
Abstract
This study explored the embodied experience of body change using a qualitative design. Eight previous plastic surgery patients of a London hospital took part in in-depth, semi-structured interviews 1 year post a plastic surgery procedure to remove excess skin around their abdomen, resulting from weight loss. Participant interviews were analysed using Interpretative Phenomenological Analysis. Two sub-themes titled ‘Shame of the hidden body’ and ‘Lack of acceptance; the future focused body’ are presented in this article. Findings are considered in relation to theories of ‘Body Shame’ and in the current cultural context.
Introduction
Western culture’s preoccupation with beauty and thinness exists alongside a fixation with an obesity ‘epidemic’. The Department of Health (DoH) (2011) published new health agenda aiming at sustained downward trend in levels of excess weight in adults and children by 2020. Despite the apparent prevalence of obesity, it is not accepted in a culture that designates the obese body as out of control and ‘rapacious’ (Orbach, 2009). It is, therefore, not surprising that at any one point in time 1 in 4 women and 1 in 10 men are estimated to be dieting to lose weight (NICE, 2006).
Sarwer et al. (2008) report that many obese individuals seek bariatric surgery for its anticipated psychosocial effects. In their review and meta-analysis, Blaine et al. (2007) concluded that psychosocial well-being (e.g. self-esteem, depression) is generally improved by weight loss treatment. Literature suggests that body image and body dissatisfaction do improve with weight loss (e.g. Guisado et al., 2002), but often it remains significantly higher than that of controls (e.g. Hotter et al., 2003), particularly in the case of childhood onset obesity (Adami et al., 1998). Quality of life (QOL) measures have been shown to improve following weight loss (e.g. Tolonen and Victorzon, 2003), and these changes are mainly accounted for by improvements in physical health (Swan-Kremier, 2005).
In the context of extreme weight loss, it is common for people to experience body dissatisfaction due to the ‘frequent’ resultant excess skin on ones abdomen, arms, face and thighs (Swan-Kremier, 2005: 112). This has been reported to cause discomfort and significant appearance-related distress (e.g. Boccheieri et al., 2002). Kinzl et al. (2003) report that 70 per cent of their participants considered that excess skin was a negative consequence of weight loss (Kinzl et al., 2003).
It has been suggested that the ‘curious omission’ of the experience of excess skin in the literature may be due to a bias of obesity research to ignore negative outcomes of weight loss (Boccheieri et al., 2002: 160). It is predicted that as more obese people lose significant amounts of weight, the demand for cosmetic surgery to remove their resultant excess skin will increase substantially (American Society of Plastic Surgeons, 2003).
Plastic surgery
A recent audit by the British Association of Aesthetic Plastic Surgeons reports that despite the recent recession, the amount of cosmetic surgery procedures rose by a further 6 per cent in the United Kingdom between 2010 and 2011. They report that 90 per cent of these procedures are carried out on women. Social commentators criticize the normalization and rhetoric of empowerment of plastic surgery in today’s society (e.g. Orbach, 2009), and it is discussed as the most provocative and controversial aspect of the new ‘make over culture’ (Jones, 2008). In a time when so many are encouraged to transform their bodies, it seems pertinent to consider the psychological experience of body transformation.
Plastic surgery following weight loss
Excess skin is removed from post-weight-loss patients using a variety of different plastic surgery methods. Excess skin is typically removed from the abdomen (abdominoplasty), thighs, arms, back and breasts. These procedures are grouped together as ‘body-contouring’ procedures (Taylor and Shermak, 2004). Of the 3375 abdominoplasty procedures that were reported in 2011 in the United Kingdom, 3251 were performed on women (BAAPS, 2012).
Mitchell et al. (2008) report that 33 of the 70 participants, who had undergone a gastric bypass 6–10 years earlier, reported undergoing 38 body-contouring procedures. The most common was the abdominoplasty (24.3%) followed by breast lifts (8.6%) and thigh lifts (7.1%). They report that participants were not ‘uniformly satisfied’ with their body-contouring surgery, stating that the affected area was ‘unattractive’. They also report that the majority of participants expressed a desire to have body-contouring surgery on several parts of their body. Seemingly, a significant subgroup of people who have lost weight wish to and do undergo body-contouring surgery.
It is clear that in recent years, the calls for more investigation into the experience of excess skin and its removal after weight loss have been answered in the form of quantitative research. Typically, body image appears to have been improved by the post-weight-loss plastic surgery (Bolton et al., 2003; Lazar et al., 2009; Pecori et al., 2007; Song et al., 2006; Stuerz et al., 2008). Measures of QOL have also typically improved post surgery (Cintra et al., 2008; Lazar et al., 2009; Song et al., 2006). Studies have shown that self-esteem does not improve (Bolton et al., 2003), whereas anxiety and depression have appeared to remain stable (Bolton et al., 2003; Song et al., 2006; Steurtz et al., 2008).
The literature on this experience paints a complex picture. It appears that functional and psychosocial improvements are likely to be experienced, but that in the latter, changes are limited and are likely to vary from person to person. The studies into this experience have been of a positivist, quantitative nature with much of it being conducted by bariatric and plastic surgeons considering specific variables. The reliance on constructs such as ‘Body Image’ and the assumptions, which underlie such reliance, have been highlighted as problematic by Gleeson and Frith (2006).
As has been mentioned by Bocchieri et al. (2002), it could be the case that the pervasive nature of anti-obesity bias has led to particular questions being asked and not asked. For these reasons, it is suggested that a qualitative enquiry into this field would be timely and would return the voice to the individuals who live the experience. As a result, it would hopefully distance itself from pre-existing theories about benefits of weight loss and from possible anti-fat bias. It could also enable a broader approach, remaining open to novel aspects of experience.
Methodology
Design
The study used a qualitative design with one-to-one semi-structured in-depth interviews.
Participants
Eight women who, approximately 1 year ago, had excess skin removed by plastic surgery following significant weight loss participated. All participants had their procedure(s) at the same London hospital and were identified using the hospital’s surgical records. The 1-year time frame means that their surgical scars are likely to have ‘settled’ and stopped changing in feel and appearance. The age range was 29–60 years. While males were invited, only females responded to the invitations. Of the sample who were invited only 3 were men and 26 were women.
Procedure
Potential participants were sent an invitation to participate along with an information sheet by post. They were invited to communicate their interest in participating in the research project by contacting the researcher and encouraged to read the information sheet thoroughly before doing this. Interested potential participants were invited to discuss any queries they had with the researcher and/or members of the Plastic Surgery Department. Interviews were predominantly conducted at participants’ houses but two were conducted in a hospital clinic room. The researcher reviewed the consent form with the participants before they signed it, ensuring fully informed consent was obtained. Interviews took between 50 and 80 minutes. The interview schedule consisted of open-ended questions regarding the participants’ experience of their body change such as ‘how do you feel when you think of your body as it is now? And prompt questions such as ‘what does that mean to you?’
Participants were provided with various contact details in the event of the interview bringing up issues that they wished to discuss further. Interviews were conducted by the researcher and were digitally recorded and transcribed. Interview transcriptions included all spoken words, pauses, false starts and other aspects worth noting (e.g. laughter).
The researcher engaged in three reflexivity interviews to ‘make explicit’ some of the features she may have brought into the research. Particular attention was paid to the fact that she is an outsider to the experience of the participants and the effect this could have on the already rife power differentials in any research interview.
Ethical approval was gained from the University of the researcher, the research and development department of the hospital and the local centralized National Health Service (NHS) Research Ethics Committee
Data analysis
Transcribed interviews were analysed using Interpretative Phenomenological Analysis (IPA) to make sense of the subjective accounts of the participants. As Larkin et al. (2006) state, the phenomenological commitments of IPA ‘give voice’ to the concerns of the participants, while the interpretative aspect allows for the researcher to ‘make sense’ of and contextualize these experiences from a psychological perspective.
Broadly speaking, IPA is a process that continually moves from detailed description of the text to interpretation and from looking at the particular lived experience to the shared. To this end, it has been described by Smith (2007) as an iterative and inductive cycle. Six stages of the analysis were engaged-in, which were most recently outlined by Smith et al. (2009).
Analysis and discussion
The analysis yielded two constituent themes consisting of several sub-themes each. Please see Table 1 for all theme titles. Due to the breadth of the findings and the depth that is required to consider them appropriately, this article will present two interrelated sub-themes of the constituent theme 2 ‘Self-acceptance in continued flux’. These themes were selected due to their link to commentary regarding the current cultural context, their related theoretical explanations as well as their potential to shed light on more general experiences of body change.
Table illustrating titles of all the themes that emerged from the analysis process

The two interrelated sub-themes presented are ‘Lack of acceptance; the future focused body’ and ‘Shame of the hidden body’. The analysis presented is intended to be the researchers’ interpretation of the participants’ interpretation of their lived experience.
Lack of self-acceptance; the future focused body
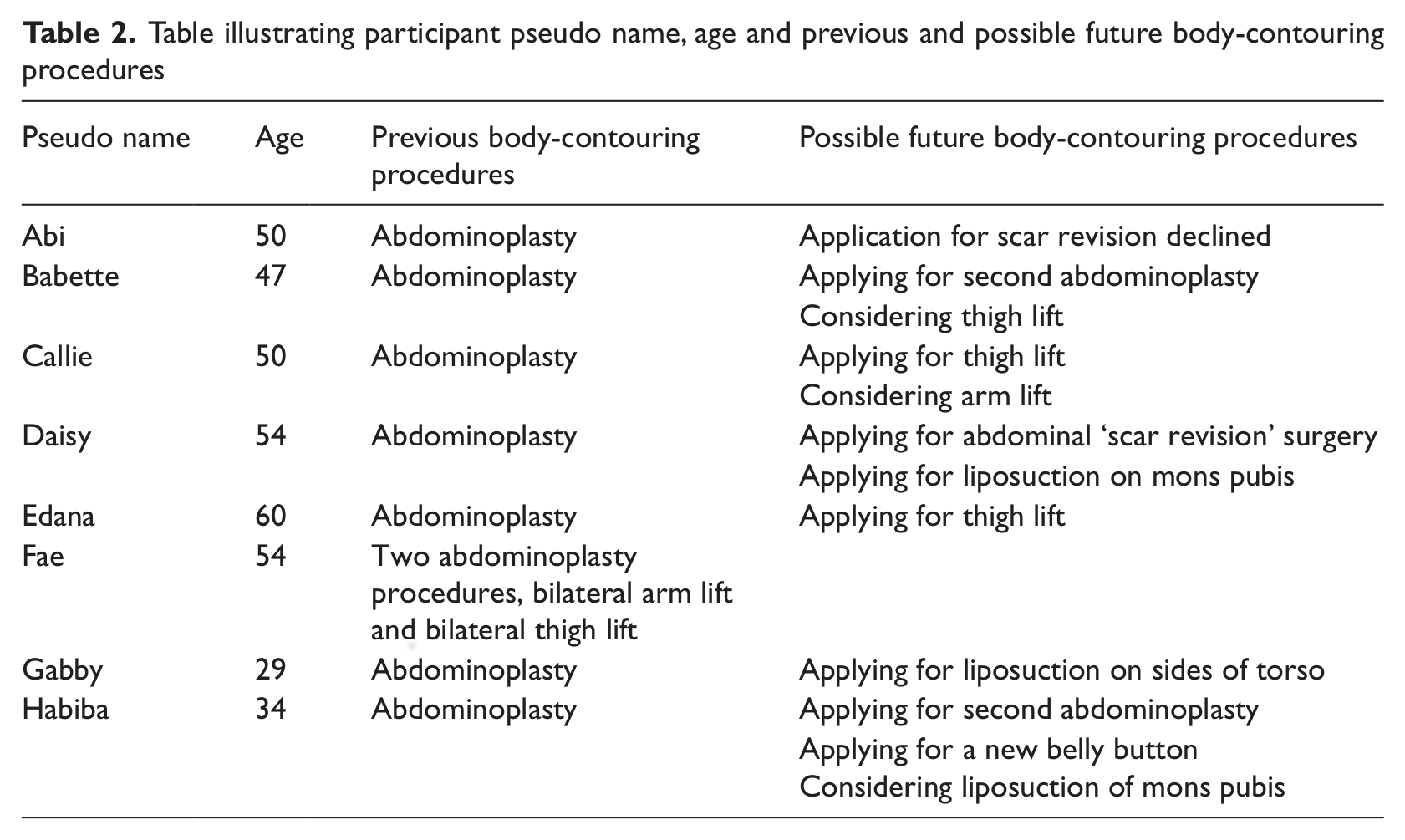
This theme describes the tendency for all participants to talk about their hopes for their bodies in the future, even when asked to reflect on their body in the present. As is evident in Table 2, all but two of the participants in this study were hoping to have further procedures to remove their excess skin on other body areas funded by the NHS. Of the two not applying, one had applied but had been told that she would not receive any more funding and the other had already undergone four body-contouring procedures. In addition, most expressed hopes for further weight loss. All participants appeared to prefer to consider their body in the future once it had been ‘improved’ rather than ‘inhabiting’ their body in the present.
Table illustrating participant pseudo name, age and previous and possible future body-contouring procedures
Below is an example of a typical interaction:
1 If you think of your body now, maybe unclothed, what does it get you thinking, what comes up for you?
That I want to take those two stone off and get back so I can wear those clothes that made me feel a lot better. But also, I want this corrected. (Daisy, 23/10)
Here, Daisy responds to the question about her body in the present with a set of aims and improvements for her future. This is reflective of most other participants. It seems that it is difficult for her to consider her body in the present suggesting a lack of acceptance of how things are currently. Her language also suggests that her body is still faulty as she describes her wish to have her body ‘corrected’: I am waiting for some more correction because they somehow did it completely skew whiff. I really love my one side but I have an overhang on the left, so I have to go back and get that corrected. (Daisy, 1/18)
Here, she repeats the word ‘corrected’ and describes ‘have’[ing] to be corrected. This suggests a refusal to accept and a determination to change her body physically. In reality, it is not certain that she will have this ‘corrected’ by the NHS. Her positioning of the ‘overhang’ as the problem could have implications for her experience of her body in the future.
Gabby discussed an increase in confidence following her previous body change but appears to be considering a future (after another procedure) in which she hopes to be more confident: But yeah I am more confident now. Once I have had this other surgery now hopefully I will be totally totally confident. (Gabby, 34/28)
Babette describes her expectations of her next procedure: I know the operation is not one that is going to be a miracle but it will be a lot better than what I am now. (Babette, 22/4)
She appears to see surgery as being an improvement rather than an end point. Interestingly, Babette talks about her self being improved by the surgery, not just her body; ‘better than what I am now’. This suggests that she views her body as inextricably bound-up in her ‘self’ and therefore describes an embodied experience.
Callie describes her consideration of her future and the possibility that she will undergo the plastic surgery procedures that she wants to have: I have got no idea about that, that is something that is put on a different shelf. It’s not like you can go and buy one get one free [Plastic Surgery procedures]. You can’t. That’s a different issue. That is something that I am learning to cope with. Not live with but cope with. (Callie, 33/2)
She uses the metaphor of a shelf as a place to leave something that is problematic, possibly implying it is too distressing to be considered fully.
Callie states that she is learning to ‘cope’ with the uncertainty of whether she will be offered further plastic surgery on the NHS. It appears that she does not feel able to ‘live’ as she is. Perhaps she feels that life would only be a matter of coping while she inhabits the body she has. She seems far from accepting of how things are now and does not believe that she can reach acceptance without further physical change.
Many aspects the participants reported appear to support previous quantitative research. This includes the lack of regret regarding weight loss and plastic surgery (Lazar et al., 2009; Stuerz et al., 2008). In addition, all participants reported improved overall QOL following weight loss (e.g. Tolonen and Victorzon, 2003) and removal of excess skin (Cintra et al., 2008; Lazar et al., 2009; Song et al., 2006). Despite this change, previous studies found that participants were keen to undergo further body-contouring procedures following their first one (Mitchell et al., 2008) and this was reflected in this study.
Previous researchers in this field suggest that the tendency to seek further plastic surgery after the initial procedure was due to participants’ happiness with the service they received (Cintra et al., 2008), their initial procedure ‘intensifying’ their desire for plastic surgery (Stuerz et al., 2008) and their initial procedure triggering dissatisfaction with other areas of their bodies (Song et al., 2006). The findings from this analysis suggest that participants’ continual desire for more surgery might be born out of continued disappointment as a result of particular needs not being met by the surgery and the continued hope that it will be the next procedure that enables the psychosocial shifts they have been hoping for.
Flux and the ‘transformation culture’
Commentators on the current ‘cultural moment’ have discussed the ‘transformation culture’ (e.g. Jones, 2008; Orbach, 2009). Jones (2008) refers to the ‘make over culture’ that positions the body as something to be ‘fixed’, and this theme seems to corroborate these ideas. It appears that while the participants hold ideas and hopes of the bodies they want in the future, they are unable to ‘be’ in their bodies in the present. This idea could go some way to explain the findings that while all participants discussed improvements in their QOL since weight loss (e.g. buying ‘normal’ clothes), their dissatisfaction with their bodies seemed not to have improved as they would have liked.
Many participants voiced concern that they would not get NHS funding for the next procedure they wanted because they were unable to afford it privately. Interestingly, Abi, who was recently told that she would not be offered any more surgery, appeared to find this helpful in enabling her to be more accepting of her body in the present. It could be that the mere possibility of plastic surgery to improve the body makes acceptance of a body as it is harder to achieve.
Shame of hidden body
A common theme in participants’ accounts related to a long history and a current behaviour of hiding their bodies. It appeared that this was motivated by a sense of shame and an assumed lack of acceptance of their body by others.
See, clothes I can hide everything but unclothed no. I haven’t got a full-length mirror in the house. I wouldn’t have a full-length mirror.
What would that be like for you to have to look at yourself in a full length mirror unclothed?
No, no. I wouldn’t. No. That’s why I don’t like my hubby seeing me. I have only got to look down at it and I am looking at a different angle, not full on. (Callie, 25/13)
It seems as though Callie feels unable to think about looking at herself naked in the mirror. She appears to be fearful and avoidant of what she might see in the reflection and how it might make her feel. She repeats the word ‘no’ four times in her last two sentences, which emphasizes the strength of her resolution to avoid considering herself in this way. This resolution could result in a distanced relationship with her body.
Callie’s lack of acceptance appears to be transferred on to her husband, as she assumes that he would not be accepting either. Avoiding exposing her body to her husband could service to maintain the situation as it removes the opportunity for her to experience possible acceptance from him, which might, in turn, serve to help challenge her own ideas. Callie describes her feelings towards her husband seeing her naked:
Even now, if he was to open the door to the bathroom, he’d think nothing of the way I look now but I would break his nose with the door with the way I slam it. You know it does cause problems.
So after the apronectomy it means a lot for …
Yeah because it’s exposed other areas … yeah, yeah, that I couldn’t see because it was under my stomach. (Callie, 16/7)
There appears to be a conflict here for Callie about whether her husband would be accepting or not of the appearance of her body. She appears to believe that he would ‘think nothing of it’ and yet she would take extreme measures to hide her body from him. It could be that she has an underlying belief that her body could not be accepted by anyone, and that while her husband might have reassured her, she cannot believe that he would not experience the same shame and disgust that she reports.
Callie goes on to describe the fact that since her abdominal overhang was removed, other areas have become visible to her that she was previously unaware of. This has implications for the embodied experience and the alienation that she might feel from her body, or parts of it. In addition, the hope for surgery to help her relationship with her body is complicated by its revealing new ‘problematic’ areas. It seems as though the removal of the overhang has provided an exposed feeling and the arrival of other reasons to feel ashamed. She later describes her body as ‘gross’ and her remaining excess skin as ‘horrible’.
Gabby describes her imagined responses of others to her body:
What are you thinking other people might think [about your body if they saw it]?
Just looking at how disgusting I am. How disgusting.
Gabby states that people would find her disgusting, implying the body and self are inextricably bound-up with one and other and would trigger disgust in others. This suggests an intensely difficult and upsetting experience: You know I wouldn’t. I wouldn’t have done that [worn a bikini in public] when I was big, I won’t do it now, even after my surgery. I think even if I looked perfect I wouldn’t do it now. Because I have lost that kind of, umm, I have still got inhibitions. I have lost that kind of freedom if you see what I mean. But I have put that on myself. (Gabby, 37/2)
Interestingly, Gabby is now referring to her body in a more distanced and objectifying manner; as ‘it’ not ‘me’. She describes a strong sense of loss, which she blames on herself. I think that this is a very poignant point, which appears to encapsulate the experiences articulated by all the participants; that because of their previous size, they have lost the opportunity to live in a body without such restrictive ‘inhibitions’.
Edana articulates her concerns about showing her body in public: I don’t think I would allow anyone to see it [current body]. To tell you the truth, it’s not fair for the other people because other people on the beach will be sick. (Edana, 16/27)
This is an illuminating description of the beliefs that Edana holds about her body and its impact on others. It appears that Edana, like Gabby, anticipates disgust responses to her body, such as nausea. This might reflect her own distressing response to her body.
Later in the interview, I asked Edana what she imagined someone might think if they saw her body. She responded: I don’t, I am a monster and I am cut into pieces. Maybe they make funny comments. I don’t think I could accept, do you understand? (Edana, 24/15)
It feels important to acknowledge the emotional potency of this statement, which implies a painful, brutal and intense experience for Edana. Edana seems to believe that people would think of her as un-human, as a monster. Again, this could be representative of her own perception of her body as not human and cut into pieces. Edana’s statement also relates to another theme ‘functional but butchered body’ that relates to the trade-off described between a more functional post-plastic surgery body and the body being ‘butchered’ and becoming unnatural. Several participants made references to ‘Frankenstein’. Edana implies that she feels highly sensitive and vulnerable to judgement like this from others.
This theme relates to the lack of acceptance of the body by others (imagined or real), which seems connected to the lack of acceptance of the body by the self. When a body is hidden, it is less likely that the individual will be able to experience acceptance of the body by another and thus the shame of the hidden body is likely to pervade. It is important to underscore the point that with Western society’s negative appraisals of overweight people, there may be some reality in the fear that these individuals’ bodies would have not been accepted by others. It is proposed that this state of lack of acceptance from the self and others leads to a continued sense of flux where people perceive their body, the very means by which they communicate with the world around them, will be not accepted by that world.
The psychologist reporting in the Lazar et al.’s (2009) study stated that after the long duration of suffering because of their obesity, the new body image can become a source of deep shame and humiliation. Shame has received increasing research and theoretical attention recently (Gilbert, 2002).
It seems that most participants hoped to put an end to their body shame through their body transformation; however, most seem to have been disappointed as many participants continue to be ashamed of their bodies. Having already changed considerably in body shape and size, and to still be experiencing shame, it seems unlikely that it will disappear following further physical change.
The focus and experience of shame described here appear to corroborate Gilbert’s (2002) bio-psychosocial conceptualization of ‘body shame’. Gilbert (2002) highlights the fact that as with most emotions, while some people are able to tolerate shame without acting out defensive behaviours, others find it intolerable and go to great lengths to avoid it as well as avoid situations that might induce it. This avoidance of external shame (being shamed by others) and internal shame (negative, shaming thoughts about the self) is evidenced both in participants continuing to hide their bodies from others and in their avoidance of acknowledging their body as it is in the present.
Gilbert highlights the vital role of social and cultural contexts that provide the ‘threads from which shame and stigma are woven’ (Gilbert, 2002: 35). Orbach comments that in today’s cultural moment, failing to get one’s food and size right can signify failure, rejection of societal values and, of course, shame (Orbach, 2009). The role of ‘self-control’ in relation to stigma is also discussed by Gilbert (2002) and seems particularly relevant to the present sample. Rozin et al. (1999) investigated a theory regarding the different emotions that are evoked from a variety of different ‘violations’. They state that losing control over one’s body and desires (e.g. food) tends to elicit disgust. Some participants vividly described their sense of disgust at their bodies. This appears to have manifested itself in beliefs that the sight of it would make others physically sick (e.g. Edana) and an avoidance of seeing or even thinking about seeing the body themselves (e.g. Callie). It seems likely that this sense of disgust at one’s own body could be connected to the sense of shame. It could be that participants are assuming that how they feel about their body (disgusted) is how others would also feel.
Shame and self-discrepancy theory
Self-discrepancy theory suggests that those who experience high discrepancy between actual-self and ideal-self are likely to experience dejection-related emotions such as sadness, where one’s hopes and aspirations are unfulfilled. In an actual-self and other-ought discrepancy (where the self is perceived as different from what you perceive others think you ought to be), individuals are suggested to experience anxiety resulting from the idea that they have not met standards set by others and so are vulnerable to punishment (Higgins, 1987). There is evidence of dejected disappointment and sadness in not having achieved the aesthetic and psychosocial attributes that they had hoped to achieve through weight loss and plastic surgery. In addition, there is evidence of individuals experiencing anxiety stemming from a fear of punishment (e.g. rejection) by others due to their bodies not being how they ‘ought’ to be. It seems plausible that both of these states could trigger a sense of shame about the self. In the context of this study, the ‘significant other’ who sets standards to be attained could be Western contemporary culture. Therefore, when the body of an individual is perceived as different from their ought-self (thin and young body, stipulated by the media), anxiety is experienced due to fear of lack of acceptance and disgust from others influenced by the same cultural messages.
Shame and lack of acceptance both influence each other in that shame may prevent the body being accepted as it is. In turn, the continued future focus on the body and how it ‘should’ be places the body in the present as not how it should be, and therefore as shameful.
General discussion
This study provides an in-depth consideration of this lived experience and provides rich and novel findings regarding experiences of body change and appearance-related distress. The sample is self-selecting and small, and therefore, no claims can be made about the representative nature of these findings.
The findings of this study suggest that it would be pertinent to consider a broader range of measures in future large-scale quantitative studies (e.g. shame, disgust, intimacy and acceptance).
With regards to clinical implications, there appears to be an inherent tension that is important to address. On the one hand, it is important to avoid pathologizing individual responses to problematic sociocultural messages of specific homogenous cultural ideal of beauty. Psychologists such as Kagan (2007) encourage the development of an increasing ecological and community consideration in the psychologist role, and it seems that lobbying the media and other areas with social influence might be a worthy point of intervention for a psychologist.
On the other hand, it seems important to offer intervention for those who are particularly struggling with reduced self-esteem, distress about appearance, shame and lack of acceptance of the body as a result of these wider issues. Cognitive behavioural interventions have been shown to be effective in addressing body image dysphoria, anxiety and depression (Cash and Lavallee, 1997; National Institute for Health and Clinical Excellence, 2007a, 2007b). In addition, cognitive behavioural therapy (CBT) models, for example Gilbert’s (2002) model of body shame, appear to explain the experience of participants in this study well. In the last decade, third-wave developments in CBT have skyrocketed. Mindfulness and acceptance have been radical additions to behavioural traditions. In the cognitive field, more importance has been placed on the present moment and the function, and not just the form, of cognitions (Hayes, 2004). It seems that the development of a compassionate and accepting approach to the self, and of mindfulness skills, could be helpful interventions for this group of individuals. In particular, problems of lack of acceptance can be formulated in the context of a typically striving culture and can be addressed directly.
Kent and Thompson (2002) suggest that medical treatment for disfigurements only address problems with appearance superficially. This also appears to be the case for participants in this study. In some cases, while underlying psychological processes and factors in relation to appearance are not addressed, it is likely to be difficult to reach psychosocial goals. This is particularly pertinent in the context of findings suggesting that initial aims of weight loss are often psychosocial (e.g. Tinker and Tucker, 1997). Research looking at the effectiveness of clinical interventions (such as those listed above) prior to and post body-contouring plastic surgery would be instrumental in developing guidance for clinical work in this field.
Conclusions
Having gone through a tremendous amount of change in body shape and size, participants seemed to be in a continued state of flux in relation to their bodies. How they relate to their bodies appears to be confused and destabilized, and they communicated high levels of internal and external body shame. Connected to this was a tendency to only consider the body in the future after further potential transformation and to avoid considering it, let alone accepting it, in the present. It is proposed that these aspects of experience are interconnected and maintain each other in their development. While participants have gone about changing themselves physically, it seems that what they have truly been seeking can be summed up in the words of Gabby: [To be able to] accept me for who I am and allow other people to accept me for who I am.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.