
Abstract
This study sought to examine whether two facets of weight self-stigma (fear of enacted stigma and self-devaluation) were associated with weight change and treatment engagement for 188 individuals participating in a 3-month online weight loss program. Fear of enacted stigma predicted less weight loss 3 months later after controlling for demographics, eating problems, and psychological symptoms. Self-devaluation did not predict weight loss. Neither weight self-stigma variable predicted engagement in the online program. These results add to the literature indicating the negative effects of weight self-stigma while highlighting the central role of fear of being stigmatized by others in this process.
Introduction
People with obesity are frequently exposed to bias, discrimination, and ridicule (e.g. Carr and Friedman, 2005; Karnehed et al., 2006; Maranto and Stencien, 2000; Puhl and Heuer, 2009, 2010; Schwartz et al., 2003) and are almost universally ascribed negative characteristics (Allison et al., 1991; Allon, 1982; Weiner, 1995). It is well documented that the direct experience of weight-related stigma is associated with a myriad of poor psychosocial outcomes (Puhl and Brownell, 2001; Puhl and Heuer, 2009, 2010). There is evidence suggesting that the effects of weight-based stigma become more severe when they are internalized (referred to hereafter as “weight self-stigma”), particularly when combined with poor coping skills (Friedman et al., 2005; Lillis et al., 2011; Puhl and Brownell, 2006), making it a potentially important target for study and intervention.
Research on weight self-stigma has been limited in part by lack of definitional clarity. Weight self-stigma refers to both the self-devaluation and the fear of enacted stigma that result from one’s identification with a stigmatized group (Lillis et al., 2010; Link and Phelan, 2001). Specifically, self-devaluation is the internalization of negative beliefs about oneself and association with negative characteristics due to the stigmatization. Fear of enacted stigma is the fear that others will have unfavorable attitudes and engage in ridicule, bias, or discrimination toward the individual. In short, self-stigma is when individuals come to associate themselves with negative characteristics and fear that others will too.
Consistent with the homeostatic theory of obesity, self-stigma could lead to poorer eating habits (e.g. more consumption of high calorie, high-density comfort foods) by contributing to higher levels of discontent and negative affect (Marks, 2015, 2016). Research in controlled settings has supported this notion (e.g. Schvey et al., 2011); however, there is currently little research on the impact of weight self-stigma on weight control efforts. In addition, the existing literature has focused exclusively on the self-devaluation component of weight self-stigma, and methodological aspects of existing research such as the reliance on self-report and cross-sectional designs limit interpretability.
Carels et al. (2009) found that the attribution of fewer positive and greater negative personality traits to people with obesity was associated with higher attrition from a weight loss program. However, it was only the attribution of fewer positive traits to individuals with obesity people that predicted poorer weight loss in the context of a self-help behavioral weight loss program (N = 46). Although endorsement of stigmatizing attitudes relates to self-devaluation, the study did not directly assess any aspect of weight self-stigma, such as applying these attitudes toward oneself (Carels et al., 2009).
A recent cross-sectional study (N = 549) examined the impact of weight bias internalization on maintaining a weight loss. Weight bias internalization, which could be a good representation of the self-devaluation component of weight self-stigma, was associated with reduced odds for maintaining a weight loss (Puhl et al., 2017). Although this provides some evidence for the impact of weight self-stigma on weight control, the study was limited by a cross-sectional design and the use of self-report methods that assessed weight loss and maintenance retrospectively.
This study examines both aspects of weight self-stigma (self-devaluation and fear of enacted stigma) in the context of a 3-month online weight loss program. The first aim was to test for associations between participant characteristics at baseline and weight self-stigma. The second aim was to examine the impact of self-stigma on weight loss. It was hypothesized that greater self-devaluation and fear of enacted stigma at baseline would be associated with poorer weight loss at 3 months and poorer treatment engagement. This study is the first to examine the impact of weight self-stigma prospectively in relation to weight change.
Methods
Design
This is a non-randomized weight loss intervention study that utilized baseline variables to predict 3-month weight change. The study was part of a larger trial in which individuals with overweight or obesity were initially invited to complete a 3-month online weight loss intervention and then were randomized to one of the three conditions to facilitate maintenance, which is still ongoing. Data analyzed for this report come from the initial, non-randomized 3-month intervention. All study activities were conducted at the Weight Control and Diabetes Research Center in Rhode Island, United States. The Miriam Hospital Institutional Review Board (IRB) approved all study procedures.
Participants
Inclusion criteria
Included participants were 18–70 years of age and had a body mass index (BMI) between 27.5 and 45 kg/m2.
Exclusion criteria
Participants were excluded for current participation in another weight loss program; current pregnancy or plans to become pregnant during the study period; reported heart condition, chest pain or inability to engage in walking exercise; report of conditions that would render them unlikely to follow the protocol, including terminal illness, plans to relocate, a history of substance abuse, or a recent psychiatric hospitalization.
Recruitment and screening
Participants were self-referred via newspaper ads and direct mailings and completed a phone screen that assessed BMI and basic health status information. Potential participants then attended an in-person group orientation session where detailed information about the study was provided and informed consent was obtained.
Intervention
The Internet-based weight loss intervention was previously developed and shown to be effective for physician referred individuals with overweight and obesity (mean weight loss 5.8% at the end of the 3-month program (Thomas et al., 2015). It included two main components: (1) training in the behavioral weight control strategies that have been shown to be effective in past research studies accomplished via weekly interactive multi-media lessons that participants access via their computer, and (2) automated, computer-generated feedback provided weekly to participants in response to their self-monitoring records to increase accountability. Each week a new lesson was made available to participants. Lessons were audio/video presentations by weight control experts on topics such as energy balance, exercise goals, unhealthy eating cues, problem-solving, restaurant eating, social influences, and motivation. Target calorie goals ranged from 1200 to 1500 kcal/day and 33–42 grams of fat/day (25% calories from fat) based on starting weight. Participants were encouraged to gradually increase their physical activity to at least 200 minutes per week by the end of the program. Participants were asked to track their daily calorie intake, exercise minutes and weight via the online system (an interactive website which received data reports from participants). Paper materials were provided for self-monitoring; however, participants were encouraged to use online tools for self-monitoring if it was preferred.
Automated feedback was provided based on reported weekly calorie, physical activity and weight data. The message was based on the participant’s self-monitoring data and baseline characteristics (e.g. weight, gender, health problems), and compared the participants’ self-reported weight loss, diet, and activity to the goals that had been prescribed by the program. Each message was crafted with an opening statement that commented on weight loss for the week and overall weight loss to date. Subsequent comments differed depending on whether or not the person was achieving the weight loss goal. The tailored message then provided praise or feedback on caloric intake and activity. For example, if calories were above recommended, suggestions were provided for reducing intake, including the use of prepackaged frozen meals or following a more structured meal plan.
Measures
All measures were collected in-person at baseline and 3 months.
Anthropometric
Weight was measured to the nearest 0.1 kg using a digital scale and height was measured to the nearest millimeter with a stadiometer, using standardized procedures, and used to calculate BMI (kg/m2).
Weight Self-Stigma Questionnaire
The Weight Self-Stigma Questionnaire (WSSQ) is a 12-item measure of weight self-stigma using a 5-point, Likert-type rating that ranges from “completely disagree” to “completely agree” (Lillis et al., 2010). It contains two subscales: Self-Devaluation and Fear of Enacted Stigma. The Self-Devaluation subscale contains six items that pertain to ascribing personal blame and endorsing negative characteristics because of one’s weight. For example, one question reads, “I became overweight because I am a weak person.” The Fear of Enacted Stigma subscale contains six items that assess the degree to which someone is concerned with the possibility of being the target of ridicule, bias, or discrimination because of one’s weight. For example, one question reads, “Others will think I lack self-control because of my weight problems.” Total weight self-stigma, and its subcomponents, have demonstrated adequate internal consistency and construct validity (Lillis et al., 2010).
Eating Inventory
The Eating Inventory is a widely used measure of eating behavior that includes three subscales, restraint, hunger, and disinhibition (higher scores indicate greater endorsement of each; Stunkard and Messick, 1985). Disinhibition represents the tendency to eat in an unrestrained manner in the presence of external (seeing food) or internal (feeling sad) cues to eat, while the restraint scale represents the degree to which participants tend to restrict their eating purposefully. The disinhibition and restraint subscales were used as measures of eating pathology in the current study, as both represent behavioral aspects of problems with eating.
Patient Reported Outcomes Measurement Information System Initiative Short Forms
Depression, anxiety, quality of life, and satisfaction with relationships were assessed using standardized measures from the National Institutes of Health (NIH) Patient Reported Outcomes Measurement Information System (PROMIS) initiative (DeWalt et al., 2007). The Depression-Short Form measures depression using 4 self-report, Likert scale items. Higher scores indicate more depression. The Anxiety-Short Form measures anxiety using 4 self-report, Likert scale items. Higher scores indicate more anxiety. The PROMIS Global form is a 10-item self-report measure that assesses physical and mental quality of life. Higher scores indicate better quality of life. The Satisfaction with Relationships-Short Form measures relationship satisfaction using 4 self-report Likert scale items. Higher scores indicate greater satisfaction with relationships. PROMIS measures are well established with population norms and good validity (DeWalt et al., 2007).
Engagement
Treatment engagement was measured by the number of weeks the participant logged into the system and the number of lessons viewed (both out of 12).
Statistical analysis
All analyses were completed using IBM SPSS Statistics software version 24 for PC in 2017. First, baseline means and standard deviations (SDs) were calculated for all study variables for descriptive purposes, including separate means for males and females for weight self-stigma variables. Next, self-devaluation and fear of enacted stigma were correlated with all other study variables at baseline.
To examine the impact of self-stigma on weight loss and treatment engagement, hierarchical regression models were conducted with two steps. In step 1, self-devaluation and fear of enacted stigma were entered as predictors along with demographic variables. In step 2, eating behaviors, anxiety, and depression were entered as covariates. The dependent variables were 3-month percent weight loss, number of weeks logged in, and number of lessons viewed, with each outcome analyzed in a separate model. Hierarchical regression was chosen to examine the effects of self-stigma variables with and without covariates, as it could be argued both that (1) eating pathology and psychological symptoms are variables through which stigma could affect weight, and thus including them all in the model could underestimate the impact of self-stigma, and (2) self-stigma might just be representing generalized pathology, and thus covariates are required to show an independent effect for self-stigma.
Given that this is the first prospective study of the impact of subcomponents of weight self-stigma on weight loss, participants were also categorized as “High” (≥1 SD above norms) or “Low” (remaining participants) on baseline self-devaluation and fear of enacted stigma for descriptive purposes, using the overweight/obese, non-treatment seeking norms for the WSSQ (Lillis et al., 2010). Mean comparisons (one-way analysis of variance (ANOVA) and chi-square) were performed on the High versus Low group for 3-month percent weight loss, percent achieving 5 percent weight loss, number of weeks logged in, and number of lessons viewed. This study is part of a larger randomized trial which was designed to achieve 80 percent power to detect a 2.5 kg (between two experimental conditions) and a 4.0 kg (between primary experimental and control condition) weight change difference at 24 months among three conditions with 190 participants.
Results
A total of 188 participants entered the study and began the Internet-based weight loss intervention. The sample was 76 percent female, 88 percent White, and had an average age of 55 ± 11 years. Table 1 presents the means and SDs for study variables at baseline. As shown, women had higher levels of fear of baseline disinhibition, restraint, anxiety, total self-stigma, and fear of enacted stigma.
Baseline means, standard deviations, and comparisons by gender.
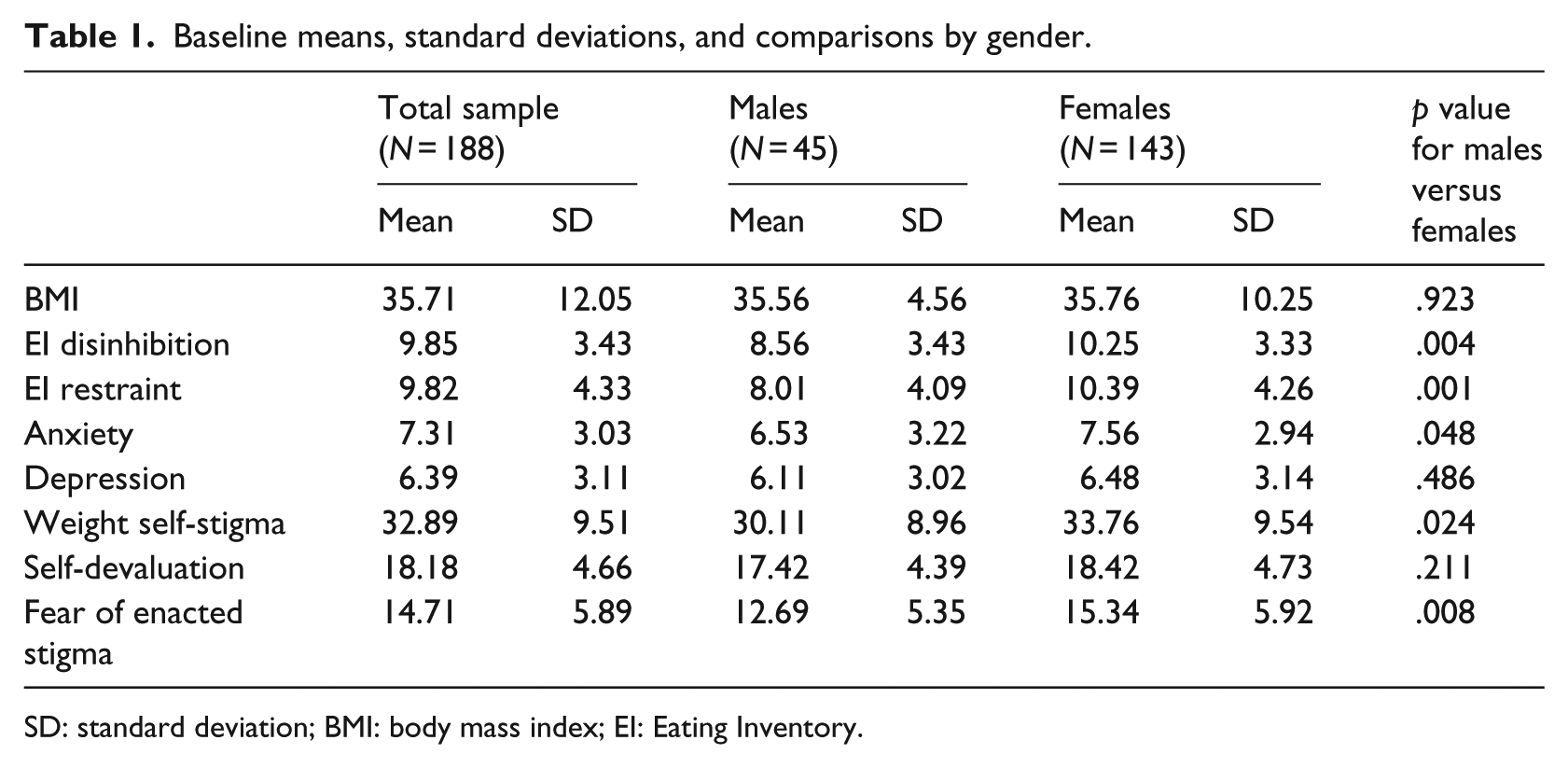
SD: standard deviation; BMI: body mass index; EI: Eating Inventory.
We also examined the proportion of this sample who were ≥1 SD above the norms for non-treatment seeking individuals (Lillis et al., 2010). Approximately, 33 percent (n = 63) of the participants reported high self-devaluation while 39 percent (n = 74) reported high fear of enacted stigma. There was a significant difference based on gender, with a higher percentage of females versus males reporting high fear of enacted stigma (44% vs 24%, χ2 = 5.52, p = .019), but no significant difference between men and women on self-devaluation (36% vs 27%, χ2 = 1.24, p = .265).
Weight self-stigma correlations
The two aspects of self-stigma—Self-Devaluation and Fear of Enacted Stigma—were strongly correlated (r = .61) with each other. Table 2 shows the correlations for self-devaluation and fear of enacted stigma with other baseline variables. Both self-devaluation and fear of enacted stigma were significantly associated with more psychological symptoms and eating pathology. These correlations identified multiple possible confounding factors to control for in subsequent analyses.
Correlations between baseline characteristics and weight self-stigma subcomponents.
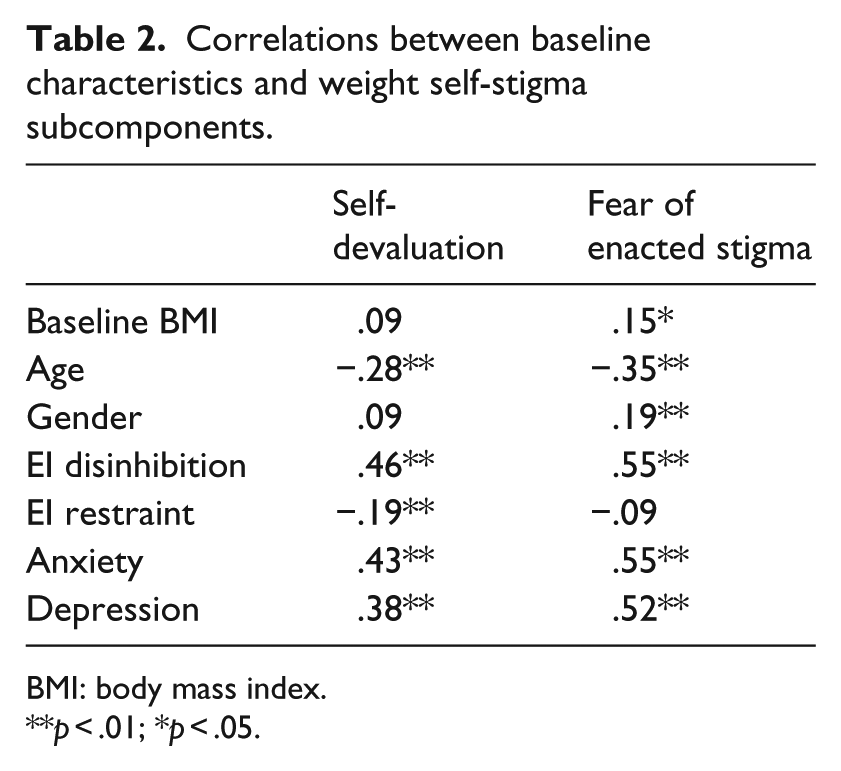
BMI: body mass index.
p < .01; *p < .05.
Weight loss
Table 3 shows the results of the hierarchical regression analysis. Higher fear of enacted stigma was associated with poorer weight loss over 3 months when controlling for baseline demographic variables and BMI and remained significantly associated when eating pathology (disinhibition and restraint) and psychological symptoms (anxiety and depression) were added as covariates. Self-devaluation was not significantly associated with weight change.
Hierarchical regression results using self-stigma and covariates to predict 3-month percent weight change.
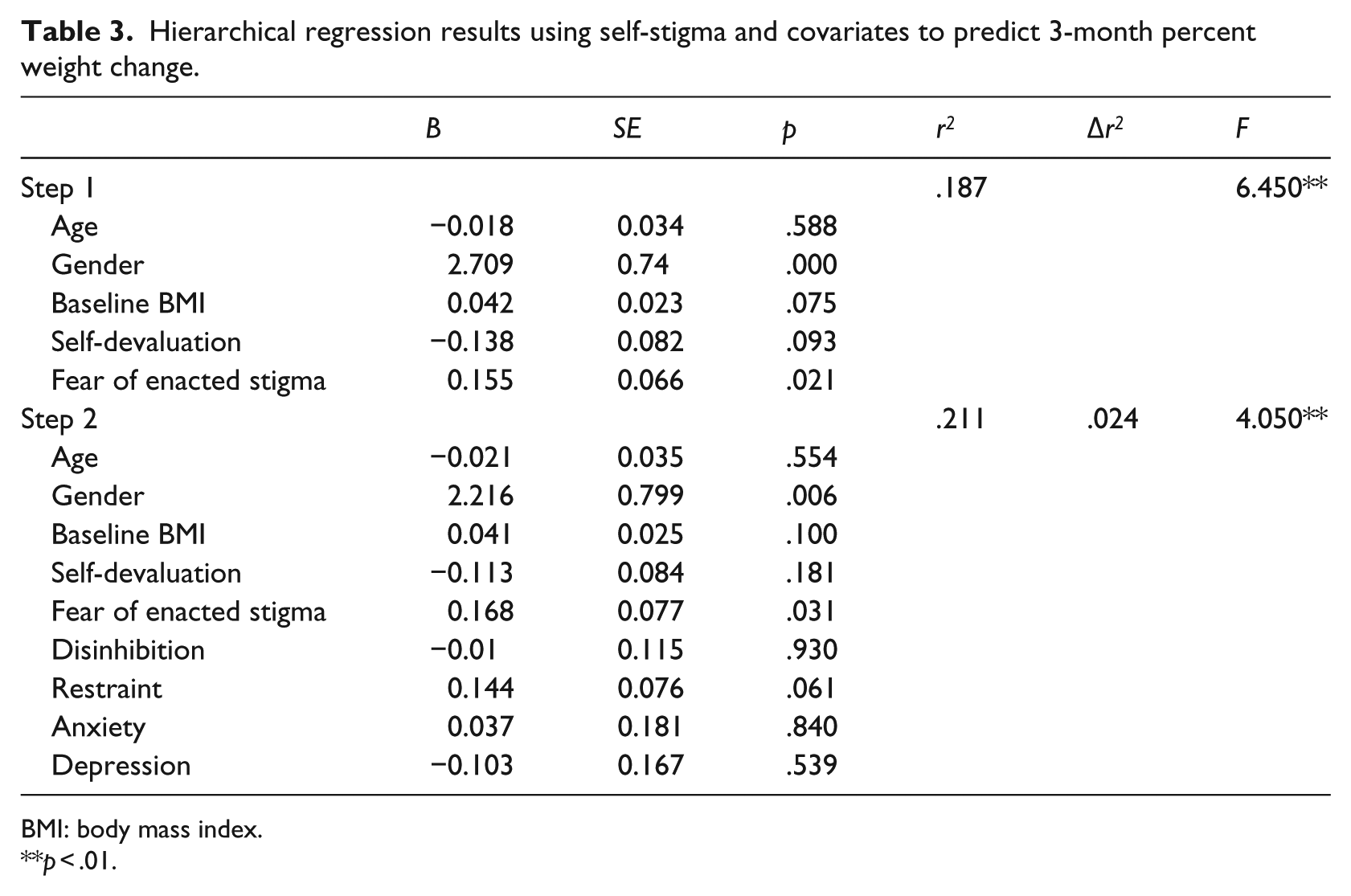
BMI: body mass index.
p < .01.
When examined categorically, participants who reported high fear of enacted stigma (i.e. ≥1 SD above norms) lost significantly less weight when compared to participants reporting less fear of enacted stigma (−5.67 ± 3.8 vs −7.80 ± 3.8; F = 10.79, p = .001, d = .56; see Figure 1). Participants who reported high fear of enacted stigma were also less likely to reach the 5 percent weight loss goal (57% vs 79%, χ2 = 7.86, p = .005). There were no significant differences in mean weight change for participants categorized as reporting high self-devaluation versus low (−6.70 ± 3.9 vs −7.11 ± 3.9; F = 0.33, p = .568, d = .11).
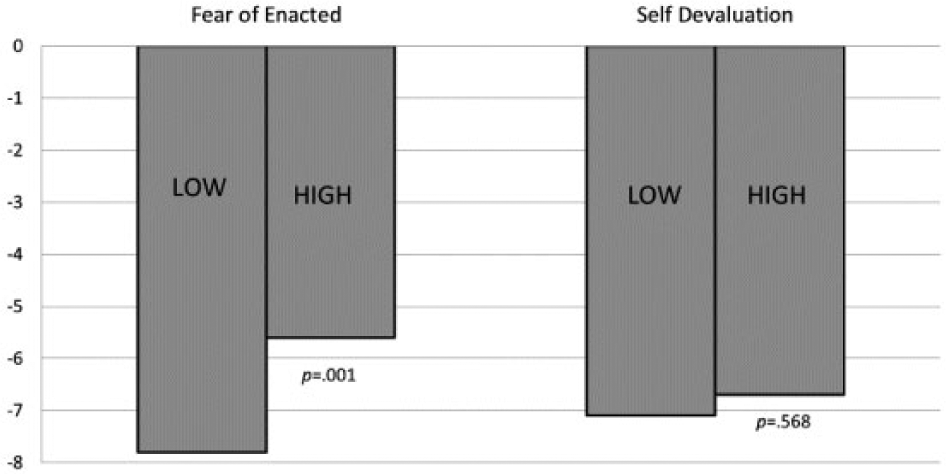
Three-month percent weight loss by self-stigma category.
Program engagement
Hierarchical regression analyses showed that weight self-stigma subcomponents were not associated with total weeks logged in (Step 1, self-devaluation p = .383; fear of enacted p = .542) and total lessons viewed (Step 1, self-devaluation p = .528; fear of enacted p = .870).
When examined categorically, participants who reported high self-devaluation viewed fewer lessons when compared to participants reporting less self-devaluation (7.31 ± 3.9 vs 8.50 ± 3.7; F = 3.99, p = .047, d = .32). There were no significant differences for participants reporting high versus low fear of enacted stigma on average number of lessons watched (7.49 ± 3.7 vs 8.49 ± 3.8; F = 3.14, p = .078, d = .27).
There were no significant differences in mean number of weeks logged in for participants reporting high self-devaluation versus low (9.62 ± 3.4 vs 10.09 ± 3.3; F = 0.85, p = .357, d = .14) or high fear of enacted stigma versus low (9.57 ± 3.4 vs 10.18 ± 3.3; F = 1.49, p = .114, d = .18).
Discussion
This study was the first to examine the impact of weight self-stigma on weight loss prospectively, and the first to examine the two aspects of weight self-stigma, self-devaluation and fear of enacted stigma, in the context of a weight loss intervention. Consistent with hypotheses, fear of enacted stigma was associated with less weight loss with a medium effect size. Contrary to hypotheses, self-devaluation was not associated with less weight loss.
Although the negative psychosocial impact of weight stigma is well documented, less is known about its impact on efforts to control weight. To date, research on weight self-stigma and weight control has focused on the impact of self-devaluation (often referred to as weight bias internalization or internalized stigma). Results from this study suggest that it is important to distinguish between the two aspects of self-stigma, and that fear of enacted stigma is an important dimension that warrants inclusion in future studies.
Gender also played a role in weight loss. Being female and having high fear of enacted stigma were both independently associated with poorer weight losses. Unfortunately, the low number of males in the sample precluded a categorical comparison of high/low stigma in males versus females. Related results showed that men reported similar levels of self-devaluation, but lower levels of fear of enacted stigma. To date, there has been little examination of gender differences in relation to weight self-stigma, and many studies on the topic have utilized exclusively female cohorts. This study suggests that interaction between gender and stigma and their combined impact on weight control warrants future attention.
It is not clear from this study why fear of enacted stigma, but not self-devaluation, had an impact on weight loss. There was some evidence from the categorical analyses that fear of enacted stigma might be associated with poorer treatment engagement (fewer lessons viewed); however, self-devaluation showed a similar, slightly stronger effect. Fear of enacted stigma is the experience of wondering and worrying about the degree to which others will reject, hurt, and discriminate against you, and could reflect a powerful demotivating process on behaviors related to controlling weight. Future research will be needed to clarify how this relationship manifests, for example, by isolation, increased binge eating, or via negative psychological symptoms, among other possible explanations.
Both self-devaluation and fear of enacted stigma were strongly associated with symptoms of anxiety and depression, suggesting more impaired psychosocial functioning. This finding is consistent with the vast literature documenting the deleterious effects of stigma. Both components of weight self-stigma were also associated with disinhibited eating. This finding is consistent with recent literature suggesting that exposure to stigmatizing situations resulted in greater caloric consumption (Schvey et al., 2011).
This study has many strengths. It is the first to examine the impact of weight self-stigma on weight loss prospectively in the context of a weight loss intervention. In addition, it is the first to examine two aspects of weight self-stigma, self-devaluation and fear of enacted stigma. The study utilized objective measurement of weight and blind assessors, which is an improvement on previous research that assessed weight via self-report retrospectively. However, this study is limited by the use of self-report measures for all other variables, lack of diversity in the sample (both in gender and race/ethnicity), and the absence of measuring experienced stigma.
If supported by future research, the results of this study could indicate a new treatment target for weight loss interventions. Coping with the chronic concerns about mistreatment from others because of one’s body shape may be an important aspect of a comprehensive weight loss intervention that is not currently addressed in standard behavioral interventions. In addition, addressing self-stigma might be important for other aspects of healthy life change, as a recent study has shown internalized stigma attenuates response to a physical activity intervention (Mesinger and Meadows, 2017). While efforts are needed to produce the cultural change necessary to reduced experienced stigma due to body shape, self-stigma may be a target more amenable to immediate change (and potentially effective in an intervention), as it can be addressed by the individual and a treatment provider directly and does not rely on changing the behavior of others.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases (K23DK097143).