
Abstract
Objectives:
Behavioral sleep problems affect 25% of children and impact functioning, but little is known about help-seeking for these problems. We identified (1) predictors for sleep problem perception and help-seeking, using nested-logit regression and (2) reasons why parents did not seek professional help for sleep problems, using chi-square.
Methods:
Parents (N = 407) of children (2–10-years-old) completed the study online. Parents indicated whether their child had no sleep problem, a mild problem, or a moderate-to-severe problem and completed additional questionnaires on parent/child functioning.
Results:
Overall, 5.4% ± 2.2% of parents sought professional help for a child sleep problem. Greater child sleep problem severity and greater child socioemotional problems were significant predictors of parents perceiving a sleep problem. Among parents who perceived a sleep problem, greater parental socioemotional problems significantly predicted professional help-seeking. Parents who perceived no problem or a mild sleep problem reported not needing professional help as the main reason for not seeking help; parents who perceived a moderate-to-severe problem reported logistic barriers most often (e.g. treatment unavailability, cost).
Conclusions:
Problem perception and help-seeking predictors resemble the children’s mental health literature. Differences in barriers, based on problem severity, suggest differential help-seeking interventions are needed (e.g. education vs access).
Behavioral sleep problems affect approximately 25% of children 2–10 years old and include problems going to sleep (bedtime resistance and delayed sleep onset) and staying asleep (night- and early-morning wakening; Simola et al., 2011). Children can experience behavior, language, and learning difficulties (Quach et al., 2009). Behavioral interventions for these sleep problems are efficacious, but the screening and management for these problems are low, contributing to fewer families utilizing these interventions (Blunden et al., 2004; Honaker & Meltzer, 2016; Meltzer & Mindell, 2014). Despite their prevalence and impacts, little is known about help-seeking mechanisms for these problems. This study examined: (1) socio-behavioral and cognitive predictors of parental perception of and help-seeking for sleep problems and (2) reasons parents do not seek help.
Previous studies have examined correlates of parents’ sleep problem perception, locations for help-seeking, and service recommendations (Etherton et al., 2016; Johnson, 1991; Sadeh et al., 2011). Sadeh et al. (2011) reported parents’ sleep problem perception depended on parents’ culture (higher in predominantly Asian countries), problem symptoms, and demographic variables (e.g. lower education). Etherton and colleagues (2016) identified several reasons parents may struggle with behavioral sleep interventions, including practical considerations (e.g. sleep disruptions) and parental anxiety. These reasons may also impact help-seeking. Parental socioemotional problems have been related to lower rates of help-seeking for children’s psychosocial problems (Ryan et al., 2015). However, theoretical help-seeking models have not been applied to parents’ help-seeking decisions for sleep problems. This study addresses these limitations.
Without help-seeking models specific to children’s sleep problems, we expected help-seeking mechanisms to resemble models from children’s mental health, as both these problems involve parent-child interactional elements. The Revised Network Episode Model (Revised NEM; Costello et al., 1998) is a comprehensive model of help-seeking including child and parent sociodemographic characteristics, problem severity, comorbidities, parental socioemotional problems, and beliefs about the problem and its treatment. The Pathways to Care Model (applied to children by Pavuluri et al. (1996)) describes parents’ progression from problem recognition to help-seeking, and states parents must traverse “levels” to seek help: parents must recognize a problem, consider seeking help, and overcome logistic barriers. Therefore, we expected two steps of parent help-seeking behavior: problem perception and help-seeking.
Potential predictors of these two steps were informed by a systematic review of parental predictors of help-seeking for children’s psychosocial problems and the children’s sleep literature. Parental burden, problem perception, and socioemotional problems were consistent help-seeking predictors; whereas parent-child relationship quality, previous service use and sociodemographic characteristics were inconsistent predictors (Ryan et al., 2015). Individual studies have linked child problem severity, co-occurring problems, and beliefs about prospective service use to help-seeking (Ford et al., 2008; Oh & Bayer, 2017).
However, these models and predictors may underemphasize parental cognitions. More negative parental sleep-related cognitions (e.g. negative affect, lower sleep knowledge) are related to greater perception of children’s sleep problems, more problematic parenting responses, and maladaptive child sleep behaviors, whereas more positive sleep cognitions (e.g. positive thoughts about limit-setting, greater sleep knowledge) have been linked to better sleep practices, such as consistent wake-times (Coulombe & Reid, 2011; Morrell & Steele, 2003; Owens & Jones, 2011). Other authors argue parents’ beliefs about sleep problems and treatment may impact help-seeking (Bessey et al., 2013) Parents who believe sleep problems are unresponsive to treatment or non-modifiable may be less likely to seek help (Bessey et al., 2013). However, these theories have not been tested.
This is one of the first studies to investigate help-seeking for children’s sleep problems. Our examination is guided by help-seeking models and the sleep literature. Understanding the help-seeking processes involved with behavioral sleep problems may improve help-seeking.
Research questions and hypotheses
1.
Help-seeking was expected to follow the parent’s problem perception. Therefore, help-seeking prediction was evaluated in a two-step model: (1) predicting problem perception, and (2) predicting help-seeking among parents who perceived a problem. Predictions at both steps were expected to be driven by sleep problem severity and child/parent socioemotional problems.
2.
Parents who perceived a mild sleep problem were expected to endorse problem conceptualization reasons for not seeking help more often (e.g. belief the problem would get better on its own or professional help was not needed); whereas parents who perceive moderate-to-severe sleep problems were expected to endorse logistic barriers more often (e.g. treatment unavailable).
Method
Participants
Primary caregivers of 2–10-year-old children, responsible for the night-time care of their child participated (N = 407). Exclusion criteria were: (1) children with a parent-reported health condition or prescription which may negatively influence sleep (e.g. Attention Deficit Hyperactivity Disorder (ADHD), Autism, stimulant prescription); or (2) parents unable to read in English.
Procedure
Ethics approval was received from two research ethics boards. Parents from Canada, the United States, and Australia were recruited online using social media (e.g. Facebook), parenting blogs, and classifieds (e.g. Kijiji, Craigslist). See supplemental materials for the full recruitment strategy. Eligibility was determined using an online screening questionnaire. Parents provided their informed consent and completed questionnaires (described below). Participants were validated using email addresses and cross-referencing location data with postal/zip codes. Participants received a $10 CAD gift card. See supplemental materials for the participant flowchart.
Measures
Demographics
Parents provided their own (age, education, ethnicity, country, employment status, relationship to child, family income) and their child’s (age, sex, birth order) demographics; items were based on the Canadian Census, with adjustments for inter-country variation (e.g. ethnicity).
Sleep-related measures
Sleep problem severity
The Children Sleep Habits Questionnaire (CSHQ; Owens et al., 2000) measured sleep problem severity with 45-items. Parents responded on a 3-point Likert scale (0 = rarely (0-1 times/week), 1 = sometimes (2–4 times/week), 2 = usually (5–7 times/week)). The CSHQ demonstrated adequate reliabilities in this (αc = 0.83) and other samples (αc’s = 0.68–0.82, test-retest reliability r ⩾ 0.62, in community samples (Owens et al., 2000; Sneddon et al., 2013)) and has demonstrated adequate validity in preschool and school-age samples (Owens et al., 2000; Sneddon et al., 2013). The CSHQ total score was used as a continuous measure of sleep problem severity. Higher scores indicated more severe problems.
Parent perception of child’s sleep problem
Parents were asked if they perceived their child as having a sleep problem (problems following bedtime routines, falling asleep, or staying asleep), based on the final item of the Brief Infant Sleep Questionnaire (BISQ; Sadeh, 2004). Parents indicated whether their child had (1) no problem, (2) a mild problem, (3) a moderate problem, or (4) a severe problem. The BISQ correlates with other established sleep measures and has demonstrated good test-retest reliability (Sadeh, 2004). The single item shows discriminant validity. For example, children with “no problem” have fewer night-wakings than children with a “severe problem” (Sadeh, 2004). This single item has been used as an outcome measure (e.g. Teng et al., 2011).
Parent attitudes and beliefs about sleep
The Sleep Attitudes and Beliefs Scale (SABS; Bessey et al., 2013) is a 19-item questionnaire measuring parents’ beliefs about sleep. The SABS is relatively new. Therefore, its factor structure was evaluated using Confirmatory Factor Analysis (see supplemental materials). A five-factor solution demonstrated construct validity and was used for subsequent analyses (comparative fit index (CFI) = 0.93, and root mean square error of approximation (RMSEA) = 0.06). Factors were: (1) organic nature of sleep problem (e.g. “Childhood sleep problems are biological in nature”; three items); (2) behavioral nature of sleep problem (e.g. “Childhood sleep problems are behavioral in nature”; two items); (3) sleep modifiability (beliefs about the malleability of children’s sleep problems; e.g. “Parents are able to change children’s sleep habits”; five items); (4) responsiveness to treatment [beliefs about how well the problem would respond to treatment; e.g. “Treatments for sleep problems are not effective in children” (negatively-worded); five items); and (5) sleep impact (beliefs about how the sleep problem impacts functioning; e.g. “A child’s sleep problem can have a big impact on the whole family”; four items). These subscales demonstrated adequate internal consistency in the original psychometric evaluation (αc 0.79–0.84; Bessey et al., 2013) and in this sample (αc 0.70–0.86). Subscale scores were formed by averaging items, with higher scores indicating stronger beliefs.
General functioning
Parenting style
The Parenting Scale (Arnold et al., 1993) assesses parents’ responses to childrearing situations. This study used the laxness (11 items) and over-reactivity (10 items) subscales. Parents responded to situations (e.g. “When I give a fair threat or warning”) on a 7-point scale anchored with an effective parenting technique at one end (e.g. “I always do what I said”) and an ineffective technique at the other (e.g. “I often don’t carry it out”). These scores are consistent over time (2-week test-retest reliability = 0.84; Arnold et al., 1993). Internal consistency was strong in this sample (Laxness αc = 0.90; Over-reactivity αc = 0.82) and the original psychometric evaluation (Laxness αc = 0.83; Over-reactivity αc = 0.82; Arnold et al., 1993). This scale has demonstrated discriminant, convergent validity (Arnold et al., 1993) and content validity (CFI = 0.98, RMSEA = 0.03 for mothers; Rhoades & O’Leary, 2007). Each subscale score was averaged. Higher scores indicated more problematic parenting.
Parental socioemotional problems
The Depression, Anxiety, and Stress Scale – 21 (DASS-21; Henry & Crawford, 2005) is the 21-item short-form of the DASS. Parents reported on the extent to which statements (e.g. “I found it hard to wind down”) applied to them during the past month on a 4-point Likert scale from 0 (Did not apply to me at all) to 3 (Applied to me very much/most of the time). The total score shows convergent validity with other socioemotional measures (Henry & Crawford, 2005). Internal consistency was strong in this (αc = 0.88) and a previous sample (αc = 0.92; Henry & Crawford, 2005). The total score was used to measure parental socioemotional problems. Higher scores indicated greater problem severity.
Child socioemotional problems
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) is a 25-item questionnaire used to measure children’s socioemotional problems. Parents responded on a three-point Likert scale from 0 (not true) to 2 (certainly true). The total SDQ score is the sum of each of the four problems subscales (emotional, conduct, peer, hyperactivity/inattention). The SDQ has demonstrated construct, concurrent, and convergent validity (Stone et al., 2010) and adequate internal consistency in a review of 26 studies (αc = 0.80; Stone et al., 2010) and in this study (αc = 0.79). The total score indexed child socioemotional problems. Higher scores indicated greater problem severity.
Help-seeking behavior
Parents were asked: “In the past 6 months, did you talk to any professional for help with a child sleep problem?” Yes or No. Those who responded “yes” were classified as “help-seeking.” This question was based on a previous study (Reid et al., 2011).
Non-help-seeking parents reported the main reason they did not seek professional help from a list of options (parents could also write-in a response), based on previous children’s mental health help-seeking research (Pavuluri et al., 1996). These options were recoded into six categories: (1) “thought the problem was not that bad,” (2) “thought the problem would get better by itself,” (3) “thought we could manage it ourselves,” (4) “my child does not need professional help,” (5) believed professional could not help (i.e. “I didn’t think professional help would do any good”), and (6) logistic barriers (i.e. “I didn’t know where to get help,” “I never got around to it (e.g. too busy),” “It would have been too hard to schedule,” “I tried, but the wait was too long,” “It was going to cost too much,” “getting there was a problem,” “child refused to go”). The main reasons parents did not seek help were scored using frequencies.
Data analyses
Preliminary analyses and approach to missing data
The missing data in this study was minimal (0%–1.7%). As such, complete-case analysis was used. The help-seeking and perceived sleep problem frequencies were generated with 95% confidence intervals.
Which child, parent, and sleep related factors predict help-seeking?
Univariate relations between predictors and outcomes (i.e. perceiving a sleep problem and help-seeking) were assessed. Due to sample size constraints, only significant univariate predictors were included in the 2-step nested-logit model (Tabachnick & Fidell, 2001). The 2-step nested-logit was conducted in STATA 14 (StataCorp). Nested-logit regression is used to model hierarchically ordered behaviors. The first modeled behavior was problem perception. The second modeled behavior was professional help-seeking, among those who perceived a problem and controlling for Step 1. To increase meaningful interpretation, odds ratios (OR) for predictors scored as averages on Likert scales (i.e. SABS subscales, laxness, and over-reactivity) are reported per 1-unit change. Predictors using sums (i.e. CSHQ, SDQ, DASS-21) were recoded into half standard deviation units.
Why do some parents choose not to seek help?
Descriptive statistics and chi-square analyses were used to examine differences in the main reason professional help was not sought by perceived sleep problem severity. Then, post-hoc comparisons were made between perceived problem severity groups using standardized residuals, which are interpreted like z-scores (Sharpe, 2015). The False Discovery Rate (FDR) was used to adjust for multiple comparisons.
Results
Preliminary analyses
Table 1 presents the parent and child demographic characteristics.
Parent, child, and family demographic characteristics.

Note. N = 407.
Income remained in the currency of the participant’s country (i.e. Canadian, Australian, or US Dollars).
Help-seeking status
Twenty-two parents (5.4% ± 2.2%) reported seeking professional help for a child sleep problem during the past 6 months.
Which child, parent, and sleep related factors predict help-seeking?
Overall, 171 (42.0% ± 4.8%) parents perceived their child to have a sleep problem (29.0% mild; 10.5% moderate, 2.5% severe). Of these, 19 (11.1% ± 4.7%) sought help. 1 In the nested-logit, both Step 1 (problem perception; Likelihood Ratio χ2 (12) = 186.64, p < 0.001, Pseudo-R2 = 0.34) and Step 2 (help-seeking among those who perceived a problem; Likelihood Ratio χ2 (11) = 20.70, p = 0.037, Pseudo-R2 = 0.18) were statistically significant (Table 2). At Step 1, each half-standard deviation increase in sleep problem severity predicted a 2.69-times increase in the likelihood of problem perception (OR = 2.69, 95% CI = 2.15–3.38). Further, each half-standard deviation increase in child socioemotional problems predicted a 1.27-times increase in the likelihood of problem perception (OR = 1.27, 95% CI = 1.06–1.52). At Step 2, each half-standard deviation increase in parental socioemotional problems predicted a 1.40-times increase in the likelihood parents who perceived a sleep problem would seek professional help (OR = 1.40, 95% CI = 1.00–1.97).
Nested logit model predicting perceived sleep problem and help-seeking. .

Note. * indicates significant at p < .05; ** indicates significant at p < .01.
Odds Ratio represents increased odds per ½ SD units on the CHSQ (Children’s Sleep Habits Questionnaire), SDQ (Strengths and Difficulties Questionnaire), or DASS-21 (Depression, Anxiety Stress Scale – 21 Item Version).
Odds Ratio represents increased odds per 1 unit.
Reference group is “Undergraduate degree.”
Why do some parents choose not to seek help?
The main reasons parents did not seek help were compared across problem perception severity: no perceived problem, mild problem, and moderate-to-severe problem (Table 3). As expected, parents who did not perceive a problem most frequently endorsed that their child did not need professional help (83.7%) as the main reason professional help was not sought. Others endorsed other cognitive reasons (e.g. Thought the problem would get better by itself) or logistic barriers.
Main reasons parents did not seek help by perceived problem severity and standardized residuals.
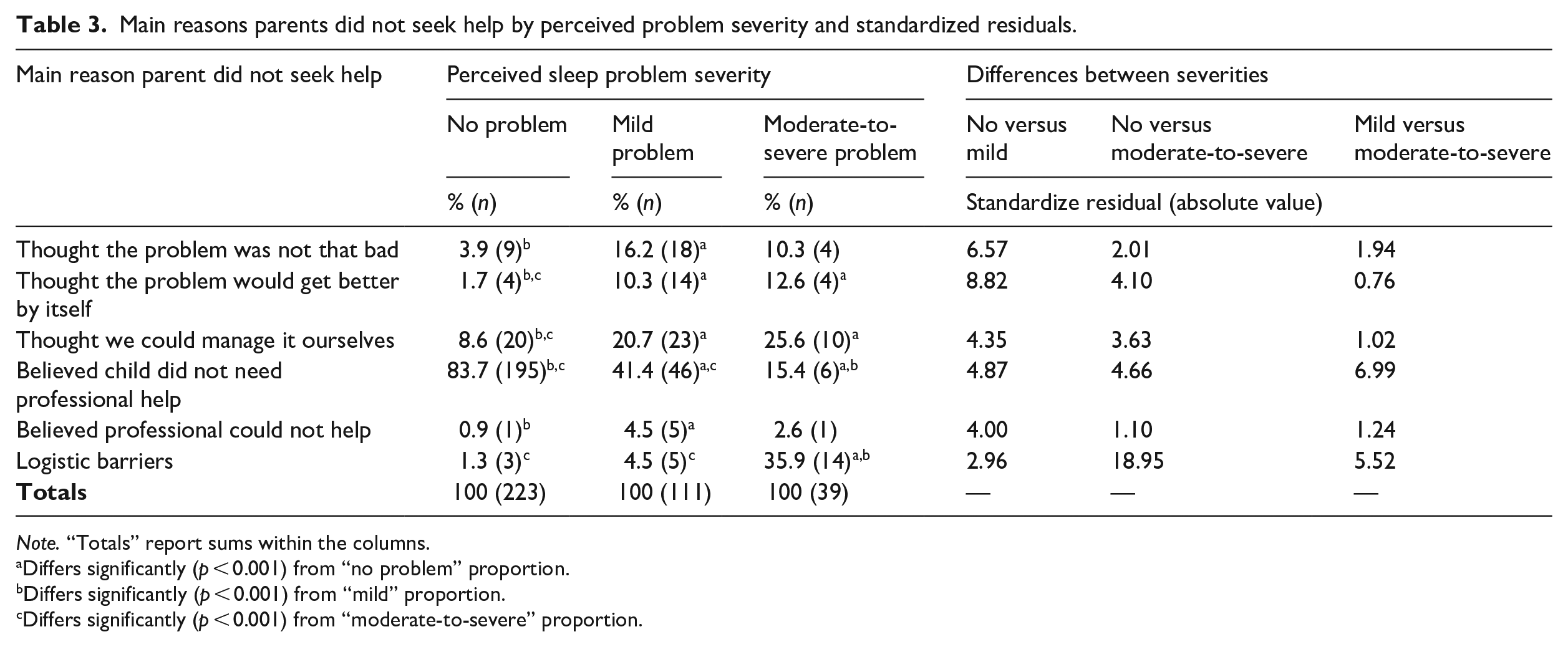
Note. “Totals” report sums within the columns.
Differs significantly (p < 0.001) from “no problem” proportion.
Differs significantly (p < 0.001) from “mild” proportion.
Differs significantly (p < 0.001) from “moderate-to-severe” proportion.
Small proportions of parents who perceived a mild problem reported specific problem conceptualization reasons for not seeking help (Figure 1). The most frequently endorsed reason help was not sought was the belief the child did not need professional help (41.4%).
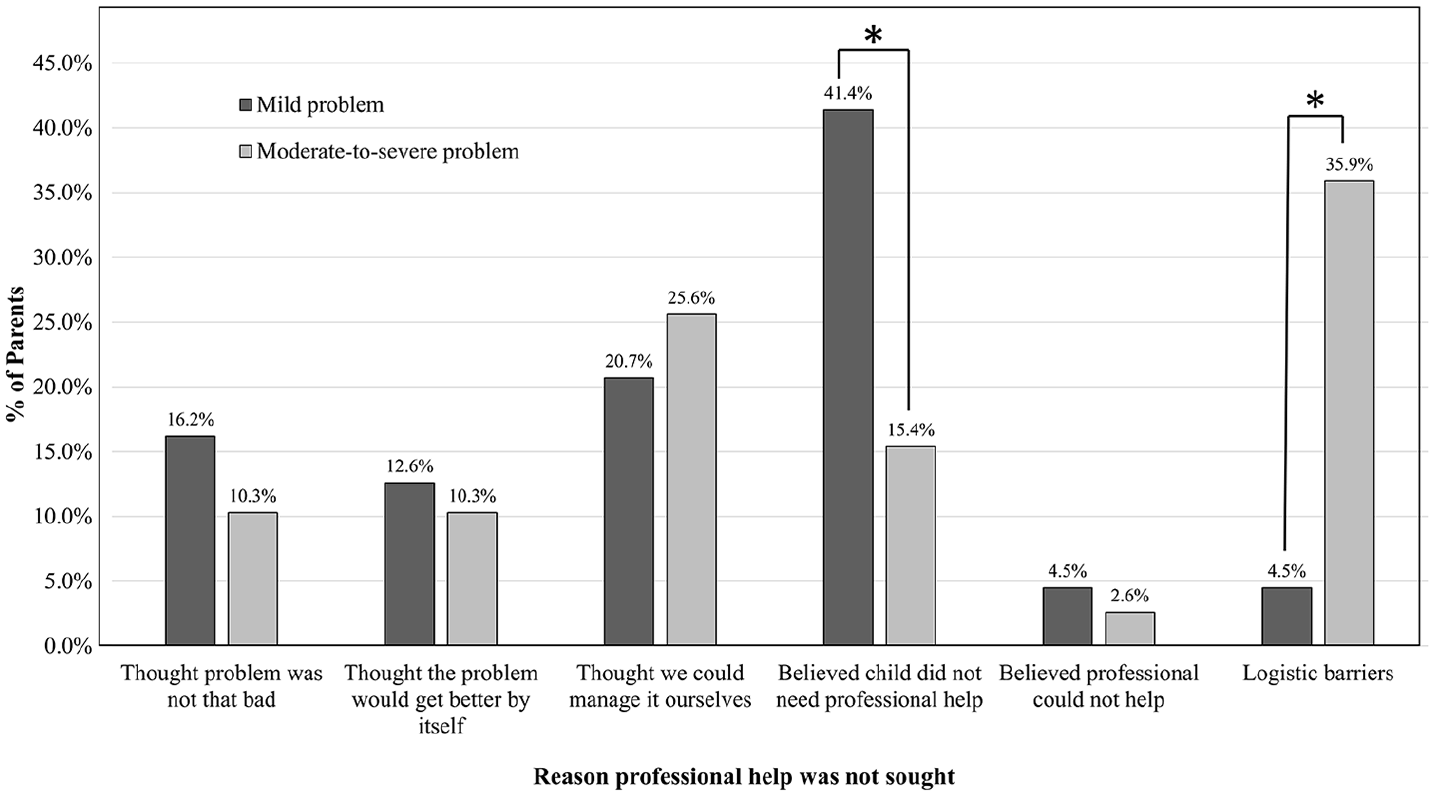
Comparing the main reason help was not sought among parents who perceived a mild or moderate-to-severe sleep problem.
Parents who perceived a moderate-to-severe problem endorsed specific problem conceptualization reasons at similar rates to parents who perceived a mild problem. Fewer of these parents believed the child did not need professional help (15.4%; Standardized Residual = −6.99, p < 0.001) than parents who perceived a mild problem. The most common reason (35.9%) these parents gave for not seeking help was logistic barriers (e.g. too costly, treatment unavailable), which was higher than those who perceived a mild problem (4.5%, Standardized Residual = 5.52, p < 0.001).
Discussion
This study identified predictors of sleep problem perception and help-seeking and reasons why parents may not seek help.
Problem perception and help-seeking predictors
Overall, 42% (± 4.8%) of parents perceived their child to have at least a mild sleep problem; however, few of these parents (11.1% ± 4.7%) sought professional help. The rate of problem perception was higher than previous studies. Sadeh and colleagues (2011) found parents reporting at least a mild sleep problem was 25%–32% for parents in the United States, Canada, and Australia. Other studies using the BISQ found rates ranging from 25%-to-31% (Sadeh et al., 2009; Teng et al., 2011).
The professional help-seeking rate was similar to studies investigating sleep problem help-seeking in primary care. Blunden and colleagues (2004) reported that 13.9% of parents of children with a clinically significant sleep problem discussed the sleep issue with their primary care provider. Secondly, Meltzer and colleagues (2014) reported that 5.2% of 0-to-18-year-old children with a sleep problem attending primary care received a sleep-related treatment recommendation (Meltzer et al., 2014).
This rate can also be compared to community help-seeking rates for children’s psychosocial problems (Georgiades et al., 2019). In a representative sample of children 4–17-years-old, Georgiades and colleagues (2019) reported about 35% of children with psychosocial problems sought help from a primary care provider. In a review, the rate of help-seeking for mental health problems ranged from 6% to 16% among children in the general population (Ford, 2008). Our frequency appears lower than what is reported in children’s mental health. Epidemiological studies are required to establish the population prevalence of help-seeking for sleep problems.
Parental socioemotional problems were a consistent predictor of help-seeking in our study and in a review of help-seeking predictors for child psychosocial problems (Ryan et al., 2015). Others have reported increased problem severity and concurrent problems as predictors of problem perception and help-seeking, as we found (Pavuluri et al., 1996; Wichstrom et al., 2014). Many help-seeking studies identify parents’ problem perception as a key help-seeking predictor but do not disentangle these steps (e.g. Ryan et al., 2015). In contrast, this study provided a two-step model of help-seeking behavior to identify differential problem perception and help-seeking predictors.
This approach assumes perception must precede help-seeking. However, a parent could seek help without perceiving a problem (e.g. spouse perceives a problem and seeks help). Unlike children’s mental health problems; it is unlikely individuals other than the parents themselves (e.g. teachers) would see a child is having a sleep problem and suggest professional help.
Reasons for not seeking help
The specific reasons for not seeking help differed by perceived sleep problem severity. These reasons can be conceptualized using the Pathway’s to Care Model (Pavuluri et al., 1996; see supplemental materials for a visual representation). Theoretically, a parent would need to transverse all levels to receive help:
Problem perception. If the parent does not perceive the child to have a sleep problem, help-seeking is unlikely.
Problem conceptualization. Parents may believe the problem will resolve on its own or that it can be managed by the parent. This level was frequently endorsed by parents who perceived at least mild problems in our study and parents who did not seek help for psychosocial problems (Pavuluri et al., 1996).
Perceived need for professional help. In this study, parents who endorsed this cognition acknowledged a problem, but felt it did not warrant professional attention. This cognition was endorsed more frequently by parents who perceived a mild problem than parents who perceived a moderate-to-severe problem.
Perceived efficacy of professional help (belief a professional could not help the problem). In this study, this cognition was rarely endorsed whereas in the Pavuluri et al. (1996) study, this cognition was endorsed by one-third of parents. Parents in our study generally had strong beliefs that sleep problems were modifiable and responsive to treatment. For psychosocial problems, parents may believe their problem is too interwoven with other problems to be addressed by professional interventions (Anderson et al., 2006). This cognition may be more relevant when investigating help-seeking behaviors among children with comorbid problems (e.g. ADHD).
Logistic barriers. Once a parent has traversed the previous levels, the parent may fully intend to seek help. However, logistic barriers (e.g. cost, availability) may impede help-seeking. Logistic barriers were the most frequently endorsed reason among parents who perceived a moderate-to-severe sleep problem. Logistic barriers may be particularly impactful for lower income families (Anderson et al., 2006).
Limitations
Help-seeking behavior was reported for the previous 6 months and other variables were reported at the time of the study, which is the standard approach when examining service use (e.g. Boyle et al., 2019). A prospective study would be needed to examine predictors of subsequent help-seeking. This study did not utilize objective measures of child sleep (e.g. actigraphy). Objective ratings of children’s sleep problems are more relevant for other research questions (e.g. sleep duration and cognitive performance). Participants were self-selecting. As such, parents who were screened and did not start or complete the survey may differ from those who completed. These non-completing parents may have less free time or greater parental burden. The consent process described the study as being about children’s sleep problems. Some parents who did not perceive their child to have a sleep problem may not have completed the survey, which may have contributed to our higher problem perception rate. Finally, most participants were white and had slightly higher socioeconomic status (SES) than the general population. Our recruitment strategy and/or Facebook’s advertisement algorithm may have influenced our sample (Lane et al., 2015). Predictors and help-seeking barriers may differ by ethnicity and SES. These differences should be tested in future studies.
Future directions
Problem perception pathways from informal (e.g. internet) to formal (e.g. family doctor) should be investigated using a longitudinal design. Secondly, given the difficulties in accessing care, we must maximize parents’ engagement in interventions once they start. Previous sleep research has addressed engagement barriers (Honaker et al., 2018). The findings from children’s psychosocial treatment can supplement this work (Becker et al., 2018). Thirdly, there may be distinct rates, patterns, and predictors of seeking help from an informal/informational source (e.g. friend or website) versus a professional source (e.g. family doctor), between different types of professionals (e.g. physician vs psychologist), for different sleep problems (e.g. sleep apnea, enuresis), and for children with comorbidities (e.g. Autism, ADHD). This research may require a retrospective sample of treatment-seeking families for adequate power. Fourthly, differential reasons for not seeking help may have distinct intervention implications. Parents who perceive logistic barriers may benefit from distance-based interventions; whereas parents who have adopted a “wait and see” approach may benefit from sleep education. Finally, more rigorous sampling techniques are needed, like stratified random sampling (to examine difference by SES and ethnicity) and geographical information systems (GIS) data to examine regional contributions to problem recognition and help-seeking.
Implications
Our results provide key implications for help-seeking theory, parents, and providers. Firstly, the results of this study support the application of the Pathways to Care Model (Pavuluri et al., 1996) and the Revised NEM (Costello et al., 1998) to help-seeking for behavioral sleep problems. Both models identify the importance of problem perception, prior to help-seeking. There may be a linear sequence of reasons parents endorse for not seeking help (i.e. Pathways to Care Model); and similar predictors were observed as would be expected, given the Revised NEM. Parents may benefit from education on normative sleep and help-seeking. Parents may be encouraged to seek support before sleep problems become overwhelming or before parental burden increases. Primary care providers and parents may benefit from education or direction on how and when to inquire about children’s sleep. Our prediction results may be applied to individual families to forecast which parents may seek help.
Supplemental Material
SUPPL-FiguresTablesCFA-REVISED.2020.06.29 – Supplemental material for Influences on help-seeking decisions for behavioral child sleep problems: Why parents do and do not seek help
Supplemental material, SUPPL-FiguresTablesCFA-REVISED.2020.06.29 for Influences on help-seeking decisions for behavioral child sleep problems: Why parents do and do not seek help by Adam T Newton, Penny V Corkum, Sarah Blunden and Graham J Reid in Clinical Child Psychology and Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Dalhousie Psychiatry Research Fund. AN received support from the Social Science and Humanities Research Council (SSHRC), the Ontario Graduate Scholarship, and the Better Nights, Better Days Training Program (funded through the Canadian Institute for Health Research). GR is supported by the Children’s Health Research Institute.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.