
Abstract
Objective
Nonsuicidal Self-Injury (NSSI) in China has increasingly interested clinicians, although few studies have investigated its risk and protective factors. This study examined the risk factors of NSSI among Chinese adolescents.
Methods
The researchers recruited adolescent participants with NSSI from a hospital outpatient clinic to form a case group and recruited adolescents without NSSI who provided informed consent from the school to form a control group. Participants completed a questionnaire, and data were analyzed using logistic regression.
Results
A total of 138 cases and 276 controls participated in this study. Binary multivariate logistic regression analysis with adjusting for age and sex showed that domestic violence (OR = 8.615, 95%CI: 3.081–24.091), parental overconcern (OR = 6.995, 95%CI: 3.447–14.192), guilt (OR = 4.949, 95%CI: 2.227–10.996), and school bullying (OR = 21.676, 95%CI: 6.799–69.109) increased the risk of NSSI, while peer support (OR = 0.068, 95%CI: 0.030–0.150) and living in an urban environment (OR = 0.157, 95%CI: 0.056–0.437) decreased the risk of NSSI.
Conclusion
Some psychosocial factors were confirmed to be independent risk and protective factors for NSSI in this study. However, the clinical significance of the results needs to be interpreted with caution due to sample size limitations.
Keywords
Introduction
Nonsuicidal self-injury (NSSI) is the intentional, self-inflicted damage to the surface of the body without suicidal intent (Brown & Plener, 2017) and is considered a separate class of behavior in the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) by the American Psychiatric Association (Halicka & Kiejna, 2018). Adolescents engage in NSSI behavior because NSSI has adaptive functions, including self-punishment, emotional regulation, and communicating distress. (Edmondson et al., 2016; Klonsky, 2007). A meta-analysis of characteristics of NSSI indicated that the most common trait is managing or altering a person’s intrapersonal state (e.g., emotions, thoughts, or bodily sensations) (Taylor et al., 2018). Existing research and guidelines demonstrate that NSSI adolescents are at significant risk of unhappiness, distress and even unnatural death. Additionally, NSSI is associated with a number of psychiatric disorders, including depression, anxiety, post-traumatic stress disorder (Bentley et al., 2014), and eating disorders (Kiekens & Claes, 2020).
Nock’s theoretical model posits that NSSI is mainly caused by distal risk factors, personal vulnerability factors, and stressful events (Nock, 2009). This theoretical model guides researchers and physicians thinking about the etiology of NSSI, although the precise causes of NSSI remain unclear. Currently, many risk factors, such as bullying, a history of abuse, and family conflicts (Plener et al., 2018), are known to increase the risk of NSSI. Especially, childhood abuse, including emotional neglect, emotional abuse, sexual abuse, physical abuse, and physical neglect, has been found to increase the risk of NSSI (Liu et al., 2018). Shame has also been shown to significantly predict NSSI status (Hack & Martin, 2018). An affectionless control childrearing style was associated with a history of trauma and have been positively associated with NSSI in a recent review (Fong et al., 2022; Catalan et al., 2017). Further, children who experienced multiple separations from their parents during childhood have an increased risk of NSSI (Astrup et al., 2017). These studies independently examined whether one factor increases the risk of NSSI, therefore there is a lack of studies which discuss multiple risk factors in one single sample.
Clinical practice and epidemiological surveys have also found that some psychosocial factors can reduce the incidence of NSSI in adolescents. A survey of 2980 participants found that increased social support can reduce the risk of NSSI (Christoffersen et al., 2015). Children who migrate from rural to urban environments or from urban to rural environments experience increased stressful life events, which places them at higher risk of developing NSSI (Gao et al., 2020). Frequent changes of living environment may cause instability or lack of social support for adolescents (e.g., unfamiliar new school and new students). The effects of social support and migration on adolescent NSSI may be more easily observed in China, where many teenagers frequently change places of residence and lose contact with their former friends due to rapid unbanization and industrialization. Currently, in China, many children and adolescents living in rural areas remain in rural areas to attend school while their parents live and work in cities. These children and adolescents who are separated from their parents have been referred to “left-behind children” (von Boch-Galhau, 2018), this reality results in a lack of parental care to the children. In addition, because of the small number of schools and the low concentration of students in rural areas, many children and adolescents attending primary and junior high schools choose to live independently because their parents cannot take care of them. However, children and adolescents living in cities do not face these challenges. To date, few studies have explored the relationship between living environment and self-injury.
This study aimed to explore whether multiple associated factors are risk or protective factors for NSSI among adolescents in a sample. A meta-analysis has reported a greater prevalence among women than men (Bresin & Schoenleber, 2015). Given this, sex is also a factor in NSSI behavior. Existing risk factors are closely related to the social environment and have been primarily studied in Europe and the United States, and China has a high incidence of NSSI (29%) (Tang et al., 2018). In this study, we speculated that the risk factors for NSSI in China might differ from those reported in the existing literature. Although many epidemiological surveys of NSSI among Chinese adolescents have been conducted in recent years, few case–control studies have explored its etiology. This study examined the risk factors for NSSI in Chinese adolescents aged 12–20 using a hospital- and school-based case–control study.
Materials and methods
Study sample
Participants included adolescents aged 12–20 years with and without a history of NSSI who attended the outpatient clinic of the Clinical Psychology Department of the Affiliated Hospital of Qingdao University between November 2021 and June 2022. Participants in the control group were middle school students, high school students, and college freshmen who agreed to participate in the study. All participants completed a self-report questionnaire (Supplementary material-S1) that included demographic characteristics (e.g., age and sex), possible risk and protective factors (e.g., history of emotional neglect, emotional abuse, sexual abuse, physical neglect, physical abuse, domestic violence, peer support, parental control, school bullying, guilt, separation from parents in childhood, residential environment), and medical history (e.g., whether the participants had a history of central nervous system disease). Participants were asked to answer “Yes” or “No” to indicate their history of exposure to the investigated factors during childhood. The questionnaire results and demographic data of 414 adolescents were included in this study. Participants aged 18 and older provided consent to participate. Those participants under the age of 18 provided assent, and their parents provided consent. This study was approved by the Ethics Review Committee of the Affiliated Hospital of Qingdao University (ethics approval number QYFY WZLL 26,864), and all participants and their parents provided written informed consent.
Case and control selection
Adolescents were included in the case group if they met the following criteria: (1) having a self-reported history of self-injurious behavior (e.g., cutting, scratching, hitting or banging, carving, and scraping); (2) being aged 12–20 years; and (3) lacking a history of central nervous system diseases or other major medical illnesses. The final case sample included 138 patients.
From October 2021 to March 2022, 276 teenagers under the age of 20 living in Qingdao, Shandong, China, agreed to participate in the study and denied a history of NSSI. The participants completed a questionnaire identical to that of the case (Supplemental material-S1). The response rate to the questionnaire was 100%. Students were included in the control group if they met the following criteria: (1) lacking a self-reported history of self-injurious behavior, (2) being students who were aged 12–20 years; and (3) having no central nervous system disease or a history of another major medical illness. All study participants were residents of the local areas and had lived there for a long time.
Statistical methods
We analyzed the differences in the proportion of exposure to the risk and protective factors between the case and control groups. All tests were two-tailed, with the significance level set at p < .05. Odds ratios were calculated for the incidence of each exposure factor in the case and control groups, and the 95% confidence interval was calculated. First, a univariate analysis was performed for the two groups by calculating the chi-square and p-values to assess the association between exposure factors and NSSI. Variables that were significant in the univariate analyses were identified, including emotional neglect, emotional abuse, physical neglect, physical abuse, domestic violence, peer support, parental control, school bullying, guilt, separation from parents in childhood, and residential environment. Since NSSI is more common in women aged 16–19 (Kądziela-Olech et al., 2015; Wilkinson et al., 2022), we adjusted for age and sex in the binary logistic regression model using the forward likelihood ratio. Age and sex were added to obtain a binary logistic model that adjusted for age and sex. The Hosmer–Lemeshow test was performed to determine whether there was a significant difference between the regression equation and the saturated model. All statistical analyses were performed using the IBM SPSS ver. 26 software.
Results
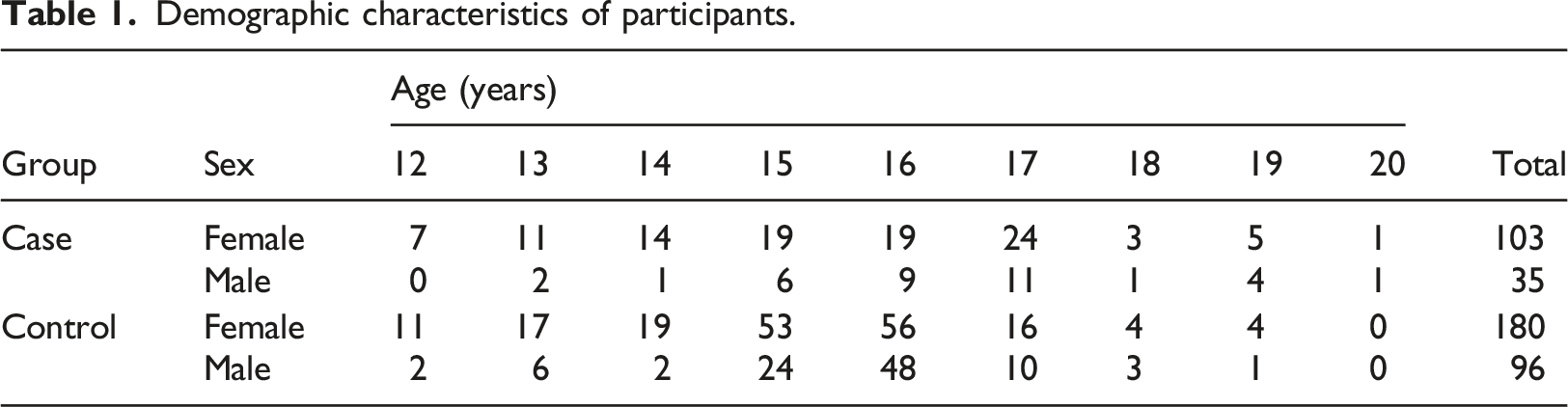
Demographic characteristics
Demographic characteristics of participants.
Demographic characteristics of the case and control groups.
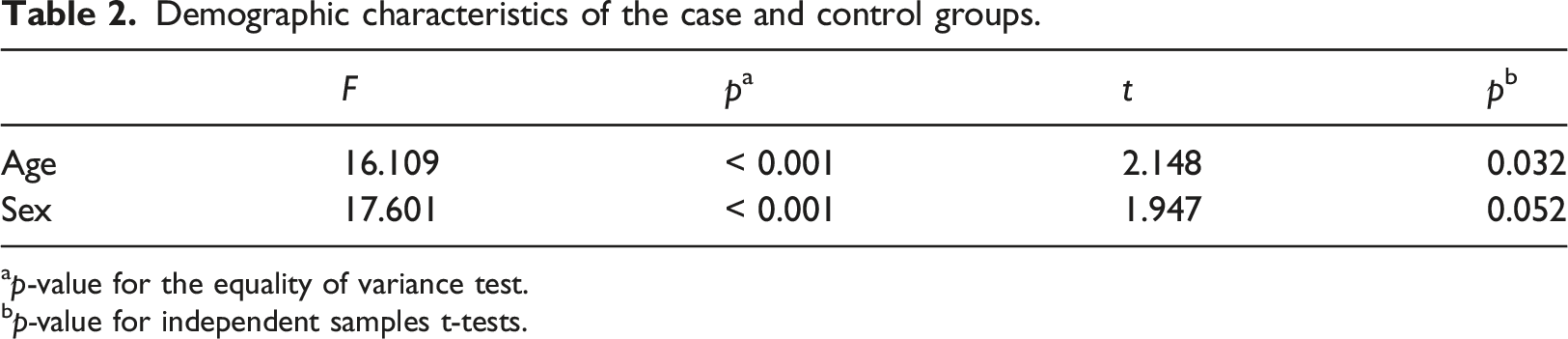
ap-value for the equality of variance test.
bp-value for independent samples t-tests.
Univariate analysis
Risk and protective factors for nonsuicidal self-injury.
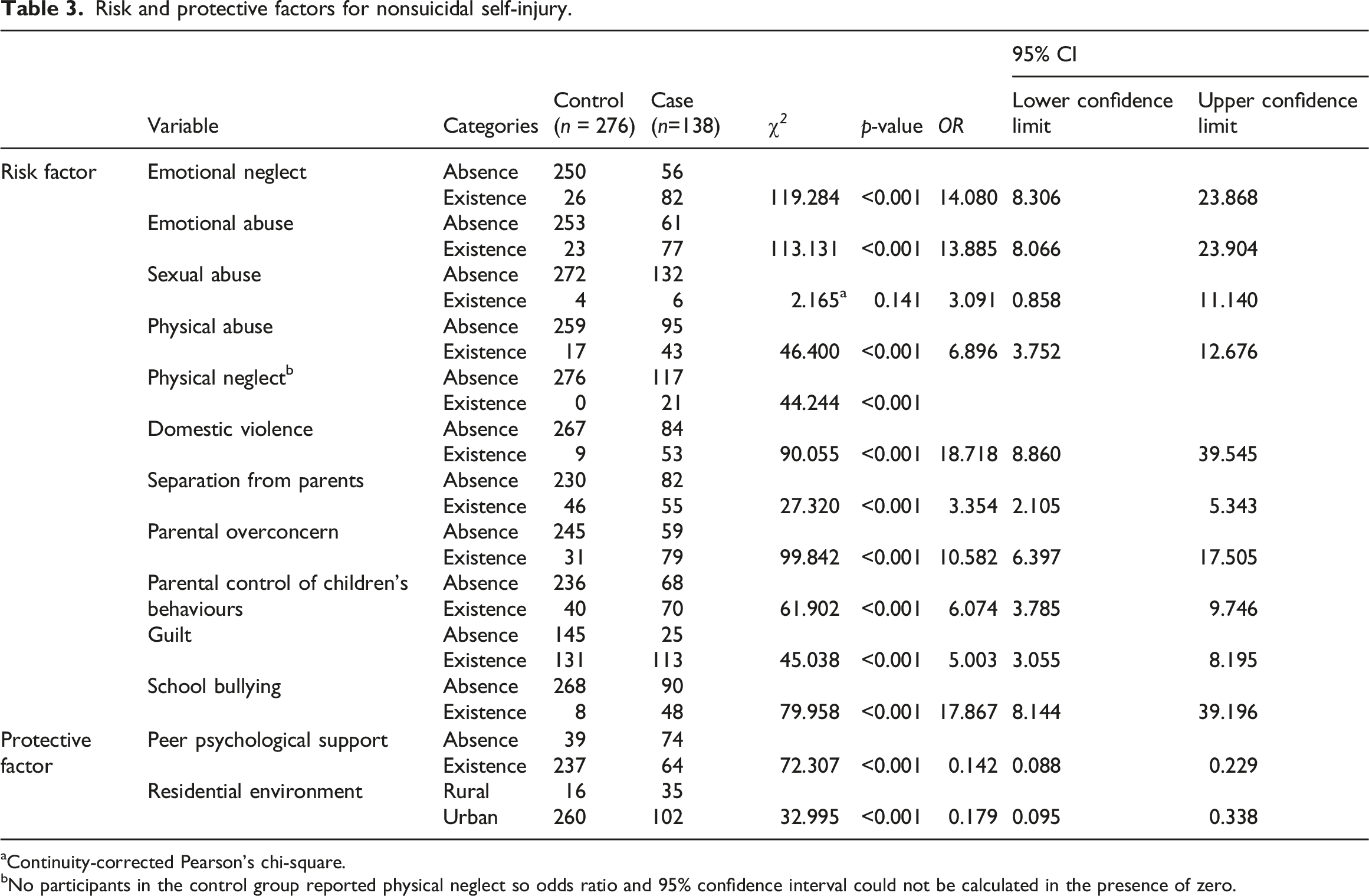
aContinuity-corrected Pearson’s chi-square.
bNo participants in the control group reported physical neglect so odds ratio and 95% confidence interval could not be calculated in the presence of zero.
Regression analysis
The variables that were significant in the univariate results (Table 3) were selected for the binary multivariate logistic regression model, adjusting for age and sex. The forward likelihood ratio method was used. The forward likelihood ratio method automatically filtered variables that are significantly related to the outcome, and eight variables were entered into the final logistic regression model.
Variables included in the initial binary multivariate logistic regression equation with adjusting for age and sex by forward likelihood ratio.
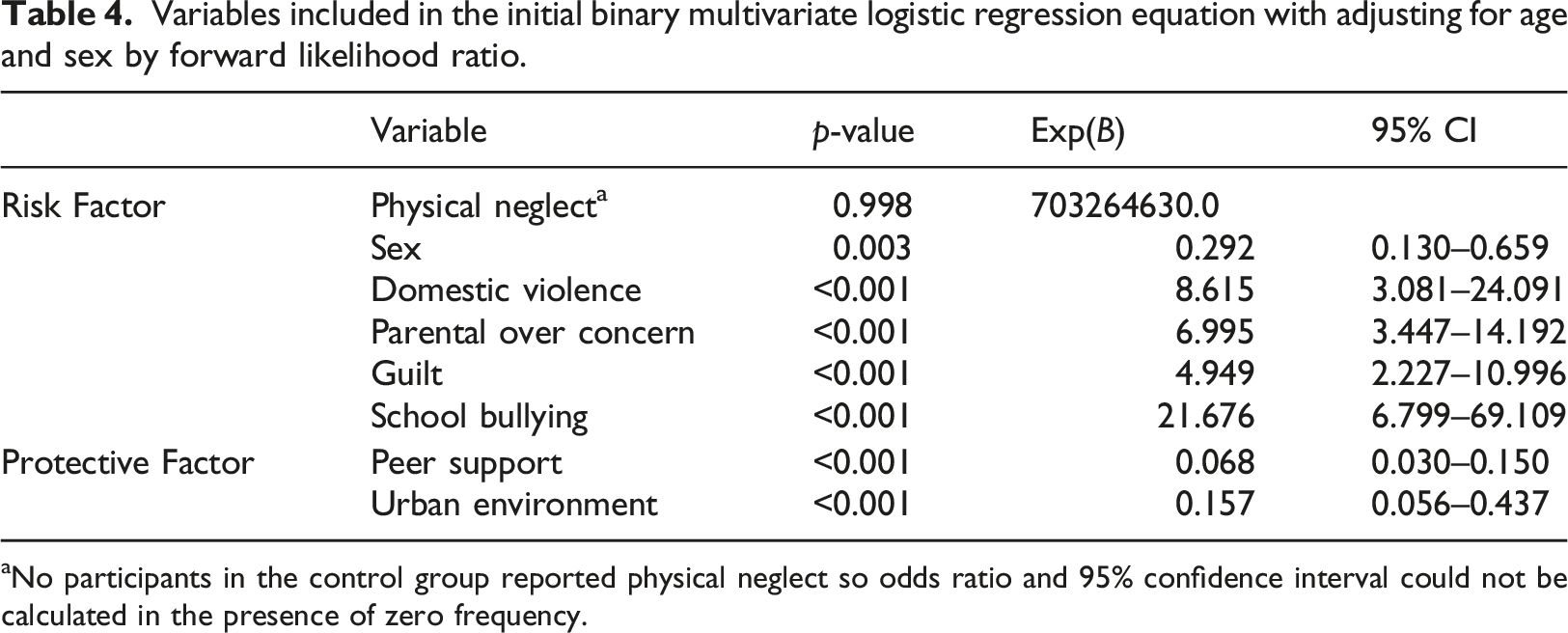
aNo participants in the control group reported physical neglect so odds ratio and 95% confidence interval could not be calculated in the presence of zero frequency.
Discussion
This study investigated possible risk and protective factors of NSSI to guide clinical psychotherapy. Significant risk factors included domestic violence, parental control, guilt, and school bullying, and the protective factors were peer psychological support and living in an urban environment. The strength of this study is that it is the latest study on the differences between adolescents with NSSI and adolescents without a history of NSSI in China. The study compared the childhood experiences of the case and control groups by reviewing the participants’ experiences before the age of 12. Therefore, this study provided some novel and critical information on the etiology of NSSI. Compared with the univariate analysis, the multivariate regression model provided better evidence of each variable’s joint effect on NSSI.
This study has several limitations. First, the sample size is small. As the multivariate binary logistic analysis required a sample to be 10 to 20 times the number of variables, the results of this study need to be interpreted with caution. In particular, some of the results were inconsistent with previous research, and it is unclear if the setting of Qingdao, China led to these surprising findings. In addition, although efforts were made to design a retrospective study, the differences in the results could be due to the self-report survey method; therefore, it is difficult to draw a convincing conclusion.
Numerous studies have pointed to the female identity as a risk factor for NSSI (Brown & Plener, 2017; Idig-Camuroglu & Gölge, 2018). NSSI has been found to be more common in young women aged 16–19 years, with no significant differences observed for the other age groups (Wilkinson et al., 2022). This study has relevance for clinical treatment, and sex cannot usually be changed. Since sex has a great impact on NSSI, sex and age matching was used in this study to reduce any sex effects on the results that were not eliminated through matching (Pearce, 2016).
Childhood abuse, including emotional, emotional, sexual, and physical abuse, and physical neglect, has previously been shown to be a proven risk factor for NSSI (Liu et al., 2018). However, Liu et al.‘s (2018) meta-analysis did not include research conducted in China and did not reflect childhood abuse in China, which may be due to the lack of NSSI-related research in China. This case–control study may add to the clinical studies and meta-analyses of NSSI etiology. Although sexual abuse has been established as a definite risk factor (Devries et al., 2014; Klonsky & Moyer, 2008), the present study, conducted in Shandong, China, did not identify sexual abuse as a significant risk factor. We believe this relates to China’s social environment and cultural background. Chinese families rarely ignore teenagers and instead pay much attention to them. This conjecture must be confirmed through further research. The five forms of child abuse often co-occur or partially co-occur (Liu et al., 2018), as shown in other studies (Finkelhor et al., 2007) (Teicher et al., 2006). This co-occurrence could explain why some factors were associated with NSSI in the univariate analysis but not in the multivariate binary logistic regression and were excluded from this study. Various types of abuse do not exist in isolation, and multiple types often occur unintentionally in a family (DeJong et al., 2022).
Evidence-based medical evidence has demonstrated the relationship between social support (Christoffersen et al., 2015), parental control, separation from parents, and NSSI. A child’s experience of being separated from their parents increases their risk of developing NSSI. Such an experience may lead to children being alienated from their parents, which is considered a form of trauma (von Boch-Galhau, 2018). Parental control includes both behavioral and response control (Fong et al., 2022), and previously, parental affectionless control was found to increase the risk of NSSI (Goschin et al., 2013). However, parental control may be a consequence of NSSI rather than a cause (You et al., 2017). One strength of this study was the inclusion of more factors than in previous studies and the finding that parental control, parental separation, and peer psychological support were correlated. These factors correlated with child abuse; however, since this was a cross-sectional study, any causal conclusions about whether these factors (i.e., parental control, parental separation, peer psychological support) caused NSSI could not be made. Further prospective studies are required to demonstrate the causal relationship between these familial characteristics and NSSI.
Emotional rumination may mediate the relationship between childhood emotional abuse and NSSI (Gu et al., 2020). Other forms of abuse which were described above may lead to identity confusion. Parental warmth and authority-control patterns contribute to children’s healthy development (Lavi & Slone, 2012), while excessive parental control has been associated with various psychiatric disorders (e.g., depression and anxiety) (Yap et al., 2014). Shame coping strategies can amplify psychopathology (Martin et al., 2021), and NSSI is one way of coping with shame and providing temporary relief (Mahtani et al., 2019; Møhl and Rubæk, 2017).
Peer relationships play a key role in the occurrence of NSSI, and experiences with school bullying and peer rejection increase the occurrence of NSSI (Esposito et al., 2019). Peer psychological support is both a type of peer relationship and social support, and its key protective effect occurs when participants perceive this social support (Nemati et al., 2020). There is little clear evidence or theory regarding the protective role of living in an urban environment on the occurrence of NSSI; however, the current findings suggest that living in an urban environment reduced child abuse and parental control and increased social support. Although our results showed that living in an urban area was an independent protective factor, our study did not examine participants’ urban-rural migration. Thus, this result should be interpreted with caution.
Psychotherapy is the preferred treatment modality for adolescents with NSSI (Plener et al., 2018). Clinicians can refer to possible psychosocial etiologies identified in the literature when communicating with patients and their family members. However, a paucity of well-controlled studies have examined the efficacy of treatment for NSSI (Turner et al., 2014). Dialectical behavior therapy (DBT) appears to be the most effective treatment currently available, as demonstrated in randomized controlled trials (McCauley et al., 2018; Ramsey et al., 2021). However, DBT research on affective disorders and long-term prognosis in adults with NSSI is lacking. Until a suitable treatment for NSSI adolescents is available, creating policies to prevent some negative parental behaviors toward their children is necessary to potentially reduce the social and medical burdens of NSSI. However, the ability of these measures effectively reducing the incidence of NSSI requires evaluation by policy-making and technical experts.
This study did not clarify whether the risk and protective factors of NSSI in China differ from those previously identified worldwide. As a rigorously designed case–control study, this study adds to the existing literature. Consistent with existing research, the present study indicated that childhood abuse, domestic violence, parental control, and school bullying increased the risk of NSSI, and peer support reduced the risk. No previous research has explored the relationship between NSSI and urban and rural living environments. The present results show that living in an urban environment may reduce the risk of NSSI, which is clinically relevant for the diagnosis and treatment of NSSI in different urban or rural environments. Future research should focus on the social and cultural characteristics of each distinct region to motivate policymakers to reduce the occurrence of NSSI based on the relevance of these characteristics to NSSI.
Supplemental Material
Supplemental Material - Risk factors and protective factors for nonsuicidal self-injury in adolescents: A hospital- and school-based case–control study
Supplemental Material for Risk factors and protective factors for nonsuicidal self-injury in adolescents: A hospital- and school-based case–control study by Shuo Geng, Lin Wang, Jinping Sun, Mingdong Xu, Li Zhang, Zhi Yi, Jun Ji and Xu Zhang in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. Assistant Professor Wen Zhang provided grammar and writing assistance during the revision process, and we would like to sincerely thank her.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Review Committee of the Affiliated Hospital of Qingdao University (ethics approval number QYFY WZLL 26864), and all participants and their parents provided written informed consent.
Patient consent statement
Paticipants in this study have signed informed consent. Permission to reproduce material from other sources.
Data availability statement
Data available on request due to privacy/ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.