
Abstract
The risk of exposure to intimate partner violence (IPV) between caregivers is increased during early childhood. The adverse effects on the health and development of the youngest children may be severe. Effective and promising interventions for children who have experienced IPV have been developed and evaluated. However, there is a lack in knowledge about how the children themselves experience the interventions. The aim of this study was to contribute to the evaluation of group treatment designed to improve the psychological health of young children in the aftermath of family violence by elucidating the children’s experiences of participating. Nine children, aged 4 to 6 years, were interviewed after participating in group programmes specifically designed for children who have been exposed to intimate partner violence. A semi-structured interview guide with open-ended questions was used. The interviews were transcribed and analysed using interpretative phenomenological analysis, to ensure a focus on the children’s own views and experiences. Five master themes embracing the children’s experiences were identified: joy – positive emotional experience of participation; security – feeling safe; relatedness – relationships within the group; to talk – externalised focus on the violence; and competence – new knowledge and skills. Theoretical and clinical implications and the benefit of including very young children’s views and experiences in research are discussed.
Keywords
Introduction
Effective and promising interventions for children who have experienced intimate partner violence (IPV) have been developed and evaluated for use in different contexts (in social services and psychiatric care), with different age groups (from infants to teenagers) and in divergent settings (individual and dyadic, as well as group; Cohen, Mannarino, & Deblinger, 2006; Graham-Bermann, Lynch, Banyard, DeVoe, & Halabu, 2007; Jouriles et al., 2009; Lieberman, Van Horn, & Ippen, 2005). The interventions in general aim at reducing symptoms of psychological distress and behaviour difficulties among the children; additionally, the treatment interventions focus to various degrees on self-regulation, social interaction, difficulties in the parent–child relationship, psychoeducation on violence and trauma, and the non-offending parent’s psychological health.
There is broad agreement that experiencing violence against a caregiver is a serious risk factor for children’s psychological health and development. Several studies have shown increased risk for a variety of symptoms of psychological distress (mainly anxiety, depression and post-traumatic stress reactions) and for behaviour disorders, disturbances in self-regulation, difficulties in social interaction, including difficulties in peer relationships and disorganised attachment (Chan & Yeung, 2009; Evans, Davies, & DiLillo, 2008; Holt, Buckley, & Whelan, 2008; Kitzmann, Gaylord, Holt, & Kenny, 2003; Levendosky, Huth-Bocks, & Semel, 2002; McCloskey & Stuewig, 2001; Margolin & Vickerman, 2007; Zeanah et al., 1999). Some 40% to 60% of children exposed to IPV are estimated to exhibit clinically significant problems and are in need for treatment (Grych, Jouriles, Swank, McDonald, & Norwood, 2000). Furthermore, it has been recognised that babies and toddlers, who often stay physically close to their parents, are at increased risk of exposure to violence between caregivers and that the effects on their development may be most severe due to the neurological sensitivity of the growing brain (Fantuzzo, Boruch, Beriama, & Atkins, 1997; Gjelsvik, Verhoek-Oftedahl, & Pearlman, 2003; Howell, 2011; Levendosky, Huth-Bocks, Semel, & Shapiro, 2002).
Among the broad range of treatment methods designed for children with experience of IPV that have been developed, few methods have so far shown enough effectiveness to be recommended for dissemination (Australian Center for Posttraumatic Mental Health and Parenting Research Center, 2014). Interventions with scientific support are, for example, trauma-focused cognitive behaviour therapy (TF-CBT) for school-aged children and adolescents, child parent psychotherapy (CPP) for toddlers and preschool-children and Kids Club for school-aged children (Cohen et al., 2006; Graham-Bermann et al., 2007; Lieberman et al., 2005). The development of new methods and the adjustment of available methods are continuing.
Group interventions for children exposed to IPV are reported as appreciated by parents (Georgsson, Almqvist, & Broberg, 2007; Grip, Almqvist, & Broberg, 2011) but there is a lack in knowledge of how young children experience the treatment. Low correlation has been shown between school-aged children’s and their parents’ experiences of mental health services in general, which suggests that parents cannot represent their children in questions of experience and satisfaction with mental health care (Biering, 2010; Garland, Haine, & Boxmeyer, 2007; Lambert, Salzer, & Bickman, 1998).
One possible explanation for the neglect of children’s views can be concerns about children’s capacity to express their views reliably (Day, Carey, & Surgenor, 2006), even though children from the age of 3 have been shown to form and retain accurate, organised and verbally accessible memories of past experiences (Fivush, 1998). If interviews with young children are developmentally appropriate, children as young as 3 and 4 years have been shown to provide meaningful information about their experiences (Hershkowitz, Lamb, Orbach, Katz, & Horowitz, 2012; Lamb et al., 2003). Techniques that enhance the possibility of children being competent informants about their experiences include establishing rapport and offering the children a chance to practice providing detailed information of experienced neutral events before turning to substantive issues, as well as clearly informing the children about their role as expert informants and the acceptability of their disagreeing with or correcting the interviewer (Lamb & Brown, 2006). The use of open-ended questions and prompts and the use of information previously mentioned by the children as cued invitations have proved to elicit more detailed and more correct information than forced-choice and suggestive questions (Lamb et al., 2003). One can argue that some experiences, such as parental IPV, are more demanding for children to recall and describe than other experiences, but asking the children to describe their own actions and perceptions has been shown to facilitate the narration of even such stressful events (Georgsson, Almqvist, & Broberg, 2011).
Adding the perspective of the children to the field of research on interventions for children exposed to IPV is important for several reasons. Children’s right to be heard and to express an opinion on issues that concern themselves is one of the cornerstones in the UN’s Convention on the Rights of the Child (United Nations, 2014). The satisfaction of children may additionally be related to completion of treatment, receptiveness to treatment for future problems and readiness to recommend services to others (Godley, Fiedler, & Funk, 1998). Furthermore, the perspectives of children contribute to knowledge that is useful in developing, evaluating and implementing services in clinical settings (Carlberg, Thorén, Billström, & Odhammar, 2009; Day et al., 2006; Dew & Bickman, 2005).
While there is a lack of research on children’s views in research concerning interventions for children exposed to IPV, there are a few studies available with children as informants concerning general mental health services (Biering, 2010; Carlberg et al., 2009; Dew & Bickman, 2005; Godley et al., 1998). These studies concern children’s experiences of participating in individual, family and group therapy, mainly involve school-aged children and teenagers and show contradictory results; the majority of the children have described negative as well as positive aspects of participating (Buston, 2002; Midgley, Target, & Smith, 2006). Many children seem to appreciate therapy and have described it as helpful (Broberg et al., 2011; Carlberg et al., 2009; Day et al., 2006; Georgsson et al., 2007; Midgley et al., 2006). They value being listened to and being included in the therapy and appreciate a supportive professional relationship (Buston, 2002; Stith, Rosen, McCollum, Coleman, & Herman, 1996; Strickland-Clark, Campbell, & Dallos, 2000). Furthermore, children seem to prefer treatment that includes activities and the possibility of play (Day et al., 2006; Lobatto, 2002; Moore & Seu, 2011; Stith et al., 1996). Children taking part in group treatment have reported that the main benefit was to meet other children with similar experiences, which made it possible for them to speak openly and to feel less isolated and different (Metel & Barnes, 2011).
Nevertheless, a substantial proportion of children who have been in psychotherapy have also reported negative feelings and experiences. They feel insecure about the reasons for and the purpose of therapy, as well as about the rules of the therapeutic sessions (Lobatto, 2002; Paul, Foreman, & Kent, 2000). Children have described being wounded by judgements and reprimands during the sessions, and some children have stated that therapy can be a painful experience of feeling overwhelmed and also not understood (Strickland-Clark et al., 2000). They have reported that therapy can make certain aspects of their life worse, including making them feel different in relation to peers, and some children wish not to take part (Carlberg et al., 2009; Midgley et al., 2006; Paul et al., 2000).
There is a gap in knowledge concerning children’s experiences of taking part in psychotherapeutic and supportive interventions directed towards them, including children exposed to IPV. In particular, knowledge of younger children’s experiences of participating in such interventions is insufficient. The aim of this study was to contribute to the evaluation of group treatment for young children exposed to IPV by elucidating the children’s experiences of participating in treatment.
Method
The sampling, data collection and analysis were performed in accordance with the principles of interpretative phenomenological analysis (IPA), which was considered useful, as it can contribute to understanding the phenomenon from the perspective of the informant (Smith, Flowers, & Larkin, 2009).
Participants
The sampling in IPA is typically purposive, as the informants are chosen for their ability to contribute to the research question. A homogeneous sample is preferable since it makes it possible to elucidate the phenomena more specifically. Furthermore, the number of informants is usually small (3–10), permitting analysis of each case as thoroughly as possible (Smith et al., 2009). In this study, nine children from two different agencies were interviewed: five girls and four boys, aged between 4 and 6 years (M = 5.5 years, Med = 5.5 years, no siblings). Five of the children attended one agency and four the other. Background data were obtained from the caregiver who took part in treatment, eight mothers and one foster-parent.
The children had all experienced IPV against the mother for a significant period of their lives. In seven cases, the perpetrator was the biological father; in one case, the biological father plus a stepfather; and in one case, a stepfather. The violence against the mothers included slaps, hits, kicks, strangulation and sexual abuse. The mothers reported that the physical violence had ceased, although six mothers reported that they were still exposed to verbal offence and threats from the perpetrator. According to their mothers, seven children had been physically abused by the same perpetrator (e.g. slaps, hits, pushes and strangulation attempts). No ongoing violence against the children was reported at the time of the interview.
All children lived in one of the two major urban areas in Sweden and were Swedish speaking. Six children had at least one parent who was not native Swedish. Seven children lived with the abused parent, one child lived in foster care and one child lived alternately with both parents. Seven children had no contact with the abuser.
Treatment
Children were recruited from two treatment agencies with well-established, manual-based and documented group interventions for children exposed to domestic violence. Both programmes consisted of weekly sessions in a group setting for children and parallel groups for abused parents, with two experienced group leaders, either psychologists or social workers, per group. Children in the groups were within an age span of 18 months, with 4–5 children in each group. Treatment length was 12–15 weeks, with weekly sessions on a fixed day and time, and took place in secure premises that had a locked entrance and were well equipped according to the developmental needs of children (e.g. toys, materials, furniture). For a child to be accepted for treatment, the experience of IPV was to be considered the major problem for the child and the violence had to be ended before enrolment. Participation was voluntary and free of charge.
One agency was community-based, to which parents exposed to IPV were able to apply for support for their children. This agency offered a group intervention with a psychoeducative approach based on Children Are People Too (CAP), a programme originally developed for children of parents with alcohol and drug addiction (Hawthorne, 1990), which has been adapted for children exposed to IPV (Georgsson et al., 2007; Grip et al., 2011, 2012). The other agency was a child and adolescent psychiatry unit, specialising in treatment for traumatised children. Children were referred to this unit because of complex symptomatology. The group treatment offered at this agency was developmentally informed trauma-focused psychotherapy based on trauma theory and psychodynamic theory (Ekbom & Landberg, 2003). At both agencies, the programmes were highly structured, and included reoccurring rituals and trauma-focused components. Every session was structured around a theme such as violence, security, family relations, separation, recognition and expression of feelings or affect regulation. The sessions were planned addressing several modalities at each occasion including verbal, relational and body-focused activities. Creative techniques such as play, drawing and role-playing were used as well as structured games and exercises. Children were offered a variety of tools to express themselves: toys, creative materials, books and so on. The sessions also included a joint snack. Children were accompanied to treatment by their caregiver, and during sessions caregivers stayed in an adjacent room.
Procedure
Parents received verbal and written information about the study when they were invited to take part in the intervention, and were asked for consent to participate at their next appointment. At the end of the intervention programme, the parents were asked about scheduling a research interview for their child. All the parents approached agreed to their child’s participation. The parents were encouraged to inform their child about the study before the interview.
At the time of the interview, the children received verbal information from the interviewer, and were asked for consent to participate. The children’s consent was seen as an ongoing process, and during the interview, they were given the opportunity to influence their own participation (Dockett & Perry, 2007, 2011). The children could end the interview, take a pause or pass on a question at any time. All the children wanted to participate. Eight children were interviewed without their parents, while one child chose to have the mother in the room during the interview. Each interview lasted between 27 and 53 minutes, and all interviews were performed in May and June 2013 at the agencies. The interviews were performed by the first author, an experienced child psychologist and psychotherapist, who was independent of the treatment agencies.
Instrument
In research with children, the guidelines for conducting interviews need to be adapted to permit extended time for the children to become comfortable, as well as a more active and guiding approach from the researcher than otherwise (Smith, 2004). In the present study, the children were first asked to talk about going to preschool or about what they liked doing at home, in order to establish rapport and allow the children to practise being interviewed (Lamb & Brown, 2006). A semi-structured interview guide was then used that focused on the core request to tell about their experiences of participating in the group treatment, with possible follow-up questions within several areas (see Table 1). Prompts and probes such as ‘Can you tell me more about that?’ and ‘Can you explain what you mean?’ were frequently used. In addition, all the children were asked to make a drawing representing themselves doing something in the intervention programme: when appropriate, the drawings were then used as cues for further questions. All interviews were recorded and transcribed verbatim.
Structure of the interview guide.
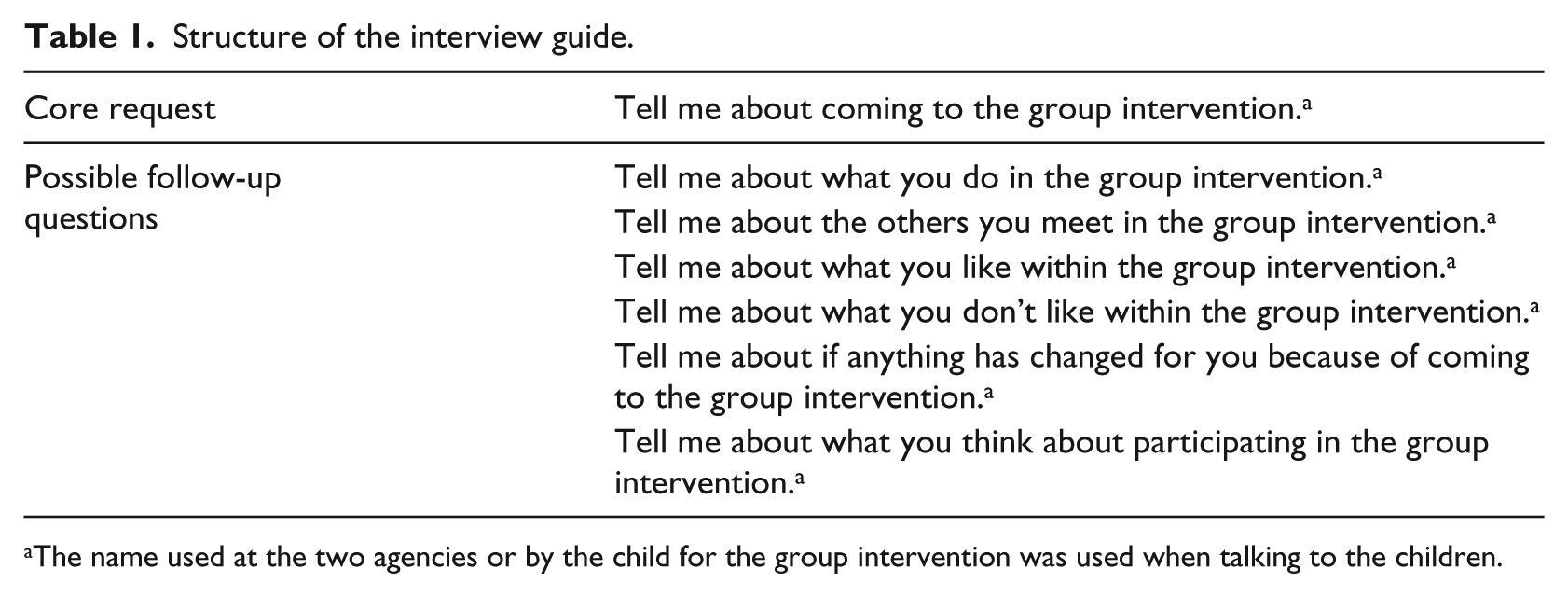
The name used at the two agencies or by the child for the group intervention was used when talking to the children.
Analysis
The transcribed interviews were analysed using IPA; the approach is inductive, which can allow unexpected themes to emerge, and the interpretation is descriptive, empathic and critical (Smith, 2004; Smith et al., 2009). The analysis was carried out in five steps according to Smith et al. (2009). The first three steps were (1) listening to the interviews and repeatedly reading the transcripts while making initial descriptive comments, (2) drawing emerging themes out of the initial comments and (3) forming clusters of themes as superordinate themes, which were listed together with illustrating quotations. These three steps were repeated for each interview and the two final steps were then taken: (4) carrying out analysis across cases to find common structures and master themes that embraced commonalities and discrepancies in the phenomena and (5) transforming each theme to a narrative account, with illustrating quotations to explain the content. During the analysis, themes and interpretations were checked against the transcripts. Each step of the analysis was initially carried out independently by the first author, and then revised in collaboration with the second author before moving to the next step.
Ethical considerations
Research involving vulnerable and traumatised children or children with parents in conflict implies specific challenges, including the child’s consent, the child’s vulnerability and risk for re-traumatising, possible conflicts of loyalty for the child and the imbalance in power between researcher and child. During this study, the notions above were held in mind and an effort was made to recognise each child’s limits of participation, to warrant the positive approval of the child’s participation from the abused parent and to keep to the focus of the interview and not encourage the child to speak about trauma. The study was approved by the Regional Ethics Committee in Uppsala (Dnr 2012/246).
Results
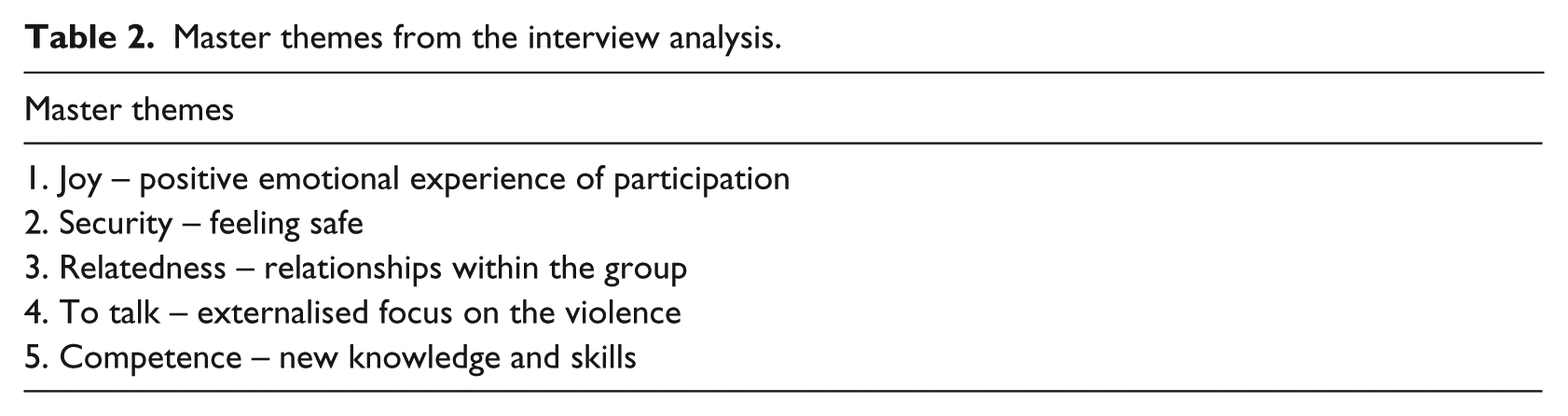
Five master themes emerged in the analysis of the interviews with the children (see Table 2). The first three themes embody how the children experienced the context of taking part in the interventions, and the two latter themes describe experiences about the content of the interventions. In this section, the themes are outlined one by one and are illustrated by quotes from the children.
Master themes from the interview analysis.
Joy – positive emotional experience of participation
All children expressed positive experiences of participating in the groups. The theme of joy contains an overall positive experience and an expressed motivation to participate.
Joy and appreciation of having fun was expressed: ‘Fun. I liked everything. I want to go there’, ‘I like playing, I like laughing, I like having fun . . .’, ‘It feels good . . . that I want to be here. It’s fun . . . and I want to be here, because it’s just fun to be here, it is fun to play here’, ‘It’s good that I can feel happy; I can laugh, I can do what I want and play’. The other participants were part of the joyful experience: ‘It’s fun to play with my friends’, ‘It’s good because we play . . . that we do fun things in the group, coming here is really good . . . to play’; and in some instances children expressed joy in the organised activities: ‘We do fun things’, ‘Working . . . it’s something really fun!’
The children described having a strong motivation to participate. They wanted to take part in the intervention and to be part of the group: ‘I like coming to the group’, ‘I like to work in the group’, ‘I want to participate’.
Security – feeling safe
Several children expressed feelings of safety in the group. The theme contains experiences of physical safety as well as emotional security.
The children in this study did not seem to assume that safety was something they could take for granted, as they explicitly stated that they appreciated being safe and protected from violence and threat while in the group: ‘What’s good about the group is that you can play, feel happy; nobody is frightening, you are not afraid, nobody is fighting and stuff’, ‘In the group you don’t have to do anything you don’t want to’. This theme was given clear superiority for one child: ‘What I like best about the group is that nobody frightens me here’.
Predictability in terms of the room, the furniture and the fixed day and time were all aspects mentioned, as were ritualised activities and the stability in meeting the group leaders and the other participants. Recurring activities and predictability seemed to provide a stability that promoted a sense of security, reflected in the children’s frequent use of the expression ‘we use to’ when talking about the intervention: ‘After that, we use to go in to that room, we use to paint and draw, and we use to do [a certain task]’, ‘We use to sit on the red carpet’, ‘I use to have a get-together . . . I use to play here’. Some of the children seemed to have acquired a sense that this was a time and place where they could feel protected, relaxed and not alone. Within this space, they thought it possible not only to have fun and meet others, but also to listen and talk about distressing matters, such as the experienced violence. For some of the children, the treatment setting appeared to be a preferred condition, possibly in contrast to their everyday life: ‘I wanted to be here all day with mum, all, almost all night . . . then I would be here all day, not even go home’, ‘It is so pleasant to be here, to come here, other times it is not so pleasant, so I like most to be here a lot’.
The fragility of feeling safe was highlighted by some children’s distress at seemingly small incidents, such as a fight between two children, a group leader being more authoritative than usual or a change in the schedule of the group meetings: ‘I don’t like it when somebody fights me’, ‘I didn’t like . . . we threw things . . . it was fun when they started . . . but then I didn’t like it’. Referring to the group meeting once being rescheduled to a different weekday, one child said: ‘That day I thought it was pretty sad that I could not be here . . . sad, all of my body felt sad’.
Relatedness – relationships within the group
The majority of the children gave substantial descriptions of the importance of relationships within the group. The theme of relatedness contains two sub-themes: peer relationships and relating to the group leaders as significant adults.
Relationships with other children in the group were described as an important and joyful part of coming to the intervention: ‘It’s fun to play with my friends’, ‘It’s fun to play house with X’. Some of the children explicitly reported thinking of the other children when not seeing them: ‘I think only about the other children . . . about my friends who are here . . . when I am home and lie in my bed’, ‘I think about the other ones: ‘where is X now?’’, ‘I’m thinking about buying a walkie-talkie and we will talk to each other’. One girl expressed sadly how she felt when she could not participate on one occasion: ‘I think that they are not able to play with me . . . and feel that they cannot play with me . . . even though I want to’.
The relationships with the group leaders seemed to be of great importance to some children, while more neutral to others, and not mentioned at all by some. Most children described the group leaders as being well intentioned and as taking responsibility for the structure and the process: ‘They show things we are going to do . . . they are only good’, ‘We do as they say’, ‘They said when we should gather, and when we should finish’. Some children expressed an experience of the adults as important because of the relationships that had evolved: ‘I want to hug them before I leave . . . it feels pleasant in my body’. Two children expressed explicitly that they experienced a special and unique relationship with a specific group leader; one child explained that ‘I have met X more times’ and drew a picture of himself and the specific group leader holding hands. Another child reported that she had told certain things only when she had met one of the group leaders alone before the group intervention started, and that her relationship with this specific person was therefore different from that with the others.
To talk – externalised focus on the violence
To talk or not to talk, together with to be listened to and to listen to others, was a recurrent theme when the children spoke about their experiences in the programmes. Although the children seldom mentioned the concrete trauma-focused activities that were part of the interventions, the core of the theme is the focus on trauma and on talking about violence experienced by those in the group. This theme includes more variation and contradiction than the other themes. Children expressed ambivalent experiences of the act of talking and listening, and positive feelings of being relaxed, as well as the risk of being overwhelmed by trauma reactions: ‘In the group you talk . . . what happened . . . that dad does something bad . . . it is so-so’, ‘It feels bad to talk about it’, ‘Yes, maybe you tell what, what . . . you tell it to them, and why you come there . . . you get peace and quiet . . . so that they know’. For some children, the trauma-focused talking and listening seems to have led to an experience of a more general experience of being able to talk and share events and emotions, and of being listened to: ‘We talk about how we feel in the whole body, angry or happy or something . . . it’s sort of fun’.
Some children struggled to understand where and to whom to talk about what:
We have talked, first when only X and I were here [during intake], we talked about what it was about, about safety . . . what he has done; he hit us. No, no we don’t talk about such things there [in the group], there you can’t do that, it is only here . . . it feels bad to talk about it. ‘No, you don’t talk about that [being angry about somebody fighting] here, you talk about that at home’.
One child clearly expressed the difference of feeling understood or not:
It feels bad to talk about it . . . because, because nobody understands what I’m saying . . . when I was at, when I was at the police, there, I, I talked about what happened and then, but she did not understand what I said.
In the group, this boy sensed that everybody understood what he said and described that: ‘because I speak slowly, when I was at the police I spoke too fast . . . and [group leaders] they listen, they don’t talk’. He explained further: ‘In the group it does not feel bad, because, they have blocks, toys, and there you can meet other children’.
Competence – new knowledge and skills
Some children described that they gained new competence through participating in the programme. This theme encompasses the experience of obtaining new knowledge as well as new skills.
New knowledge that was mentioned mainly concerned violence and safety – for example, knowing that violence is not acceptable and knowing what to do if violence occurs. One girl spontaneously explained that she had learned what one should do if a father hit a mother: ‘You should call the police, or tell the mum to call the police, and you should lock the door, or tell the mum to lock the door’. Another child stated: ‘It really helps to know that you’re not allowed to hit people’.
One child spoke about new competence in emotional and physical regulation reached through skills in relaxation: We do, we do a relaxation. It is like, you do a jellyfish, you lay down, and then you relax and you are a jellyfish, first you are a fishbone and become tense [shows] . . . and then you, you calm down, then you’re calm, then you are the jellyfish, and then you feel: ah! It’s really easy, a piece of cake! Look [shows]!
Discussion
The present study aimed at elucidating young children’s experiences of participating in group treatment for children exposed to IPV. The children perceived treatment as a safe place to have fun and meet others, a place where they can talk about distressing matters and gain new abilities. The three most salient themes emerging from the interviews – joy, security and relatedness – refer to aspects of treatment that are not specific to the intervention programmes in this study. These aspects can be seen as curative components of treatment in their own right, as well as conditions that permit the children to benefit from specific interventions or techniques, such as trauma-focused components and the introduction of new skills and knowledge. It was evident that the children experienced these non-specific aspects as, in fact, constituting the intervention, and expressed more appreciation of them than of the trauma-specific content.
The result that all children expressed positive experiences of participating in the group treatment was striking. The experience of joy was strongly anchored in all interviews, in contrast with previous studies describing some children having negative experiences of treatment (Buston, 2002; Carlberg et al., 2009; Midgley et al., 2006; Paul et al., 2000; Stith et al., 1996; Strickland-Clark et al., 2000). In this study, none of the children expressed not wanting to attend or feeling psychologically insufficient or alienated in relation to their peers. Some children said that they disliked specific activities or moments in treatment but the same children expressed an overall positive experience. However, none of the studies reporting children disliking treatment included children taking part in group-based intervention: These studies examined individual or family-based treatment. It is possible that the group format offers a setting that normalises experiences and reactions, as well as participation in treatment, and furthermore, prevents alienation in relation to peers and offers training of skills in social interaction (Metel & Barnes, 2011).
Children’s descriptions of positive playing together with peers contrast with frequent descriptions of how children exposed to IPV develop severe disturbances in their ability to form positive relationships with peers (Levendosky, Huth-Bocks and Semel, 2002; McCloskey & Stuewig, 2001). Both intervention programmes in this study had taken precautions to avoid destructive interaction between the children by having a fairly small number of children (4–6) and two experienced group leaders in each group. The setting made it possible for the group leaders to support and guide relationships between the children, thus enabling positive experiences in activities as well as in interaction.
In light of the previous experience of violence and danger and the enhanced risk of insecure and disorganised attachment (Zeanah et al., 1999), these children can be expected to have specific needs when it comes to feeling safe and secure. The combination of a safe place protected from violence and predictable relationships with trustable adults was clearly appreciated by the children in this study. Furthermore, these new experiences may contribute to a process of change in working models and inner representations affecting expectations and behaviour. The possibility of experiencing joy and security in real-life relationships can be seen as a new and potentially curative experience (Fonagy, Gergely, Jurist, & Target, 2002; Schore & Schore, 2008; Sroufe, 2005; Zeanah, Berlin, & Boris, 2011). The sensation of security – not being afraid – further enables relaxation and thereby lessens emotional arousal. The improved capacity to regulate emotions enhances the possibility to benefit from trauma-focused interventions and to gain new skills and knowledge (Corrigan, Fisher, & Nutt, 2011; Ogden, Minton, & Pain, 2006; Schore & Schore, 2008).
The children’s appreciation of a secure place shed light on the notion that other places in their lives may not have been secure. Treatment offers an idea that things can be different, but the secure space offered in treatment is time-limited in terms of each session and the span of treatment. For children to recover from the experience of IPV and its aftermath and gain healthy development, safety has to be available in their everyday life (Broberg et al., 2011). A central task in interventions for children exposed to IPV will be to constitute and maintain a secure space in treatment, and at the same time help parents to protect their children and themselves, and be the protective shield that their child needs in life (Lieberman & Van Horn, 2005).
Young children as informants
This study supports the viewpoint that children as young as 4 to 6 years are able to contribute to research with valuable information that augments current knowledge of how they experience being in treatment (Hershkowitz et al., 2012; Lamb et al., 2003). The results emphasise the importance and relevance of acknowledging even very young children as competent and able subjects in research in issues that concern them, in accordance with the UN’s Convention on the Rights of the Child. However, questions about the reliability of children must be deliberated. These questions include the developmental implications on memory and reflective capacity; the possibility that highly stressed children have difficulty in information retrieval; and methodological considerations on the imbalance in power between adults and children, and on children’s possible wish to please the interviewer or to do what they think is expected of them. The results indicate that a developmentally sensitive approach – including enabling children to establish rapport and practice being interviewed, conducting open interviews, focusing on concrete issues, using cued invitations and seeing children’s consent as an ongoing process – can promote and augment the possibility for young children to contribute substantially with their experiences and opinions.
Clinical implications
It may be that the experience of joy should be valued as an important component in treatment for children with experience of IPV. To promote joy and well-being could be seen as a significant part of the work done by providers of IPV-interventions to facilitate children’s participation and possibility to benefit from the treatments offered. Furthermore, the results indicate the essential role of security, which may imply a responsibility of professionals to enhance and maintain the feeling of security in activities and interactions during treatment. Establishing the treatment setting as a safe place suggests a focus on issues concurrent with traditional child psychotherapy, such as predictability when it comes to the physical environment, the group leaders and the structure of sessions, including the use of ritualised activities and play. Finally, group interventions may provide a potentially unique curative setting for children at risk of developing difficulties in peer relationships.
The above implications carry influence in designing treatment interventions and considering what treatment to offer to a specific child. Specific considerations such as which and how many children to include in group treatment will be of importance in achieving conditions that allow group leaders to promote benign interactive processes and maintain security throughout treatment. In most cases, these considerations will speak in favour of a small group size with a narrow age span.
Limitations and need for further research
The objective of this study was to explore how the children interviewed experienced the specific treatments they had taken part in. However, the research design does not admit generalisation to other groups or settings. Further research can reveal if the themes found are specific to these children or are shared with others. Related areas would be research on the experiences of young children exposed to IPV in individual or dyadic treatment, and the experiences of older children or of children with different areas of difficulties in group treatment.
The quality of the interviews must also be considered. The location, the time of day, the interviewer’s ability and the interviewer’s concern for the children’s vulnerability and well-being are all factors that may impact the content of the interviews. Furthermore, limitations can be attributed to the fact that children participate and contribute according to their age and developmental stage, or may have specific difficulties expressing their experiences as a consequence of their symptoms and difficulties. Whilst the view of the child is important, it is also limited, and the descriptions from parents or group leaders may be different.
There is a need for clinically based studies to be carried out and to take into account the perspectives of young children. An important strength of this study was that it was performed in a naturalistic setting and that children were given a developmentally informed opportunity to express their experiences.
Conclusion
The interviewed children described treatment as a safe place to have fun and meet others, offering an opportunity to talk about distressing matters and to gain new abilities. These are general needs of young children, needs that may be insufficiently met among children exposed to IPV, a situation that often leads to symptoms. Consequently, these children appreciate and benefit from a context that meets their needs in the areas where they have difficulties. The study further highlighted the benefit of listening to children; the importance of not being overly focused on specific components of treatment, but primarily on issues of genuine and positive relationships, security and joy; and the need to consider these important non-specific areas in psychological treatment when choosing or evaluating treatment methods.
Footnotes
Acknowledgements
We would like to thank Bojen in Gothenburg and the Child and Adolescents Psychiatry Trauma Unit in Stockholm for their collaboration on this study. We would also like to thank all participating children and their caregivers for their contributions.
Funding
The study was funded by the County Council of Kronoberg and the County Council of Värmland.