
Abstract
Generalized anxiety disorder prevalence and comorbidity with depression in coronary heart disease patients remain unquantified. Systematic searching of Medline, Embase, SCOPUS and PsycINFO databases revealed 1025 unique citations. Aggregate generalized anxiety disorder prevalence (12 studies, N = 3485) was 10.94 per cent (95% confidence interval: 7.8–13.99) and 13.52 per cent (95% confidence interval: 8.39–18.66) employing Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria (random effects). Lifetime generalized anxiety disorder prevalence was 25.80 per cent (95% confidence interval: 20.84–30.77). In seven studies, modest correlation was evident between generalized anxiety disorder and depression, Fisher’s Z = .30 (95% confidence interval: .19–.42), suggesting that each psychiatric disorder is best conceptualized as contributing unique variance to coronary heart disease prognosis.
Introduction
Major depressive disorder (MDD) is the most commonly researched internalizing/emotional disorder in coronary heart disease (CHD) patients. Previous meta-analyses indicate that MDD and depression symptoms confer greater CHD morbidity risk (Barth et al., 2004; Nicholson et al., 2006), culminating in the American Heart Association advocating routine depression screening among these patients (Lichtman et al., 2008). However, the fact that depression screening and intervention have only translated to a modest impact on cardiovascular outcomes (Baumeister et al., 2011; Pizzi et al., 2011) suggests that what is understood about the MDD–CHD link is in the nascent stages and incomplete. Recent findings also indicate that other emotional constructs such as anxiety and negative affect, in particular, increase CHD risk, raising the possibility that MDD is not a discrete psychiatric risk factor for CHD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Phillips et al., 2009; Scherrer et al., 2010; Tully et al., 2011). In fact, the extent to which the recent CHD prognostic findings reflect unique depression variance, independent from anxiety and negative affect, remains largely unchallenged. Quantifying the degree of comorbidity between MDD and anxiety disorders in CHD can help inform whether these disorders contribute independent variance to cardiovascular prognosis or, alternatively, whether the co-occurrence of disorders largely reflects common variance (e.g. negative affect, shared diagnostic symptoms and artificial diagnostic splitting). Although the extent of overlap between psychosocial constructs in CHD has long been highlighted as crucial to define (Kubzansky et al., 2006; Kubzansky and Kawachi, 2000; Smith, 2010); Suls and Bunde, 2005; Tully et al., 2008), we are not aware of a previous study to pool such data together and thereby quantify the association between depression and anxiety in CHD patients.
Among all psychiatric disorders, generalized anxiety disorder (GAD) is the most commonly comorbid disorder with MDD, both concurrently and across the lifespan, among individuals primarily free from CHD (Krueger, 1999; Sherbourne et al., 1996; Watson, 2009). In fact, in primary care settings over half of unipolar MDD, cases are comorbid with GAD (Sherbourne et al., 1996), so much so that scholars have long debated whether these even form separate diagnostic and clinical disorders (Mennin et al., 2008). Explanations for high comorbidity between GAD and MDD include shared diagnostic criteria (i.e. fatigability, restlessness/psychomotor agitation, concentration and sleep difficulties) (American Psychiatric Association, 2000), common genetic factors and common diathesis (Mineka et al., 1998) and related cognitive processes such as rumination and worry (Brosschot et al., 2006; Soo et al., 2009). For these reasons, GAD would serve as a suitable diagnostic exemplar to determine the extent to which depression shares variance with anxiety among CHD patients.
The dilemmas imposed by the overlap between depression and GAD are exemplified further in recent aetiological and prognostic studies. Recent research generally supports that MDD is associated with CHD, though largely contrasting results have been reported for GAD. For example, a recent epidemiological survey of 43,093 US civilians showed that the largest psychiatric association with physician diagnosed cardiovascular disease was attributable to GAD, as opposed to any other affect or mood disorder (adjusted odds ratio (OR): 1.83; 95% confidence interval (CI): 1.39–2.39) (Goodwin et al., 2009). Some studies have suggested that GAD is associated with cardiovascular outcome independent of MDD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Phillips et al., 2009; Tully et al., 2011) and another dataset reported reduced cardiovascular risk attributable to GAD (Parker et al., 2011), raising the possibility that these psychiatric disorders are highly collinear in CHD. Given that the degree of interrelation between GAD and MDD in CHD patients and the overall prevalence of GAD are not known, a critical gap is evident with respect to interpretation of the extant literature, particularly aetiological and prognostic studies.
Only by identifying the prevalence of GAD and the comorbidity rates between GAD and MDD will the extent of potential confounding variance in the MDD–CHD association be known. If comorbidity between GAD and MDD is small, then both GAD and MDD might best be conceptualized as discrete psychiatric risk factors in CHD. This, in turn, could feasibly redirect psychosocial research and interventions towards treatments tailored towards the phenotypic processes and biobehavioural mechanisms that confer CHD risk, beyond simply depression. Conversely, if high comorbidity rates were evident, research and intervention efforts may facilitate a shift away from disorder-specific treatments towards transdiagnostic approaches targeting common and modifiable vulnerability risk factors for depression and anxiety in CHD (Barlow et al., 2011; Dozois et al., 2009). Therefore, the purpose of this systematic review was to quantify the prevalence of GAD in CHD and comorbidity with MDD with two study aims:
What is the prevalence of GAD in populations with verified CHD?
What are the current comorbidity rates between depression disorders and GAD in populations with verified CHD?
Methods
Literature search
Using standardized criteria (Stroup et al., 2000), one systematic search of the Medline, Embase, SCOPUS and PsycINFO electronic databases was performed for English language studies or unpublished doctoral dissertations, reporting the prevalence of GAD in CHD or comorbidity rates with depression published between January 1975 and May 2011. Free text searches without language restrictions included the term GAD in combination with CHD, cardiovascular disease, heart disease, ischaemic heart disease, myocardial infarction (MI), cardiac death, coronary artery bypass graft (CABG), percutaneous coronary intervention, angioplasty and heart failure. These cardiac search terms were then combined with ‘anxiety’ and several common structured diagnostic interview tools: Anxiety Disorder Interview Schedule (ADIS), Composite International Diagnostic Interview (CIDI), Diagnostic Interview Schedule (DIS), MINI International Neuropsychiatric Interview (MINI) and Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R) (SCID).
Selection criteria
Eligibility criteria were established before the literature search. Editorial, letter, case report, conference abstract or qualitative reviews were excluded. Studies with post-stroke, cerebrovascular accident populations, heart transplant and mitral valve prolapse populations were also excluded, unless CHD patients were reported separately. Only studies with more than 50 patients were included to provide reliable prevalence and comorbidity estimates and sufficient power for studies. Studies were eligible for inclusion if the sample showed physician verified or documented CHD (e.g. positive stress test, coronary atherosclerosis, MI and coronary revascularization procedure) or end-stage heart failure. Studies employing only self-report CHD diagnosis/symptoms were ineligible.
Diagnosis of GAD and MDD (current and lifetime) was derived from either structured interview or self-report with the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1987, 2000, 2010) and International Classification of Diseases-10 (ICD-10; World Health Organization, 2007) criteria, or documented with relevant codes corroborated by a physician in medical records. Non-current International Classification of Disease codes for ‘anxiety states’ and ‘anxiety neurosis’ were not searched for and were excluded.
Data extraction
The two authors independently reviewed articles for eligibility. In the case of title/abstract disagreements, the study was subjected to full-text review. Additional studies were identified by inspection of the reference section of articles selected for full-text review. Disagreements were resolved by discussion. The quality of studies was not rated because there are no agreed upon measures of study quality, and the use of subjective rating scales may lead to bias (Petitti, 1994). Standardized data were extracted for each study including authors and citation, sample size, CHD sample characteristics, country, age (mean (M), standard deviation (SD)) and percentage female sex, GAD criteria, current and lifetime GAD prevalence, GAD and MDD comorbidity rates. Like other meta-analyses (Hackett et al., 2005), articles were judged to be from the same cohort if there was evidence of overlapping study dates, recruitment sites and similar study sample characteristics and grant funding numbers. In the case of multiple reports for the same sample, the study with the most comprehensive data and largest sample was retained.
Search results
Figure 1 displays the flow chart for exclusion and selection of studies. Table 1 describes the characteristics of the included studies reporting GAD prevalence and CHD outcomes in CHD. From 1025 unique citations, 934 were excluded by title/abstract (Kappa agreement = .91). Among 91 subjected to full-text review, in addition to 15 identified by manual searching, a further 94 were excluded. A total of 12 studies were retained that reported GAD prevalence and seven of these also reported comorbidity with MDD.
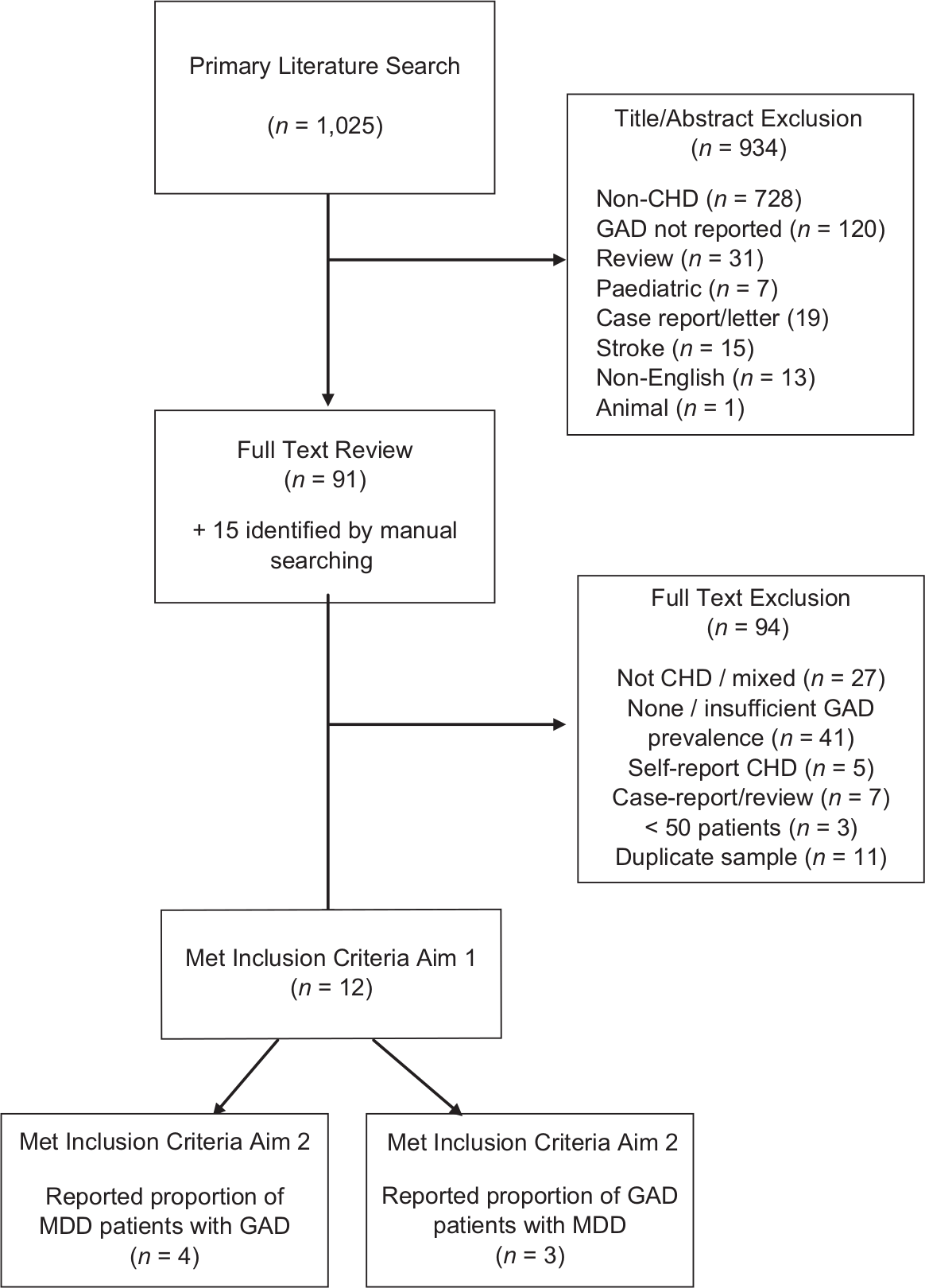
Flow chart of selected studies.
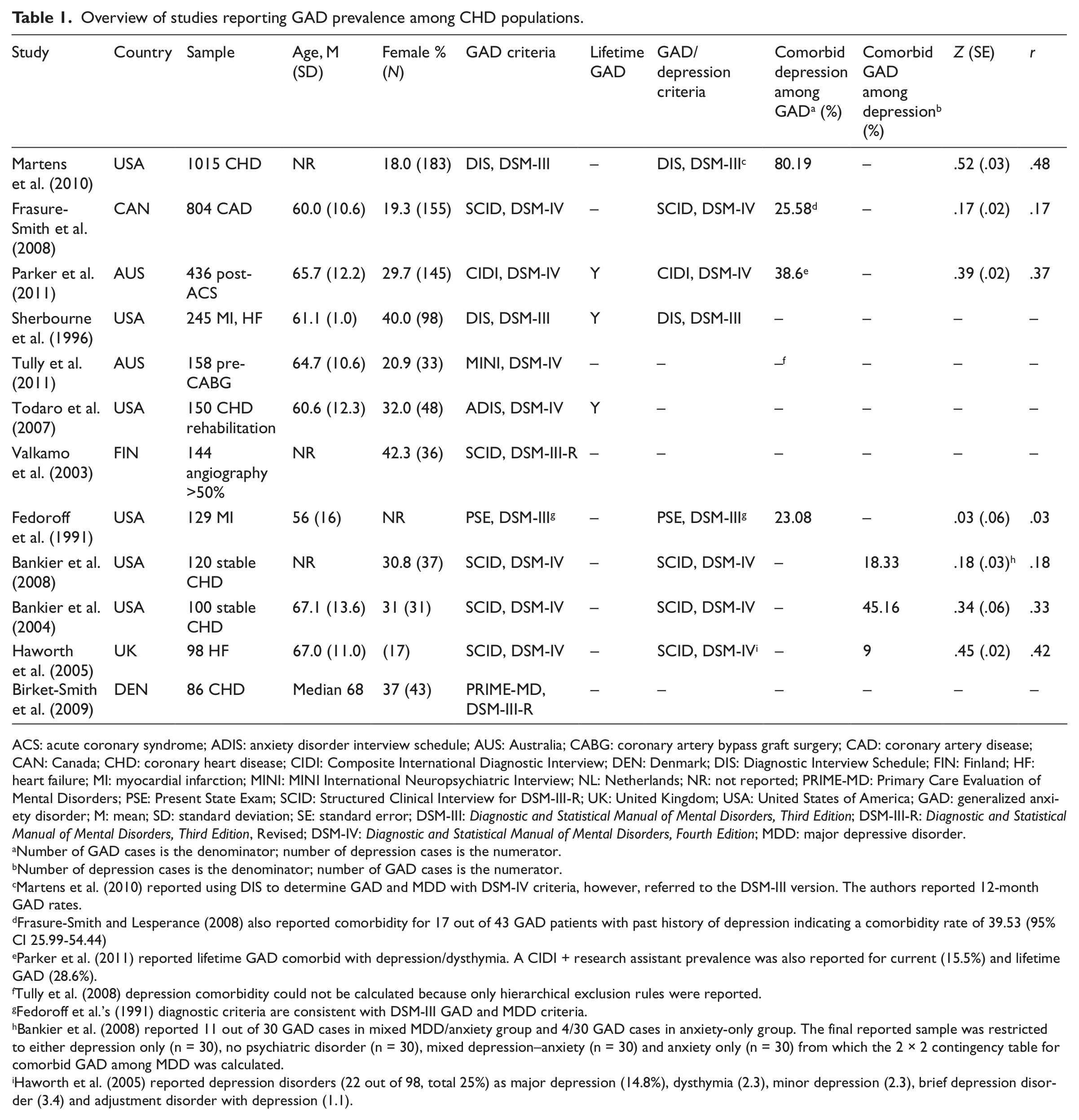
Overview of studies reporting GAD prevalence among CHD populations.
ACS: acute coronary syndrome; ADIS: anxiety disorder interview schedule; AUS: Australia; CABG: coronary artery bypass graft surgery; CAD: coronary artery disease; CAN: Canada; CHD: coronary heart disease; CIDI: Composite International Diagnostic Interview; DEN: Denmark; DIS: Diagnostic Interview Schedule; FIN: Finland; HF: heart failure; MI: myocardial infarction; MINI: MINI International Neuropsychiatric Interview; NL: Netherlands; NR: not reported; PRIME-MD: Primary Care Evaluation of Mental Disorders; PSE: Present State Exam; SCID: Structured Clinical Interview for DSM-III-R; UK: United Kingdom; USA: United States of America; GAD: generalized anxiety disorder; M: mean; SD: standard deviation; SE: standard error; DSM-III: Diagnostic and Statistical Manual of Mental Disorders, Third Edition; DSM-III-R: Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; MDD: major depressive disorder.
Number of GAD cases is the denominator; number of depression cases is the numerator.
Number of depression cases is the denominator; number of GAD cases is the numerator.
Martens et al. (2010) reported using DIS to determine GAD and MDD with DSM-IV criteria, however, referred to the DSM-III version. The authors reported 12-month GAD rates.
Frasure-Smith and Lesperance (2008) also reported comorbidity for 17 out of 43 GAD patients with past history of depression indicating a comorbidity rate of 39.53 (95% CI 25.99-54.44)
Parker et al. (2011) reported lifetime GAD comorbid with depression/dysthymia. A CIDI + research assistant prevalence was also reported for current (15.5%) and lifetime GAD (28.6%).
Tully et al. (2008) depression comorbidity could not be calculated because only hierarchical exclusion rules were reported.
Fedoroff et al.’s (1991) diagnostic criteria are consistent with DSM-III GAD and MDD criteria.
Bankier et al. (2008) reported 11 out of 30 GAD cases in mixed MDD/anxiety group and 4/30 GAD cases in anxiety-only group. The final reported sample was restricted to either depression only (n = 30), no psychiatric disorder (n = 30), mixed depression–anxiety (n = 30) and anxiety only (n = 30) from which the 2 × 2 contingency table for comorbid GAD among MDD was calculated.
Haworth et al. (2005) reported depression disorders (22 out of 98, total 25%) as major depression (14.8%), dysthymia (2.3), minor depression (2.3), brief depression disorder (3.4) and adjustment disorder with depression (1.1).
Additional data from personal communication
The lead authors of some studies were contacted if required using the provided contact e-mail address. No response was received from the authors of one study (Bankier et al., 2008) who reported GAD prevalence results of 120 patients from a total recruited sample of 143. The GAD prevalence and MDD comorbidity rate were thus derived from the reported cohort of 120. A broad ‘all anxiety disorder’ category was reported in some studies. As the original GAD prevalence data in well-defined CHD groups could not be provided, these studies were excluded.
Statistical analyses
The Mix 1.7 software was employed for data analyses (Bax et al., 2006b); a software description was reported by Bax et al. (2006a, 2007). The summation of current and lifetime prevalence estimates was reported as the proportion of GAD patients within the total CHD sample. Aim 2 data were reported by describing the comorbidity between GAD and MDD (proportion of GAD patients with depression) and the comorbidity between MDD and GAD (proportion of depressed patients with GAD). Aim 1 and Aim 2 prevalence data were reported as proportions with 95 per cent CI calculated via the Wilson score method without continuity correction (Newcombe, 1998). To report GAD and MDD comorbidity rates, the r value was calculated (Rutledge and Loh, 2004), and then a standardized conversion to Fisher’s Z with standard error was applied (Field, 2001). Correlation effect sizes can be interpreted according to Cohen’s criteria (Cohen, 1992): small < .10, medium = .10 to <.30, large = .30 to .50. Heterogeneity statistics were evaluated; I2 > 50 per cent in fixed-effects analyses represents considerable heterogeneity, while in random effects models, when τ2 approaches zero, there is no homogeneity (Tak et al., 2010). When Aim 1 and 2 data were pooled together with a fixed-effects model, the inverse variance approach was selected. In the random effects models for Aim 1–Aim 2 data, the DerSimonian–Laird method (1986) was employed to provide a more conservative estimate of effect size (Tak et al., 2010). To evaluate the presence of publication bias, the fail-safe N was reported, along with Begg and Mazumdar’s (1994) and Egger et al.’s (1997) tests.
Results
GAD prevalence in CHD
There were 12 studies (total N = 3485) reporting GAD prevalence among populations with documented CHD. The Heart and Soul study recruited the largest sample, reporting GAD prevalence among 1015 stable CHD patients (Martens et al., 2010). A Canadian study recruited 804 stable coronary artery disease (CAD) patients (Frasure-Smith and Lesperance, 2008). An Australian study performed structured interviews 4 days after acute coronary syndrome among 436 patients (Parker et al., 2011). A primary care sample reported GAD prevalence rates for 245 patients with MI or heart failure (Sherbourne et al., 1996). Others reported prevalence among CHD patients attending cardiac rehabilitation (Todaro et al., 2007), an outpatient cardiology clinic (Bankier et al., 2008) and coronary angiography >50 per cent stenosis (Valkamo et al., 2003). The only CABG surgery study performed structured interview before surgery (Tully et al., 2011). Another report compared MI patients with stroke and spinal cord lesions, reporting MI patients separately (Fedoroff et al., 1991). The smallest studies were among 100 CHD patients (Bankier et al., 2004), 98 heart failure patients with left ventricular systolic dysfunction (Haworth et al., 2005) and 86 CHD outpatients (Birket-Smith et al., 2009).
When pooling the GAD prevalence data together, there was evidence of heterogeneity (I2 = 89.17%). When a random effect model was specified, the pooled GAD prevalence was 10.94 per cent (95% CI: 7.8–13.99; z = 7.01, p < .0001; τ2 = .0024), data shown in Figure 2. The fail-safe N statistic indicated that an additional 1051 missing studies would be required to bring the p value from .00 to .05. Neither Begg and Mazumdar’s nor Eggar’s test supported the evidence of publication bias. A sensitivity analysis was performed excluding the studies adopting DSM-III-R or earlier criteria. Again, there was evidence of heterogeneity (I2 = 90.09%), and a random effects model from seven prevalence studies supported a 2 per cent higher prevalence and 13.52 per cent pooled prevalence (95% CI: 8.39–18.66; z = 5.16, p < .0001; τ2 = .004). There was no evidence of publication bias from Begg and Mazumdar’s and Eggar’s test. The fail-safe N statistic indicated that an additional 394 missing studies would be required to bring the p value from .00 to .05.
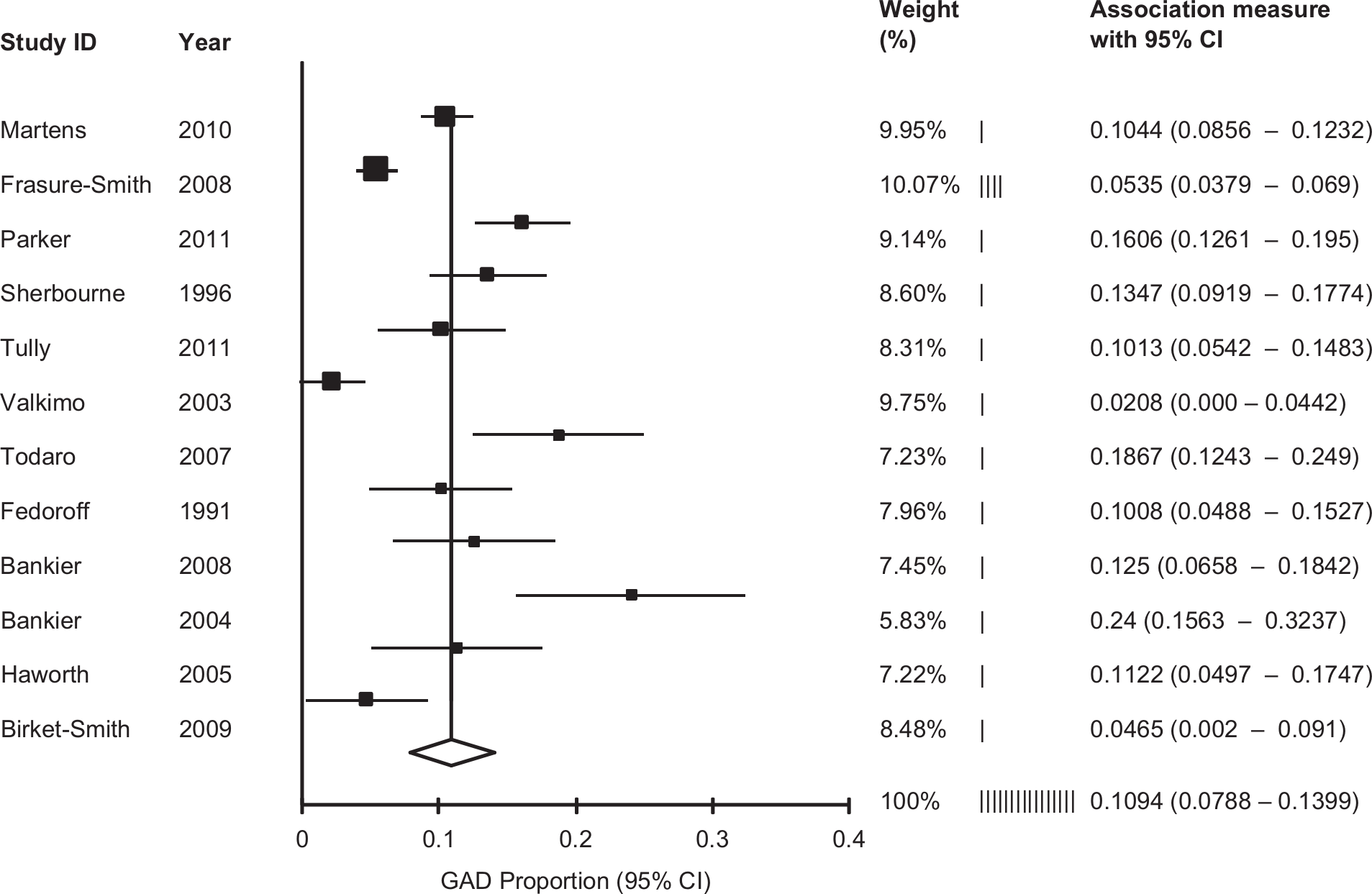
Forest plot of generalized anxiety disorder prevalence in CHD (random effects).
Lifetime GAD prevalence
Three studies reported lifetime GAD in CHD, and the combined N was 884 patients (Parker et al., 2011; Sherbourne et al., 1996; Todaro et al., 2007). Due to heterogeneity (I2 = 60.89%), a random effects model was specified and showed that the pooled lifetime GAD prevalence was 25.80 per cent (95% CI: 20.84%–30.77%; z = 20.67, p < .001; z = 10.19, p < .0001; τ2 = .0012). There was no evidence of publication bias from Begg and Mazumdar’s or Eggar’s test, and the fail-safe N statistic indicated that an additional 216 missing studies would be required to bring the p value from .00 to .05.
Pooled comorbidity results for depression and GAD in CHD
There were seven studies where the comorbidity between MDD and GAD could be calculated (N = 2702). One study provided comorbidity rates among a subsample of patients, but not the total recruited sample (Bankier et al., 2008). As there was evidence of heterogeneity (I2 = 97.20%), comorbidity data were pooled together in a random effects model, and this model suggested a modest association between MDD and GAD, Fisher’s Z = .30, 95 per cent CI: .19–.42; z = 5.11, p < .001; τ2 = .0228), data shown in Figure 3. There was no evidence of publication bias. The fail-safe N indicated that an additional 1861 missing studies were required to bring the p value from .00 to .05.

Forest-plot of generalized anxiety disorder and depression comorbidity in CHD (random effects).
Proportion of GAD patients with comorbid depression in CHD
In moderator analyses, only studies reporting the proportion of MDD cases among GAD patients were included (combined N = 2384). As there was evidence of heterogeneity (I2 = 97.77%), comorbidity data were pooled together in a random effects model, which suggested a modest association, Fisher’s Z = .28 (95% CI: .10–.46; z = 3.19, p = .0015, τ2 = .0301). There was no evidence of publication bias. The two studies with stable CHD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010) provided a higher comorbidity association in random effects model (Fisher’s Z = .34, 95% CI: .01–.69; z = 1.97, p = .05, τ2 = .0605) than the acute coronary syndrome studies (Fedoroff et al., 1991; Parker et al., 2011) (Fisher’s Z = .21, 95% CI: −.14 to .58; z = 1.19, p = .23, τ2 = .0629).
Proportion of depressedpatients with comorbid GADin CHD
The proportion of GAD cases among MDD patients could be determined in three studies (Bankier et al., 2004, 2008; Haworth et al., 2005). Comorbidity rates ranged between 18.33 per cent and 61.54 per cent. A random effects model was specified (I2 = 96.35%), and this test showed modest comorbidity between MDD and GAD (Z = .32, 95% CI: .13–.52; z = 3.2985, p < .0001). There was no evidence of publication bias from Begg and Mazumdar’s and Eggar’s test. The fail-safe N indicated that an additional 391 missing studies were required to bring the p value from .00 to .05.
Discussion
This systematic review was the first to quantify the degree of overlap between categorical depression and anxiety disorders in CHD patients with meta-analysis techniques. The results suggested approximately 11 per cent–14 per cent GAD prevalence in CHD samples, dependent on the diagnostic criteria employed to determine psychiatric disorder status. This finding approximates previous MDD prevalence estimates of 15 per cent in CHD samples (Thombs et al., 2008). The pooled lifetime GAD prevalence was 26 per cent. Generally speaking, the pooled comorbidity data showed correlations in the small to modest range (Cohen, 1992) between MDD and GAD and, thus, each psychiatric disorder is best conceptualized as sharing small to moderate variance in CHD populations.
The low comorbidity rates in CHD patients reported here noticeably contrast with those reported in clinical psychiatric samples. Evidence from three national epidemiological surveys in the Netherlands, United States and Australia (total N = 29,014) showed that GAD shared more variance with the mood disorders (r = .65) than with the other anxiety disorders (range r = .42–.58) in weighted analyses (Watson, 2009). A possible explanation for the discrepancy in comorbidity rates includes that the phenomenology of MDD in cardiovascular patients is discrepant from non-cardiovascular MDD, as previous authors have questioned (Carney and Freedland, 2012). For example, results from the Sequenced Alternatives to Relieve Depression showed that patients with CHD reported more symptoms of sympathetic nervous arousal (Fraguas et al., 2007). However, contrasting results have been reported as to whether a particular cardiovascular depression subtype might be associated with CHD morbidity (Carney and Freedland, 2012; Hoen et al., 2010; Tully et al., 2011).
Indeed, it is also plausible that the phenomenology of GAD is dissimilar among CHD patients. That said, Hoehn-Saric et al. (2004) reported that GAD patients without documented CHD scored significantly higher on cardiovascular and respiratory anxiety symptoms than other psychiatric patients and suggested that such symptoms were markers for somatic focussed worry in GAD. Challenging that illness worry and fear would be significantly elevated in CHD patients, Marker et al. (2008) reported that persons without documented atherosclerosis scored significantly higher on a measure of heart focussed worry/fear than persons with heart disease. Similarly, a Swedish sample of 767 chronic stable angina patients found evidence for lower worries about the future among persons with MI history than those without MI history (25% vs 37%, p < .01) (Billing et al., 2000). Comparably, lower worries were also found for persons with a heart failure diagnosis than persons without heart failure (26% vs 36%, p < .01) (Billing et al., 2000).
As the pooled correlation between MDD and GAD was modest, these findings have implications for interpretation of previous prognostic studies that have inferred heightened CHD morbidity risk to MDD and/or GAD. At the very least, findings here do not suggest that studies reporting prognostic CHD risk are merely confounded by a large degree of shared variance between MDD and GAD. With respect to prognostic studies examining MDD and GAD concurrently, the Heart and Soul study showed that GAD increased the risk for subsequent major cardiovascular events between 61 per cent and 74 per cent, while MDD impacted the strength of this association by less than 5 per cent, corroborating independence of these psychiatric disorders (Martens et al., 2010). Also, Frasure-Smith and Lesperance (2008) showed that both MDD and GAD were associated with a twofold increased risk for major adverse cardiovascular outcome. However, the authors also noted that a diagnosis of either MDD or GAD conferred the greatest cardiovascular morbidity event risk, despite the small correlation between psychiatric disorders in the sample (Fisher’s Z = 17, p = .04). As such, it is not known whether MDD and GAD work through similar or discrepant biobehavioural mechanisms to portend greater CHD morbidity risk. Curiously, despite low comorbidity rates in CHD, both MDD and GAD have been associated with reduced vagal control and autonomic nervous system activity (Brosschot et al., 2006). Additionally, previous research links both MDD and GAD to CHD risk factors such as smoking, alcohol use, lower exercise and lower medication adherence (Barger and Sydeman, 2005; Grant et al., 2004; Martens et al., 2010; Wiltink et al., 2011).
Collectively, a sparse number of studies met the inclusion criteria, suggesting that further GAD research is required in CHD to clarify these preliminary findings. Dugas et al. (2010) highlighted the low rate of publications and concluded that GAD research continues to lag behind the other anxiety disorders. In CHD, previous research and intervention efforts appear to have consolidated depression as the predominant psychosocial factor (Denollet, 2008), whereas GAD research is seemingly in the nascent stages. For example, few of the CHD studies reported here investigated prognostic cardiovascular outcomes (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Parker et al., 2011) or receiver operating characteristic evaluations of self-report measures to identify GAD (Frasure-Smith and Lesperance, 2008; Haworth et al., 2005; Tully and Penninx, 2012). As other systematic reviews have shown, GAD is a chronic and disabling condition that deleteriously impacts upon quality of life (Bereza et al., 2009), with significant unmet needs (Sherbourne et al., 1996) and associated financial costs in primary care (Hoffman et al., 2008). Thus, given the relatively modest comorbidity rates between GAD and MDD, the recommendation for further GAD research in CHD cannot be understated. The predominance of CHD research concerning non-specific self-reported anxiogenic constructs such as trait and state anxiety may hamper efforts to examine specific disorders such as GAD. It was the case here that studies were excluded because various anxiety disorders were collapsed together into an ‘any anxiety disorder category’ that is not clinically informative in cardiac settings (Tully and Baker, 2012). In fact, such research practices neglect the heterogeneous presentation of anxiety disorders and the phenotypic variance that makes each disorder relatively unique (Watson, 2009).
This study is presented with several strengths including the systematic data retrieval and meta-analyses techniques to provide a novel quantification of the degree of overlap between depression and anxiety disorders that confer CHD risk. Studies prone to bias with samples fewer than 50 and those adopting self-reports of CHD were excluded. A large proportion of total variance was explained by heterogeneity in the studies, and one potential explanation was the types of CHD patients recruited. For example, only one study was identified among CABG surgery (Tully et al., 2011), one among cardiac rehabilitation attendees (Todaro et al., 2007) and two studies after acute coronary syndrome (Fedoroff et al., 1991; Parker et al., 2011). Other potential sources of heterogeneity include the type of diagnostic criteria to determine GAD, gender ratio and age of patients. A limitation concerns the categorical classification of depression and anxiety when these negative emotional constructs are known to reflect a continuum, and critically appraised as potentially reflecting a single disorder (Mennin et al., 2008). Further research might investigate the overlap between MDD and GAD with continuous self-report measures that match diagnostic criteria (e.g. patient health questionnaire (PHQ)-9 and GAD-7) (Kroenke et al., 2010), and could pool together r values using a similar methodology to that outlined here.
In conclusion, these data approximate 11 per cent–14 per cent current and 26 per cent lifetime GAD prevalence in CHD. The pooled data showed small to modest correlations between MDD and GAD and, thus, each psychiatric disorder is best conceptualized as sharing moderate amount of variance in CHD populations. These findings support that GAD and MDD each contribute unique variance to CHD prognosis and may assist interpretations of the extant literature.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.