
Abstract
The impact of pharmaceutical drug names on people’s evaluations and behavioural intentions is still uncertain. According to the representativeness heuristic, evaluations should be more positive for complex drug names; in contrast, fluency theory suggests that evaluations should be more positive for simple drug names. Results of three experimental studies showed that complex drug names were perceived as more hazardous than simple drug names and negatively influenced willingness to buy. The results are of particular importance given the fact that there is a worldwide trend to make more drugs available for self-medication.
Not all that long ago, the decision about what medication a patient should take was solely in the hands of a physician. After a close inspection of the patient’s health status, the physician would reach a decision about the medical treatment, write down a prescription, provide advice on dosage level and dosage frequency and refer the patient to the pharmacy. Patients were more or less passive and voiceless about medication decisions. Today, however, patients play a more active role in decisions about which medication to take (Botti et al., 2009; Loewenstein, 2005; Siminoff and Step, 2005). Patients are free to discuss medical treatments with their physicians and are encouraged to express their preferences regarding treatment alternatives.
The more active role of patients is also reflected in the growing market of over-the-counter (OTC) drugs that are available to people without a prescription from a health-care professional. Since OTC drugs are sold in pharmacies, groceries and convenience stores, the assumption can be made that recommendations from physicians and other health professionals represent one, but not the sole, determinant of patients’ OTC drug purchase choices. Compared to prescription drugs, the decision to buy OTC drugs will also be influenced by factors such as advertisement, recommendations from family and friends, habits and the design of a product. In addition, people might also possibly apply heuristics, or rules of thumb, when evaluating and choosing health products and pharmaceutical drugs.
One important heuristic that could play a major role in the evaluation of a drug is the representativeness heuristic (Gilovich et al., 2002). Representativeness heuristics suggest that if an object resembles another on some salient dimension, then the two may act similarly (Pratkanis, 1995). Notably, the influence of representativeness on causal judgement is particularly strong in the domain of medical beliefs, because people often assume that the symptoms of a disease should resemble its cause, its cure or both (Gilovich and Savitsky, 2002). Many people assume that a greater size or quantity of a drug will do a better job, for instance, that two pills of a painkiller will work better than one. In addition, many drugs are supplemented with non-effective, bitter-tasting substances in order to meet people’s expectations that only bitter pills are effective. It also stands to reason that the polysyllabic, complex names of many drugs are consistent with people’s medical beliefs about the effectiveness of drugs. Thus, from the representativeness heuristic, one would assume that drugs with a complex name would be perceived as more effective than drugs with a simple name because only drugs with complex names would be expected to be able to fight diseases effectively, especially if the disease itself is rather complex.
Recent research from fluency theory, however, suggests that this story may be more complicated than it first appears. Processing fluency denotes the ease or difficulty with which new, external information can be processed (Reber et al., 2004; Schwarz, 2004; Schwarz et al., 2009). Fluently processed stimuli are judged as more familiar and therefore elicit a more positive affective response than disfluently processed stimuli (Schwarz et al., 2009). Since fluently processed stimuli seem more familiar, they should also be perceived as less threatening and less risky. In a recent experiment, Song and Schwarz (2009) tested this assumption and presented participants with names of fictitious food additives that were either easy or difficult to pronounce. Participants were asked to rate the hazardousness of these food additives, and food additives with difficult-to-pronounce names were rated as more hazardous. Thus, from fluency theory, one would assume that simple drug names should be evaluated more positively (i.e. as less hazardous) than complex names because they are directly connected to familiarity. People may follow the logic that if a drug name is familiar, it presumably has not hurt anyone in the past.
This research examines the impact of a drug name’s complexity on evaluations and behavioural intentions. More precisely, it aims to test the conflicting hypotheses that can be derived from the representativeness heuristic and fluency theory.
Study 1
According to the representativeness heuristic, evaluation of a drug should be more positive if the drug bears a complex name because it can be assumed that people believe that complex names more strongly resemble the cause of a disease than do simple names. Thus, behavioural intentions (willingness to buy the drug) should be mediated by the perceived effectiveness of the drug. Fluency theory, in contrast, suggests that complex names imply hazardousness and thus negatively influence people’s evaluation. Accordingly, willingness to buy should be attenuated for drug with a complex name because hazardousness may act as a mediator between ease of pronunciation and behavioural intentions. In Study 1, we sought to test these hypotheses against each other.
Method
Pretest
A total of 16 pretest words, composed of 12 letters, were taken from Song and Schwarz (2009). In our pretest, a German-speaking sample (N = 20) judged all words according to how easily the words could be pronounced (1 = very easy, 7 = very difficult). The five easiest and the five most difficult words differed significantly in ease of pronunciation, t(19) = −17.01, p < .001, r = 0.97, and were used for the following experiment.
Participants and design
Participants were 22 students (14 females, 8 males, age: M = 24 years, standard deviation (SD) = 3 years) from the University of Zurich and ETH Zurich, who received financial compensation for their participation. Study 1 was a two-level, single-factor, within-subject experiment in which participants judged 10 fictitious drugs that had either a simple (Fastinorbine, Calotropisin, Tonalibamium, Zionialosium and Allotoneline) or a complex name (Cytrigmcmium, Nxungzictrop, Ribozoxtlitp, Hnegripitrom and Fluthractnip). The within-subject design was used because it resembles real-life decisions more strongly than a between-subject design (i.e. a person who wants to buy a drug in a pharmacy can usually choose among a wide range of products and brands).
Material and procedure
Upon arriving at the laboratory, participants were seated in laptop-equipped cubicles, where the entire experiment took place and all instructions were presented. Participants were informed that the study would be about different drugs and that they would be asked to judge them. Drug names were presented in two different random orders. Judgements about the drugs were made about their hazardousness (1 = very safe, 7 = very hazardous) and effectiveness (1 = very ineffective, 7 = very effective). Furthermore, participants indicated whether they believed that the drug had side effects (1 = strongly disagree, 7 = strongly agree) and whether they would buy the drug (1 = strongly disagree, 7 = strongly agree). After answering standard demographic questions, participants received debriefing and were thanked for their participation.
Results and discussion
Drugs with simple names were perceived as less hazardous (M = 3.87, SD = 1.13) than drugs with complex names (M = 4.67, SD = 0.88; t(21) = −3.10, p = .005, r = 0.56). Participants also expected that drugs with a simple name would have fewer side effects (M = 4.10, SD = 1.07) compared to drugs with a complex name (M = 4.74, SD = 0.94; t(21) = −2.96, p = .007, r = 0.54). Furthermore, willingness to buy was higher for drugs with simple names (M = 3.86, SD = 1.24) than for drugs with complex names (M = 3.29, SD = 1.23; t(21) = 2.92, p = .008, r = 0.54). However, we found no effect of name on the drug’s perceived effectiveness. Drugs with simple names were perceived as effective similar to drugs with complex names (easy: M = 4.36, SD = 1.00; difficult: M = 4.06, SD = 0.91, p > .10).
To test whether hazardousness mediated the relationship between name and willingness to buy, we employed the method outlined in Judd et al. (2001) for testing mediation in repeated-measures designs. Having shown that the name (independent variable) affected hazardousness (mediator) and willingness to buy (dependent variable), we tested whether hazardousness was significantly related to willingness to buy at each level of the independent variable. Note that hazardousness scores were reversed, so that lower numbers always indicated that drugs were judged as more hazardous. For both the simple and complex names, hazardousness predicted willingness to buy (simple: β = .86, p < .001; complex: β = .72, p < .001). In a final step, a change in the dependent variable was regressed on change in the mediator and the centred sum of the mediator values. According to Judd et al. (2001), full mediation is indicated by a significant coefficient for the mediator accompanied by a non-significant coefficient for the intercept term, indicating that the difference in hazardousness predicts all of the difference in willingness to buy. This is precisely what we found. The results indicated that the difference in hazardousness significantly predicted willingness to buy (β = .80, p < .001), while the intercept coefficient was not different from zero, p > .50.
The study revealed a clear support for the fluency hypothesis. Complex drug names imply hazardousness and thus negatively influence people’s behavioural intentions (i.e. willingness to buy). However, based solely on the results from Study 1, we cannot rule out the possibility that participants assumed that all of the presented drugs were used for the treatment of a rather simple illness. According to this, only simple names would be representative of the illness, and representativeness could still account for the effect in the dependent variable. Thus, a limitation of the first study is that we did not control for the complexity of the illness.
Study 2
According to the fluency hypothesis, a simple name would decrease perceived hazardousness and increase willingness to buy, regardless of the complexity of the illness. In contrast, an interaction effect of illness and name on willingness to buy would be expected if representativeness of the name was a key factor; according to this, people may assume that a complex illness could be best treated with a drug bearing a complex name, while for a simple illness, a drug with a simple name would be the better cure.
Method
Participants and design
Participants were 28 students (16 females, 12 males; age: M = 27 years, SD = 7 years) from the University of Zurich and ETH Zurich, who received financial compensation for their participation. The study employed a 2 (name: simple vs complex) × 2 (illness: simple vs complex) within-subject design. We chose the four easiest (Fastinorbine, Calotropisin, Tonalibamium and Zionialosium) and the four most difficult to pronounce names (Cytrigmcmium, Nxungzictrop, Ribozoxtlitp and Hnegripitrom) from the pretest as stimuli for Study 2. Headache, which is not life threatening and is easy to treat, served as a simple illness, while pancreatic cancer, which is life threatening and difficult to treat, served as a complex illness.
Material and procedure
The experimental procedure was similar to that of Study 1. Participants were seated in separate cubicles and completed the experiment on a laptop. In the first part of the experiment, participants were asked to imagine that they were suffering from headaches and that different drugs could be considered to treat the headache. Subsequently, respondents judged four drugs according to their hazardousness (1 = very safe, 7 = very hazardous), effectiveness (1 = very ineffective, 7 = very effective), side effects (1 = strongly disagree, 7 = strongly agree) and willingness to buy (1 = strongly disagree, 7 = strongly agree). Two drugs had a simple name and two had a complex name. In the second part, participants were asked to imagine that they were diagnosed with pancreatic cancer and that different drugs could be considered to treat the cancer. Again, two simple and two complex names were presented, and participants judged the drugs according to their hazardousness, effectiveness, side effects and willingness to buy. In addition, we controlled for presentation order effects: half of the participants conducted the study in the sequence described above, while the other half were first asked about pancreatic cancer (complex illness condition) and then about headaches (simple illness condition). We also employed a yoked design: The order of the drug names was rotated such that for every drug name encountered by a participant in the simple illness condition, there was a participant who had encountered the same drug name in the complex illness condition. Finally, participants answered demographic questions and were thanked and debriefed.
Results and discussion
A 2 (name: simple vs complex) × 2 (illness: simple vs complex) repeated-measures analysis of variance (ANOVA) was carried out on each dependent measure (see Table 1). First, we analysed the results for hazardousness. This analysis yielded a significant main effect for name, F(1, 27) = 13.77, p < .001,
Means of hazardousness, effectiveness, side effects and willingness to buy as function of name and illness.
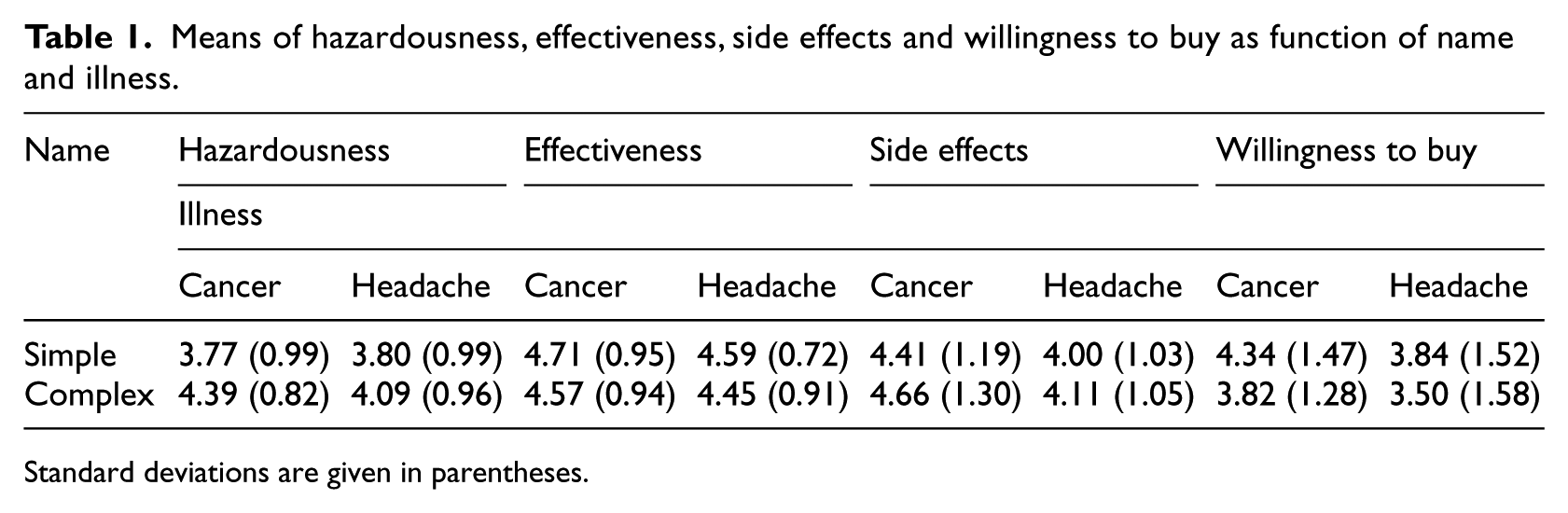
Standard deviations are given in parentheses.
Next, as in Study 1, we analysed whether hazardousness mediated the effect of name on willingness to buy. As outlined above, name emerged as a significant predictor for both the mediator and the dependent variable. In addition, the more hazardous a drug name was judged, the less participants were willing to buy the drug, which was true for both conditions (simple: β = .62, p < .001; complex: β = .55, p = .003). For the third and final step for testing the mediation, we regressed the change in willingness to buy on changes in hazardousness and the centred sum of the hazardousness values. This analysis showed that hazardousness, as was found in Study 1, fully mediated the effect on willingness to buy. The difference in hazardousness significantly predicted willingness to buy (β = .43, p = .028), while the intercept coefficient was not different from zero, p > .10. Again, the study provides clear support for the fluency hypothesis and contradicts the notion that representativeness is key when evaluating drug names.
Study 3
In Study 3, we wanted to examine the robustness of the finding that simple drug names increase positive product evaluations and behavioural intentions to buy the drug. Therefore, we use a random sample instead of a student sample in order to extend the generalizability of the results found in Studies 1 and 2. Robustness was further addressed by giving participants more detailed information about the drug. It is unclear whether the drug name would be still relevant for people’s judgement if they were also informed about the price, particularly since price is also easier to evaluate than the name. According to the evaluability hypothesis (Hsee, 1996, 1998), attributes that are difficult to evaluate have little impact on decision-making. Evaluability is easier if a person is aware about an attribute’s range or its neutral reference point (Hsee, 1998). Therefore, compared to the name, the price should be more dominant in people’s decisions to buy a certain product.
To determine the relative importance of the name of a drug compared to the price, we used conjoint analysis. In a conjoint analysis, participants evaluate or rank a set of real or hypothetical products that are characterized by specific attributes, such as the price or the name of the product. Attributes are made up by attribute levels, which are the specific values of the product attributes (e.g. price ranges). Because the product attributes are considered jointly rather than in isolation, conjoint analysis forces the respondent to evaluate conflicting attributes; thus, it maintains a high degree of realism and resembles real choice situations (Hair et al., 1998). Furthermore, conjoint analysis allows for identifying preference heterogeneity (Green and Krieger, 1991; Hair et al., 1998). That is, participants can be grouped into different segments with similar preferences. The segments are usually derived using cluster analysis. It is possible that not all people’s evaluations are driven by a name’s fluency; instead, it could be that a certain percentage of respondents apply the representative heuristic when evaluating drug names. This segment would remain undetected if only total sample means are considered.
Method
Participants
The data for Study 3 were obtained from a large-scale mail survey conducted in the German-speaking part of Switzerland. A questionnaire and an accompanying letter were sent to a random sample of addresses from the telephone book. The household member over 18 years of age whose birthday was closest to the date that the questionnaire was received was asked to fill out the survey.
A response rate of 28 per cent (N = 804) was achieved. The mean age was 54 years (SD = 15); 48.0 per cent (n = 386) of the respondents were women, and 50.5 per cent (n = 406) were men. In all, 11 participants (1.4%) did not report their age, and 12 participants (1.5%) did not report their gender. The self-reported education level ranged from primary and lower secondary school (8.5%, n = 69) and upper secondary vocational school or upper secondary university preparation school (57.3%, n = 461) to college or university (32.5%, n = 261). Overall, 13 respondents (1.6%) did not indicate their education level.
Material and procedure
In the questionnaire, participants were asked to imagine that they had a sore throat and difficulty swallowing and that they wanted to buy cough tablets. The pharmacy offered different cough tablet brands with different prices. Six different fictitious products were described to the participants that were characterized by the following two attributes: price (CHF 9.30, CHF 10.50, CHF 11.80) and name (Fastinorbine, Cytrigmcmium). In order to keep the prices in a realistic range, levels of the attribute price were chosen according to real market conditions. The low (high) price was two SDs lower (higher) than the mean market price of CHF 10.50 for cough tablets. Participants were asked to assess their willingness to buy each product by placing a mark on a horizontal line that was labelled ‘I would certainly not buy it’ on the left side and ‘I would certainly buy it’ on the right side. At the end of the questionnaire, standard demographic questions were asked.
Results and discussion
Using SPSS CONJOINT (SPSS, 2007), we calculated aggregated part-worth utilities (total sample). Part-worth utilities provide a quantitative measure of the preference for each attribute level. The range between the lowest and the highest part-worth utility value within each attribute indicates the relative importance of each attribute; relative importance scores always add up to 100 per cent. Data from participants with missing values or invariable responses were excluded.
The conjoint analysis revealed that participants, on average, deemed price to be the most important factor when buying a drug (see Table 2). However, the name of the drug was relevant, too, and was also taken into consideration by respondents; the relative importance scores for price and name, which were derived via conjoint analysis, were 71 per cent and 29 per cent, respectively. A closer look at the attribute levels discloses that participants showed positive utility for the cheapest product and a negative utility for the most expensive product. In addition, participants were more willing to buy a drug with a simple name and rejected the drug with a complex name. Thus, in general, a cough tablet named Fastinorbine that costs CHF 9.30 was the most preferred product.
Importance values of the attributes’ price and name and part-worth utility of each attribute level (total sample and clusters).
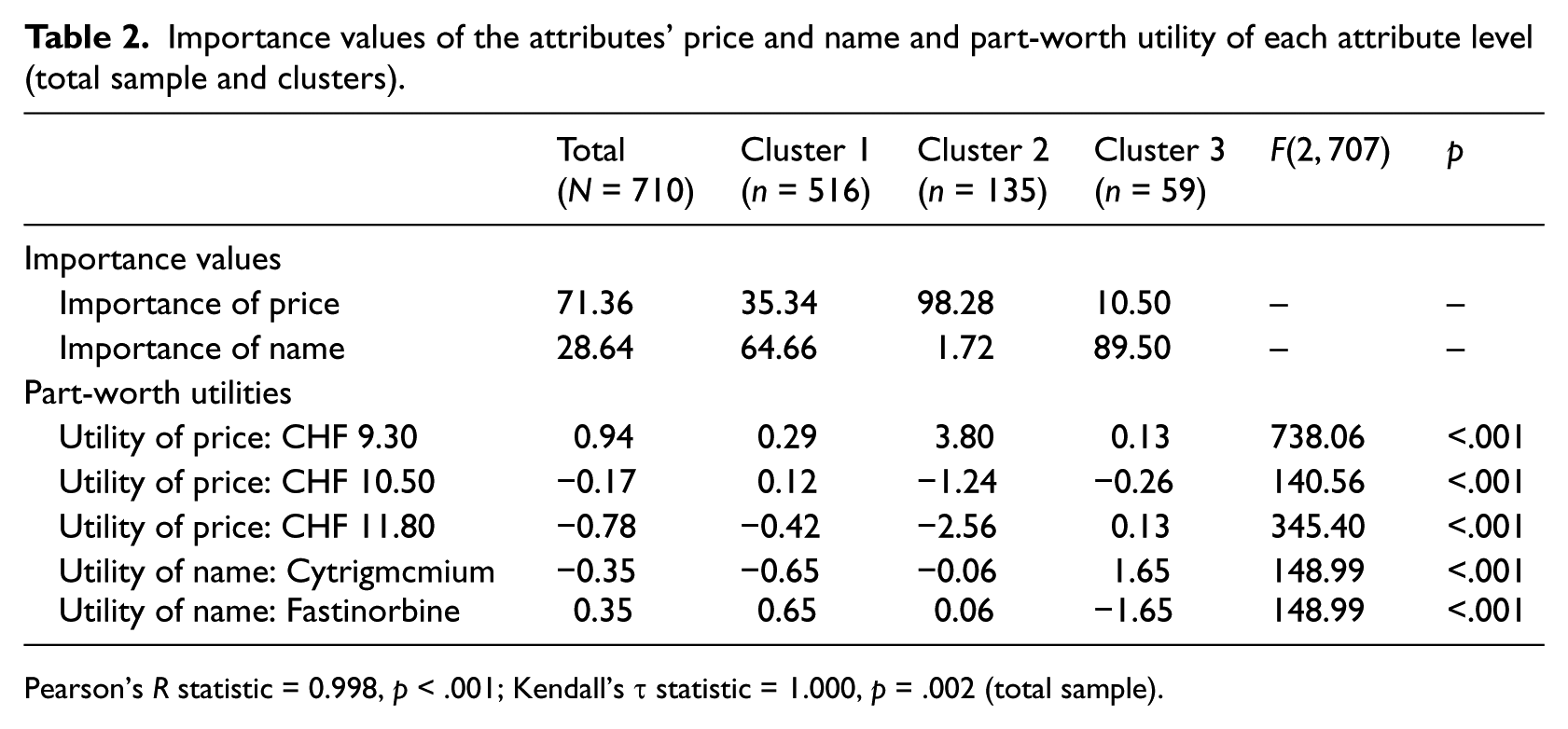
Pearson’s R statistic = 0.998, p < .001; Kendall’s τ statistic = 1.000, p = .002 (total sample).
Cluster analysis based on the individual part-worth utilities was used to detect preference heterogeneity and to classify participants into homogeneous subgroups. Hierarchical (Ward’s method) and k-means cluster analysis were used successively. A three-cluster solution was found to have the best fit, and part-worth utilities were significantly different between the clusters. Results of the conjoint analysis separately for each cluster together with the size of the cluster are shown in Table 2.
Cluster 1 was the largest cluster (n = 516). Both price and name of the drug played a role in participants’ willingness to buy, and in contrast to the total sample, name (65%) was more important than price (35%). Cluster 1 preferred a drug called Fastinorbine (a simple name) to a drug called Cytrigmcmium (a complex name). Cluster 2 represented a highly price sensitive group (n = 135). The cheaper the product, the more willing participants were to buy the drug. In contrast, Cluster 3 (the smallest cluster, n = 59) was characterized by high name sensitivity; participants in this cluster placed much more importance on the name (90%) than on the price of a drug (10%). Notably, Cluster 3 was the only group that was more willing to buy a drug with a complex name than a drug with a simple name. The results for Cluster 3 suggest that a simple drug name may not always lead to more positive evaluations, and it is possible that Cluster 3 applied the representativeness heuristic when evaluating different drugs.
In summary, the implications from Study 3 are threefold. First, the findings show that the name of a drug is a crucial determinant for people’s behavioural intentions to buy a drug, even if another highly relevant attribute is given together with the name, that is, the price. Because a clear range of prices was presented in Study 3, price was also easier to evaluate than the name of the drug; still, the name was an important criterion for many people. Second, the conjoint analysis highlights that most people would buy a drug that bears a simple name. Together with Studies 1 and 2, this result provides clear support for the fluency hypothesis. Third, there were segments of respondents who either (a) did not care about the drug name because they were only focused on the price of the product or (b) preferred complex to simple names, presumably because they used the name’s representativeness as a heuristic. These segments were identified via cluster analysis, and they were relatively small. Taken together, the finding that simple drug names increase positive product evaluations stands as a remarkably robust phenomenon.
General discussion
In three studies, we found strong evidence that fluency is most relevant for evaluations of drug names. In general, people judged drugs with simple names as safer, assumed that those drugs had fewer side effects and were more willing to buy those drugs. Our results have important implications for health promotion and brand naming. From our research, the assumption can be made that people believe that a drug with a complex name will lead to more side effects, and thus, they will be less inclined to buy the product. This is of particular importance given the fact that there is a worldwide trend to make more drugs available for self-medication. Thus, decisions at the point of purchase of OTC drugs may be influenced by factors other than recommendations from health professionals, and our results suggest that the name of the drug may be an important determinant of people’s purchase decisions. This effect might be particularly strong for product innovations. Compared to established products, new products or product lines are influenced little by habits. Thus, heuristic cues such as the complexity of the drug’s name will presumably be more relevant for people’s decisions when new products are introduced onto the market.
This research is not limited to OTC drugs. The complexity of a drug’s name may also have an influence on a patient’s evaluation of prescribed drugs. In Study 2, participants were asked to evaluate and indicate willingness to buy an anti-cancer drug. Although these types of medications are only available by prescription, participants gave consistent answers for these drugs. An anti-cancer drug with a complex name was perceived as more hazardous than an anti-cancer drug with a simple name. Likewise, willingness to buy was higher for an anti-cancer drug with a simple name. Thus, the effect of fluency is not limited to the type of drug (OTC or prescription drug) or to the disease (simple or complex and life threatening).
Therefore, we believe that the effect of a drug’s name may have far-reaching consequences. Because a complex name for a prescribed drug leads patients to believe that the drug has many side effects, the possibility exists that complex drug names may lower the extent to which patients take medications as prescribed by their health-care providers. Poor medication adherence is common and related to poor health outcomes and increased health-care costs (Gray et al., 2011; O’hea et al., 2005; Osterberg and Blaschke, 2005; Saal and Kagee, 2012). In contrast, a simple name may awaken false expectations about the safety of a drug, leading to possible overuse. It should be noted, however, that these hypotheses were not measured directly in this study, and further studies should provide more direct evidence that the name of a drug has an effect on dosing or medication adherence.
Some limitations of our research have to be addressed. Participants were confronted with hypothetical scenarios. Quite possibly, people may react differently when they are really affected by a disease. However, the existing literature shows that the influence of heuristic cues (such as the complexity of a name) is even more pronounced when people are stressed and distracted (Chaiken, 1987). Accordingly, we may have even underestimated the effect of a drug name’s complexity on people’s evaluations and preferences. Examination of real-world data would be interesting for further investigation of whether the influence of a name’s complexity on people’s evaluations is a robust finding and still plays a role in naturalistic settings.
In summary, our studies suggest that a drug name is a powerful determinant of people’s evaluations and intentions. Whether it is a rather harmless headache or a life-threatening disease, this research indicates that a complex drug name raises different expectations compared to a simple drug name. Results of three experimental studies showed that complex drug names were perceived as more hazardous than simple drug names and negatively influenced willingness to buy.
Footnotes
Acknowledgements
We would like to thank Nadine Belser, Nina Spiri and Cristina Zulian for their indispensable practical support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.