
Abstract
We used secondary data analysis to examine associations among aspects of patient–provider relationships and mental and physical health indicators. Positive patient perceptions of patient–provider relationships were associated with fewer mental health symptoms in this outpatient sample of HIV-positive men who have sex with men (N = 171). Regression analyses revealed the role of anxiety and depression in explaining associations between two aspects of patient–provider relationships (i.e. quality of information offered and provider interactional style) and health-related quality of life. The findings demonstrated the importance of patient–provider relationships to improving physical health and functioning and maintaining engagement in care, among HIV-positive men who have sex with men.
Evidence supports the importance of patient–provider relationships (PPRs) to patient satisfaction, disease management, and health-related outcomes for individuals with chronic illness, including HIV (Stewart, 1995; Swendeman et al., 2009). For people living with HIV, HIV-related stigma may contribute to the challenge of establishing strong and trusting relationships with providers (Mahajan et al., 2008). The majority of HIV-positive individuals in the United States are men who have sex with men (MSM), in terms of both prevalent and incident infections (Centers for Disease Control and Prevention (CDC), 2010). Thus, many people living with HIV may experience unique challenges in their relationships with providers because of stigma related to their sexual orientation (Mimiaga et al., 2007) and to the disease itself (Skelton, 2006).
Given HIV’s history as a highly stigmatized medical condition, it is likely that a strong, positive PPR is especially important for this population (Logie and Gadalla, 2009). The published literature examining PPRs for HIV-positive patients has demonstrated the importance of these relationships to medical care, including engagement and retention (Mallinson et al., 2007), medication adherence (Abel and Painter, 2003; Murphy et al., 2004; Roberson et al., 2009; Schneider et al., 2004), disease self-management (Swendeman et al., 2009), and health-related quality of life (HRQOL; Préau et al., 2004). In one qualitative study of HIV-positive men and women, provider behaviors described as “connecting,” “validating,” and “partnering” facilitated patients’ engagement and retention in care (Mallinson et al., 2007). In another study, HIV-positive women also identified patient–provider communication as a critical factor facilitating adherence to antiretroviral therapy (ART; Abel and Painter, 2003). Numerous other quantitative studies have demonstrated the relation between PPRs to medication adherence among HIV-positive women (Roberson et al., 2009), as well as men and women (Murphy et al., 2004; Schneider et al., 2004). Finally, PPRs may be related to HRQOL, such that trust in one’s provider is associated with mental HRQOL, while satisfaction with information offered is associated with physical HRQOL (Préau et al., 2004).
Studies have also demonstrated that factors such as stigma and perceptions of insensitive providers impact PPRs. In at least one study, MSM reported encountering providers they perceived as insensitive or judgmental, and endorsed that they are less likely to disclose their health information and needs to providers who they perceived as less comfortable treating MSM (Mimiaga et al., 2007). Other evidence suggests that HIV-related stigma often accounts for individuals failing to disclose their HIV status to sex partners (Bird and Voisin, 2011). This stigma may similarly serve to discourage patients from communicating openly with their providers or remaining engaged in care (Kinsler et al., 2007).
The importance of understanding PPR among MSM, especially as it relates to psychosocial functioning and stigmatized health behaviors (e.g. drug use, sexual behavior), has been clearly established. Depression and anxiety are the most commonly endorsed mental health problems of HIV-positive MSM (Berg et al., 2004), and high levels of psychological distress are observed in MSM independent of HIV status (Gibbie et al., 2012). HIV-related stigma, when experienced in high levels, is also associated with depression (Dowshen et al., 2009). Thus, the importance of providers identifying and treating these mental health symptoms, as well as addressing stigma-related concerns, could serve to improve physical health functioning for these men (e.g. Pence, 2009).
Overall, the extant research has clearly shown the importance of PPRs for HIV-positive patients. Few studies, however, have quantitatively examined associations between different aspects of PPRs (i.e. factors contributing to the quality of the PPR) and physical or mental health status in people living with HIV, and no studies we identified examined indicators associated with PPRs among HIV-positive MSM. Moving forward, it may be useful to pinpoint more specifically which aspects of PPRs (e.g. quality of medical information offered by providers) are most influential among MSM, as these findings could be useful in informing specific recommendations for provider behavior. For example, HIV-positive patients engaged in discussions about substance abuse with providers are more likely to receive substance use treatment compared to similar patients not engaged in such discussions (Korthuis et al., 2008), thus demonstrating clear benefit to providers initiating or following-up on patient comments about psychosocial issues. Despite these findings, a recent qualitative study demonstrated that providers of HIV medical care feel comfortable discussing sexual risk behaviors with patients but less comfortable discussing substance abuse behaviors (Drainoni et al., 2009).
Therefore, in this study, we examined three different aspects of PPRs by investigating their associations with measures of mental and physical health. Given that a patient’s perception of his PPR may be more influential to his health than his provider’s perception of the relationship, or the actual quality of the relationship, we chose to assess patients’ perceptions of the quality of (a) information provided by their HIV providers, (b) providers’ overall interactional styles, and (c) the psychosocial assessments conducted by providers. In this secondary data analysis, using information from a cross-sectional study of HIV-positive MSM engaged with medical care, we aimed to examine (1) relations among three aspects of patient perceptions of PPRs, (2) relations between aspects of PPRs and mental health functioning, (3) relations between aspects of PPRs and physical health functioning, and (4) whether mental health indicators play a mediating role in the associations between PPRs and physical health indicators. We anticipated that the three aspects would all correlate, such that patients who rated their providers highly in one area would rate them highly in other areas. We hypothesized that each PPR aspect would be related to mental and physical health indicators, such that patients perceiving higher quality PPRs would exhibit better mental and physical health. Finally, we expected that mental health indicators would account in part for associations between PPR aspects and physical health indicators.
Method
Procedures
As part of a larger study (Pantalone et al., 2010), we recruited a cross-sectional convenience sample of HIV-positive MSM in 2006–2007 from two university-affiliated, public, urban, outpatient HIV/AIDS clinics in Seattle, Washington, using a purposive (i.e. targeted) sampling strategy (Watters and Biernacki, 1989). The smaller of the two clinics serves 180 patients (n = 14), while the larger serves over 1900 medically underserved patients (n = 157). Patients at both clinics include ethnic minority individuals (33%–44%) and individuals receiving public assistance (50%–77%). Participants recruited from the two clinics did not differ significantly on any demographic characteristics assessed. Potential participants were referred by a social worker or nurse if they expressed willingness to participate in a computer-based study about how psychosocial factors affect their health (Project LEAP; Life Experiences Affecting Prognosis). Given that clinic patients were not targeted for any specific characteristics, the referring providers did not track rates of or reasons for refusal from patients who declined to be referred to the study.
Eligible individuals were active patients at either clinic, over 18 years old, biologically male at birth, English speaking, and self-identified as gay/bisexual/MSM. All eligible referred patients were consented and enrolled. Participants were paid $20 and provided with a list of low-cost community resources focused on needs of people living with HIV/AIDS.
Participants
The mean age of participants (N = 171) was 44 years; they had been living with HIV for an average of 12.7 years (64% reported AIDS diagnosis). Most men identified as European American/White (63.6%), while 18.5 percent identified as African American, 7.7 percent as multiracial, 6 percent as Native American, and 4.2 percent declined to identify their race; 12.3 percent identified their ethnicity as Hispanic/Latino. Nineteen percent were employed, and 61 percent were both unemployed and considered disabled by the government. A majority of participants (82%) reported average monthly incomes <$18,000/year.
Measures
Participants responded using a computer-assisted self-interview (CASI) format to decrease socially desirable responding and maximize efficiency, confidentiality, and data management (Rhodes et al., 2002). Skip patterns were used to eliminate irrelevant questions. Well-validated self-report measures with established psychometric properties were used whenever possible. At the end of the study, data reflecting physical health indicators (i.e. CD4 count, viral load, and adherence) were extracted from participants’ electronic medical records (EMRs) by two research assistants using a standardized form; interrater reliability for exact matches across items was >93 percent.
Sociodemographics measured included age, race/ethnicity, education, income, employment and disability status, time since HIV diagnosis, diagnosis with AIDS, and probable transmission route. Social desirability was measured with the short-form Marlowe–Crowne Social Desirability Scale (Crowne and Marlowe, 1960; α = .73).
PPR
Quality of the PPR, as perceived by patients, was assessed with an established nine-item self-report scale (Wilson and Kaplan, 2000). In this study, we divided the scale into three subscales, with (a) three items each addressing the patient’s perception of the quality of information offered by the provider (α = .90), (b) two items addressing the patient’s perception of the provider’s interactional style (α = .91), and (c) four items addressing the patient’s perception of the provider’s ability to conduct a screening of the patient’s psychosocial status (α = .92). The quality of information subscale asked patients to rate how good their HIV health-care provider is at (1) “Explaining the results of tests in a way that you understand”; (2) “Giving you facts about the benefits and risks of treatment”; and (3) “Telling you what to do if certain problems or symptoms occur.” Items relating to participants’ perceptions of providers’ interactional styles included: (4) “Demonstrating caring, compassion, and understanding” and (5) “Understanding your health worries and concerns.” Finally, patients were asked to consider providers’ abilities to screen for psychosocial risk factors by (6) “Talking with you about your sex life”; (7) “Asking you about stresses in your life that may affect your health”; (8) “Asking about problems with alcohol”; and (9) “Asking about problems with street drugs like heroin and cocaine.” Participants were asked to consider the communication of their HIV provider by assigning ratings for all items (1 = excellent; 5 = poor). To ease interpretation of results, we recoded ratings such that higher ratings indicated better quality communication as perceived by patients (i.e. recoded 1 = poor; 5 = excellent). This scale was originally validated with HIV-positive patients (N = 264) and found to load onto two factors, with five items assessing general communication (α = .93) and four items assessing HIV-specific communication (α = .92; Wilson and Kaplan, 2000).
Mental health indicators
Depressive symptoms were assessed with the Center for Epidemiological Study Depression Scale (CES-D; Radloff, 1977; α = .92) and anxiety symptoms with the state subscale of the State-Trait Personality Inventory (STPI; Spielberger, 1979; α = .79).
Physical health indicators
HRQOL and perceptions of health status were measured by the Medical Outcomes Study HIV Health Survey (MOS-HIV; Wu et al., 1997). We used all 19 items from the physical health subscale (α = .77) and excluded mental health and cognitive functioning items due to potential redundancy with other psychosocial measures. CD4 count and viral load (HIV-1 polymerase chain reaction (PCR) RNA) were extracted from participants’ EMRs as close in time to the study visit as possible (M = 30.4, standard deviation (SD) = 27.7, range: 0–118 days).
As no uniformly accepted HIV medication adherence measures exist, we considered recommendations in a review of self-report adherence measures (Simoni et al., 2006) to develop investigator-created items assessing adherence. Given evidence that use of a dichotomous item is the best way to avoid overestimating adherence (Pearson et al., 2007) and that the most valid recall period is 30 days prior to interview (Lu et al., 2008), we report the proportion of our sample indicating 100 percent medication adherence in this time frame. As a proxy for disengagement with health care, coders noted from EMRs whether participants had any period of 4 months (in the year prior to assessment) without HIV-related clinical visits. Patients were considered disengaged with care if they did not meet the CDC recommendation for people living with HIV/AIDS of medical visits at least quarterly (Aberg et al., 2009) during the past year.
Data analysis
No variables presented problems with missing data (i.e. >5% missing). To examine the aspects of PPRs (perceived quality of information, interactional style, and psychosocial assessment) and their correlates, we conducted four sets of analyses: (1) correlations among the three aspects, (2) correlations among each aspect and mental health indicators, (3) correlations among each aspect and physical health indicators, and (4) multiple linear regression (MLR) analyses to determine whether mental health indicators mediated relations among aspects of PPR and physical health indicators.
Results
Relations among PPR and mental and physical health
We first calculated Pearson product–moment correlations to examine relations among the three aspects of PPRs and mental and physical health indicators. Results revealed that all three PPR variables were strongly correlated with each other, as well as moderately associated with anxiety and depressive symptoms (see Table 1). For physical health indicators, we found small to moderate correlations between HRQOL and quality of information (r = .23, p = .002, r2 = .05) and interactional style (r = .20, p = .008, r2 = .04; see Table 1). Notably, results also indicated that lower ratings of the quality of information offered (r = −.25, p = .012, r2 = .03) were associated with greater patient viral load, even when controlling for ART adherence and CD4 count. A post hoc hierarchical MLR revealed that this association could not be accounted for by disengagement with care. Specifically, quality of information offered significantly predicted viral load (F(1,160) = 5.27, p = .023), but the model was no longer significant after entering disengagement (F(1,159) = 2.62, p = .076). Lastly, an independent samples t-test indicated that patients who had recently been disengaged with care (M = 12.88, SD = 2.76) reported poorer quality of information (t(54.8) = 2.09, p = .041) than patients who had been consistently engaged with care in the past year (M = 13.86, SD = 2.01).
Correlations among PPR and mental and physical health indicators.

HRQOL: health-related quality of life; PPR: patient–provider relationship.
p < .05; **p < .001.
Mediation models
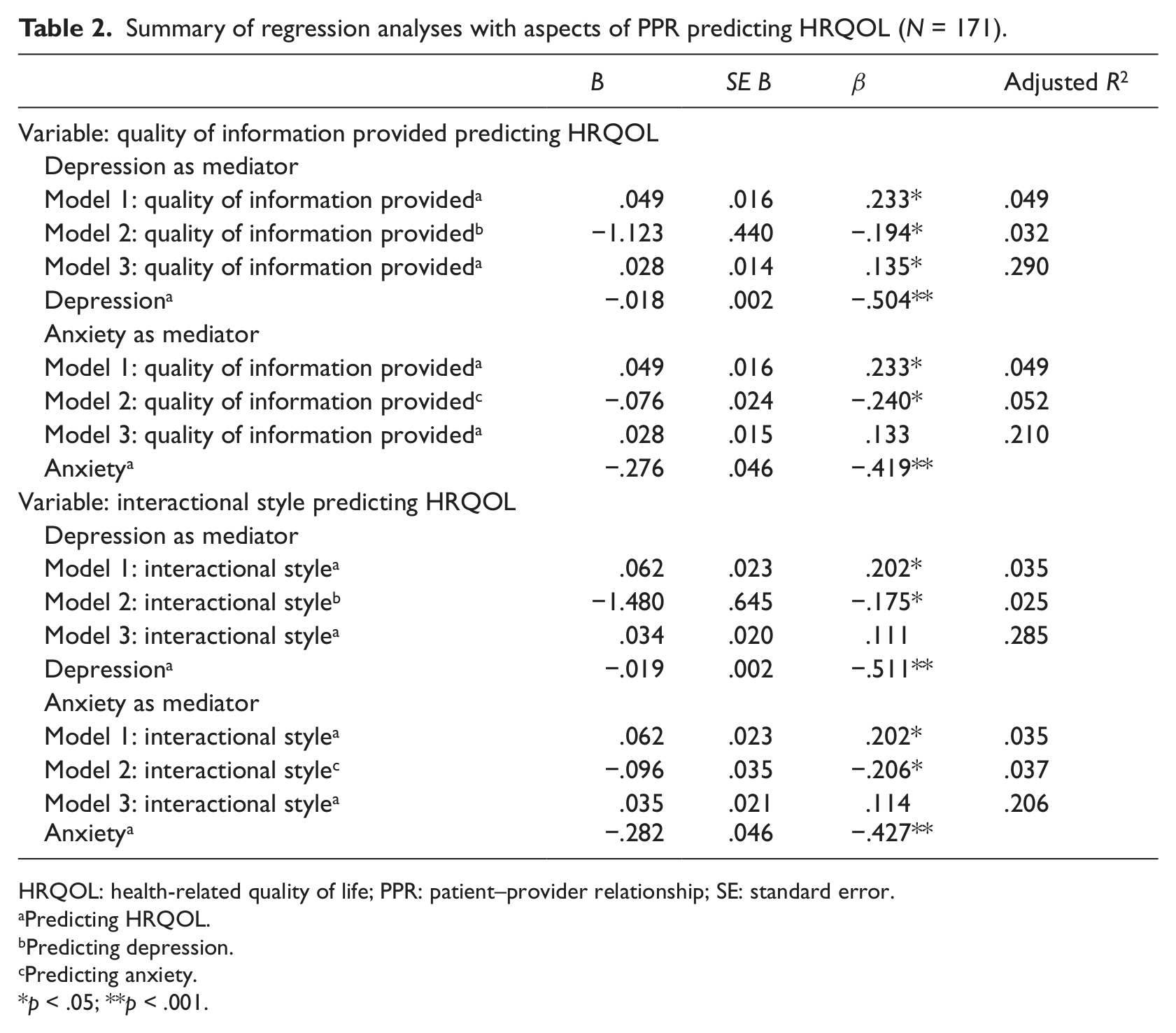
We conducted mediation analyses to identify potential mechanisms explaining the relations among PPRs and physical health indicators. We used Baron and Kenny’s (1986) model for mediation to examine whether mental health indicators mediated relations among aspects of PPRs and physical health indicators. Our first set of results revealed that no mental health indicators emerged as mediators between aspects of PPRs and physical health indicators. Next, we ran MLR models to test each mental health indicator’s impact on relations among quality of information provided, each aspect of PPRs, and each physical health indicator. Results revealed that depression and anxiety each partially mediated the relation between quality of information and HRQOL and the relation between provider style and HRQOL (see Table 2).
Summary of regression analyses with aspects of PPR predicting HRQOL (N = 171).
HRQOL: health-related quality of life; PPR: patient–provider relationship; SE: standard error.
Predicting HRQOL.
Predicting depression.
Predicting anxiety.
p < .05; **p < .001.
Discussion
In this study, we examined relations among PPRs and mental and physical health indicators in a sample of HIV-positive MSM engaged with medical care. This is the first study of which we are aware to investigate associations among PPRs and mental and physical health specifically for HIV-positive MSM, the population with the highest incidence and prevalence of HIV infections in the United States (CDC, 2010). Our findings underscore the importance of strong PPRs, particularly two aspects—quality of information communicated and provider interactional style. Participants who perceived these aspects more positively evidenced better mental and physical health status by a variety of indicators.
We predicted that the three aspects of PPRs would be correlated and, indeed, found moderate to strong associations among all the subscales, with provider style and quality of psychosocial screening emerging as the strongest correlation. As individuals perceived the psychosocial screening conducted by their provider to be higher quality, they also experienced their provider as more caring, compassionate, and understanding. This finding makes sense, given evidence from the social psychology literature on source credibility, suggesting that communicators perceived as trustworthy are also assumed more credible (Pornpitakpan, 2004), and has obvious implications for the necessity of training medical providers to foster a collaborative, supportive “bedside manner” with patients.
Second, we anticipated that PPRs would relate to indicators of patients’ mental and physical health (Stewart, 1995). Each aspect was associated with several areas of functioning. Alarmingly, patients who had been disengaged from care (vs. those continuously in care) in the past year reported a poorer quality of information received from providers. It is possible that patients who lacked confidence in their providers were more likely to skip appointments (Mallinson et al., 2007). Alternatively, patients who had been engaged intermittently with care may have felt personally judged or guilty—either because of, or irrespective of, their providers’ actions. Given the cross-sectional nature of our data, it is impossible to know the direction of these associations. Additionally, individuals reported fewer anxious and depressive symptoms when they perceived more positive provider interactions and believed they were receiving higher quality medical information and psychosocial screenings. Lower viral load and higher HRQOL (both biomarkers of good HIV health) were also associated with perceptions of higher quality information. Providers may have more difficulty connecting with patients with mental health symptoms and, thus, patients accurately perceive a weaker relationship (e.g. Ye and Shim, 2010). Alternatively, patients experiencing anxiety or depression may perceive provider’s interactions inaccurately, as social judgments tend to be mood congruent (Forgas, 1995).
Finally, we identified mental health variables that appear to mediate the association between PPRs and HRQOL, a well-established measure of physical functionality. We discovered that patients’ perceptions of quality of information and interactional style are, in part, related to HRQOL through anxiety and depression. That is, in this sample of HIV-positive MSM, mental health appears to serve as a link between patient perceptions of PPRs and their self-report of physical functionality. This highlights the importance of diagnosing and treating both threshold-level mental disorders and subthreshold presentations of common mental health symptoms (Nierenberg et al., 2010). Providers should screen, assess, and then refer or treat all HIV-positive MSM for mental health problems, as these appear to play an important role in the PPR outcome link (Nel and Kagee, 2011). Through screening and treating symptoms of depression and anxiety, factors that partially explain how PPRs impact patients’ physical health, health-care providers may be able to more effectively communicate and interact with patients, which, in turn, could improve patients’ functionality. Although assessing for mental health symptoms may impact PPRs, our findings clearly show the importance of addressing these concerns, if only through brief screenings.
Clinical and research implications
Overall, these findings suggest that two aspects of PPRs are critical to the mental and physical health of MSM living with HIV: patient perceptions of the quality of information received from providers (Stewart, 1995) and patient perceptions of providers’ interactional styles (Mallinson et al., 2007). Providers who demonstrate caring, compassion, and understanding, including explaining information clearly and thoroughly, are likely to see better mental and physical health-related functioning in their MSM patients. Many barriers prevent providers from developing optimal relationships with patients and explaining information well (e.g. Alexander et al., 2004). One such structural barrier to consider is how time constraints may impact PPRs, in terms of information offered and provider style. Although average time spent during medical visits varies significantly by specialty, providers may spend anywhere from 5–20 minutes with patients (Dugdale et al., 1999). Studies have consistently shown that as providers spend more time with patients, not only does the quantity of information provided increase, but patient satisfaction with the interaction increases as well (Yarnall et al., 2003). This suggests that, in addition to educating medical professionals on the importance of supportive “bedside manner” and maximizing time spent during each visit, structural modifications may be needed. A team approach to clinical care could alleviate some of the burden on primary care providers, whereby clinical care and patient education are provided by multiple providers, such as nurse practitioners and professional health educators.
Specific provider-level factors could impact PPRs as well, such as length of time practicing or status of the physician (e.g. intern vs. attending). Length of time practicing has been shown to be inversely related to interpersonal skills, such that as medical students progress through training toward independent practice, interpersonal skills seem to decrease (Gordon and Edwards, 1995). Given this concerning finding, perhaps interpersonal skills should be incorporated into training and evaluation throughout one’s tenure as a health-care professional.
Of particular importance is the relation between the patient’s perception of the quality of information and patient disengagement from care which is substantiated in the literature (e.g. Cruz and Pincus, 2002). To target and potentially increase patient engagement, training programs for health-care professionals should consider educating providers on how to communicate clear and accessible information to patients, taking into account the health literacy of the patient. Explaining information well, presenting facts about the benefits and risks of treatments, and describing what to do if symptoms exacerbate or side effects occur may be especially important for patients who are ambivalent about treatment or those who have other life stressors that they judge to be more urgent. Future research should measure patient ambivalence about treatment, in addition to quality of information received, to examine the role of PPRs in engaging ambivalent individuals in treatment. Furthermore, our findings show that PPRs are related to HRQOL through mental health; this result highlights the importance of screening for mental health symptoms when interacting with patients. Since mental health seems to be one mechanism by which PPRs are related to health (Nel and Kagee, 2011), future research should measure how well providers screen, and refer for or treat, mental health problems during routine interactions. Providers should be encouraged to include as standard practice at least basic screenings of mental health symptoms, which seem to be closely tied to health-related functioning (Lyketsos et al., 1994).
Limitations
As with any individual study, there are several notable limitations. Given that the data are cross-sectional, we cannot know whether patients experiencing better mental and physical health are, therefore, more likely to have more positive perceptions of their health-care providers. Regardless of the causal direction, it is important to recognize the associations between PPRs and health-related functioning, as patients experiencing poorer mental and physical health may require additional attention to the development and maintenance of strong and supportive strong and supportive PPRs. Additionally, given that this study involved secondary data analysis, we did not assess for all relevant information, including information about participants’ providers (e.g. level of training). Finally, patients in our sample patients in our sample reported high overall quality of PPRs and were already engaged in HIV care. It seems important to better understand PPRs for patients who perceive their providers more negatively (qualitative work may be needed to record and examine patient–provider interactions) and who are initiating a new PPR. Future research in this area could extend to patients with more diverse perceptions of their providers and experiences with care.
Conclusion
This study advances the literature by closely examining aspects of PPRs and their associations with mental and physical health indicators in HIV-positive MSM outpatients. Findings reveal the importance of providers offering high quality, accessible information—and utilizing positive interactional styles—in minimizing poor psychosocial functioning for patients, and improving HRQOL and physical health status. Finally, the medical information offered by providers appears to be a potential key feature in preventing patient disengagement with care.
Footnotes
Acknowledgements
The authors wish to express sincere gratitude to the project’s research assistants at the University of Washington, as well as the staff and patients of the cooperating clinics.
Funding
This research was supported by a National Institute of Mental Health award (F31 MH71179, mentored by Jane Simoni) and a small grant from the Robert C. Bolles Research Fund of the University of Washington, both awarded to David Pantalone.