
Abstract
The objective of this study was to examine the impact of workplace bullying on self-esteem, including the mediating effect of internalized stigma and the moderating effect of spirituality, among hepatitis C virus patients. Data were collected from 228 employed hepatitis C virus patients who had been admitted to Gastroenterology and Hepatology wards in Pakistani hospitals. We found support for the hypothesis that workplace bullying is associated with low self-esteem via internalized stigma. In addition, spirituality moderated the association such that participants with greater spirituality were buffered from the impact of stigma on self-esteem.
Introduction
Hepatitis C virus (HCV) is positioned among the three most prevalent chronic viral infections worldwide, impacting millions of people (Alavian et al., 2005; McCarron et al., 1997). There are 10 times more people living with HCV than HIV (Joint United Nations Programme on HIV/AIDS (UNAIDS), 2006), making HCV a major global health problem (Brown and Gaglio, 2003). Many chronic diseases are associated with stigma or social devaluation and discrediting (Goffman, 1963). This stigma is manifested as prejudice and discrimination toward people with disease (Ainlay et al., 1986; Falk, 2001; Fiske, 1993; Wendell, 1990), and negatively impacts the social, psychological, and physical well-being of people living with disease. Emerging evidence suggests that HCV is associated with stigma, with people living with HCV reporting discrimination from others (Brener et al., 2007). Despite its widespread prevalence, researchers have argued that HCV is generally understudied (Zacks et al., 2006) and that HCV stigma is specifically understudied (Paterson et al., 2007).
Pakistan has the second highest prevalence rate of hepatitis in the world, with 18 million people living with either hepatitis B or C (Qasim, 2013). Hepatitis causes 150,000 deaths in Pakistan annually. A total of 11 million people are living with HCV specifically, with a 20 percent greater prevalence than other Asian countries (Bashir et al., 2012). Recent work suggests that disease-related stigma is generally understudied in Asian countries (Brohan et al., 2010; Reidpath et al., 2005), ultimately leading to less knowledge of disease-related stigma in Asian contexts. We argue that stigma associated with HCV is important to study in Pakistan due to both the high prevalence of HCV in Pakistan and the dearth of studies examining stigma associated with chronic disease in Asian contexts such as Pakistan.
Thanks to improved health care and treatment, people living with HCV in Pakistan are living longer and healthier lives. Many are employed. Yet, many people living with chronic diseases experience stigma in the workplace (Surgevil and Akyol, 2011). This stigma impedes career progression and personal development opportunities for individuals living with chronic diseases (Jagose, 1997) and further hinders organizational success (Judge and Cable, 2011; Paetzold et al., 2008). Workplace stigma experienced by people living with HCV has received limited attention in comparison with workplace stigma experienced by people living with diseases such as HIV (e.g. see King, 1989; Malcolm et al., 1998). It is critical to understand the stigma-related experiences of people living with HCV in Pakistani workplaces to inform interventions to address stigma in these contexts (Pinel and Paulin, 2005), thereby facilitating more positive outcomes for both employees living with HCV and the organizations in which they work
In the current investigation, we focus on workplace bullying experienced by employees living with HCV in Pakistan. Workplace bullying, or harassment of individual employees (Zapf et al., 1996), has received considerable attention in the literature (Samnani, 2013). When directed at people living with socially devalued characteristics such as HCV, workplace bullying can be conceptualized as a manifestation of stigma similar to discrimination. Experiences of stigma affect self-esteem (Wiener et al., 2012), and we argue that experiences of workplace bullying among employees living with HCV ultimately lower their self-esteem. Additionally, because spirituality induces tolerance (Mitroff, 2003), we hypothesize that spirituality can help reduce the impact of stigma on self-esteem. This study aims to explore these associations within a sample of employees living with HCV in Pakistan.
Theory and hypotheses
Workplace bullying and self-esteem
Bullying is characterized by devaluation of others (Hadjifotiou, 1983) and often involves emotional abuse (Keashly, 1997) and aggression (Einarsen and Raknes, 1997a, 1997b). Resultantly, individuals who experience workplace bullying may feel worthless (Einarsen, 1999), devalue themselves, and even experience self-hatred (Reece, 2003). Bullying may therefore threaten self-esteem, which is characterized by self-worth or self-respect (Crocker and Quinn, 2000; Quinn and Crocker, 1999) and is associated with happiness (Michalos, 2004). These findings suggest that stigma affects individual employee’s self-esteem, and thus, we propose our first hypothesis as follows:
H1. Workplace bullying is negatively associated with self-esteem.
Mediating role of internalized stigma
Experiences of discrimination, including bullying, have potential to damage psychological well-being and threaten individual identity (Major and O’Brien, 2005). Recent longitudinal evidence suggests that perceptions of public stigma predict increased internalized stigma over time (Vogel et al., 2007). That is, people who perceive greater social devaluation associated with a characteristic are more likely to endorse negative beliefs and feelings associated with that characteristic and ultimately apply those beliefs and feelings to the self. Perceptions of public stigma may be driven by experiences of discrimination, including workplace bullying. People who experience greater workplace bullying associated with HCV may perceive greater stigma associated with HCV and, in turn, internalize HCV stigma. Internalized stigma undermines feelings of self-worth (Major and O’Brien, 2005) and thus is associated with lower self-esteem (Hinshaw, 2004, 2005; Miles et al., 1997; Ow and Lee, 2015; Wiener et al., 2012). Therefore, our second hypothesis is as follows:
H2. Internalized stigma mediates the relationship between workplace bullying and self-esteem.
Moderating role of workplace spirituality
Workplace spirituality involves a linkage between employees’ inner lives and their surroundings, wherein their inner lives are nourished by meaningful work that leads to self-development (Ashmos and Duchon, 2000; Barnett et al., 2000; Mitroff and Denton, 1999). Spirituality aids in individuals’ search for meaning and purpose in life (Karakas, 2010; Tepper, 2003).
A recent study suggests that spirituality moderates the relationship between stigma and depression among people living with HIV (Chaudoir et al., 2012). Spirituality may buffer people experiencing discrimination from poor mental health because it helps them cope with stressors such as discrimination (Szaflarski, 2013) and provides important support (Grodensky et al., 2015). Spirituality may ultimately serve as a resistance resource (Sowell et al., 2000), helping people living with stigmatized characteristics achieve positive health outcomes despite stigma (Ritsher et al., 2003). We argue that spirituality will buffer the relationship between internalized stigma and self-esteem, and therefore, our hypothesis about the moderating role of workplace spirituality is stated as follows:
H3. Spirituality moderates the relationship between internalized stigma and self-esteem such that the association between spirituality and self-esteem is weaker when spirituality is high.
Figure 1 includes a visual depiction of our hypotheses.
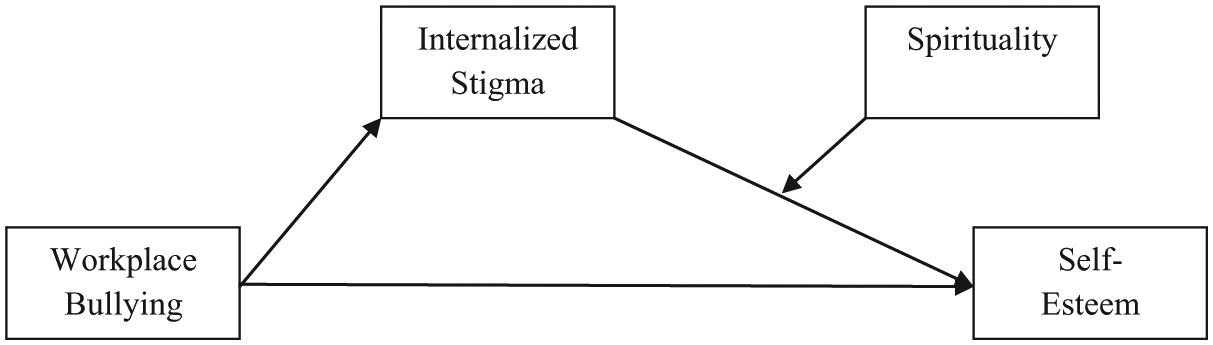
Conceptual figure of associations between workplace bullying and self-esteem.
Method
Population and sample
The first author visited hospitals across Pakistan and gathered information about HCV patients admitted in Gastroenterology and Hepatology wards. HCV patients were eligible for the study if they were employed in public sector organizations, banks, and academic institutions. Questionnaires were distributed to 350 HCV patients meeting these criteria. A cover letter explaining the purpose of the study was attached to the questionnaire, and the respondents were assured that the collected data would be used only for academic purposes and that individual surveys would not be shared with anyone. A total of 228 questionnaires were returned (65% response rate).
Regarding sample composition, 46.9 percent of respondents had attained an educational level of masters or above, 21.9 percent had attained a bachelor’s degree, and 31.1 percent had attained less than a bachelor’s degree. More participants were male (58.8%) than female (41.2%). Many participants (40.4%) were between 20 and 30 years old, with fewer between 30 and 40 years old (25.9%), 40 and 50 years old (11.8%), or 50 years or older (21.9%).
Measures
All items in the questionnaire were in English and self-reported using a five-point Likert-type scale with 1 representing “strongly disagree” and 5 representing “strongly agree.”
Workplace bullying
Workplace bullying was measured using the 22-item “Bullying at Work Scale” developed by Einarsen and Hoel (2001). Examples of items include the following: “Being ignored and excluded,” “Spreading of gossip and rumors about you,” and “Hints or signals from others that you should quit your job.” Alpha reliability for the scale was 0.84.
Internalized stigma
Internalized stigma was measured using the 11-item “Internalized Stigma Scale” developed by Earnshaw and Quinn (2012). Sample items included the following: “It is my fault that I have a health condition,” “I feel I’m not as good a person as others because I have a health condition,” and “Because I have a health condition, I’m not a good employee.” Alpha reliability for the scale was 0.87.
Self-esteem
The 10-item “Rosenberg Self-Esteem Scale” developed by Rosenberg (1965) was used to measure self-esteem. Examples of items include the following: “I feel that I’m a person of worth, at least on an equal plane with others,” “I take a positive attitude toward myself,” and “I wish I could have more respect for myself.” Alpha reliability for the scale was 0.71.
Spirituality
The 22-item “Human Spirituality Scale” developed by Wheat (1991) was used to measure spirituality. Sample items include the following: “I experience a feeling of being whole and complete as a person,” “I actively seek a sense of purpose in my life,” and “It is important that each of us find meaning in our lives.” Alpha reliability for the scale was 0.78.
Results
Table 1 includes correlations between the variables. There was a negative correlation between workplace bullying and self-esteem, indicating that greater workplace bullying was associated with lower self-esteem. Internalized stigma was positively correlated with workplace bullying and negatively correlated with self-esteem. Although internalized stigma and workplace bullying were highly correlated, the value inflation factor was lower than 10 indicating a lack of multicollinearity. The mean values of bullying and internalized stigma were above the scale midpoints, suggesting that participants generally agreed that they experienced workplace bullying and internalized stigma.
Means, standard deviations, and correlation.

SD: standard deviation.
p < .05 and **p < .01.
Table 2 includes the results of hierarchical regression analyses that were performed to test Hypotheses 1 and 2. In these analyses, demographic characteristics including age, gender, and qualification were controlled for within the first step. In support of Hypothesis 1, workplace bullying was negatively associated with self-esteem (Table 2). Therefore, participants who reported greater workplace bullying had lower self-esteem. In support of Hypothesis 2, workplace bullying was positively associated with internalized stigma indicating that participants who experienced more workplace bullying internalized greater stigma. Additionally, internalized stigma was negatively associated with self-esteem indicating that participants who internalized greater stigma had lower self-esteem. Controlling for the effect of internalized stigma, the effect of workplace bullying on self-esteem became statistically nonsignificant (Table 2, Step 3 of mediation analyses). Therefore, internalized stigma fully mediated the association between workplace bullying and self-esteem.
Results of hierarchical regression analyses.
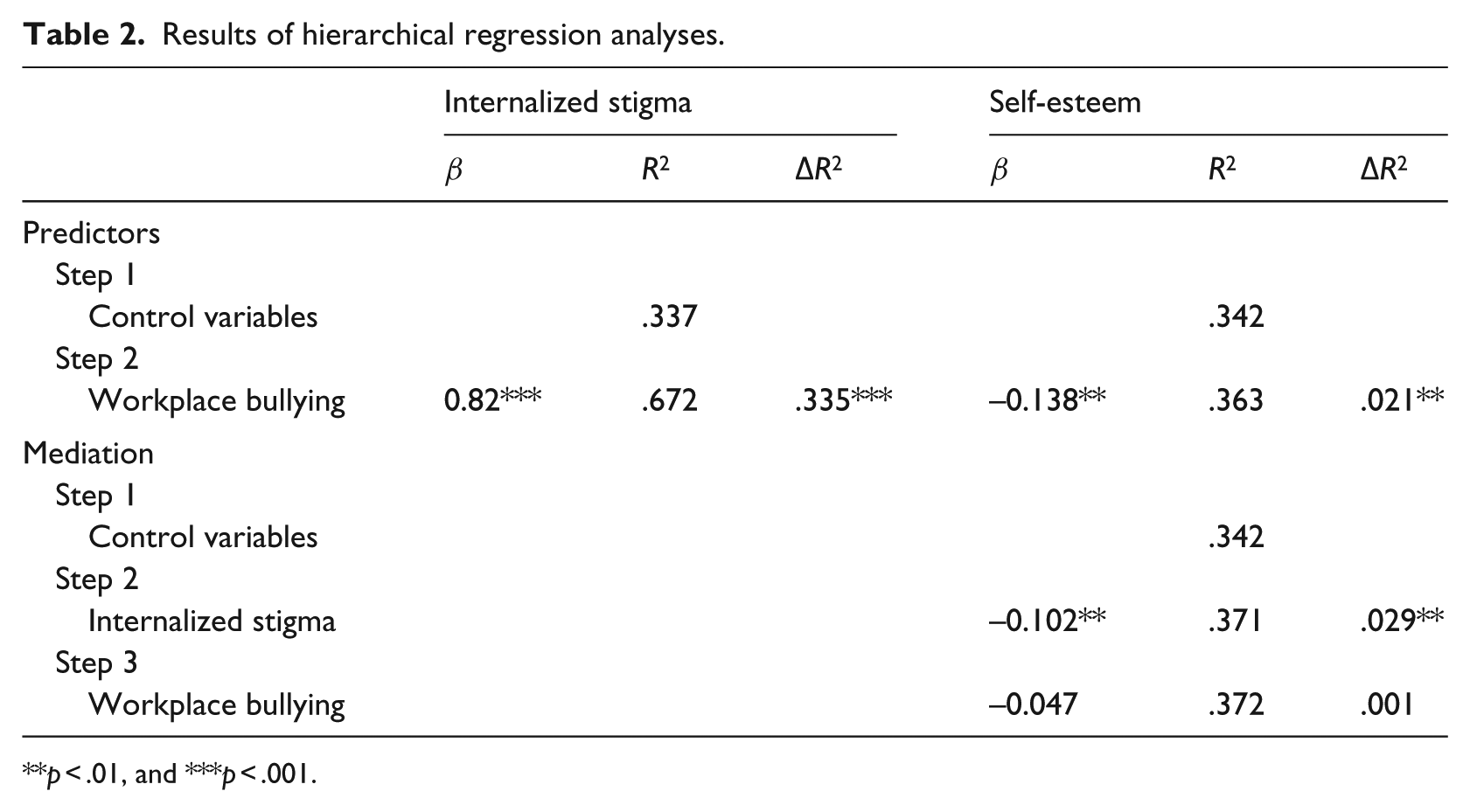
p < .01, and ***p < .001.
Table 3 includes results of a step-wise regression analysis to test Hypothesis 3. Demographic variables were again controlled for within the first step of the analysis, internalized stigma and spirituality were entered in the second step, and the interaction between internalized stigma and spirituality was entered in the third step. The interaction term was statistically significant, indicating that spirituality weakened the relationship between internalized stigma and self-esteem.
Results of a step-wise regression analysis.
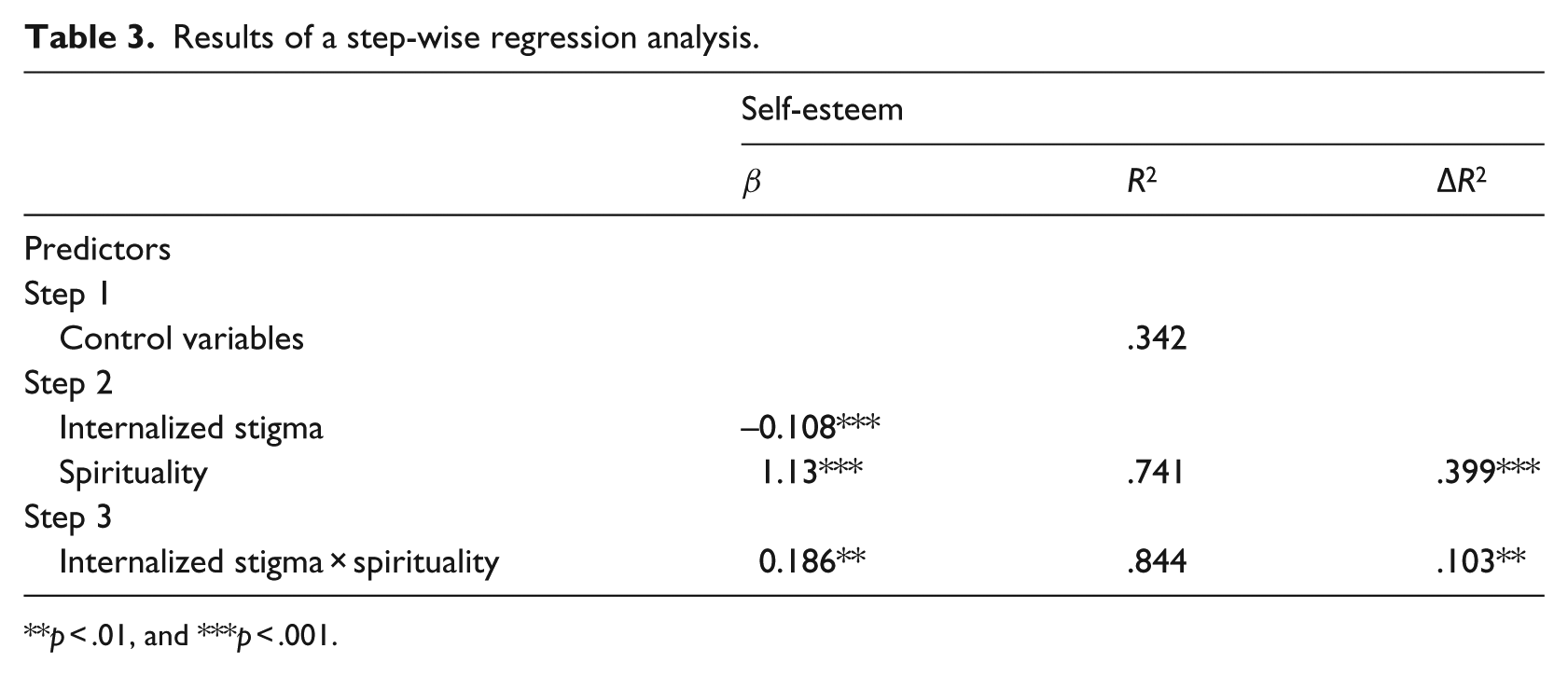
**p < .01, and ***p < .001.
Discussion
Results of this study provide insight into associations between HCV-related workplace bullying, internalized stigma, spirituality, and self-esteem in Pakistan. HCV stigma is an important, yet understudied, issue in many Asian countries. Consistent with previous work showing that workplace bullying lowers self-esteem (Einarsen et al., 1994; Vartia, 1996), workplace bullying was associated with lower self-esteem among people living with HCV in the current sample. This study further suggests that internalized stigma is a mechanism through which workplace bullying affects self-esteem. This process is supported by modified labeling theory (Link et al., 1989), which suggests that discrimination due to a socially devalued characteristic can lead individuals to devalue themselves and, in turn, experience poor outcomes (Kilinç and Campbell, 2009). In this study, discrimination in the form of workplace bullying was associated with internalized stigma, which in turn was associated with lower self-esteem among people living with HCV in Pakistan.
Many participants of this study reported experiencing workplace bullying and internalizing stigma associated with HCV. HCV stigma is strong in Pakistan. HCV is viewed as highly controllable, and people are considered personally responsible for acquiring HCV (Sambisa et al., 2010). People living with HCV may be assumed to engage in negligent or unsafe behaviors and may even be considered a threat capable of spreading the disease to others. Lack of awareness about modes of transmission through which HCV spreads may further fuel HCV stigma in the workplace. HCV is not spread through casual contact, yet participants of this study informally told one of the authors that their coworkers avoid eating and sharing utensils with them. For example, a custodial staff member who made tea in their office kitchen was banned from entering the kitchen once their HCV status was disclosed. They were yelled at by coworkers if found in the kitchen. Stigma associated with HCV is similar to stigma associated with HIV in workplaces in Pakistan, with both HCV and HIV stigma associated with negative workplace outcomes (Bashir, 2011).
In addition to demonstrating the negative impact of internalized stigma on self-esteem via internalized stigma, this study contributes to the disease-related stigma literature by suggesting that spirituality curtails the impact of internalized stigma on self-esteem. Although understudied in relation to stigma, spirituality offers a range of benefits which may help to explain why it is protective. Spirituality assists in cultivating purpose-fulness in one’s work (Emmons, 1999) and enhances motivation (Gotsis and Kortezi, 2008) to live purposefully and ethically in the workplace (Giacalone and Jurkiewicz, 2003). Spirituality further acts as a cognitive resource by helping people cope with illness and distress (Larson and Larson, 2003). Previous work suggests that spirituality can be a means to reducing negative psychological outcomes of diseases like HIV (Carson and Green, 1992), cancer (Ell et al., 1989), and spinal cord injury (Decker and Schulz, 1985). Our work extends this literature to HCV and suggests that spirituality can buffer people from the negative effects of internalized stigma on self-esteem. The spiritual beliefs of people living with HCV may help them to face distress associated with stigma and learn how to adapt to bullying and stigma in the workplace.
Limitations
This study provides a promising way to understand the complexity of HCV stigma. However, the results are not without limitations. The first limitation is in regard to the sample. Participants were from a convenience sample of people admitted to hospitals at the time of data collection; therefore, the generalizability of findings to other samples, including people who work in other domains, is unknown. Hence, future studies should seek to explore these associations among a more representative sample of people living with HCV from various work settings. Another consideration is that the high R2 value for control variables in explaining variation in internalized stigma and self-esteem (37% and 34%) indicates that we can expect a considerable impact of age, tenure, and gender on internalized stigma and self-esteem. Future studies may further explore the role of these demographic characteristics to better understand internalized stigma and self-esteem among employees living with HCV in Pakistan.
Conclusion
Stigma can be controlled in the workplace (Beatty and Kirby, 2006), and this study provides some insight as to how that can be achieved. We draw some tentative conclusions based on our results:
Although workplace bullying is associated with lower self-esteem via internalized stigma among people living with HCV, spirituality acts as a protective factor by reducing the harmful effects of internalized stigma on self-esteem.
Globally, there are many people living with HCV in numerous Asian countries (Thanachartwet et al., 2007; Wang et al., 2008) where stigma is not appropriately understood (Van Rie et al., 2008). Very few studies have addressed HCV in Pakistan, however, where HCV prevalence is frighteningly high (Kuo et al., 2006). Employers need to acknowledge and reduce HCV bullying and stigma to achieve more positive outcomes for both individuals living with HCV and the overall organizations in which they work.
Because spirituality has a beneficial impact on self-esteem, organizations may design interventions focusing on enhancing spirituality to improve the self-esteem of employees living with HCV.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.