
Abstract
Background
European countries face the challenge of promoting refugee and immigrant children’s well-being within their host communities, invoking the necessity of adequate mental health assessment. This study aims to contribute to document the psychosocial well-being of primary school refugee and non-refugee immigrant children in Flanders, Belgium.
Method
A total of 120 children (8–12 years old) with migration backgrounds participated in the study. Through self-report, parent and teacher questionnaires we scrutinized externalizing and internalizing behavioral problems, post-traumatic stress problems, and classroom relationships.
Results
Thirty percent of the participants reported high levels of post-traumatic stress; around 25% reported a high or very high prevalence of internalizing and externalizing behavioral problems. Self-reported mental health problems are elevated in comparison to the general population. Refugee children did not report more difficulties than their immigrant peers. In the perception of parents and teachers, respectively 20% and 5% of children showed high or very high amounts of internalizing and externalizing behavioral difficulties. Almost 70% of the participants perceived the class climate as unsafe.
Conclusions
Refugee and immigrant children are at risk for mental health difficulties, and experience classroom dynamics as markedly distressful. School-based intervention might be particularly suited to support these children’s psychosocial well-being in resettlement.
Introduction
European societies face the challenge of promoting refugee and non-refugee immigrant children’s adaptation within their host communities. Indeed, studies document how migration histories and resettlement conditions render these children at an increased risk for mental health difficulties. For refugee children, pre-migratory stressors of collective violence as well as flight-related stressors of family separation and deprivation are compounded by post-flight stressors of cultural change, residence insecurity, isolation and experiences of discrimination (Spaas et al., 2022). These cumulative stressors may also impact affective security within refugee family relationships and invoke family conflict and decreased parental availability (De Haene et al., 2010b). Studies indicate how refugee children’s mental health may be at-risk in the face of this cumulation of disruptive life-experiences and document high prevalence of post-traumatic stress disorder (PTSD), depression, and internalizing and externalizing problems (e.g., Hodes & Vostanis, 2019).
For non-refugee immigrant children (referred to as immigrant children in what follows), studies consistently show that migration status is associated to at-risk mental health functioning, particular internalizing problems (for review, see Kouider et al., 2014). Although resettlement stressors of acculturation, discrimination, or deprivation are contextual factors immigrant children share with refugee children, it remains unclear whether immigrant children’s increased mental health vulnerability shows analogous profiles as compared to refugee children. Here, the paucity of evidence is equivocal: while a US-based study by Betancourt et al. (2017) documented higher levels of trauma exposure and post-trauma symptoms in refugee than in immigrant children, another US study showed high levels of trauma exposure (including domestic and community violence) in recent (non-refugee) immigrant children (Jaycox et al., 2002).
With studies indicating psychosocial vulnerability in refugee and immigrant children, it seems relevant to explore mental health profiles in both groups in which migration histories may comprise of shared and non-shared stressors. In exploring mental health profiles in both groups, an exploration of school-based social relationships as complementary outcome variable seems relevant. Studies demonstrate the role of school-related variables (e.g., positive peer and teacher relations, school belonging) in determining young refugees’ and immigrants’ mental health. For refugee children, positive peer and teacher-pupil relationships are associated with improved psychological functioning, being important sources of support in coping with distress and social exclusion or discrimination (Fazel, 2015). School-related factors like school belonging and sense of safety at school have been found to protect against psychiatric disorders such as PTSD, depression and anxiety (e.g., Due et al., 2016). Similarly, for immigrant children, studies highlight the detrimental impact of exclusion and discrimination, and document the protective role of positive peer relationships and sense of belonging in the school context (Gharaei et al., 2019). These findings in both refugee and immigrant children indicate how school-based social relationships may operate as both a buffer against the psychological sequelae of migration-related stressors or as risk factor for mental health problems. Therefore, assessing mental health profiles in the context of school and including an exploration of their sense of belonging and safety in the classroom peer context seems relevant.
In this study, we aim to investigate mental health profiles in refugee and immigrant children in the primary school context, including an exploratory assessment of class well-being and social relationships. As existing studies for the Belgian context have focused on adolescent refugees and immigrants (e.g., Derluyn et al., 2008; Vervliet et al., 2014), this study provides a first systematic assessment of mental health in primary school-aged refugee and immigrant children.
Methodology
Study setting and participants
This study is part of a larger research project on the impact of a creative arts-based expression program (Rousseau et al., 2004) on refugee children’s mental health and peer relationships. The study reports on the baseline assessment of mental health problems and classroom relationships.
Purposive recruitment of schools was conducted in 2017–2018 in the Flemish community of Belgium. Targeting schools with a high number of refugee and immigrant pupils, 30 schools were contacted through the Agency of Educational Services (AGODI); three schools were selected, based on their multi-ethnic composition and presence of refugee pupils, interest in study participation, expected pupil drop-out rates (e.g., asylum decisions), and geographical location. The schools were located in one Flemish multi-ethnic city, which increased homogeneity in participants’ social environment and ensured accessibility for data collection and intervention implementation. Pupils in the third to sixth grade (aged 8–12) were eligible for participation, in line with the target group of the intervention under study and the skills needed to complete self-report questionnaires.
Children were included in the study when their parents provided active informed consent: following a collective information session including visual and interpreter support, parents received oral and written information about the study and could sign consent. Through close collaboration with school teams, we engaged in an intensive process of outreach to parents, for example, addressing them at parent-teacher meetings or at the school gate. Out of the 274 children approached for participation, parental informed consent was obtained for 120 of them. This 44% response rate mirrors the complexities of access and alliance-building in research with refugee communities (De Haene et al., 2010a; de Smet et al., 2020).
Following informed consent, parents completed standardized questionnaires on background characteristics (e.g., child gender, child age, children’s and parents’ country of origin, time in Belgium, parental education, legal status). Based on these background characteristics, participants were categorized as refugee children or immigrant children. Life-trajectories of forced displacement induced by persecution, war, or violence were a precondition to be categorized as refugees. The country of origin (e.g., Syria, Afghanistan) and legal status (e.g., refugee, asylum seeker) informed the categorization as refugees, in unclear cases complemented by an oral exploration with parents. Fifty-five participants were categorized as refugee children, 62 as immigrant children, and for three participants information that would allow categorization was lacking.
Demographic characteristics (%) of the participants.

a‘Other’ includes legal statuses not specified otherwise (e.g., a European work permit, residence permit without further specification).
Chi-Square tests of independence regarding demographic characteristics indicated a significant difference in terms of maternal education, with more mothers of refugee pupils having received no schooling (χ2(2) = 20.88; p < .001). In addition, there were significant differences between on migration-related variables, as could be expected: refugee and immigrant participants differed from each other in terms of legal status (χ2(5) = 70.24; p = .002); time in Belgium (χ2(3) = 15.41; p = .002); and country of birth (χ2(30) = 98.11; p = .001).
Measures and procedures
Strengths and difficulties questionnaire
The SDQ is a 25-item measure of emotional and behavioral problems in children (Goodman et al., 2000), with extensive application in culturally diverse study settings (including translations in over 40 languages) (Bourdon et al., 2005; Goodman, 2001). Five small subscales (emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behavior); two broader subscales (externalizing and internalizing problems); and a total difficulties score can be computed. The self-report version is intended for use with 11- to 16-year-olds, yet has also been validated with younger children (Curvis et al., 2014). In our study we invited children, their parents and teachers to complete the SDQ. Except for the self-reported internalizing problems (α = .54), all three informants’ total difficulties scores, externalizing and internalizing subscale scores showed satisfactory to good internal consistency (α > .60; Taber, 2018). Several of the smaller subscales of the SDQ had Cronbach’s alphas below .60 and were not further studied, although the use of these smaller subscales is generally more recommended in high-risk samples (Goodman et al., 2010).
Youth self report – post-traumatic stress problems scale
The Youth Self Report (YSR) is part of the Achenbach System of Empirically Based Assessment (ASEBA). The ASEBA forms have been translated in over 100 languages (Achenbach & Rescorla, 2007). The YSR was developed for use with 11- to 18-year-olds, yet YSR scores for younger children (ages 7–10) show good psychometric properties (Ebesutani et al., 2011). In this study, only the 14 items of the post-traumatic stress problems scale of the Youth Self Report (PTSP; Achenbach & Rescorla, 2001; 2007) were included in the children’s self-report questionnaires. These items assess a broad range of post-trauma symptoms and trauma-specific behavioral problems, and result in a scale score ranging from 0 to 28, enabling the level of PTSP to be categorized as ‘normal’, ‘borderline’, or ‘clinical’ (α = .73).
Climate scale
Two 8-item subscales of the Climate Scale (CS; Donkers & Vermulst, 2014) were included in the self-report questionnaires. The Climate in the Class (CIC) subscale assesses children’s perceptions of classroom peer interactions. The Quality of Mutual Peer Relationships (QMP) subscale measures pupils’ satisfaction with the connectedness and cohesion among classroom peers. Standardization data were gathered among a large sample of pupils in The Netherlands, resulting in satisfactory norms for general primary schools (COTAN, 2014), though standardization for refugee and immigrant children is lacking. Studies have provided evidence for the validity of the subscales (Donkers & Vermulst, 2014). Cronbach’s alpha in our sample was .84 for the CIC subscale and .79 for QMP.
In the multi-informant data-collection (March 2018), teachers completed questionnaires independently; data collection with children and parents was organized in (class) group, assisted by the research team. Children and parents received additional support by means of pictograms, translation by qualified interpreters, translated questionnaires, and standardized clarifications by the researchers. Participants worked independently. Socially desirable responses were discouraged as much as possible by ensuring participants that their answers would be treated confidentially. Prior to the study, approval of the research design was obtained from the university’s Ethics Committee.
Analysis
Descriptive statistics were used to describe demographic characteristics and the outcome variables for the refugee, the immigrant and the total sample. Given that the assumption of normality was not met for several of the variables in our participant sample, non-parametric Mann-Whitney tests were performed to compare the means of both groups. In addition, the clinical significance of outcome measures was examined using categorizations and cut-off scores based on large population-based surveys. Finally, cross-tabulations and kappa statistics were used to investigate the level of agreement on the amount of total difficulties between the multiple informants that completed the SDQ (Tang et al., 2015).
Results
Mental health problems
Mental health problems in primary school refugee and immigrant children.
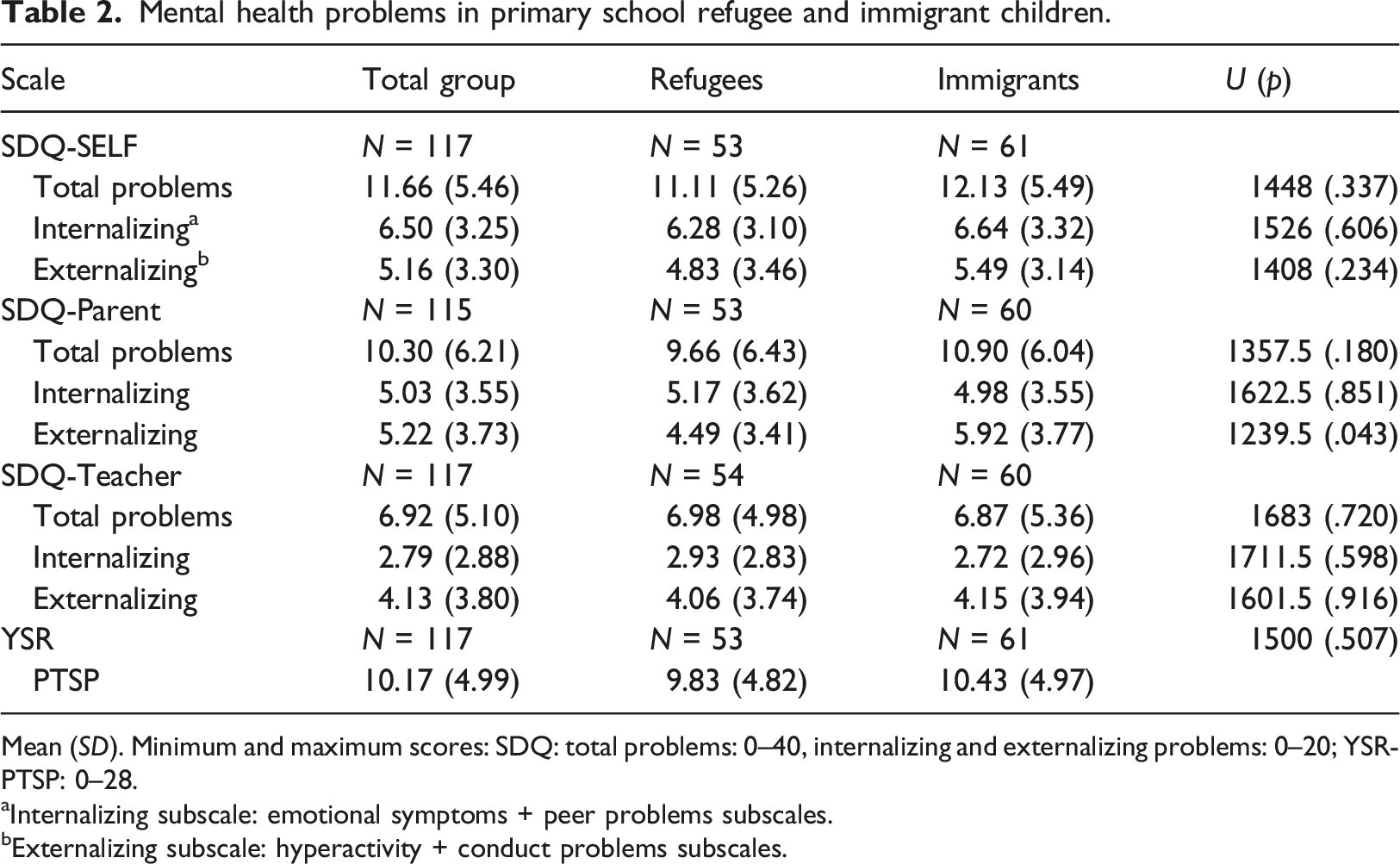
Mean (SD). Minimum and maximum scores: SDQ: total problems: 0–40, internalizing and externalizing problems: 0–20; YSR-PTSP: 0–28.
aInternalizing subscale: emotional symptoms + peer problems subscales.
bExternalizing subscale: hyperactivity + conduct problems subscales.
Clinical categorization (%) of SDQ and YSR scores.

Agreement between informants on SDQ-Total difficulties in the child (%).
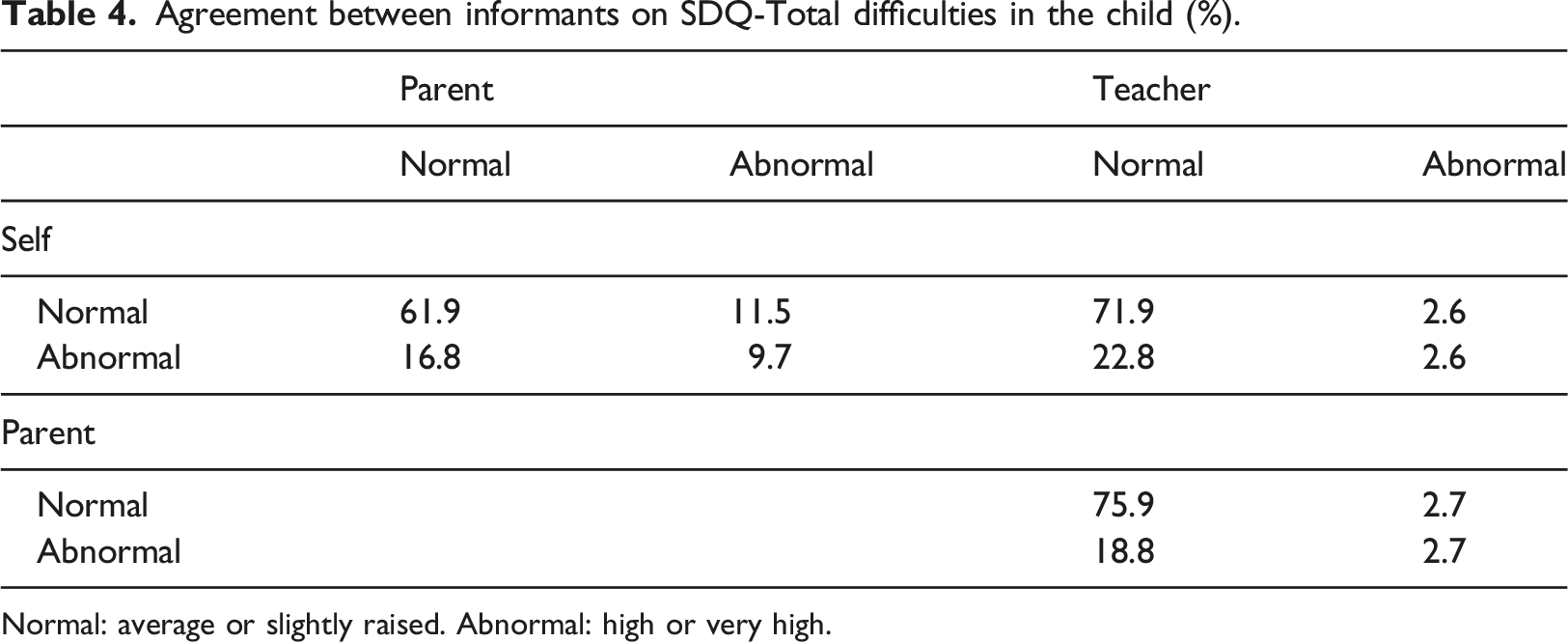
Normal: average or slightly raised. Abnormal: high or very high.
Social classroom relationships
Social classroom relationships as reported by primary school refugee and immigrant children.
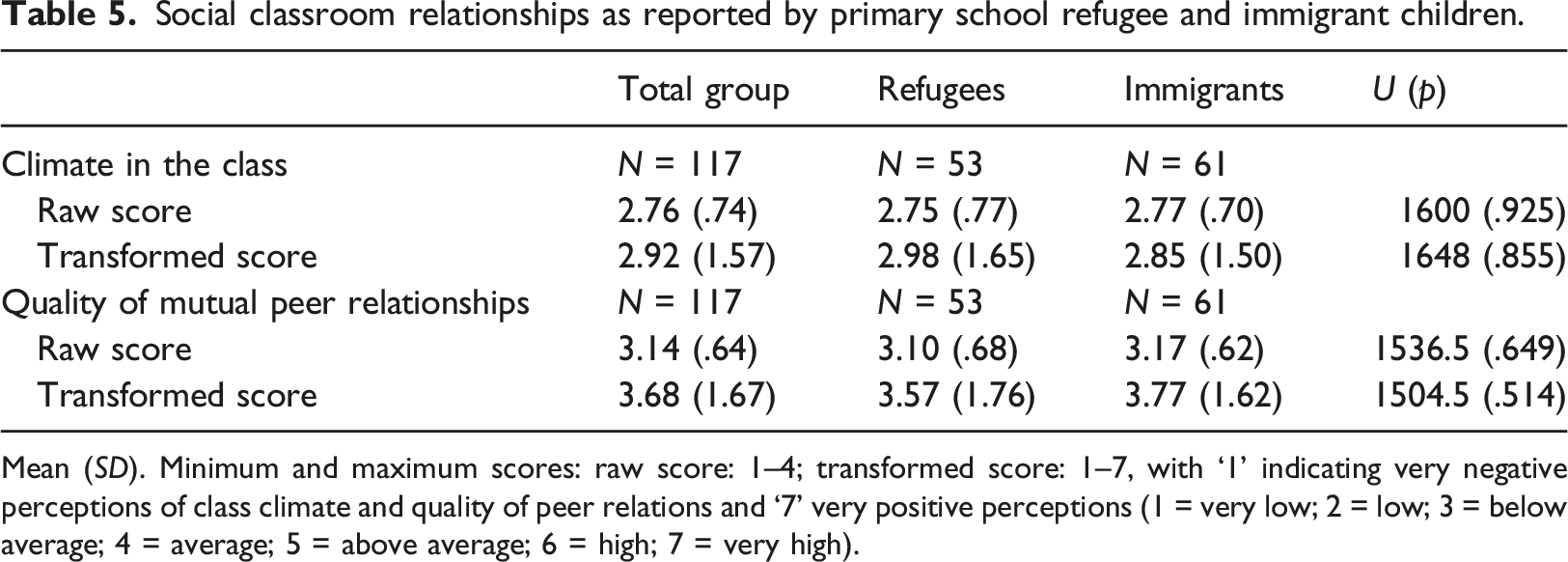
Mean (SD). Minimum and maximum scores: raw score: 1–4; transformed score: 1–7, with ‘1’ indicating very negative perceptions of class climate and quality of peer relations and ‘7’ very positive perceptions (1 = very low; 2 = low; 3 = below average; 4 = average; 5 = above average; 6 = high; 7 = very high).
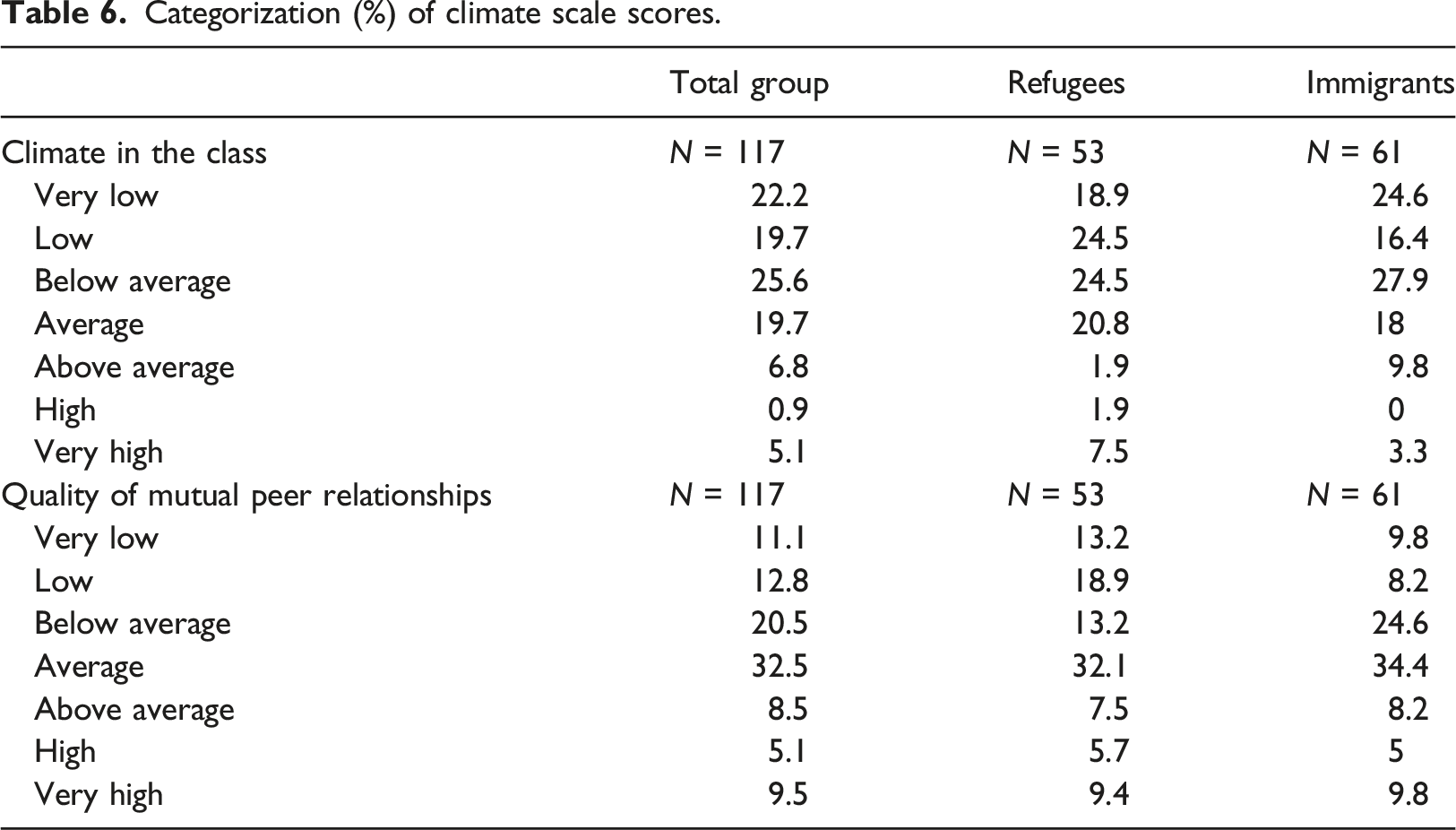
Categorization (%) of climate scale scores.
Pearson correlations between mental health outcomes and social classroom relationships.
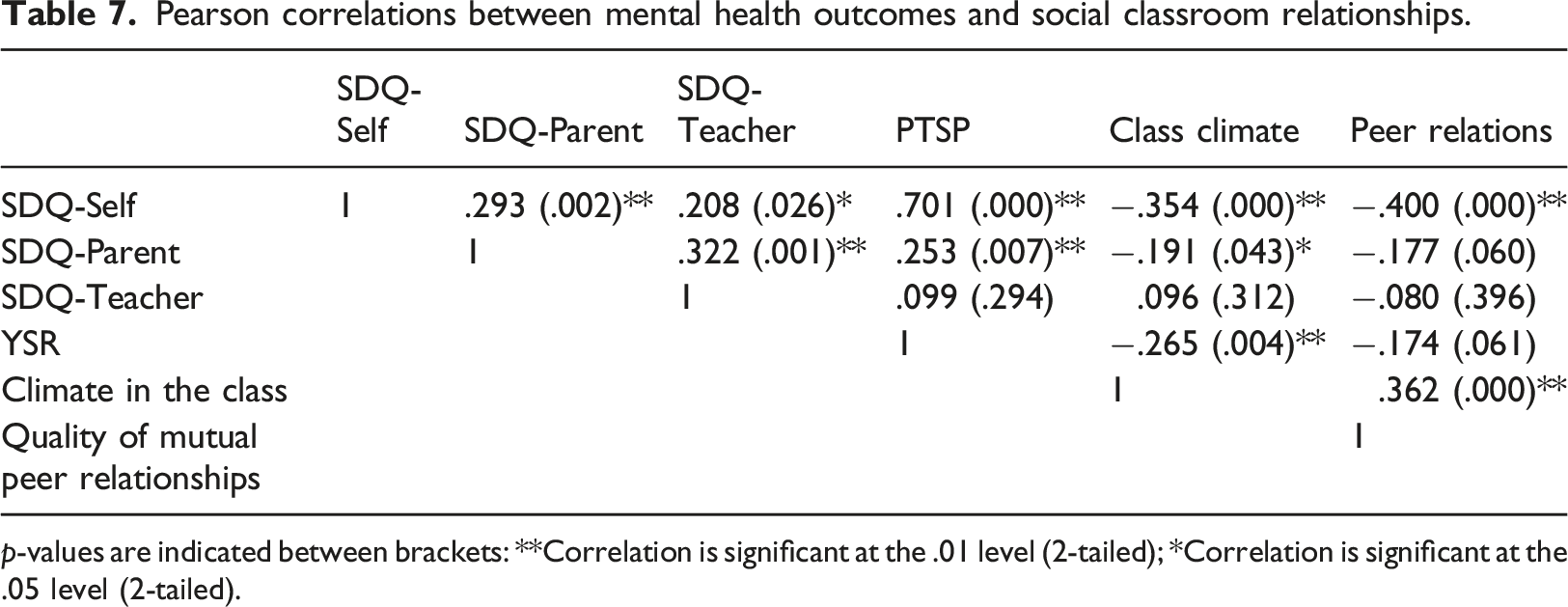
p-values are indicated between brackets: **Correlation is significant at the .01 level (2-tailed); *Correlation is significant at the .05 level (2-tailed).
Discussion
Through a multi-informant assessment, this study explored mental health profiles and classroom relationships in primary school-aged refugee and immigrant children.
This study shows self-reported mental health problems that are elevated as compared to those documented in population-based surveys: on emotional and behavioral problems, around 25% of participants scored high or very high, while this percentage in European community samples generally lies around 10% (e.g., Wright et al., 2020). On PTSP, around 30% of the total participant sample scored in the borderline or clinical range, while prevalence of PTSD has been estimated at <1–10% in the general youth population (Mollica et al., 2004). Comparing our study results to other studies using this YSR subscale, the percentage of participants scoring in the borderline or clinical range corresponds to that found in poly-victimized adolescents (Kirchner et al., 2014). Scores for emotional and behavioral problems, nor for PTSP, statistically differed for refugee versus immigrant participants, with exception of immigrants’ parents reporting more externalizing problems than refugees’ parents.
For refugee children, 28.3% scored borderline or clinical on PTSP, which lies within the range of estimated prevalence rates of PTSD for this group, situated between 19 and 54% in previous studies (Kien et al., 2019). The 9.4% of refugee participants scoring ‘very high’ on emotional and behavioral difficulties echoes findings of Dutch study with asylum-seeking children (9%; Wiegersma et al., 2011). Immigrant participants, almost 90% of which were first or second generation immigrants, reported similar rates of emotional and behavioral difficulties as refugee participants. Refugee and immigrant children share resettlement stressors of social isolation, elevated poverty risks, discrimination, and lack of belonging, with previous studies demonstrating how these risk factors increase psychological problems among immigrant children (Ceri et al., 2017). Remarkably, PTSP-rates in immigrant participants were high, and indicate the importance of further understanding immigrant children’s trauma exposure and its mental health impact. Indeed, with a present-day lack of quantitative studies on posttraumatic stress in non-refugee immigrant children, our study points to the need of adopting sensitivity to how traumatization may impact these children’s psychosocial functioning. With few studies pointing to the role of community violence (Jaycox et al., 2002), domestic violence (e.g., Gray et al., 2014), and traumatic stressors during migration, future research is needed to support an in-depth understanding of trauma exposure in immigrant children.
Whereas around 25% of participant children report a high or very high prevalence of emotional and behavioral problems, teachers make a less alarming assessment. They locate 5% of participants within the range of (very) high symptomatic functioning. Cross-informant comparisons indicate that an important group (22.8%) of children reporting (very) high difficulties is not detected by their teacher. A comparison of mean scores furthermore indicates that teachers identify different symptoms: while children report more internalizing than externalizing problems, teachers observe more externalizing symptomatology. This low correspondence is in line with previous research that indicated low teacher-child correspondence, with teachers perceiving a lot less internalizing problems than refugee children themselves (Goldin et al., 2008). These findings underline the importance of focusing on the advancement of teachers’ expertise in the early identification of children with internalizing difficulties (Weiss et al., 2019).
Another remarkable finding of our study was the relatively conflictual and unsafe appraisal of classroom atmosphere by the majority (70%) of participants. The percentages of very low and low ratings are much higher in our sample than the ones found in population-based standardization research, where only 35% of children in the norm group rated the climate in the class as very low to below average (Donkers & Vermulst, 2014). In our participants, perceived unsafety in the classroom furthermore related to higher post-trauma symptomatology. PTSD is, among other symptoms, characterized by increased arousal (e.g., hypervigilance, irritability) and distrust (APA, 2013). This might result in difficult peer relationships, negative perceptions of classroom peer interactions, or withdrawal, and potentially intersect with bereavement or missing a (sometimes idealized) home country. On the other hand, an unsafe classroom context, characterized by conflicts and bullying, might increase PTSD symptomatology in traumatized children, potentially also compounding previous migration-related traumatic experiences (Kira et al., 2014). Given that previous research has associated a perceived sense of safety at school with low risk of PTSD (Geltman et al., 2005), it seems crucial to make classroom safety and positive peer interactions central foci in school-based interventions aiming to improve young refugees’ and immigrants’ well-being. These perspectives highlight also the importance of supporting teachers in sensitively identifying and regulating traumatic distress in their pupils.
Limitations and future directions
Findings are based on a relatively small sample size, associated with difficulties in recruitment of refugee families. While relatively small sample sizes are generally accepted in this field due to the uniqueness of the study population and the urgency of the public health issue under study (e.g., Fête et al., 2019), studies with larger samples remain pivotal.
Our study was implemented in three schools with a high concentration of immigrants in school composition. While schools frequented by refugee and immigrant children are often characterized by multi-ethnic school composition with a lower socio-economic profile in an urban setting (Pulinx et al., 2017), the high number of refugee and immigrant children in participating schools may limit the generalizability of our study’s findings to similarly composed school contexts. Future research on refugee and immigrant children’s mental health might furthermore consider ethnic school composition in itself, as scholars documented the role of school composition in pupils’ self-esteem and the quality of the interethnic peer relationships (e.g., Agirdag et al., 2012).
Concerning assessment instruments, both SDQ and YSR were originally developed for use with youth aged 11 and older, while a substantial part of our participant sample was younger. Although reliability and validity of these scales for younger children has been studied (Curvis et al., 2014; Ebesutani et al., 2011), the diverse cultural, linguistic, and migratory background of the participants might have further complicated assessment (Stolk et al., 2017). Also, while overall the internal consistency of measures proved satisfactory, the lower internal consistency of self-reported internalizing problems (SDQ) necessitates careful interpretation of our findings.
Lastly, our aim was to describe mental health in populations of refugee and immigrant children. While differences were found between both groups, this does not necessarily mean that these differences can be attributed to children’s refugee status. Indeed, we found that both groups differed in various aspects (e.g., maternal education) and it is possible that differences in mental health are due to these (or other) aspects instead. Unfortunately, our relatively small sample size did not allow for an in-depth comparison of refugees’ and immigrants’ mental health profiles, taking into account potentially confounding factors such as gender, time in resettlement, socio-economic profile, and maternal educational status. This is especially true because some potential confounding variables are categorical with few observations per category and because of missing values. With our study raising hypotheses on the potential role of different migration-related and socio-economic factors in both refugee and immigrant subsamples, future large-scale studies may develop a better understanding of the interplay between these variables and refugee and immigrant child mental health (Dogra et al., 2012).
Conclusion and implications
This study reports findings with important public health implications: it offers insight into the vulnerable mental health profiles of refugee and immigrant children in multi-ethnic classrooms in an urban Flemish sample. High levels of emotional and behavioral difficulties and post-trauma functioning in immigrant pupils indicate that not only refugee, but also immigrant children form a population at risk for traumatization. Further research is needed on forms of past and current trauma exposure. The study also highlights high degrees of stress and conflict experienced in the classroom by children, indicating the potential role of school-based intervention in promoting safety and well-being for an at-risk group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fund for Scientific Research Flanders (FWO – Fonds voor Wetenschappelijk Onderzoek) under Grant number G0F5117N (FWO-Rode Neuzen)