
Abstract
The present study examined the moderating role of social support and challenging behaviour on the stress–physical health relationship in parents caring for children with intellectual disabilities. Parents of children with intellectual disabilities (n = 70) reported more physical health problems compared to control parents (n = 45) and were more likely to visit their general practitioner. Furthermore, challenging behaviours, but not social support, moderated this association: parents of children with intellectual disabilities reported poorer physical health when both challenging behaviours and stress were perceived to be high. These findings suggest that interventions need to be directed towards ameliorating the impact of challenging behaviours.
Introduction
Parents caring for a child with an intellectual disability (e.g. autism, Down syndrome and Fragile X) report more psychological distress compared to parents of typically developing children (Dunn et al., 2001; Eisenhower et al., 2005). Moreover, in recent decades, interest in the relationship between psychological stress and physical health has been growing rapidly (for reviews, see Cohen and Herbert, 1996; Schneiderman et al., 2005). Psychological functioning, in particular, exposure to chronic psychological stress and the emotional reactions to the same, has been implicated in the development and progression of a wide range of physical diseases including diabetes, as well as increases in psychosomatic symptoms such as gastrointestinal problems and upper respiratory tract infections (see Cohen and Herbert, 1996; Pinquart and Sorensen, 2003; Ramachandruni et al., 2004). In other caring contexts such as caregivers of patients with schizophrenia (Dyck et al., 1999) and dementia (Lee et al., 2003; Schulz and Beach, 1999), caregiver stress was found to predict poorer physical health with higher rates of infection and greater risk of cardiovascular morbidity and mortality being observed in these caregiver groups, respectively. However, much of this research linking caregiver stress to physical health indices has tended to concentrate on older family caregivers, with few studies examining these associations in relatively younger caregiver families, in particular parents caring for children with intellectual disabilities. More importantly, a call for research on the determinants of physical health outcomes in these parents has just recently been made (Miodrag and Hodapp, 2010).
Like older caregivers, parents providing extraordinary care to children with intellectual disabilities may also be at increased risk of poor physical health. In comparison to controls, parents of children with intellectual disabilities rate their general health as poorer (Allik et al., 2006; Hedov et al., 2000), and older parents were found to report greater limitations from arthritis than controls (Magaña and Smith, 2006). These effects are often more pronounced in mothers (Allik et al., 2006), a likely consequence of being the primary caregiver. In a mixed disability sample (children with cerebral palsy, epilepsy, mental handicap and learning disability), caregiving parents, relative to control parents, were more likely to report greater numbers of specific debilitating health problems such as back problems and arthritis (Lach et al., 2009). However, studies examining the predictors of psychosomatic symptoms such as headaches, gastrointestinal problems and rates of infectious episodes in these parents are extremely rare. In fact, such symptoms have been associated with poorer quality of life (García-Campayo et al., 2008) and lower job satisfaction (Meeusen et al., 2010) and are predictive of future health service use even after controlling for objective indices of health (Sha et al., 2005). Together, these studies suggest that the physical health status in parental caregivers is cause for concern and that research in this field is clearly warranted.
In terms of exploring the underlying pathways, challenging behaviours are one of the main sources of stress in these parents (Blacher and McIntyre, 2006; Floyd and Gallagher, 1997; Hastings et al., 2006; Ludlow et al., 2012) and have been associated with poor mental and physical health in spousal caregivers of dementia patients (Pinquart and Sorensen, 2003). They have also been linked to perturbations of the stress hormone cortisol (Seltzer et al., 2010) and immune response to medical vaccinations in parents of children with intellectual disabilities (Gallagher et al., 2009a, 2009b), both of which are related to a number of physical health conditions (e.g. rates of infection, diabetes). Thus, it could be that challenging behaviours are a likely candidate to explore in this context. Moreover, physical health status was found to be poorer in parents of children with neurodevelopmental disabilities who displayed higher behavioural challenges (Lach et al., 2009) implying that this may be a key determinant of health outcomes in this group. Furthermore, in parents caring for children with intellectual disabilities, increased stress is associated with impaired quality of life and poorer psychosocial functioning (Allik et al., 2006), while in other contexts, stress has been found to be positively associated with poor physical health (Cohen et al., 1991) in particular rates of infectious episodes; those who reported higher stress were more likely to succumb to upper respiratory tract infections compared to those who reported lower stress. Not only do these studies highlight the existence of associations between challenging behaviours, parental stress and poor physical health but they also provide an opportunity to see whether the association between stress and physical health problems in parents caring for children with intellectual disabilities is influenced by children’s challenging behaviours. Thus, it could be that challenging behaviour and stress either alone or in combination are increasing vulnerability to physical health problems in this parental group. For example, in combination, it could be that any association between stress and physical health problems in parents of children with intellectual disabilities could be moderated by the challenging behaviours displayed by the child.
A growing body of evidence has also accumulated demonstrating clear links between social support and a number of physical health outcomes (see Berkman et al., 2000; Uchino, 2006). For example, population-based studies indicate that individuals with low levels of social support have higher mortality rates from coronary heart disease (Berkman et al., 1992; Brummett et al., 2001). There is also evidence linking greater support to lower rates of infectious disease (Lee and Rotheram-Borus, 2001; Patterson et al., 1996), better immune response and recovery from surgery (Kiecolt-Glaser et al., 1998). While in older caregivers of patients with dementia, physical health status was not only associated with patient challenging behaviours and psychological distress but also related to their perceived availability of social support (Schultz et al., 1995). In the context of parental caregiving, social support was found to be particularly important and protective for the physical health of parents of children with cerebral palsy (Raina et al., 2005). Research also demonstrates that stress in parents caring for a child with an intellectual disability is ameliorated through greater social support (Dunn et al., 2001; Ludlow et al., 2012; Weiss, 2002). In fact, one of the key mechanisms linking social support to physical health is through its buffering effects on psychological stress, that is, the stress-buffering hypothesis (Cohen et al., 2001; Cohen and Wills, 1985). The evidence above highlights the links between social support, stress and physical health, and it could be that parents of children with intellectual disabilities with greater social support may report less stress and better physical health compared to those with poorer social relationships.
Therefore, the aim of this study was to examine whether parents of children with intellectual disabilities would report more physical health problems compared to parents caring for typically developing children (controls). Based on the above evidence, it is hypothesized that, first, parents of children with intellectual disabilities would report more physical health problems than parents of typically developing children; second, any association between stress and physical health problems in parents caring for children with intellectual disabilities will be moderated by (1) child’s challenging behaviours and (2) levels of social support.
Methods
Participants and procedure
Seventy parents of children with intellectual disabilities and 45 parents of typically developing children (controls) participated in the study. Parents of children with intellectual disabilities were recruited via special need schools and syndrome-specific newsletters, and through word of mouth. In total, 122 parents expressed interest and requested more information and questionnaire packs. Out of these, 80 parents returned the questionnaires (66% response rate) and 10 were discarded due to incomplete data. Inclusion criteria for these parents were providing home care for a child with autism, Down syndrome or other types of intellectual disability (e.g. Cornelia de Lange syndrome, Smith–Magenis syndrome). The syndrome types were chosen as they represent a wide variety of intellectual disability phenotypes. Twenty-eight of these parents self-reported caring for a child with autism, 20 caring for a child with Down syndrome and 22 caring for a child with other syndromes types (e.g. Wolfram syndrome, Smith–Magenis syndrome). Controls were parents caring for typically developing children recruited via local schools, word of mouth and university advertisements. In all, 64 control parents responded to our call for volunteers, and each was sent a pack of questionnaires and a prepaid envelope in which to return them. Out of these, 45 parents returned completed questionnaires: a response rate of 69 per cent. Furthermore, there were no differences between the groups on the number of parental dyads involved; there were nine dyads in our parents caring for children with intellectual disability sample and seven in the control group, χ2(1) = 0.16, p = .69. Parents who did not return the packs invariably cited time pressures and other family commitments as reasons for non-participation. The study was approved by the relevant University Research Ethics Committee and all participants gave informed consent.
Measures
Participants’ socio-demographics were assessed by standard questions. The Registrar General’s social class classification that is based on the United Kingdom’s occupational status was used as a measure of socio-economic status (Office of Population Censuses and Surveys, 1978). Participants were asked to specify their occupation or that of the principal breadwinner, which was scored as 1, professional (e.g. physician); 2, managerial (e.g. director); 3, non-manual/clerical (e.g. secretary); 4, skilled manual (e.g. carpenter); 5, semi-skilled manual (e.g. bus driver) and 6, unskilled manual (e.g. labourer). This measure has been used previously in caregiver research (Gallagher et al., 2010, 2009a).
Psychological stress
The Perceived Stress Scale (PSS; Cohen et al., 1983) was used to measure psychological stress. This abbreviated 4-item scale, used previously in caregiver research (Gallagher et al., 2009b), measures how stressful individuals perceive situations they have experienced to be over the last month. Scale responses range from 0 (never) to 4 (very often) and include two reverse-scored items, with higher scores indicating greater perceived stress. Items in the scale include ‘In the past month, how often have you felt able to control the important things in your life?’ and ‘In the past month, how often have you felt that things were going your way?’ This scale shows good test–retest reliability (r = .80) and internal consistency reliability (Cronbach’s α = .75). In the present study, an internal consistency reliability of α =.88 was observed.
Social support
Social support was assessed using the 12-item Support Functions Scale (Dunst et al., 1988). Parents rated each source of support available to them, including practical (e.g. ‘someone to help take care of my child’) and emotional (e.g. ‘someone to talk to about things that worry me’) support on a 5-point Likert scale ranging from 1 (never) to 5 (quite often). The total score was used for analysis, with higher scores indicating more social support. It has been shown to be reliable (Cronbach’s α = .86) and has been used previously in intellectual disability research (White and Hastings, 2004). A high internal consistency reliability (α = .89) was also evident for the present sample.
Child’s challenging behaviours
The 25-item Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) was used to screen for child’s challenging behaviours. The measure has five subscales, with one assessing prosocial behaviour (e.g. ‘kind to younger children’) and the other four assessing challenging behaviour problems, such as emotional symptoms (e.g. ‘often unhappy, downhearted or tearful’), conduct disorder (e.g. ‘often argumentative with adults’), hyperactivity (e.g. ‘easily distracted, concentration wanders’) and peer relationships (e.g. ‘rather solitary, tends to play alone’). Parents are asked to rate whether a behaviour of their child is 0 (somewhat true), 1 (true) or 2 (certainly true) with higher scores indicating more problem behaviour. Some items are reversed scored (e.g. generally obedient, usually does what adults request). The scale has been shown to be reliable (Cronbach’s α = .76) and effective at identifying challenging behavioural problems in children (Goodman and Scott, 1999). Furthermore, it has been used extensively in research with children with intellectual disabilities (Hastings et al., 2006). Internal consistency reliability for the whole scale in this study was .88.
Physical health
Self-reported physical health was measured using the Physical Health Questionnaire (PHQ; Schat et al., 2005). This is a brief 14-item self-report scale of somatic symptoms that include sleep disturbances, headaches, gastrointestinal problems and respiratory infection episodes. Parents are asked to rate how often they have experienced these symptoms during the last year, from 1 (not at all) to 7 (all the time). The scale asks questions on sleep (e.g. ‘How often do you wake up during the night?’), headaches (e.g. ‘How often have you experienced headaches?’), digestive problems (e.g. ‘How often have you suffered from an upset stomach?’) and colds and flu (e.g. ‘How often have you had minor colds?’). A high score indicates poor self-reported physical health. A high internal consistency reliability was observed here for the total scale (α = .84). Analogous values were observed for each subscale, sleep disturbances (α = .81), headaches (α = .95), gastrointestinal problems (α = .92) and respiratory infection episodes (α = .87). There is also a single-item question whereby parents were asked ‘Compared to others of your age and sex, how would rate your general health?’ and asked to choose from one of the following: excellent, above average, average, below average or very poor. A simple yes/no question asking participants whether they had been to see their family physician to treat any of these symptoms was also inserted.
Statistical analyses
Initial analyses of group differences were by Chi-squared and univariate analysis of variance (ANOVA), with partial eta-squared (η2p) as the measure of effect size. These analyses were employed to test the first hypothesis. Occasional differences in degrees of freedom reflect missing data from uncompleted questionnaires. To test the second set of hypotheses, which focused solely on parents caring for children with intellectual disabilities, linear regressions, mainly testing hierarchical models, were conducted. In these models, to see if any of the psychosocial variables were predictive of physical health in these parents, each variable was entered separately at Step 1. In subsequent models, we aimed to test for moderation by children’s challenging behaviours and social support on stress and physical health. For this analysis, the approach described by Aiken and West (1991) and Holmbeck (2002) was used. Here, prior to all the analyses, all linear predictor variables were centred at their means to avoid multi-collinearity before entering the cross product into the model in Step 2, with both predictors entered simultaneously at Step 1. As none of the socio-demographic variables were associated with physical health scores in this group, these were not added to any of these models.
Results
Group differences in socio-demographic characteristics, psychosocial factors and physical health
In terms of socio-demographics, 10 per cent of caregivers reported being professional, 17 per cent managerial, 40 per cent non-manual/clerical, 11 per cent skilled manual, 12 per cent semi-skilled manual, and finally, 11 per cent as unskilled manual. Nineteen per cent of controls reported being professional, 18 per cent managerial, 26 per cent non-manual/clerical, 8 per cent skilled manual, 3 per cent semi-skilled manual, and finally, 26 per cent as unskilled manual; there was no statistical difference between the groups χ2(6) = 11.88, p = .07. The majority of our sample reported being White (86% vs 95%) and married/living together (76% vs 93%), for parents of children with intellectual disabilities and controls, respectively; these were not statistically different. The other characteristics of the parental groups are presented in Table 1. As can be seen, the groups are well matched on most variables, although parents of children with intellectual disabilities were slightly older and spent more time caregiving over the course of the day.
Demographic, psychosocial and physical health characteristics of parents caring for children with intellectual disabilities (caregivers) and control parents.
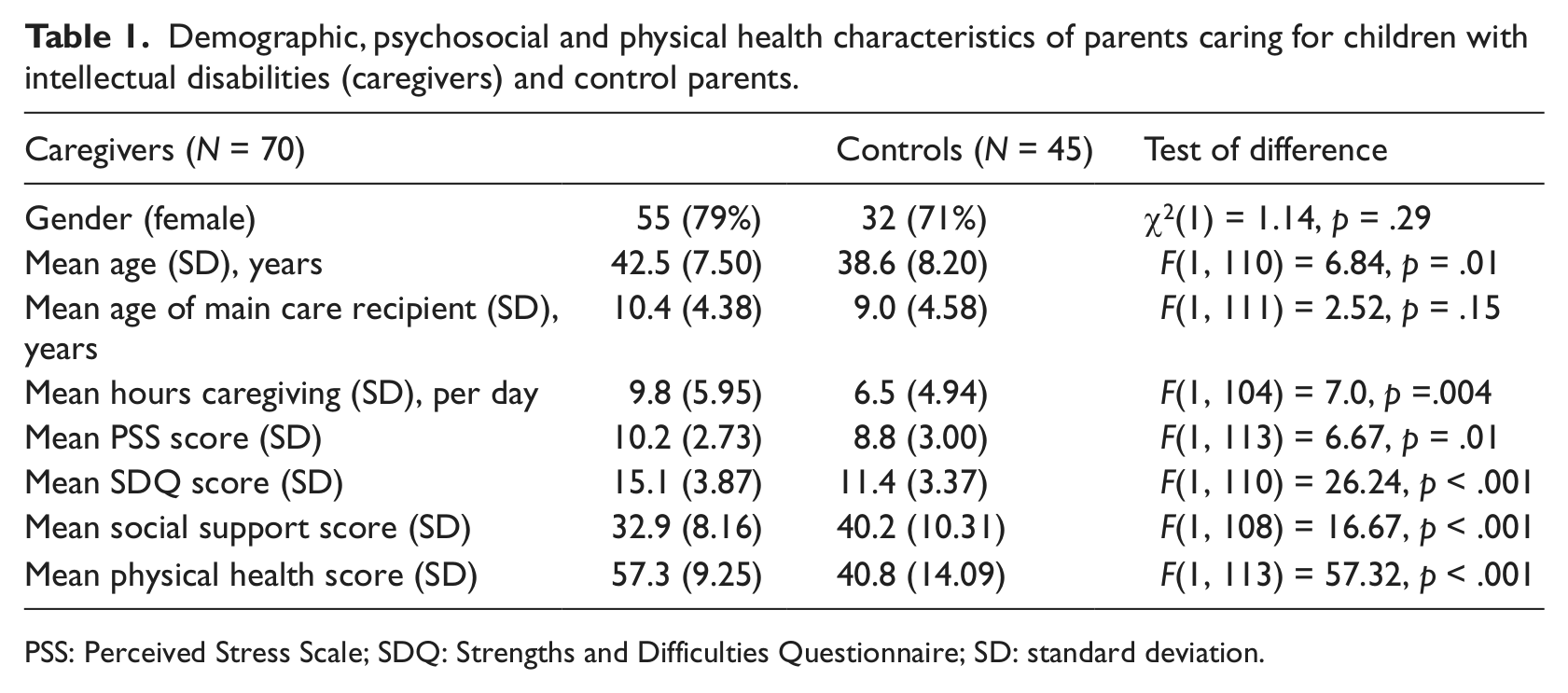
PSS: Perceived Stress Scale; SDQ: Strengths and Difficulties Questionnaire; SD: standard deviation.
As expected, there were differences between groups on perceived stress, social support, challenging behaviours and physical health, and the effect sizes observed for these were partial eta-squares (η2p) of .05, .13, .19 and .34, respectively. Moreover, these η2p values signify small, medium and large effect sizes (Pierce et al., 2004). Parents of children with intellectual disabilities reported higher perceived stress, more challenging behaviours in their children, less social support and more physical health problems than control parents (see Table 1). Furthermore, PHQ subscale analysis revealed significant differences in the domains of sleep disturbances, F(1, 113) = 69.57, p < .001; headaches, F(1, 113) = 41.76, p < .001; gastrointestinal problems, F(1, 113) = 38.07, p < .001 and rates of infection, F(1, 113) = 10.56, p = .002, all of which were higher in parents of children with intellectual disabilities; these are illustrated in Figure 1. A higher percentage of control parents were also more likely to rate their health as above average compared to parents of children with intellectual disabilities, 67 per cent versus 33 per cent, p = .003, and 33 per cent of control parents compared to 54 per cent of parents of children with intellectual disabilities were more likely to seek medical treatment from their general practitioner for these physical health complaints, χ2(1) = 4.84, p = .03.
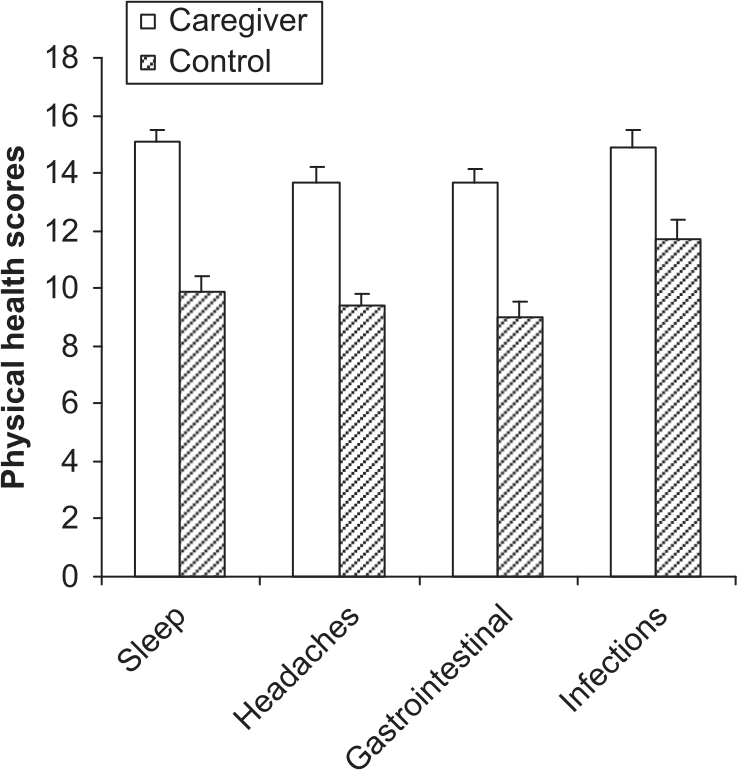
Difference between parents caring for children with intellectual disabilities (caregivers) and control parents on physical health problems in domains of sleep disturbances, headaches, gastrointestinal problems and respiratory infection episodes; high scores indicate poorer health.
Associations between perceived stress, challenging behaviour, social support and physical health in parents of children with intellectual disabilities
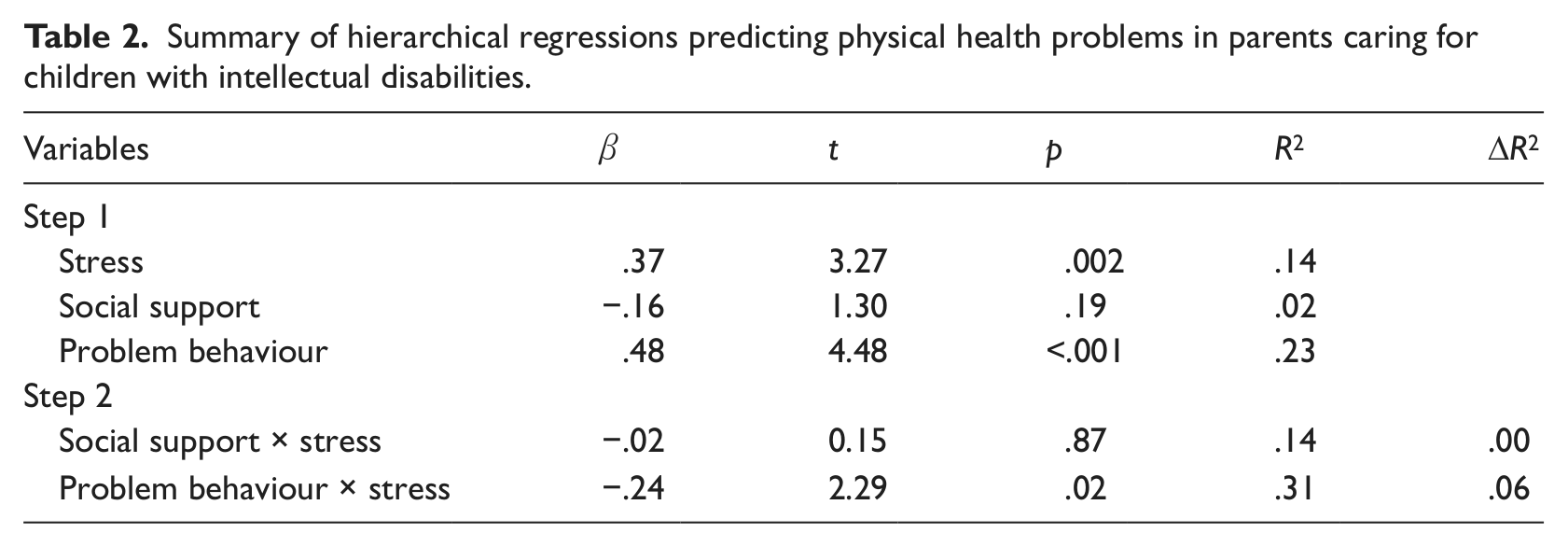
In hierarchical linear regression analysis, perceived stress and challenging behaviours were significant predictors of physical health problems in parents of children with intellectual disabilities at Step 1 (see Table 2 for summary statistics). In analyses in which each of the challenging behaviour subscales were entered simultaneously, only conduct behaviours emerged as a predictor of physical health problem scores, β = .44, t = 3.45, p < .001; greater reporting of conduct behaviours was associated with more physical health problems. Furthermore, after mean centring the predictor variables, a significant interaction between perceived stress and challenging behaviours was found at Step 2, and in combination, these variables accounted for an additional 6 per cent of the variance in physical health problem scores. This interaction is illustrated in Figure 2, where high and low refer to +1 standard deviation (SD) and −1 SD, respectively. As can be seen, lower reporting of challenging behaviours during times of low stress appears to be associated with better physical health scores. In contrast, when parents of children with intellectual disabilities reported high challenging behaviours in their children and perceived their stress to be high, they also reported poorer physical health. Social support was not significant in the equations nor did it interact with perceived stress.
Summary of hierarchical regressions predicting physical health problems in parents caring for children with intellectual disabilities.

Interaction between children’s challenging behaviours and perceived stress on physical health problem scores in parents caring for children with intellectual disabilities.
Discussion
The present study tested whether parents of children with intellectual disabilities would report poorer physical health problems compared to parents of typically developing children. As expected, these parents were found to report more physical health problems, and these were specific to the domains of sleep, headaches, gastrointestinal problems and respiratory infection episodes. In relating our results to the existing literature, they are somewhat consistent with other studies in parents caring for children with mixed disabilities (Lach et al., 2009; Raina et al., 2005); the health problems in these studies were more debilitating and chronic (e.g. asthma, arthritis). Although the type of disability was not disclosed, there is some consistency with one study that found a greater number of headaches, sleep complaints and backaches that were found in a sample of parents caring for children with disabilities compared to a control sample whose children were not disabled(Ha et al., 2011). There is also congruency with previous studies reporting higher sleep problems in parents with children with intellectual disabilities (Gallagher et al., 2010; Hedov et al., 2002) as well as poorer self-rated health (Allik et al., 2006); thus, our findings tend to resonate with the wider literature on family caregiving. Nonetheless, it must be acknowledged that the mean score of 57 on the PHQ reported by parents of children with intellectual disabilities is less than that seen in other stressful roles; Schat et al. (2005) evidenced a mean score of 69 across a range of health-care personnel when developing the PHQ.
More importantly, this study also found that parents of children with intellectual disabilities were less likely to rate their health as above average, and a higher percentage of these compared to control parents reported visiting their family physician for treatment of these physical health problems, 54 per cent versus 33 per cent, respectively. To our knowledge, this is the first study that has tested this particular relationship between reporting of physical health problems and increased consultations with general practitioners. The economic implications of this are quite obvious, but it must be acknowledged that roughly 75 per cent of patients report resolution or improvement of these types of problems within a few weeks of seeing a health-care provider (Kroenke, 2003); those symptoms most likely to persist are headaches, pain and musculoskeletal complaints.
This study also investigated whether perceived stress, social support and challenging behaviours would be associated with poorer physical health in parents caring for children with intellectual disabilities. Although the association between social support and physical health was in the expected direction, it was non-significant. Furthermore, there was no support for the stress-buffering hypothesis. One explanation for the lack of significance could be attributed to the scale used; in the present study, the scale focused on ‘perceived availability of emotional support’ and perhaps a scale such as the Family Support Scale (Dunst et al., 1984) that focused on ‘helpfulness of sources of support’ (e.g. formal and informal) may have been more appropriate in this context. It could also be that supportive respite services and not perceived support is what is most important for these particular parents. Another possibility is that our recruitment strategy was biased towards those already well connected through special need schools and family support groups, thus less connected families may be more isolated and have poorer health. Despite this, we found that perceived stress and child’s challenging behaviours were most predictive, and as hypothesized, the interaction between these two factors was significant. The negative consequences of increased stress on physical health found here are similar to that found elsewhere for other health indices in these parenting families (e.g. quality of life and chronic conditions) (Allik et al., 2006; Brehaut et al., 2004). Moreover, as in other ‘carer’ families (Lach et al., 2009; Raina et al., 2005), child’s challenging behaviours were associated with poorer physical health. Furthermore, in our subscale analyses on the challenging behaviour questionnaire, it was conduct problems that appeared to drive this negative association and this is congruent with our previous studies (Gallagher et al., 2009a) that found that greater reporting of conduct problems by these parents was associated with poorer immunity.
Interestingly, the interaction between perceived stress and child’s challenging behaviours explained an additional 6 per cent of the variance of physical health problems in parents caring for children with intellectual disabilities. Although associations between child’s challenging behaviours and parenting stress and well-being have been reported previously (Baker et al., 2003; Hastings and Beck, 2004), our findings add to the growing body of evidence linking these factors to the poor physical health seen in parents caring for children with intellectual disabilities. However, what is unique to the present study is that the association between perceived stress and poor physical health was moderated by children’s challenging behaviour. Here, we found that these negative effects were more pronounced when parents reported high challenging behaviours in conjunction with high stress, whereas low challenging behaviours and low stress appeared to be associated with better physical health. It is perhaps worth mentioning that the negative effects of challenging behaviour and stress are not only limited to self-report of health but they have also been linked to lower immune responses to medical vaccinations (Gallagher et al., 2009b) and poor neuroendocrine functioning (Seltzer et al., 2010) in these parents, two likely physiological mechanisms that may underlie these reported associations.
There are a number of study limitations that must be taken into account. First, the findings in this research are based on cross-sectional data; therefore, it is not possible to infer causation. For example, parents of children with intellectual disabilities who report more health problems may have done so even before the birth of their child or it could be that those who report poorer health are more likely to report higher stress and more child problem behaviours. Similarly, the association between stress and behaviour problems could be bidirectional and has been observed elsewhere (Baker et al., 2003). Thus, longitudinal designs may help with this issue. Second, most of the findings in this research rely on self-report from parents for the psychosocial, socio-demographic and physical health variables. Thus, this gives a subjective view of parents’ circumstances and relies on parents to be willing to reveal an accurate picture of the extent of their child’s problem behaviour or their health status for example (Lach et al., 2009). Clearly, this may not give an entirely representative account; however, these types of self-report measures are commonly used within caregiver research and have been shown to be reliable and valid (Gallagher et al., 2009a; Lach et al., 2009). Furthermore, we did try to elicit a more objective measure by asking parents whether they visited their physicians for treatment for these issues and this was significant and more pronounced in those caregiving families. Third, it is difficult to know what type of stressor was being perceived as most challenging as the PSS does not capture such data. Future studies could try and assess this in more detail. Fourth, our sample size may also be considered as small but these family caregivers are very time pressured and quite difficult to recruit. Fifth, there is the possibility of confounding due to unmeasured variables (e.g. financial status) that may be important in this context so caution is warranted when interpreting our results. Finally, our disability sample was a mixed syndrome group, thus it could be that different social and psychological factors are at play across disability subtypes. However, when we split this sample into parents of children with autism and mixed syndrome, there was no difference between the two groups on physical health scores (data not shown).
In summary, despite its limitations, this study has contributed to the literature and extended previous research. Importantly, it has demonstrated the potential risk for impaired physical health that these parents caring for children with intellectual disabilities have. Moreover, parents of children with intellectual disabilities were more likely to seek treatment for these physical health problems relative to control parents. Furthermore, our results showed stress and child challenging behaviours to be key determinants of physical health status in parents caring for children with intellectual disabilities. In particular, we found that child problem behaviour moderated the association between stress and self-reported physical health problems, but protective benefits were only observed when perceptions of the stress and behaviours were both low. Together these findings help to elucidate the dynamic influence of child’s characteristics and stress appraisal on physical health and underscore the importance for researchers to examine the precise components of these interactions (Miodrag and Hodapp, 2010). Moreover, this should inspire further research and influence the design of interventions, in particular, those that combine stress and behaviour management techniques that have been found to be most effective for improving well-being in these parents (Hastings and Beck, 2004). Indeed, in other family caring contexts, parents using positive reinterpretation by focusing on the positive aspects of the situation and finding meaning had greater reductions of depression and stress (Cheshire et al., 2010).
Footnotes
Acknowledgements
The authors would like to express their appreciation to North Staffordshire Carers Association, Autism West Midlands, and Lorna Shandley for their help with the recruitment process. They would also like to thank the Social Issues Reading Group at the University of Limerick, Ireland, for helpful comments on earlier drafts of this article. A special thanks is also extended to the parents caring for children with intellectual disabilities and the parents caring for typically developing children who made this research possible.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.