
Abstract
Marriage can enhance health for individuals with a chronic disease, yet spouses may also undermine disease management. The current study investigated spousal undermining of dietary regimen in 129 patients with type 2 diabetes mellitus. A total of 40 patients reported that their spouses tempted them with forbidden foods, and 15 reported that their spouses conveyed disregard for their diabetic diet. Spousal tempting was associated with worse dietary adherence, and spousal disregard with worse nondietary adherence. Spousal undermining is relatively rare but is associated with patients’ disease management and warrants further investigation to better understand how spouses influence partners’ day-to-day management of chronic diseases.
Social relationships are usually beneficial for health (Cohen, 2004; House et al., 1988). Broadly, being with others is associated with better health, even for individuals who are suffering from chronic illness. Because many of the activities of disease management occur in the context of interactions between spouses, the effects of marriage have been studied most extensively. Interactions with a spouse may be especially consequential for the management of illnesses, such as type 2 diabetes mellitus (T2DM), that require continuous attention to diet, exercise, and other health behaviors. Spouses have long been shown to be unique influences on health behaviors (Broman, 1993; Umberson, 1992). While social support from many sources can be beneficial for health, particularly among individuals with chronic disease, the spouse appears to be a particularly important source of health behavior support and influence (Baron et al., 2011; Falba and Sindelar, 2008; Gallagher et al., 2011; Homish and Leonard, 2008). Patients often report that spousal support is a key source of help for activities of disease self-management (Trief et al., 2003), and when partners are actively involved in patients’ health behavior, relationship satisfaction is higher (Schokker et al., 2010).
However, although spouses of individuals with chronic illnesses often facilitate patients’ day-to-day adherence to a treatment regimen by providing emotional and tangible support (Gallant, 2003), patients also report that actions by their spouses can contribute to problems with adherence (Garay-Sevilla et al., 1995). The marital relationship is a key source of health-enhancing support, but it can also be a source of health-damaging stress and interference (Vinokur and Vinokur-Kaplan, 1990). Such interference may take the form of undermining partners’ efforts to maintain or improve their health, either by encouraging unhealthy behaviors or by hindering healthy behaviors.
Undermining can come from a variety of sources, but the spouse may be the most important source (Cranford, 2004). Moreover, social support and undermining do not appear simply to be opposite ends of a continuum but are, rather, relatively independent constructs. However, spousal undermining has received limited attention thus far in the literature on chronic illness. This study sought to address that gap by examining the disease-management implications of spousal undermining of dietary adherence among older adults with T2DM.
Diabetes self-management, dietary adherence, and spousal undermining
Diabetes is a chronic, life-threatening condition in which an individual’s body cannot properly use insulin, a hormone that helps to regulate blood sugar levels (American Diabetes Association (ADA), 2011). The treatment of diabetes requires adherence to a stringent routine involving medication management, physiological monitoring, and commitment to nutrition and exercise plans. Maintaining strict adherence creates a considerable treatment burden for patients (Vijan et al., 2005), however, and adherence rates can be as low as 31 percent (Odegard and Capoccia, 2007). Dietary adherence, in particular, is one of the most difficult components of the diabetic regimen (Beverly et al., 2008). Because of the social aspect of eating (Gallant, 2003), dietary adherence may be more subject to social influences than other disease-management tasks. Family members are often integrally involved in meal planning and food choices, making it important to understand how patients’ dietary adherence is affected by the family context (Choi, 2009).
Unfortunately, family members’ reactions to patients’ dietary requirements are often cited as barriers to dietary adherence, and spouses, in particular, can hinder as well as facilitate dietary adherence among patients with diabetes (Beverly et al., 2008). Patients exhibiting poor glycemic control report receiving less family assistance with food preparation and experience greater family undermining of their diet, such as family members offering foods that are not on the diabetic meal plan (Brewer-Lowry et al., 2010; Chesla and Chun, 2005). Indeed, people with diabetes often report that it is difficult for them to maintain their own healthy diets when those around them are unwilling to make dietary changes (Gallant, 2003). In one study, the top-ranked barrier to dietary adherence was “being around people who are eating and drinking [prohibited] foods” (Wen et al., 2004: 987). Social occasions, such as birthday celebrations, and lack of support and understanding from the family, such as family members’ insistence on take-out food, have also been cited as barriers to proper nutrition for individuals with diabetes (Wong et al., 2005). Although existing evidence is scarce, it appears that undermining, whether intentional or not, is harmful to diabetes treatment adherence.
What constitutes spousal undermining?
A limitation of existing research is the lack of consensus regarding what constitutes undermining of another individual’s health behaviors. Undermining in the context of health behavior has been defined in a variety of ways, including the expression of negative affect or evaluations (Cranford, 2004; Vinokur and Vinokur-Kaplan, 1990), hindrance of an individual’s health goals (Cranford, 2004), nagging (Choi, 2009), denial of the seriousness of the illness, unhelpful or conflicting advice, and unwillingness of family members to change their diets (Gallant, 2003). Existing measures of spousal undermining are scarce, but some measures emphasize participants’ reports of how much their spouse annoys, criticizes, or otherwise acts in an unpleasant manner toward them (Vinokur and Vinokur-Kaplan, 1990; Westman et al., 2004). Other measures of undermining emphasize the extent to which spouses attempt to constrain their partner’s health behavior. In a study of smoking cessation, for example, undermining was assessed with items that included ratings of how often the spouse “Refuse[s] to let you smoke in the house” or “Ask[s] you to quit smoking” (Roski et al., 1996).
Construing and assessing undermining as behaviors by others that are critical or unpleasant do not necessarily capture the essence of undermining, as conceptualized in this study—attitudes or behaviors that subvert or weaken an individual’s goal pursuit, such as the goal of adhering faithfully to a prescribed treatment regimen. Similarly, undermining construed and assessed as nagging or pressure to improve a health behavior (e.g. to abstain from smoking) would capture behaviors intended to promote, rather than undermine, sound health behavior. While such nagging or pressure aimed at promoting sound health behavior might be aversive (cf. Franks et al., 2006; Lewis and Rook, 1999), it does not seem to reflect undermining per se. We believe that undermining should be construed as attitudes or behaviors that subvert or interfere with (rather than foster) an important goal, such as adherence to a treatment regimen. In the context of diabetes, therefore, undermining by others would be reflected in such behaviors as tempting (e.g. by offering an individual forbidden foods) and expressing disinterest in or disregard for the individual’s health-related goals (e.g. by ascribing lack of importance to the goals, denying the gravity of unhealthy behaviors, or ignoring the individual’s concerns about those goals). In this sense, undermining is similar to the concept of interpersonal hindrance of personal projects advanced by Ruehlman and Wolchik (1988).
The current study
The current study investigated the extent to which older adults with T2DM experience diet-related undermining by their nondiabetic spouse, such as the spouse tempting them to eat foods not on their diabetic diet or the spouse showing disregard for how well they follow their diabetic diet. We also examined whether spousal undermining was associated with the patients’ treatment adherence and glycemic control. We predicted that patients’ reports that their spouse tempts them with forbidden foods or that their spouse does not care how well they follow their diet would be associated with poorer dietary adherence and glycemic control. Additionally, although the primary focus of the study was adherence to the diabetic diet, we also examined patients’ adherence to nondietary aspects of their treatment regimen (such as exercising and checking their feet) in view of the importance of such adherence to patients’ overall disease management. It is plausible that adverse effects of diet-related undermining might spill over to nondietary aspects of the diabetic treatment regimen, perhaps by eroding the patients’ motivation to follow the treatment regimen. We accordingly predicted that patients’ reports of spousal undermining would be associated with worse nondietary adherence and worse dietary adherence. These hypotheses were examined, controlling for diet-related spousal support in adherence, to evaluate our assumption that spousal undermining exhibits associations with patient disease outcomes that are independent of low spousal support.
Method
Participants
The data for this study came from the baseline assessment of a larger three-wave study of spouses’ involvement in the disease management of older patients with T2DM. The participants were recruited through announcements in newspapers, radio stations, medical offices, diabetes education centers, and senior citizen centers. Interested individuals called a toll-free number and were screened for eligibility. Eligibility criteria included having a primary medical diagnosis of T2DM, being in a marriage or a marriage-like relationship with a partner who did not have diabetes, being 55 years or older, residing in the community, and having been recently advised by a primary care provider to make dietary improvements. Of 235 couples who were screened, 58 couples were not eligible (e.g. both partners had diabetes); among eligible couples, 48 declined to participate. The resulting sample consisted of 129 couples (258 individuals).
Half (50%) of the patients were female, and their mean age was 66 years (standard deviation (SD) = 7.71); 76.2 percent were White, 22.2 percent were African American, and 1.6 percent were of another ethnicity. The participants had a mean of 14 years of education, with 12.4 percent of patients having completed less than high school, 27.9 percent having completed high school, and 59.7 percent having completed education beyond high school. Couples had been married, on average, for 38 years.
Procedures
Couples were interviewed in their homes about their health, their diabetes management, and their interactions with their spouses regarding their diabetic regimen, particularly their diabetic diet. During the visit, a trained research assistant interviewed patients while the spouse completed self-report questionnaires in another room. After the patient interview was completed, the spouse was interviewed while the patient completed the self-report questionnaires. The current study examines patient data from the interviews and questionnaires and also from electronic daily diaries. Every evening for 24 days, patients recorded in an electronic diary how well they adhered to their diabetic diet as well as their blood glucose values for the day.
Measures
The in-person interviews, self-administered questionnaires, and electronic daily diaries included closed- and open-ended ended questions regarding the participant’s demographic characteristics and health status, emotional health, adherence to the diabetic regimen, and perceptions of the spouse’s involvement in the diabetic diet. All instruments and procedures were approved by a university Institutional Review Board. Statistical analyses were completed using the SPSS 18 (SPSS; Chicago, IL) statistical package. A complete description of study procedures can be found in Stephens et al. (in press).
Spousal undermining
Spousal undermining was assessed using three items that were part of a larger set of items that assessed spousal involvement in the patient’s management of his or her diabetic diet. Specifically, patients were asked how often during the past month their spouse had “Tempted you to eat foods not on your diabetic diet,” “Showed that (s)he does not care about how well you follow your diabetic diet,” and “Showed that (s)he does not think your diabetic diet is important.” Ratings were made on a 5-point scale (1 = not at all, 2 = once or twice, 3 = once a week, 4 = several times per week, or 5 = every day). The items were not strongly intercorrelated (all rs < .50) and appeared to capture two different aspects of spousal undermining: interference via offering proscribed foods and disregard for the patient’s dietary adherence. Disregard was best captured by the item indicating that the spouse did not care how well the patient followed the diabetic diet; reports that the spouse showed that the diabetic diet was unimportant were rare. To reduce the number of analyses, spousal undermining was assessed using the two most frequently endorsed items that reflected spousal tempting and disregard.
Adherence to the diabetic diet
Given the importance of dietary adherence to the day-to-day management of T2DM (Centers for Disease Control and Prevention (CDC), 2011) and given that diabetic patients find dietary adherence to be especially difficult (Daly et al., 2009; Woodcock and Kinmonth, 2001), we obtained daily assessments of patients’ dietary adherence. The patients reported on their dietary adherence in the electronic daily diary at the end of each day, responding to five items adapted from the diet subscale of the Summary of Diabetes Self-Care Activities Measure (SDSAM; Toobert et al., 2000). The participants rated the extent (1 = not at all, 2 = somewhat, or 3 = very much) to which they had made unhealthy choices during the day that got them off-track with their diabetic diet (reverse-coded); followed a healthful eating plan; ate five or more servings of fruits and vegetables; avoided high-fat foods, such as red meat or full fat dairy products; and spaced carbohydrates evenly throughout the day. These items were averaged to create a composite measure of mean daily dietary adherence (Cronbach’s α = .74).
Adherence to nondietary aspects of the diabetic regimen
Adherence to nondietary aspects of the diabetic regimen was assessed with four items in the baseline interview that asked patients to report on how many days during the preceding week (0–7 days) they had taken their recommended diabetes medications or injections, had participated in at least 30 minutes of continuous physical activity, had tested their blood sugar the number of times recommended by their health-care provider, and had checked their feet. These items were weakly intercorrelated (all rs < .16), a common occurrence when diverse health behaviors are examined (Newsom et al., 2005), including different facets of diabetes self-care (Toobert et al., 2000). In such cases, composite scales, nonetheless, provide meaningful information about the extent to which individuals are engaging in health-enhancing behaviors (Newsom et al., 2005). Accordingly, we averaged the four items to create a composite measure of nondietary adherence.
Glycemic control
Patients recorded their blood sugar readings for the day in the daily diary, up to a maximum of seven possible readings. The mean number of blood sugar readings per day in this sample was 1.80 (SD = 1.33). Blood glucose values were averaged within each day, and these estimates were averaged across days to create a measure of the average blood sugar level for the 24-day assessment period.
Covariates
Variables that are commonly controlled in psychosocial research on patients with T2DM, as well as variables that could plausibly affect either spousal undermining or adherence, were included as covariates in the current study. These variables included the patient’s sex (0 = male and 1 = female), age, race (0= non-White and 1 = White), depressive symptoms, and marital satisfaction. Depressive symptoms were assessed with the 20-item Center for Epidemiologic Studies–Depression Scale (CES-D; Radloff, 1977). Sample items included “I felt depressed” and “I felt that everything I did was an effort.” Items were rated on a 4-point scale that reflected how often in the past week the participant had felt that way (0 = rarely or none of the time (less than 1 day) to 3 = most of the time (5–7 days)]. The items were summed, consistent with Radloff’s scoring procedure, to create a composite measure of depressive symptoms (Cronbach’s α = .906). The patients’ marital satisfaction was assessed with five items from the Quality of Marriage Index (QMI; Norton, 1983). Sample items included “you have a good marriage” and “your relationship with your husband/wife makes you happy.” Items were rated on a 7-point scale (1 = strongly disagree to 7 = strongly agree) and were averaged to yield a composite measure of marital satisfaction (Cronbach’s α = .87).
In addition, support provided by the spouse for the patients’ dietary adherence was included as a covariate to rule out the possibility that effects of spousal undermining might reflect low levels of spousal support for adherence. Spousal support for the patient’s dietary adherence was assessed with three interview items that asked the extent to which the spouse had done something to help the patient stick with the diabetic diet, had shown appreciation for the patient’s efforts to stay on track with the diet, or had shown that (s)he understands the importance of the patient following a healthy meal plan. Ratings were made on a 3-point scale (0 = not at all, 1 = somewhat, or 2 = very much) and were averaged to create a composite measure of spousal support for dietary adherence (Cronbach’s α = .71).
Results
Preliminary analyses
Enrolled patients had been diagnosed with diabetes for an average of 11.73 years (SD = 9.41 years; range = 1–40). Most patients were taking medication to control their diabetes: 102 (79.1%) were taking oral medication, 47 (36.4%) were taking insulin, and 33 (25.6%) were taking both oral medication and insulin. Additionally, 86 (66.7%) were experiencing some diabetes complications, while only 43 (33.3%) had no complications. The patients reported a mean blood glucose level of 130.91 (SD = 25.25; range = 80.08–234.42).
Types and frequency of spousal undermining behaviors
Descriptive statistics and intercorrelations between key study variables are shown in Table 1. Spousal undermining behaviors were reported relatively infrequently, tempting the patient with proscribed food occurred more often in this sample (M = 1.43, SD = 0.78) than did spousal communication of disregard for the patient’s adherence to the diabetic diet (M = 1.19, SD = 0.61; paired t = 3.55, p = .001). These means reflect an average frequency of less than once or twice a month. Indeed, only 10 patients (7.8%) reported that their spouse tempted them to eat forbidden foods once a week or more, and only 6 patients (4.7%) reported that their spouse indicated that they did not care about adherence to the diabetic diet once a week or more. Among those patients who did experience spousal undermining, the incidence of perceived tempting (M = 3.60, SD = 0.70) was similar to that of spousal disregard (M = 3.67, SD = 0.52).
Means, standard deviations, and intercorrelations for the study variables.
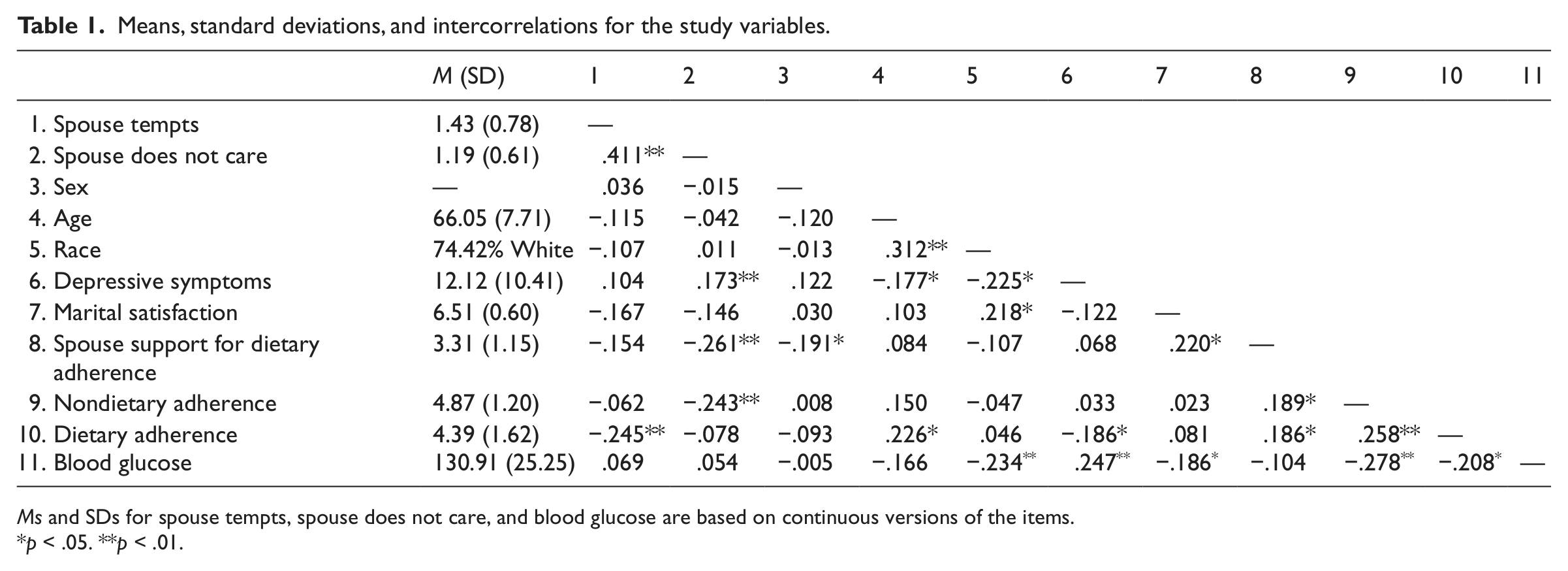
Ms and SDs for spouse tempts, spouse does not care, and blood glucose are based on continuous versions of the items.
p < .05. **p < .01.
Because spousal undermining was relatively rare, subsequent analyses (unless otherwise indicated) were conducted with dichotomized versions of the items (0 = no undermining or 1 = undermining occurred once or more in the last month). Overall, 40 patients (31.0%) reported that their spouses had tempted them with proscribed foods, and 15 patients (11.6%) reported that their spouses had indicated that they did not care about the patient’s adherence to the diabetic diet.
Perceptions of spouse tempting were moderately correlated with perceptions that the spouse does not care about the patient’s dietary adherence. Additionally, tempting was correlated with worse dietary adherence. Spousal disregard for adherence was associated significantly with less perceived support for adherence and worse nondietary adherence.
Is spousal undermining associated with worse disease management?
We hypothesized that more frequent spousal undermining would be associated with worse treatment adherence. Two multiple regression analyses were conducted in which dietary adherence and nondietary adherence were regressed on the two forms of spousal undermining (spousal tempting with proscribed foods and spousal disregard of the patient’s dietary adherence) and covariates (sex, age, race, depressive symptoms, marital satisfaction, and spousal support for dietary adherence support). The results indicated that, adjusting for the covariates, spousal disregard for the patient’s dietary adherence—but not spousal tempting with proscribed foods—was associated with worse nondietary adherence (see Table 2, left panel). In contrast, spousal tempting—but not spousal disregard—was associated with worse dietary adherence (see Table 2, right panel). 1
Association between spouse undermining and adherence to nondietary and dietary aspects of the diabetic regimen.
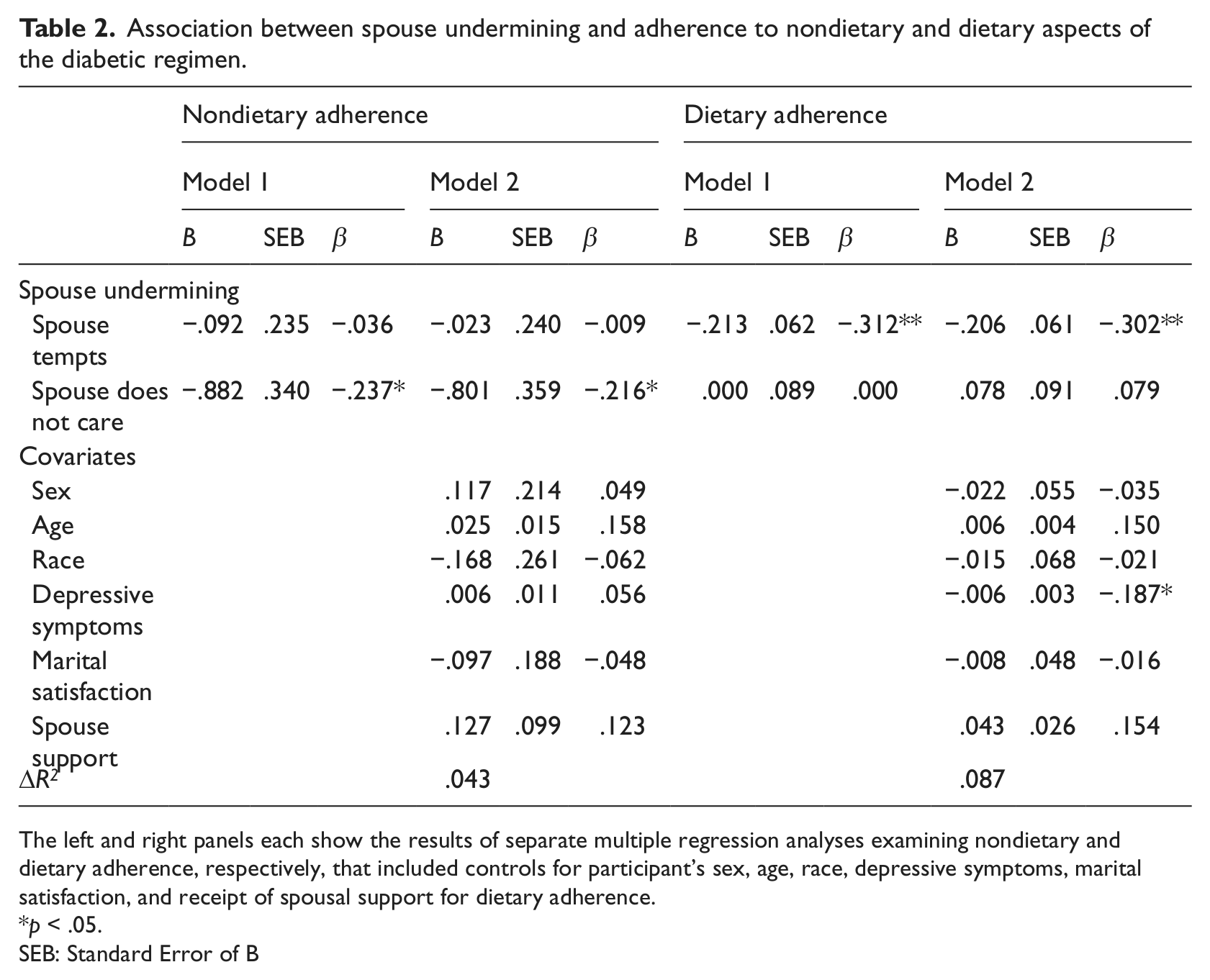
The left and right panels each show the results of separate multiple regression analyses examining nondietary and dietary adherence, respectively, that included controls for participant’s sex, age, race, depressive symptoms, marital satisfaction, and receipt of spousal support for dietary adherence.
p < .05.
SEB: Standard Error of B
We then examined whether spousal tempting was associated with an increased risk of having an average blood sugar level at or above 130 mg/dL. The results of the logistic regression analysis indicate that, controlling for the covariates, patients who reported experiences of spousal tempting were more than twice as likely to have an average blood glucose level above the ADA’s (2011) recommended range but only at a marginal level of significance (odds ratio (OR) = 2.023, p = .074). 2 Spousal disregard was not significantly associated with blood glucose levels.
Discussion
Spouses’ involvement in their partner’s management of a chronic illness has the potential to benefit the partner’s illness adaptation, treatment adherence, and disease outcomes. Spouses also have the potential to be unhelpful, however, undermining rather than facilitating their partner’s illness management. Little research has examined spousal undermining in the context of chronic illness, and the current study sought to address that gap in knowledge by investigating spousal undermining in the context of T2DM.
The findings suggested that spousal undermining of their partners’ efforts to follow a diabetic treatment regimen took two different, albeit moderately correlated, forms, each with distinctive implications for patients’ adherence and glycemic control. First, some spouses appeared to convey a lack of concern for the patient’s dietary adherence. Such apparent lack of concern was associated with worse adherence by their partners, although it was adherence to nondietary aspects of the treatment regiment, rather than adherence to the diet, that exhibited this association. This particular pattern was not expected, and it may reflect aspects of spousal disregard that we did not assess. For example, it is possible that spouses who conveyed disregard for their ill partner’s diabetic diet expressed similar attitudes about other diabetes-related behaviors, such as checking feet or exercising, although our data do not allow us to evaluate this possibility. It is also possible that spouses’ disregard for their partner’s disease management may reflect the spouses’ frustration with ill partners who exhibit poor adherence to the diabetic regimen. Spouses might feel particularly frustrated, for example, if their partners are unwilling to adhere to nondietary aspects of the diabetic regimen because nondietary behaviors are generally regarded by patients as less difficult than dietary behaviors (Clark and Asimakopoulou, 2005). Regardless, expressing disregard about a partner’s illness regimen appears to represent a passive form of undermining, and such dismissiveness may unravel collaborative resources in the spousal relationship and work against the patient’s disease-management goals.
For other spouses, undermining took the form of tempting patients with foods that were proscribed in the diabetic diet. Tempting was associated with worse dietary adherence and, marginally, with worse glycemic control. The motivations that underlie tempting may be varied, and less uniformly dismissive, than those that underlie disregard. For example, spouses who offer forbidden food may do so to cheer the patient or to include the patient in family meals and celebrations (Chesla and Chun, 2005; Wong et al., 2005). While some spouses may have more insidious motives in offering their ill partners forbidden food and many may have benevolent motives, and, as a result, tempting may not erode the sense of collaboration between partners.
Finally, the study findings emerged in analyses that controlled for patient age, sex, race, depressive symptoms, marital satisfaction, and spousal support for adherence. Associations between spousal undermining and patients’ adherence and glycemic control do not appear, therefore, to be an artifact of poor marital quality or depressive symptoms. Moreover, the effects of spousal undermining do not appear to be conflated with low spousal support.
Limitations and future directions
Several study limitations should be considered in taking stock of the study findings. First, our measures of spousal undermining were based on single-item assessments. These single-item measures performed reasonably well in the current study in that they exhibited significant associations with patient outcomes and were found to be distinct from spousal support for dietary adherence. Nonetheless, future research would benefit from multi-item assessments that capture various forms of spousal undermining and that avoid overlap with other types of spousal involvement in patients’ disease management. Second, respondents in the present study only indicated the frequency with which they perceived that their spouse engaged in undermining during the past month. Some spouses who tempt their partners with proscribed foods or who disregard their partner’s dietary needs may do so persistently, however, and future research would benefit from longitudinal methods to assess the pattern of undermining characteristic of such couples. Third, our data do not allow us to determine what kinds of behaviors or attitudes exhibited by the spouses led patients to endorse perceptions of tempting or disregard for their diabetic diet. Some spouses may engage in quite explicit undermining—– repeatedly offering off-diet foods to the patient despite their objections or remarking plainly that they do not care about the patient’s dietary needs—other spouses, in contrast, may engage in less explicit undermining—repeatedly consuming proscribed food in the presence of the patient or ignoring the patient’s concerns about adhering to their treatment regimen. The development of future measures of undermining might benefit from initial qualitative assessments of spouse behaviors that patients regard as working against their health goals and their successful disease self-management.
The cross-sectional analyses in the current study did not allow us to identify the temporal sequences that may link spousal undermining to poor patient outcomes. It is possible, for example, that spouses’ expressions of disregard of their partner’s dietary adherence are the result, not the cause, of problematic adherence, perhaps reflecting spouse fatigue and disengagement from ill partners who persistently fail to adhere to the diabetic regimen. Process-oriented longitudinal studies with more detailed assessments of spousal undermining would help to shed light on the triggers and consequences of such undermining. Finally, the sample was relatively homogeneous and was focused on one chronic disease, which limits generalizability to other populations and disease contexts (cf. August and Sorkin, 2011; Hessler et al., 2012). Marital satisfaction was also relatively high (M = 6.51; range = 1–7) in this sample, which may have played a role in the rather low rates of spousal undermining that were observed. Future studies with more diverse samples, including samples that reflect other disease contexts and a broader range of marital satisfaction, might be likely to yield higher rates, and possibly more potent forms, of spousal undermining.
Conclusion
Despite these limitations, the current study has begun to extend our understanding of the implications of spousal undermining for patients’ efforts to manage a chronic disease. We found evidence of two different forms of spousal undermining, which exhibited distinctive associations with patient outcomes, and which could potentially inform interventions for patients with diabetes and their families (cf. Barrera et al., 2006; Serlachius et al., 2012). Even though the frequency of spousal undermining was relatively low, it was related to worse adherence and worse glycemic control. Thus, although spouses have been found to be uniquely important sources of health-related support (Cranford, 2004; Gallant, 2003), they are also in a unique position to undermine patients’ disease-management efforts, making it important to learn more about spouses’ unhelpful as well as helpful transactions with chronically ill partners.
Footnotes
Funding
This research was supported by grant R01 AG24833 from the National Institute on Aging, entitled “Mind-Body Interactions in Management of Type 2 Diabetes.”