
Abstract
This descriptive cross-sectional study aimed to explore emotional representation and illness coherence, the understanding a person has about an illness which helps them make sense of the experience, in Russians with tuberculosis. In a secondary analysis of questionnaires from 105 Russians treated for pulmonary tuberculosis, social isolation and disease consequences were predictors of negative emotions related to tuberculosis and accounted for 49 percent of the variance. Participants who scored higher on illness coherence were less likely to experience negative emotions. Development of programs to help patients understand tuberculosis and to manage emotional responses and stigma is suggested.
Tuberculosis (TB) is a significant health threat, causing approximately two million deaths per year globally, and multi-drug and extensively drug-resistant forms of TB are rising (Dara and Kluge, 2011). Russia is one of 22 countries with a high disease burden and escalating rates of drug resistance (Dara and Kluge, 2011). In general, TB drug resistance, disease transmission, morbidity, and mortality are increased by delay in seeking treatment and poor adherence to prescribed medications (Craig et al., 2007; Dara and Kluge, 2011). In Russia, the causes of treatment delay and poor adherence are multifaceted, and little is known about the relationships between the emotional representation of TB, illness coherence, stigma, treatment delay, and medication adherence.
Review of the literature
Stigma is associated with diseases such as HIV/AIDS (Nyblade et al., 2009) and leprosy (Rafferty, 2005), and TB is also one of the diseases shown to produce stigma (Karim et al., 2007). Stigma exists when a person with an identifiable difference is labeled as different by other members of the social group. The labeled person is set apart from the group and often experiences discrimination by those holding status and power. Stigma is more pronounced when the difference is considered dangerous to others (Link and Phelan, 2001). In TB, stigmatization may arise as a result of the serious consequences associated with TB, such as its infectiousness or the fact that many people still believe TB is not curable (Khan et al., 2000).
People with stigmatized diseases have been shown to experience strong negative emotional responses (Richards et al., 2003), and this includes people diagnosed with TB. Women with TB in Bangladesh had higher levels of emotional stress, including shame and embarrassment (Karim et al., 2007). Depression and anxiety were also reported by Bangladeshis with TB (Husain et al., 2008). In a study of Russians with TB, 60 percent of the participants struggled with depression (Jakubowiak et al., 2008). Higher levels of depression and anxiety have been associated with a greater symptom burden, perceived seriousness of TB, and less control over TB treatment (Husain et al., 2008). Emotional responses to disease have been shown to affect treatment-seeking and adherence in TB (Barnes et al., 2004; Jakubowiak et al., 2008).
Sources of stigma include patients’ families, employers, and healthcare workers. Bangladeshi women with TB reported having families force isolation upon them (Karim et al., 2007). Healthcare workers in an urban district of Ghana strictly controlled patients’ actions and often shouted at them for getting too close to others; healthcare workers would only speak to these patients from a distance (Dodor et al., 2009). Necessary isolation precautions and prolonged duration of hospitalization exacerbate feelings of loneliness and abandonment (Chang et al., 2004b). More than half of the non-adherent TB patients in one study in Russia did not trust their TB physician, and many believed the physicians and nurses were hostile to them (Jakubowiak et al., 2008). Ecuadoreans with TB reported fear of losing their job prevented them from informing employers of their diagnosis (Armijos et al., 2008; Chang et al., 2004a). These fears were not unfounded as 15 percent of employers confirmed they would fire a person immediately upon learning of a diagnosis of TB (Armijos et al., 2008). In several studies, including one study in Russia, the fear of stigmatization, isolation, and the loss of family, social roles, and finances affected people’s decision to seek treatment and/or to adhere to treatment (Armijos et al., 2008; Dodor et al., 2008; Woith and Larson, 2008). There is still a lack of research about the relationship between negative emotions associated with TB and stigma among people with TB in Russia, and the roles these play in making decisions to seek and adhere to treatment.
Theoretical framework
Leventhal’s Common Sense Model of Self-Regulation (CSM) provided the theoretical framework for this study (Leventhal et al., 1992, 2001). The CSM has been widely used to describe relationships among variables in studies of illnesses such as hypertension (Hekler et al., 2008), diabetes (Mann et al., 2009), myocardial infarction (Cherrington et al., 2004), and depression (Fortune et al., 2004), among many others. This parallel processes model has both cognitive and emotional branches (Leventhal et al., 1992, 2001). The cognitive branch describes illness representation (how a person self-diagnoses illness) which consists of five attributes (identity, timeline, consequences, cause, and control) triggered by symptom onset. Illness identity is the label a person gives to a set of experienced symptoms. Timeline is the perceived duration of the illness and can be acute/chronic, or cyclical. The person also associates consequences with the illness and believes that there are specific causes, and that personal actions and/or treatment can cure or control the disease. Emotional representation focuses on negative feelings of depression, upset, anger, anxiety, worry, and fear experienced by the person upon making the self-diagnosis (Leventhal et al., 1992, 2001). These emotions can be related to a number of physical, cultural, or social factors (i.e. social stigma, family, or personal history) (Hagger and Orbell, 2003). The person develops action plans to cope with both illness and emotional representations.
Illness coherence is defined in Leventhal’s CSM as the mental model or understanding a person holds about an illness that helps them make sense of the experience (Jopson and Moss-Morris, 2003; Leventhal et al., 2001). People who believe they understand their illness (those with high illness coherence) have reported fewer negative emotions (Moss-Morris et al., 2002), and this may affect adherence and treatment-seeking. The effect on treatment-seeking and adherence may occur because enhanced understanding leads to a feeling of greater personal control and a stronger sense that their disease is treatable (Richards et al., 2003). It is unknown whether higher illness coherence may improve treatment-seeking and adherence among Russians with TB.
Purpose
Although there have been many studies on cognitive perceptions of TB, few have focused on emotional representation and illness coherence in treatment-seeking behaviors and medication adherence among people with TB; there are no published studies on these issues relating to Russians with TB. Given that TB patients are initially hospitalized for 3 months (or longer if diagnosed with drug-resistant TB), it is important to understand their perceptions of TB, including emotional representation and illness coherence, as well as understanding the association these may have with decisions to seek treatment and adhere to TB medications. The aims of this study were (a) to explore the relationships between emotional representation and illness coherence with illness representation, stigma, delay in seeking treatment, and TB medication adherence; (b) to identify predictors of emotional representation; and (c) to determine whether emotional representation and illness coherence predicted delay in seeking treatment and medication adherence in Russians with pulmonary TB.
Methods
Design, sample, and setting
We used a cross-sectional descriptive design to conduct a secondary analysis of the Tuberculosis Delay and Adherence dataset (Woith and Larson, 2008). The original study was conducted at two TB clinics in the Vladimir region of Russia (Woith and Larson, 2008). This region supports 15 outpatient TB clinics; the clinics used in this study were selected because of their size.
People with TB in Russia are admitted to specialized TB hospitals for the first 3 months of treatment, or possibly longer if their TB is drug-resistant. They are then discharged to outpatient treatment where medications are administered at clinics by medical staff using directly observed therapy. Participants needed to be 18 years or older, diagnosed with active pulmonary TB, and receiving medications at one of the two clinics (Woith and Larson, 2008). Of the 117 adults who met eligibility criteria, 11 declined to participate. One survey was not usable due to missing data, leaving 105 participants for a response rate of 91 percent.
Instruments and variables
We used the modified committee approach to translate study instruments from English into Russian (Behling and Law, 2000). Two bilingual Russians independently translated the instrument from English into Russian and then met with the Primary Investigator to reconcile discrepancies.
Revised Illness Perception Questionnaire
The Revised Illness Perception Questionnaire (IPQ-R) (Moss-Morris et al., 2002) was designed to measure concepts of Leventhal’s CSM, and we used it to measure emotional representation, illness coherence, and illness representation. The IPQ-R has seven subscales measuring each of the model concepts. These subscales are emotional representation, illness coherence, and the attributes of illness representation (illness identity, timeline, cause, consequences, and personal/treatment control). This instrument is designed to be adapted for use with various diseases, and researchers are encouraged to make additions to the instrument, which specifically reflect characteristics of the disease under study. Changes made to the instrument for this study are described below.
The emotional representation subscale measures emotions generated by disease (specifically, depressed, upset, anger, anxiety, worried, and afraid) (Moss-Morris et al., 2002). We adapted the items to reflect the TB, the illness we were exploring (for example, having tuberculosis makes me feel anxious), and removed the subscale item my tuberculosis does not worry me due to low inter-item reliability. Illness coherence measures the individual’s understanding of their illness through questions such as my tuberculosis is a mystery to me and my tuberculosis doesn’t make any sense to me (Moss-Morris et al., 2002). The control/cure subscale is divided into personal control (the participant’s belief that their actions can affect the disease) and treatment control (the participant’s belief that the disease can be controlled or cured through medical treatment). Consequences identify the participant’s perception of illness severity. Timeline identifies the perception that the illness is cyclical or will last a short or long time. These subscales are all measured on a 5-point Likert-type scale, with 1 being “strongly disagree” and 5 being “strongly agree.” Each subscale is summed; there is no composite instrument score (Moss-Morris et al., 2002).
To determine illness identity, participants first identified all the symptoms they experienced prior to diagnosis of TB and then selected symptoms they believed were caused by their TB. The sum of perceived TB-related symptoms comprised the illness identity score. The original identity subscale consisted of 14 symptoms commonly associated with illness (Moss-Morris et al., 2002). Seven additional symptoms identified in literature from organizations that specialize in treating TB were added to this scale (i.e. persistent cough, elevated temperature, night sweats, chest pain, decreased appetite, difficulty breathing, and blood in sputum) (Taylor et al., 2005).
In the cause subscale, participants selected items they believed caused their TB, such as a germ or virus, stress or worry, or heredity. The instrument is designed so that additional causes can be added, as appropriate to the illness under study. The causal items already present in the original instrument were appropriate for TB, so no further items were added. We conducted an exploratory factor analysis that resulted in five factors (citation here). Personal behavior encompassed the belief that their own behaviors were responsible for their TB. Emotional burnout included items that related TB to factors associated with the difficulties inherent in their daily lives and relationships which put them in an emotional state that leads to exhaustion and lower resistance. Uncontrollable circumstances described environmental factors outside of a participant’s control, such as pollution or genetics. Demoralization was participants’ belief that their condition resulted from not taking proper care of themselves, leading to a negative outlook on life. Medical misfortune was the knowledge that TB was caused by a germ which they were unfortunate enough to have contracted, with stress compounding the event (citation here).
Adaptations were made to the IPQ-R. The neutral response category (3 = neither disagree or agree) of the 5-point Likert-type scale was deleted from the Russian language version of the IPQ-R because Russians are more likely to select a neutral category when available (Carnaghan, 1996). This changed the scoring to a 4-point scale with item ratings from 1 (strongly disagree) to 4 (strongly agree). The cyclical timeline subscale was not used in our analyses because TB is not cyclical. Personal control and treatment control had low scale reliability in the Russian language version and so were not used in analyses. The IPQ-R has only been used in one other study of people with TB in Russia.
Social Impact Scale
The Social Impact Scale (SIS) was used to measure two dimensions of stigma: enacted stigma (containing the subscales social rejection and financial insecurity) and perceived stigma (containing the subscales internalized shame and social isolation) (Fife and Wright, 2000). Responses were rated from 1 (strongly disagree) to 4 (strongly agree). Higher scores were correlated with a greater awareness of stigmatization. The SIS captures financial and social impacts of stigma that have been linked to treatment-seeking delay and medication adherence in people with TB. One item, I feel I need to keep my illness a secret, was deleted from the internalized shame subscale to improve scale reliability. No other changes were made.
Delay seeking treatment and medication adherence
Delay in seeking treatment was measured with a question asking participants to mark the correct time interval between onset of symptoms and seeing a physician. Research team members accessed clinic medication administration records to determine adherence, which was calculated by dividing the number of ingested doses by the number of prescribed doses. Sample characteristics of age, gender, location, smoking, and alcohol use were collected.
Procedure
In the original study, potential participants were notified of the opportunity to participate through flyers at the two TB outpatient clinics (citation here). After patients had taken their daily medications, research assistants invited them to participate. Informed consent was obtained from all participants, and then they completed the survey. Participants were given 125 rubles (approximately US$4.80) for their time investment. Research assistants reviewed medication records when each completed survey was returned. Data from all 105 participants in the original study were analyzed in this secondary analysis.
Protection of human participants
This study was a secondary analysis of de-identified data, and no approval was required by the Institutional Review Board (IRB) at Illinois State University. The University of Illinois at Chicago’s IRB approved the original study (citation here).
Data analysis
Data analysis was done using SPSS version 18.0. Descriptive statistics were used to describe sample characteristics, delay, and adherence. Bivariate correlations were run to identify relationships among the variables. Multiple regression analysis was used to identify predictors of emotional representation. Alpha for these analyses was .05.
Results
In this section, we first describe samplecharacteristics and scale means and then report other findings according to the aims of the study. The majority of participants were men (68%) (Table 1). Mean age was 40 years. 48 men and 18 women participated from Clinic 1, and 23 men and 16 women participated from Clinic 2. In all, 48 participants (48%) delayed seeking treatment for 4 weeks or longer after symptom onset; 48 participants were less than 100 percent adherent to their medication regimen.
Sample characteristics.

SD: standard deviation.
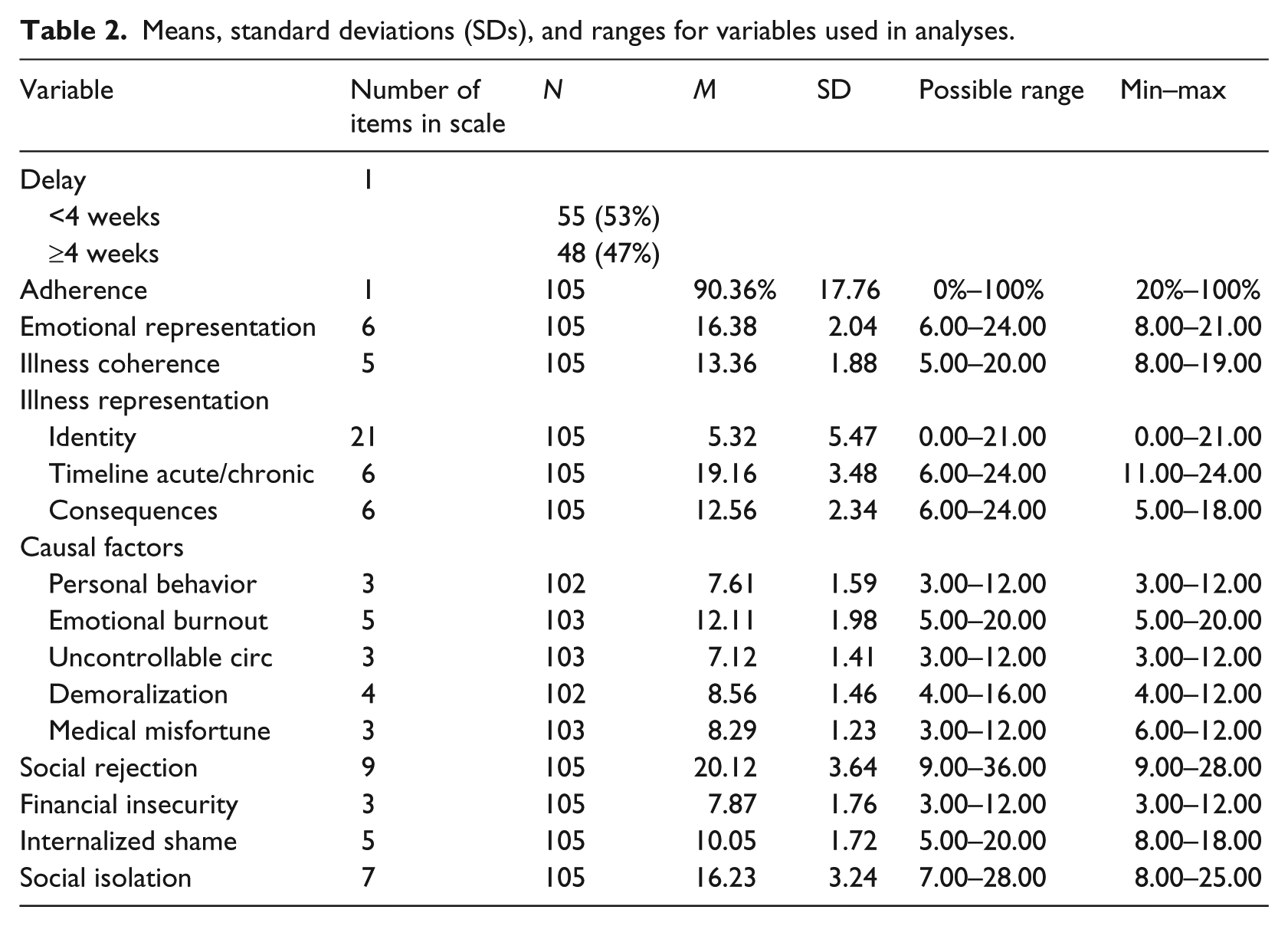
Emotional representation mean (M = 16.38, possible range: 6.00–24.00) was above the scale midpoint, indicating that participants were more likely to have experienced negative emotions related to their TB, such as depression, upset, anger, anxiety, and fear (Table 2). Mean score for illness coherence (M = 13.36; possible range: 5.00–20.00) fell above midpoint, indicating that participants were more likely to believe they understood their TB. Mean scores on IPQ-R subscales measuring attributes of timeline acute/chronic, and consequences, and on all SIS subscales fell above subscale midpoints.
Means, standard deviations (SDs), and ranges for variables used in analyses.
Older adults (r = .224, p = .022) and women (r = −.216, p = .027) were most likely to attach strong negative emotions to their TB. Older adults (r = −.302, p = .002) also demonstrated lower illness coherence, indicating they were less likely to believe they understood their TB than were younger adults.
Our first aim was to explore the relationships between emotional representation and illness coherence with illness representation, stigma, delay in seeking treatment, and TB medication adherence. Pearson’s two-tailed correlation was used to find relationships between these variables.
Emotional representation and illness representation
Participants were less likely to experience negative emotions associated with TB if they scored higher on illness coherence than people who scored lower on illness coherence (r = −.264; p = .007). Participants who experienced strong negative emotions associated with their TB perceived TB as having serious consequences (r = .543; p < .001) and perceived TB as being a chronic or long-term disease (r = .427; p < .001). Emotional representation was positively correlated with the causes emotional burnout (r = .325, p = .001) and demoralization (r = .359, p < .001), showing that people who experienced strong negative emotions related to having TB were also more likely to feel anxious, overworked, and burdened with family problems which they believed had made them more susceptible to TB. They were also less likely to have taken good care of themselves physically or mentally, and felt worn down and pessimistic. Emotional representation was not correlated with illness identity (r = .020, p = .840) or the causes of personal behavior (r = .109, p = .273) and uncontrolled circumstances (r = .150, p = .130).
Illness coherence and illness representation
Participants who scored higher on illness coherence, meaning they believed they understood their TB, were less likely to believe that TB had serious consequences (r = −.198; p = .044). Illness coherence was negatively correlated with the causes of personal behavior (r = −.264, p = .008), emotional burnout (r = −.384, p < .001), and demoralization (r = −.279, p = .005). This demonstrates that participants who believed they had a good understanding of their TB perceived their actions (such as smoking and drinking) did not cause their disease. They were also less likely to feel anxious, dejected, or worried about work and family, and they believed they had taken better care of themselves and so were not feeling worn out and pessimistic.
Emotional representation and stigma
Emotional representation was associated with both enacted and perceived stigma. Specifically, negative emotions associated with TB were positively correlated with social rejection (r = .625, p < .001), financial security (r = .473, p < .001), internalized shame (r = .350, p < .001), and social isolation (r = .648, p < .001).
Illness coherence and stigma
Illness coherence was negatively correlated with social rejection (r = −.250, p = .011), internalized shame (r = −.327, p = .001), and social isolation (r = −.369, p < .001), indicating that participants who had a good understanding of TB also felt less stigmatized. There was no relationship between illness coherence and illness identity (r = −.017, p = .862), timeline acute/chronic (r = −.069, p = .490), or the cause factor uncontrolled circumstances (r = −.062, p = .536).
Delay in seeking treatment and TB medication adherence
There was no relationship between emotional representation and delay in seeking treatment (r = .001, p = .991) or adherence (r = −.092, p = .348), or between illness coherence and delay in seeking treatment (r = .026, p = .796) or adherence (r = −.088, p = .376). We did not expect this finding.
Our second aim was to identify predictors of emotional representation. Regression analysis was conducted to test whether attributes of illness representation that were correlated with emotional representation explained the variance in emotional representation; specifically, we tested timeline acute/chronic, consequences, cause categories of emotional burnout and demoralization, and illness coherence (Table 3). Concepts of stigma that were correlated with emotional representation were also included. Age and gender were added in the first block, and the remaining variables were added in stepwise order in the second block. In the third model, with all variables in the equation, the adjusted R2 value indicated that almost half of the variability in emotional representation was predicted by social isolation and consequences, controlling for age and gender. Collinearity scores were female = .954, age = .896, social isolation = .530, and consequences = .579. Durbin–Watson test for serial correlation of the residuals was 1.907.
Predictors of emotional representation.

CI: confidence interval.
p < .05; **p < .01; ***p < .001.
Our third aim was to determine whether emotional representation and illness coherence predicted delay in seeking treatment and medication adherence in Russians with pulmonary TB. However, delay in seeking treatment and adherence to TB medications were not significantly correlated with illness coherence or emotional representation and so no further analyses were run.
Discussion
We report three main findings: emotional representation was strongly related to feeling stigmatized; people who believed they understood their TB were less likely to report negative emotions associated with TB, serious consequences, or stigma; and social isolation and consequences of TB were predictors of emotional representation.
Participants with strong negative emotional representations of their disease were more likely to have experienced enacted and perceived stigma. This has implications for healthcare workers, as they may not be prepared to manage the psychological and emotional needs of patients with TB. Hasler et al. (2009) found that healthcare workers in Russia did not assess the emotional needs of their patients with TB, nor were they aware of their own feelings. Healthcare workers employed in TB care facilities participate in annual continuing education programs, but these programs do not include content on managing emotional needs of patients. Including sessions on assessing and managing emotional needs may help healthcare workers provide better emotional support; incorporating experiential activities that help healthcare workers understand and value their own feelings may be beneficial in decreasing some of the stigmatization patients report experiencing from healthcare workers. Programs could also be designed to provide content on helping patients develop better coping skills to manage the experience of stigma.
People who believed they understood their TB were less likely to report negative emotions associated with TB, social isolation, social rejection, or internalized shame. Although we were able to describe the relationship between emotional representation and illness coherence, our study was not designed to identify a cause-and-effect relationship between these two variables. It is as likely that negative emotions may prevent understanding of TB as it is that poor understanding of TB may result in fear, anxiety, and other negative emotions. It is also possible that there is a mediating or moderating effect. The need to manage negative emotions associated with TB and understanding of the disease is evident, however, and further studies are needed to determine whether cause and effect exist as well as to identify interventions.
Social isolation and consequences of TB were predictors of negative emotions of TB. Social isolation is a valid concern as patients with TB in Russia are hospitalized for 3 months or longer. This extended time away from family, friends, and the daily routine of life would seem likely to generate feelings of being “set apart from others,” leading them to feel “lonely” and “useless.” Developing support groups for people diagnosed with TB could help manage these feelings. Including families in support groups or classes to help them better understand TB might also help reduce stigma.
Although social isolation and consequences accounted for almost half of the variability in emotional representation, emotional responses may also arise independently of stigma (Hagger and Orbell, 2003). For example, job loss can occur as a result of stigma, but it may also occur because an employee is too ill to work, or may be unrelated to the illness altogether. Therefore, people may experience anxiety and fear over the possibility of loss of job and income because they will not be able to feed their families. We found that emotional responses were more negative as people experienced difficulties in their daily lives and relationships. Further research is needed to develop a better understanding of emotions beyond those generated by stigma.
We did not find a direct relationship between emotional representation and delay or adherence; however, there was a strong correlation between negative emotions associated with TB and stigma, and stigma has been shown to be a predictor of adherence (Woith and Larson, 2008). Consequently, it is possible that there is an indirect relationship between emotional representation and adherence. Our study was not designed to test for an indirect relationship, and further exploration is suggested.
Understanding emotional and cognitive factors involved in patients’ perceptions of TB is important to providing holistic care. These multifaceted factors involve not only the patient’s negative emotions but also their perception of accompanying stigmatization. Understanding the patient’s perspective is important to developing educational programs and providing psychological support to more effectively meet their needs.
Limitations
This was a cross-sectional study, so cause-and-effect relationships cannot be determined. Participants were drawn from the outpatient clinic population in two cities in the Vladimir Region. Drawing from different geographic regions increases generalizability, but the findings remain limited to this population. The Russian language version of the IPQ-R needs further revision to improve scale reliability for some of the subscales.
Conclusion
TB is associated with serious emotional and social consequences, and this article adds to the understanding of Russian TB patients’ perception of their TB. As illness coherence improves, the negative emotional and social consequences of the disease may lessen. It is the role of Russian healthcare professionals to provide their patients with adequate education and psychological support, and this role requires preparation. Development of programs preparing healthcare workers to identify and treat the emotional responses, including stigma, associated with TB is suggested.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.