stressor in their lives (Ho & Yip, 2003). Another study found that 42.7% of parents cited their children’s education as their greatest worry (Quah, 1999). These statistics seem to support the reports of high levels of academic stress in Singapore.
At least two factors explain this heavy emphasis on academic achievement in Singapore. Socioeconomically, Singapore is a small city-state with no natural resources. Ever since Singapore gained its independence from Malaya in 1965, there has been a constant focus on the population as human capital and, through a system of meritocracy, those who do well academically are recognized and rewarded (Chen, 1983). A second factor is the Asian cultural context. This environment is collectivistic in nature, and there is great pressure to conform to expectations of both parents and the community (Yeh & Huang, 1996), especially in the area of education, which this population traditionally views as the way to get ahead in life (Shek & Chan, 1999). A third question this study attempted to answer, therefore, was “What is the relationship between parental invalidation and academic stress in the Singaporean adolescent population?”
Finally, while many researchers (e.g., Ross & Heath, 2002; Suyemoto, 1998) have concluded, based on research and clinical observations, that NSSI is more common among women than men, there are also studies that suggest the possibility that the rate of NSSI may be fairly similar in women and men (Gratz et al., 2002; Heath et al., 2009). However, these findings are all based on Western populations; hence this study also attempts to examine the relative predictive value of parental invalidation, academic stress, and gender for NSSI in the Singaporean adolescent population.
Hypotheses
The purpose of this study was to examine NSSI in the Singapore adolescent population in terms of the functions and risk factors associated with NSSI for this population. Specifically, the researchers hypothesized that emotional regulation would be the most commonly endorsed function of NSSI and those adolescents who engage in NSSI would experience a higher degree of parental invalidation when compared to those who do not engage in NSSI. The researchers further hypothesized that there would be a significant correlation between parental invalidation and academic stress. Finally, the researchers predicted that a combination of parental invalidation and gender are the factors that best predict NSSI in the Singaporean adolescent.
Method
Population
This study was conducted at the Child Guidance Clinic (CGC), Singapore, and involved the use of two samples: one sample of 30 identified adolescent outpatients who engage in NSSI (i.e., the NSSI group) and a second sample of 30 adolescent outpatients who do not engage in NSSI (i.e., the control group). Participants for the NSSI group met the following criteria: (a) was an outpatient at CGC; (b) was between 13 and 19 years of age; and (c) had engaged in NSSI in the past year. Participants for the control group comprised a group of adolescents who: (a) were outpatients at CGC; (b) were between 13 and 19 years of age; and (c) had never engaged in NSSI. In addition, as part of the concurrent embedded strategy, six participants were interviewed in depth for a more complete understanding of NSSI in the adolescent population in Singapore. Participants for the NSSI group were classified by the attending psychiatrist as having engaged in NSSI. Outpatients with mental retardation, psychosis, bipolar disorder, and illicit drug use were excluded.
The participants’ ages ranged from 13 to 19 years. The study group had a mean age of 16.30 (SD = 1.70) and the control group had a mean age of 15.97 (SD = 1.69). An attempt was made to achieve equivalence in the study and control group in terms of gender with each group having 12 male and 18 female participants.
The proportion of Chinese (83.3%), Malays (8.3%), Indians (5.0%), and others (3.2%) in the sample roughly corresponds to the national demographics of these ethnic groups in terms of their relative proportions (74.2% Chinese, 13.4% Malays, 9.2% Indians, and 3.2% others; Singapore Department of Statistics, 2009), with a slight overrepresentation of Chinese subjects. In terms of participants’ educational levels, the largest frequencies were reported for secondary level (78.3%) and junior college level (13.3%). Please see Table 1 for a comparison of family status and parental educational levels.
Frequency distribution for the sample by group (N = 60).

Population size
For this study, an application of power analysis is used to estimate an appropriate sample size. This application is based on the alpha level chosen, the desired level of power and the population effect size (Polit, 1996). The alpha level will be .05 for analyses in this study and the desired power level is .80. It is impossible to accurately gauge the population effect size since the literature is sparse concerning NSSI in Singapore. Cohen (1977), however, has created some benchmarks to qualitatively describe the absolute value of effect sizes when the effect size cannot be estimated from the literature. For t-tests, he designated an effect size of .20 as small, .50 is considered medium, and .80 is large. Based on the literature review with other populations, it is hypothesized that there will be a large mean difference between the scores of adolescents with and without NSSI, resulting in a large effect size. According to Cohen’s tables, for alpha = 0.05, power = 0.80, and effect size = 0.80, an appropriate sample size for each group should be 25 individuals. This study will use a sample size of 30 per group, in case the effect size is lower than expected.
Procedure
Researchers obtained approval for this study from the Institutional Review Board of Regent University, the Clinical Review Committee of the Institute of Mental Health, and the Domain Specific Review Board of the National Healthcare Group, Singapore. In the initial exploratory phase, researchers used a mixed method design with a concurrent embedded strategy. The researchers also used secondary qualitative data to help ascertain the validity of the quantitative data by understanding the adolescents’ personal views and possible cultural nuances. The qualitative information was useful in clarifying statistical differences and relationships between groups as well as explaining unexpected findings with participants’ subjective accounts (Creswell, 2002).
To obtain a noncoerced consent from the subject, the consent of the parent and the adolescent were done separately. Parents and subjects were also informed that information obtained from the study would not be shared with parents except in cases where there was imminent threat to self or others, or reports of neglect or abuse. In such cases, subjects’ parents and attending doctors would be informed
The researchers administered the Functional Assessment of Self-Mutilation (FASM; Lloyd, Kelley, & Hope, 1997) to only the NSSI group; however, two other measures, the Invalidating Childhood Environment Scale (ICES; Mountford et al., 2007) and the Academic Expectations Stress Inventory (AESI; Ang & Huan, 2006) were administered to both the NSSI group and the control group. Additionally, all participants completed a demographic questionnaire (DQ). As part of the concurrent embedded strategy, researchers conducted an in-depth semi-structured interview with six participants from the NSSI group to obtain a more complete understanding of NSSI in the adolescent population in Singapore. This semi-structured, qualitative interview allowed participants to discuss and clarify their experiences with NSSI, their family, and academic stress. The principal investigator transcribed verbatim the archived interviews, and then assessed the interviews using the consensual qualitative research (CQR) method (Hill et al., 2005; Hill, Thompson, & Williams, 1997).
Measuring instruments
Demographic questionnaire (DQ)
The researchers used the DQ to collect information pertaining to the respondent’s demographic background (i.e., age, gender, and race) as well as information relating to their educational accomplishments and the educational accomplishments of their parents.
Functional Assessment of Self Mutilation (FASM)
The FASM is a self-report instrument that measures the methods, frequency, and functions of NSSI (Lloyd et al., 1997). Eleven items assess the frequency and different methods of self-injurious behavior (e.g., hair pulling, cutting, burning or scraping of the skin, and biting/hitting oneself) engaged in during the previous 12 months. Twenty-two items assess the functions or reasons for engaging in NSSI, rating each reason on a scale from 0 to 3 (0 = never, 1= rarely, 2 = some, and 3 = often).
The psychometric properties of the FASM are supported through its use in studies of NSSI in both nonpsychiatric (Hilt, Cha, & Nolen-Hoeksema, 2008; Lloyd et al., 1997) and psychiatric populations (Guertin et al., 2001; Nock et al., 2006; Nock & Prinstein, 2004, 2005). Adequate levels of internal consistency have been reported for the FASM for both moderate and severe forms of NSSI (r = .65–.66), and concurrent validity of the FASM is evidenced by significant associations with measures of suicidal ideation (Guertin et al., 2001).
Nock and Prinstein (2004) evaluated the structural validity of the four-function model of NSSI through various data-analytic procedures. Reliability analysis showed moderate to high internal consistency for the four-function model, with resulting alpha co-efficients of .62 for automatic-negative reinforcement (A-NR) function, .69 for automatic-positive reinforcement (A-PR) function, .76 for social-negative reinforcement (S-NR) function, and .85 for social-positive reinforcement (S-PR) function (Nock & Prinstein, 2004). The four subscales were significantly correlated, with correlations ranging from .34 (between A-NR and S-PR) to .78 (between S-NR and S-PR; Nock & Prinstein, 2004). According to Nock and Prinstein, the magnitude of the reported zero-order correlations (rs = .39–.78) shows that, while the four functions were significantly related, they nevertheless represent distinct constructs.
Invalidating Childhood Environment Scale (ICES)
The ICES is a self-report instrument designed to measure parental invalidation (Linehan, 1993). The ICES consists of 18 items; 14 items assess specific parental (paternal and maternal) behaviors. Four final items describe the three types of invalidating environments proposed by Linehan (1993) and one description of a validating environment. For each of the 14 items that assess parental behaviors, participants rate paternal and maternal behaviors on a Likert-type scale (1 = never to 5 = all the time). The mean score for the 14 items measures the perceived levels of invalidation for each parent, with higher scores reflecting a greater perceived level of invalidation. This results in two subscores for paternal invalidation and maternal invalidation.
In a study to validate the ICES, Mountford et al. (2007), found that the ICES demonstrated good levels of internal consistency, with resulting alpha coefficients of .80 for paternal invalidation and .77 for maternal invalidation. Data on convergent validity was also reported with the strongest correlations between maladaptive distress tolerance as measured by the Distress Tolerance Scale (Costorphine, Mountford, Tomlinson, Waller, & Meyer, 2005 as cited in Mountford et al., 2007) and maternal invalidation (r = .42, p < .01).
Academic Expectations Stress Inventory (AESI)
The AESI is a nine-item inventory that measures academic stress arising from expectations of parents/teachers and self-expectations (Ang & Huan, 2006). The AESI consists of two factors; the first factor consists of five items and constitutes the expectations of parents/teachers subscale, and the second factor consists of four items and constitutes the expectations of self subscale (Ang & Huan, 2006). The AESI shows strong psychometric properties. Internal consistency was high with scores from the nine-item AESI yielding a Cronbach’s alpha of .89. The resulting Cronbach’s alpha for the parents/teachers subscale was .85 and the expectations of self subscale was .84. The two-week test–retest reliability coefficients were .85, .79, and .77 for the scores on the nine-item AESI, the expectations of parent/teachers, and expectations of self subscales, respectively. Initial evidence of convergent and discriminant validity were also reported (Ang & Huan, 2006).
Results
Descriptive analysis of the participants’ FASM data reported that the most frequently used methods of NSSI for Singaporean adolescents were hitting self (70%), cutting/carving skin (66.7%), and biting self (56.7%). A large majority (90%) of the NSSI group participants engaged in more than one type of NSSI. The average frequency of NSSI was 14.44 times over a 12-month period, with number of times indicated for a specific NSSI behavior ranging from zero to 365. Over a 12-month period, cutting oneself was the NSSI behavior that had the highest frequency of occurrence (M = 39.80, SD = 82.24), followed closely by biting self (M = 38.63, SD = 97.27). Participants (93.3%) who engaged in NSSI showed little planning or forethought before engaging in self-injury. Most subjects (36.7%) reported little pain while others (26.7%) reported no pain when engaging in NSSI. The majority of subjects (83.3%) also did not use alcohol/drugs before engaging in NSSI. Subjects who engaged in NSSI tended to begin engaging in the behavior from early adolescence with mean age of onset at 13.01 (SD = 2.49).
Emotional regulation was the most commonly endorsed function of NSSI amongst Singaporean adolescents. Following previous research using the FASM where the subscale item means were used to measure each function (Nock & Prinstein, 2005), this study found that the A-NR function was the most commonly endorsed function (M = 2.18, SD = 1.18), followed by the A-PR function (M = 1.93, SD = 1.23). In contrast, the social reinforcement functions were relatively less endorsed (M = .78, SD = 1.06) for the S-NR function (M = .79, SD = 1.00) and for S-PR function.
The percentage endorsement for each individual reason given for engaging in NSSI supports data indicating that Singaporean adolescents are more likely to engage in NSSI to regulate their emotions than for influencing others. Between 73.3% and 86.7% of participants who engage in NSSI endorsed the A-NR function (to reduce bad feelings) and the A-PR function (to produce good feelings). In contrast, less than 50% of the participants endorsed social reinforcement reasons (both positive and negative) for engaging in NSSI.
The second research question explored whether there would be a difference in the degree of parental invalidation among Singapore adolescents who engage in NSSI as opposed to those who do not engage in NSSI. The researchers conducted two t-tests for independent samples to test for significant differences between adolescents who do and do not engage in NSSI with regard to their mean ICES score, one for mothers and one for fathers. It should be noted that, prior to running these analyses, the group variances were tested for homogeneity (Levene’s test), and the variances were found to be similar.
The differences between the NSSI group and control group were found to be significant for mother ICES scores, t(56) = 5.59, p < .01. Father ICES scores were also significantly different between NSSI and control, t(56) = 5.31, p < .01. Therefore the degree of parent invalidation, as measured by the mother and father ICES scores, differed significantly for Singaporean adolescents who do and do not engage in NSSI. Specifically, adolescents who do engage in NSSI have higher mean parent invalidation scores than their counterparts who do not engage in NSSI. In the case of maternal invalidation, M = 2.63 for NSSI participants and M = 1.85 for control participants. In the case of paternal invalidation, M = 2.46 for NSSI participants and M = 1.77 for control participants.
For the third research question about the relationship between parental invalidation and academic stress in the Singaporean adolescent population, the researchers utilized two Pearson product moment coefficients of correlation to assess the relationships between the total AESI scores and the mother and father ICES scores. This resulted in two significant findings. The correlation between the mother ICES and the AESI scores was r = .35, p < .01. Similarly, r = .36, p < .01 for the correlation between the father ICES scores and the AESI scores. Thus the results indicate that there is a moderate, positive relationship between the level of parental invalidation and the level of academic stress for Singaporean adolescents.
The final research question explored the relationship among gender, level of academic stress and degree of parental invalidation as predictors to whether adolescents will engage in NSSI. A discriminant function analysis was conducted to determine whether four variables – gender, father invalidation, mother invalidation, and academic stress – could predict whether an adolescent will or will not engage in NSSI. According to Polit (1996), in terms of using discriminant function analysis, the homogeneity assumption is fairly robust when the overall sample is greater than 20 cases and groups are approximately equal in size. In this study, the groups are approximately equal in size with 28 subjects in the NSSI group and 30 subjects in the control group. Polit indicated that, if the primary goal of the analysis is classification, violation of the assumptions is less worrisome. Nonetheless, prior to running these analyses, researchers tested the group variances for homogeneity of variances for the AESI score and both ICES scores using Levene’s test. For gender, researchers ran an equality of group means. Analyses showed no significance, indicating no differences in group means or variances. Thus the assumptions of homogeneity of variance were met.
One function was generated and was significant, λ= .58, χ2 (4, N = 58) = 29.23, p < .01, indicating that the function of predictors significantly differentiated between adolescents who engage in NSSI and those who do not engage in NSSI. The canonical correlation was .65 and was highly significant (p < .01). In addition, the squared value indicated that the predictors explained approximately 42% of the variance in NSSI status. Standardized function coefficients and correlation coefficients (see Table 2) revealed that the variables of father ICES score, mother ICES score, and total AESI score were most associated with the function. This analysis included classifying all cases into groups.
Standardized function coefficients and correlation of predictor variables with the one discriminant function.

In addition, researchers used a jackknifing procedure to cross-validate and obtain a better estimate of the true classification rate. This involved omitting a case to develop the discriminant functions and then classifying the omitted case, and subsequently repeating the procedure for every case in the sample, producing a less-biased classification rate. The classification results were excellent. Original classification results revealed that 73.3% of the NSSI group was correctly classified, while 83.3% of the control group was correctly classified. For the overall sample, 78.3% were correctly classified. Cross-validation derived 70.0% accuracy for the total sample. The means of the discriminant functions are consistent with these results. NSSI participants had a function of .862, while control group participants had a mean of −.805. These results suggest that adolescents with high parental invalidation and academic stress are more likely to have engaged in NSSI. Gender is not a strong discriminator between groups.
Findings and analysis of qualitative data
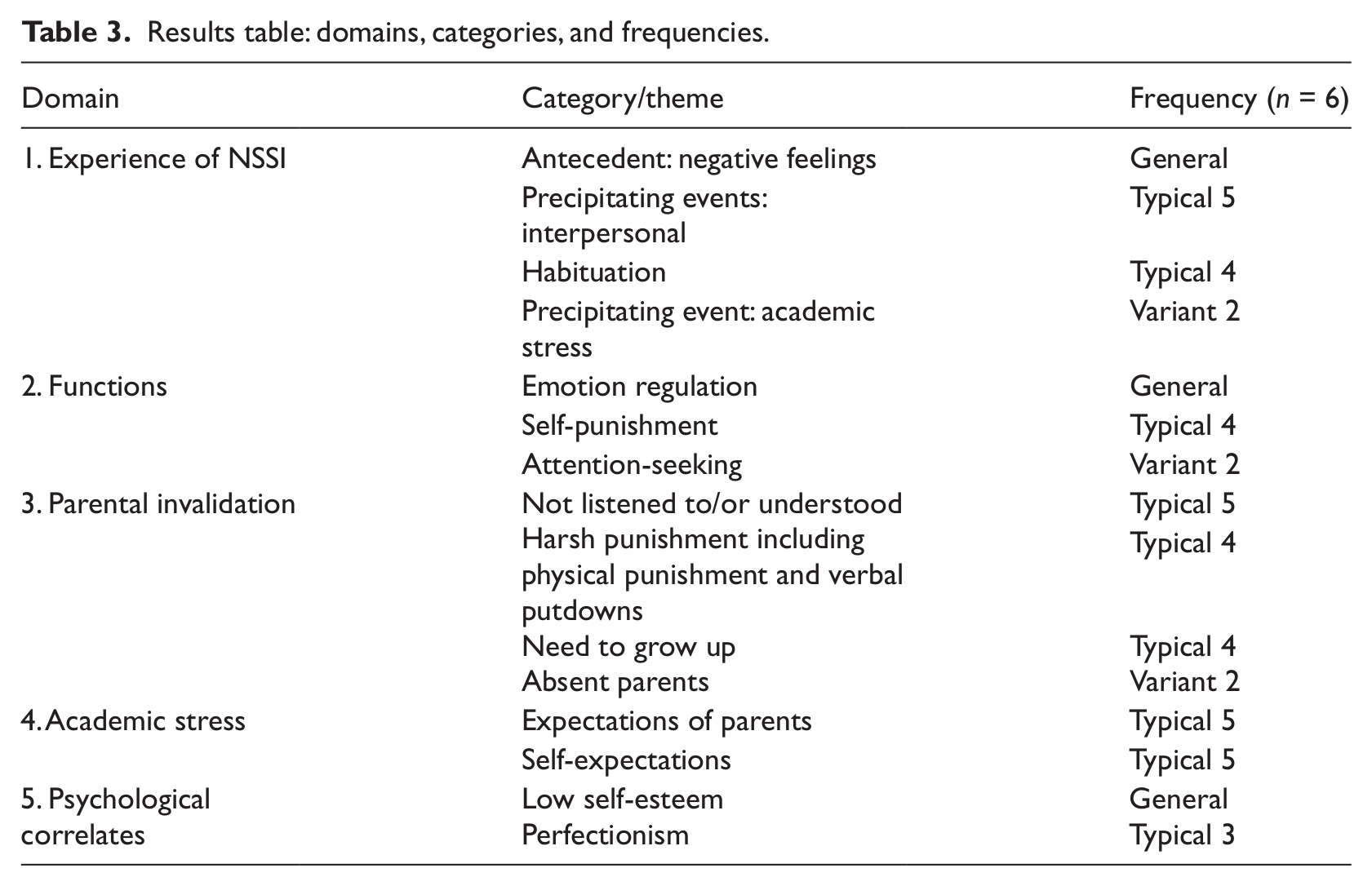
The researchers used a modified CQR method as a framework for the collection and analysis of the qualitative data. The principal investigator transcribed verbatim the archived interviews and the researchers then assessed the transcripts independently. The process began with the development of domains that identify broad topic areas, followed by the construction of core ideas that capture the main ideas in each domain. Finally, through cross-analysis, researchers compared core ideas for each domain across cases to determine the clustering of these core ideas into categories/themes (Hill et al., 1997, 2005). Throughout the process, the researchers engaged in extensive discussions to reach consensus. The researchers labeled the categories according to frequency of occurrence. The general category applies to all cases; a typical category includes at least half of the cases; and a variant category consists of a minimum of two cases (Hill et al., 1997, 2005). General and typical themes are useful in helping to interpret results; variant themes point the way for further study. The results of the analysis are presented in Table 3.
Results table: domains, categories, and frequencies.
The use of methods triangulation (with quantitative and qualitative components) and analyst triangulation (Patton, 1999) helps to establish the credibility and confirmability of the data (Lincoln & Guba, 1985). In general, the qualitative findings supported the findings from the quantitative component of the study and also provided further explication. Additional themes also surfaced which point the way to possible areas of future exploration.
Experience of NSSI
Generally, participants reported experiencing negative feelings before engaging in NSSI. Among the negative feelings reported were feelings of anger, sadness, numbness, confusion, and shame. Typically, such negative feelings were triggered by an interpersonal incident. However, a variant category that emerged had participants reporting NSSI incidents that were triggered primarily by academic stress. One subject emphatically summarized the relationship between academic stress and NSSI as “Studies cause stress, causes emotional tension, duress. A lot of stress equals really negative, pessimistic feelings, and for me there is no outlet like other people … so as a result I take it out on myself.”
It is interesting to note the emergence of another typical theme in the way participants who engaged in NSSI reported how they become habituated to the behavior. As a result, they not only increased the frequency and intensity of whatever method they were using to self-injure but also often switched to more destructive methods. As one subject put it:
I used to only at least like cut once, but then slowly over the years, because I have been cutting, so I will increase the number of cuts. Although it hurts, sometimes it really hurts, but the more I cut the more I am used to it. I am used to the pain, so I will cut a lot.
Or, as other participants reported, they either have to increase the number of cuts, “the deepness” of the cuts, or even “cut faster” to experience the same intensity of relief. The subject of habituation has not been extensively studied (see Selby, Connell, & Joiner, 2010) and suggests a possible area of future study.
Functions
One general category emerged where participants consistently reported the use of NSSI for the purpose of emotional regulation. The mechanism through which emotional regulation was achieved was suggested by some participants who reported that the act of NSSI helped to convert the emotional pain to a physical pain, which they often described as more manageable. In the words of one subject:
Most of the time when I feel upset, it’s mostly because I am upset with myself. I will punch myself, I will hit myself, to feel the pain. I actually think that … physical pain … will help lessen the pain in my heart.
Parental invalidation
Based on Linehan’s (1993) definition of an invalidating environment, parental invalidation describes a way of interaction between parents and children where the child’s feelings are not validated.
This sense that parents are not listening or attempting to understand was communicated by a participant who said, “I feel that parents don’t really understand us but they tend to have their own ways saying I am your parents so you should listen to me. Whatever we say we are right.”
Also participants typically reported the insistent message to act grown up. This reflects one of the three invalidating environments described by Linehan (1993), the typical family, where there is an emphasis on the control of one’s emotions as well as a focus on achievement and success. In the typical family, the central theme is to “behave like a grown up.” As reported by one subject, “and somehow I didn’t have the opportunity to actually be a kid. I had to be mature.”
A variant category that emerged and which has not been extensively studied is that of absent parents. One participant who had lived with her grandmother and aunt since she was 1 said:
So, the first time I self-injure is at the age of 10, because I feel that no one can help me, no one can listen to me … Sometimes I think if I can live with my parents and they listen to me, then I won’t be like this.
This variant category is consistent with the findings of Zanarini et al. (1997), who reported that 92% of a sample of borderline patients reported parental neglect and emotional denial.
Academic stress
Typically two categories emerged: expectations of parents and self-expectations. In terms of parental expectations, one participant stated, “since a young age my parents have been pushing me to be the best in something.”
Typically self-expectations in terms of academic achievement were stated as, “I have quite high expectations of myself.” The participants would also frequently deny that there was any pressure from parents. However, one participant’s account suggested a possible link between parental expectations and self-expectations. When she was asked where her high self-expectations originated from, she replied:
I think it is when I was young, my parents always do my homework with me in kindergarten … it’s probably from there I guess, because every time I get full marks they will praise me and I really love it.
That approval is somehow tied to participants doing well in exams was stated by another participant, “You must keep up your performance, the moment you don’t they won’t care for you. They will forever, not approve of you.” Another participant similarly suggested that parental pressure can sometimes be experienced in subtle ways. She said:
My parents are pretty supportive when it comes to my studies. They say you just do your best and things like that but rather than them being angry I look at their faces and their faces show more disappointment rather than being angry. It tugs on my heart strings more rather than getting angry.
Psychological correlates
One general category emerged where participants consistently reported having a low sense of self-esteem. Much of this low sense of self-esteem appears related to academic performance. One participant stated, “I would hate myself … I would compare myself to my brothers and sister. Your brother is a teacher, your sister is in uni, and what are you? You are a dropout.” There appeared to be a degree of stigmatization and consequent impact on their sense of self-esteem when participants did not perform well in school and ended up in less prestigious “neighborhood schools.” This was expressed by one participant in the following manner:
Because my school isn’t a really good school, it’s like a neighborhood school … people will judge you by the uniform. My school, the standards are not really that high so, sometimes they treat us as if we really have no IQ, which is really horrible.
Moreover, typically the category of perfectionism was noted. One participant stated, “Everything comes crashing down on you because you don’t get top of the level.” A second participant reported an incessant quest to do even better when she said:
For school, last year only I was top of my class … I thought that since I have done it once, I have to do it again, I have to do it better, as in, for the previous time I top my cohort with five subjects, this time I must top it with all my subjects … I feel like I cannot even let my percentage fall.
Discussion
Function of NSSI
One of the most common myths regarding NSSI is that individuals engage in self-injury to “get attention” (Caicedo & Whitlock, 2009). While some individuals may use NSSI as a way to get attention, the quantitative findings of this study indicate that only a minority (46.7%) of subjects endorsed this as a reason, and this was further verified through qualitative analysis. This did emerge as a variant theme during two interviews, where participants described how they resorted to NSSI as a way to get attention. However, the majority of other participants took pains to state explicitly that they “did not” engage in NSSI as a way to get attention, but rather emphasized how they took pains to hide their injury from others.
This study found that emotional regulation was the most commonly endorsed function of NSSI. However, it is also clear that participants engaged in NSSI for a variety of reasons encompassing all the different functions of NSSI and that they frequently reported mixed motivations for NSSI. Thus for this sample it appears that NSSI can serve several functions simultaneously. The finding that NSSI can serve different functions raises further questions for future research to examine NSSI in the Singapore population, including how different functions may distinguish between different subgroups of self-injurers.
Research in the West has found specific relationships between the types of distress experienced and the functions of NSSI. In their work with female adolescents, Hilt et al. (2008) found that peer victimization was related to social but not automatic functions, and internal distress and depressive symptoms were associated with automatic but not social functions. This supports the earlier work of Nock and Prinstein (2005) who found a relationship between automatic positive functions and symptoms of major depressive disorder and posttraumatic stress disorder. These Western findings may have important implications for treatment and prevention of NSSI in Singapore youths, including the use of different treatment approaches depending on the function of NSSI in youth (Muehlenkamp, 2006). Additional research is warranted concerning specific relations between identified stressors and symptoms experienced by the Singapore adolescents and the functions of NSSI.
Relationship between parental invalidation and NSSI
This study also found that a perceived invalidating environment is associated with the presence of NSSI for Singaporean adolescents. Emotional regulation as the most commonly endorsed reason for NSSI supports this finding. Since adolescents who engage in NSSI likely experience more parental invalidation, they are more likely to have problems with emotional regulation and, consequently, more likely to resort to NSSI as a way of controlling strong emotions. This is consistent with the research literature. For example, Yap, Allen, and Ladouceur (2008) suggested that adolescents whose mothers responded in invalidating ways towards their expression of positive emotions tended to report using maladaptive emotional regulation strategies more frequently.
Moreover, the qualitative data supports the quantitative findings. Participants who engage in NSSI reported that their parents did not understand them or listen to them and frequently used verbal putdowns and criticisms. For many, this nonvalidation eventually led to them choosing not to share their feelings: “I refuse to tell them my feelings. I am afraid that they will think that I am just exaggerating, or lying, or pretending to be stressed.” That an invalidating environment is associated with NSSI for the Singaporean adolescent strengthens the possibility that a more general factor such as the quality of family relationships may be implicated in the development of NSSI (Dubo, Zanarini, Lewis, & Williams, 1997; Gratz, 2003; Gratz et al., 2002). This is also consistent with observations by clinicians such as Walsh (2006) who asserted that individuals who engage in NSSI might not have experienced any form of overt abuse.
The results of this study also point to some other possible areas for future explorations. It is noted that, in this study, a higher proportion (86.7%) of control group participants came from intact families when compared to the study group participants (70.0%; please see Table 1). In line with Linehan’s (1993) observation about the possible role played by psychological unavailability in the creation of an invalidating environment, it could possibly be argued that, in nonintact families, the parent, because of the challenges posed by his or her situation, may be more psychologically unavailable to his or her children and, possibly, more invalidating. However, this speculation needs to be confirmed by further studies. Another area of interest is the relationship of parental educational levels and a validating environment. It is noted that, for this study, participants who engaged in NSSI are more likely to have parents with lower educational levels for both fathers and mothers compared to those who do not engage in NSSI (Table 1). Conversely, control group participants are more likely to have parents with higher educational levels compared to those who engage in NSSI. One possibility would be that parents with higher educational levels may be exposed to more egalitarian styles of parenting and, therefore, more likely to be aware of the need to acknowledge their children’s feelings. Again, this needs to be confirmed with future studies.
Relationship between parental invalidation and academic stress
This study also reports a moderate, positive relationship between the level of parent invalidation and the level of academic stress for Singaporean adolescents. However, as this is a causal-comparative design, the question of causality cannot be firmly established (Heppner, Kivlighan, & Wampold, 1999). Nonetheless, this preliminary finding is useful in suggesting possible relationships between academic stress and an invalidating environment. The data from the qualitative interviews also supports an association between academic stress and parental invalidation. For instance, results of the interviews demonstrated two typical categories related to academic stress: parental expectations and self-expectations. In terms of parental expectations, parents pushing their children to excel, beginning at a young age, is a consistent theme. One participant clarified how parental approval and validation is tied to subjects doing well in exams: “You must keep up your performance. The moment you don’t, they won’t care for you. They will forever not approve of you.” This finding clarifies that an invalidating environment that involves passive abuse may play a critical role in the development of NSSI behaviors amongst Singaporean adolescents. Yet future studies should seek to clarify this relationship and explore if this is also true in more diverse populations and cultures. Overall, the findings of this study raised the possibility that for different populations of subjects who engage in NSSI, unique local, socioeconomic, and cultural factors may be important in the development of NSSI.
Limitations of the study
A limitation of this study is the small clinical sample of convenience used. Based on local observations and the observations of Walsh (2006) that the profile of those who engage in NSSI in the United States has shifted from adolescents with serious emotional issues to adolescents in the community who are less psychologically impaired, the need to include a community sample in a study on NSSI is strongly indicated. However, because permission could not be secured to study a community school population, this study was limited to an outpatient population thus limiting the results. Given that participants of this study were outpatients from the CGC, the findings may not be generalizable to adolescents in the general community population. Future studies should examine the phenomenon of NSSI in the broader Singaporean community by using a school-based sample.
The use of self-reports is another limitation of this study. Self-reports raise questions as to the validity of the data. For example, subjects who engaged in NSSI may be more likely to negatively remember their childhood experiences and may not accurately recall their memories relating to self-injury. Klonsky (2007) also highlighted the problem of subjects not being able to report their motivations accurately for NSSI because they lack insight, or because they feel the need to report reasons that are more socially acceptable. In this regard, future research should consider Klonsky’s (2007) suggestion regarding the use of ecological momentary assessment studies for understanding NSSI. In ecological momentary assessment studies, participants keep daily logs that allow researchers to capture and analyze real-time descriptions of their experiences of NSSI. Another limitation of self-reports is that we cannot be sure if the condition of the participants causes them to interpret their environment as invalidating or if family interaction is indeed a risk factor for the development of NSSI. Further longitudinal studies will need to be conducted to clarify the situation.
Finally, as a pilot study was not conducted on the application of the ICES, future studies will need to validate this instrument for use in the local population. It is hoped that this initial exploratory study will provide insights that will facilitate the development of a more effective instrument specifically for the local population in the future.
Recommendations for mental health professionals
Interventions for NSSI
The finding that NSSI can serve different functions suggests that clinicians need to tailor their interventions according to the function(s) identified for a particular patient. Nock and Prinstein (2004) suggested that interventions aimed at replacing NSSI with functionally equivalent behaviors might be most effective. Therefore for patients who rely on the automatic function as a way to regulate emotions, interventions aimed at helping them better regulate their emotions could be particularly therapeutic. On the other hand, if a patient’s NSSI serves a social reinforcement function, the teaching of social and communication skills may be therapeutic. This approach facilitates the customization of treatment for the individual adolescent and may lead to the development of specific treatment protocols for different subgroups of injurers, resulting in a more targeted approach to the treatment of NSSI (Muehlenkamp, 2006). Based on the literature, dialectical behavior therapy, which targets the following areas of dysregulation: self, interpersonal, behavioral, emotional and cognitive, with its skills modules of core mindfulness, interpersonal effectiveness, distress tolerance, emotion regulation and walking the middle path, appears to be the most promising treatment approach at reducing NSSI (Miller, Rathus, & Linehan, 2007).
The finding that an invalidating environment is associated with NSSI would suggest that assessment of individuals who engage in NSSI must include both individual functioning as well as an understanding of family functioning (Crowell et al., 2008). Systemic therapy and parent training aimed at reducing family conflicts and improving communication may be helpful in reducing NSSI behaviors amongst adolescents (Miller, Muehlenkamp, & Jacobson, 2009). Similarly, the finding that academic stress is associated with parental validation should alert mental health professionals to the role academic stress and other potential stressors may have on the family environment, especially in terms of creating conditions that may lead to an invalidating environment (Fruzzetti et al., 2005).
Interventions for academic stress
The findings that academic stress is associated with invalidating environments and the tendency of some who engage in NSSI to be perfectionist also suggest the importance of exploring how academic stress can be better managed for such adolescents (Nounopoulos, Ashby, & Gilman, 2006). A potential strategy could be the use of resiliency training to enhance coping strategies, specifically to increase the use of problem-focused coping (Steinhardt & Dolbier, 2008).
Prevention program for NSSI
When considering the findings on risk factors and functions of NSSI for the Singaporean adolescent population, prevention programs that address issues relating to stress management and emotional regulation may be particularly helpful. Another area of intervention is to expand awareness and understanding of the functions of adolescent NSSI beyond clinicians and physicians to include teachers, therapists, and parents. During the semi-structured interview, a young woman poignantly shared that she was “put off” by the assumption of her therapist that her self-injurious behavior was a way to get attention. This and other misconceptions (Caicedo & Whitlock, 2009) can be addressed in informational workshops. These workshops will also equip parents and professionals who work with adolescents with the knowledge to detect adolescents who may engage in NSSI. A promising model is the Signs of Self-Injury (SOSI: Jacobs, Walsh, McDade, & Pigeon, 2009) program which has been shown to be a potentially effective prevention program (Muehlenkamp, Walsh, & McDade, 2010)
Suggestions for future research
Besides the areas highlighted elsewhere in this article, future research is needed to clarify the concept of invalidation and an invalidating environment (Linehan, 1993). While some preliminary work explaining specific outcomes of different types of invalidation exists (Hilt et al., 2008; Yap et al., 2008), more research is needed to clarify the different dimensions of invalidation. The 14 items used in the ICES to measure specific parental behaviors reflect the eight dimensions that define an invalidating environment (Mountford et al., 2007). These eight dimensions are ignore emotions, negate emotions, overreact to emotions, ignore thoughts and judgments, negate thoughts and judgments, overreact to thoughts and judgments, overestimate problem solving, and oversimplify problems (Mountford et al., 2007). Questions for future research may include the following: how do these different dimensions contribute to an invalidating environment? What are the effects of different combinations of these dimensions on emotional dysregulation? And how are these different dimensions associated with some of the psychological correlates such as dissociation (Paivio & McCulloch, 2004; Polk & Liss, 2005) and alexithymia (Polk & Liss, 2005, 2007), which have been found to be mediators between trauma and emotions dysregulation? Finally, the identification and validation of other factors besides academic stress that may contribute to an invalidating environment is an additional area for future research.
Conclusion
The researchers developed this study to learn more about NSSI in the Singaporean adolescent population. In utilizing the concept of the invalidating environment to study the role of passive abuse in the development of NSSI, this study addressed a gap in the literature and attempted to understand the role of familial and care-giving relationships in the development of NSSI. The findings of functions served by NSSI for the Singaporean adolescent population have immediate treatment implications, especially in terms of tailoring treatment approaches to the functions served by NSSI. Finally, this study, in its finding of an association between academic stress and parental invalidation, also contributes initial empirical data on the factors that may contribute to invalidation, and suggests the importance of considering local socioeconomic and cultural contexts as such factors. The findings from this preliminary study serves as a basis for future research to gain a better understanding of NSSI in the Singaporean adolescent population and to facilitate future preventative and intervention programs for NSSI.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.