
Abstract
Risk for suicidality (current or past suicidal ideation or attempt) increases after bariatric surgery; however, there is a paucity of research investigating suicidality predictors in this population. This study involved a retrospective chart review of individuals seeking psychological clearance for bariatric surgery. In total, 32 participants (15.8%) were classified as reporting suicidality. These participants endorsed greater depressive symptomatology and hopelessness, and hopelessness and mood disorder diagnosis each uniquely predicted whether or not a patient was classified as reporting suicidality. The findings within suggest that increased attention to the relationship among these variables may improve methods for identification of high-risk patients. Implications for clinical practiced are discussed.
Introduction
In 2011–2012, 34.9 percent of adults in the United States met criteria for obesity (body mass index (BMI) ⩾ 35) and 6.4 percent met criteria for extreme obesity (BMI ⩾ 40; Ogden et al., 2014). While rates of overall obesity have not shown substantial increases in recent years, the prevalence of the most severe form of obesity, extreme obesity, has continued to increase (Sturm, 2007). Extreme obesity is a risk factor for a number of severe medical problems, including heart disease and cancer, and is associated with premature mortality (Calle et al., 1999; Calle and Kaaks, 2004; Hubert et al., 1983; Mokdad et al., 2004). Furthermore, it is also associated with elevated rates of psychological problems, including mood and anxiety disorders (Kalarchian et al., 2007).
As a result of the increasing rates of extreme obesity in the United States, the choice of bariatric surgery as a weight loss method is likely to increase (Gilbert and Wolfe, 2012), with research indicating that it is the most cost-effective treatment for long-term weight loss (Martin et al., 1995). However, despite recent research demonstrating that suicidality (including suicidal ideation and attempts) increases following bariatric surgery (Adams et al., 2007; Peterhänsel et al., 2013; Tindle et al., 2010), there is a paucity of research on what factors are related to increased risk of suicidality in adults with extreme obesity. In fact, established risk factors for suicide (e.g. firearm ownership and alcohol use) do not sufficiently explain observed associations between weight and suicide (Mukamal and Miller, 2009). Consequently, empirical investigations aimed at systematically evaluating factors predicting suicidality in individuals with extreme obesity are sorely needed and have been cited as a research priority (Mukamal et al., 2007). Thus, the aim of this study was to address this issue by investigating psychological factors that may predict suicidality in a bariatric population.
A positive relationship between increased BMI and suicidality has been well established by recent research (Dutton et al., 2013; Wagner et al., 2013). For example, a population-based study examining the prevalence of suicidality in different BMI categories found that among participants with a BMI over 40, the prevalence rate was 33 percent for women and 13 percent for men (Wagner et al., 2013). Furthermore, adults with obesity have a 1.3 to 1.5 times increased risk of suicidal ideation and attempts when compared to healthy weight individuals (e.g. Mather et al., 2009), and adults with extreme obesity have approximately a 2.6 to 3.9 times increased risk of suicidal ideation compared to family members and community members (Dong et al., 2006).
Past research has also consistently demonstrated a strong relationship between obesity and depressive symptoms (De Wit et al., 2009; Roberts et al., 2003), and individuals with depressive symptoms present an elevated risk of suicidality (Ahrens et al., 2000). Additionally, 60 percent of individuals who die by suicide suffer from a mood disorder, such as major depressive disorder, dysthymic disorder, or bipolar disorder, at the time of their death (Sher et al., 2001). Although history of a mood disorder alone is not a reliable predictor of suicidality, patients experiencing depressive symptoms often display feelings of hopelessness, and the depression literature suggests hopelessness may be a particularly important risk factor for suicidality (e.g. Beck et al., 1975). In spite of these findings, hopelessness as a risk factor for suicidality has not been examined independently from a diagnosis of a depressive disorder. Thus, it is unclear whether hopelessness is simply an important component of a clinical syndrome, or whether it represents a unique construct that practitioners should evaluate separately from Diagnostic and Statistical Manual of Mental Disorders (DSM) symptoms of depression. Furthermore, as hopelessness is not an explicit symptom of depressive disorders, it often does not appear in common questionnaires used to assess depressive symptomatology (e.g. Beck Depression Inventory Second Edition (BDI-II; Beck et al., 1996) or the Quick Inventory of Depressive Symptomatology (QIDS-SR; Rush et al., 2003)). Thus, research evaluating its importance in the prediction of suicidality relative to the importance of a depressive disorder diagnosis is crucial for identification of patients who may be at risk.
Hence, based on the existing literature, we hypothesized that individuals seeking bariatric surgery who presented with suicidality would (a) endorse higher (current) levels of depressive symptomatology and hopelessness, and (b) be more likely to meet criteria for a current mood disorder diagnosis. Finally, we predicted that (c) depressive symptomatology, feelings of hopelessness, and current mood disorder diagnosis would all significantly and uniquely contribute to the prediction of suicidality.
Method
Participants
Data were abstracted from the charts of 280 patients presenting for a pre-bariatric surgery psychological evaluation. Only data from 203 individuals (36.2% men, 63.8% women) who completed all questions on the Millon Behavioral Medicine Diagnostic (MBMD) and to whom the Mini International Neuropsychiatric Interview (MINI) was administered were included in this study. Patients who were excluded from this study did not differ significantly from patients who were included on any baseline demographic factors (all p values > .14). Data were also examined for outliers before analysis.
Participants ranged in age from 18 to 69 years old (M = 41.92, standard deviation (SD) = 12.44). The majority of participants completed some coursework toward a college degree (36.3%), with 23.9 percent reporting a high school degree, 14.9 percent a college degree, and 19.0 percent reporting achievement of a graduate degree. Participants were 80.6 percent Caucasian, 11.2 percent Hispanic, 5.6 percent African American, and 2.5 percent other. Participants’ BMIs ranged from 33.06 to 72.80 (M = 45.85, SD = 7.15), with 16 percent of participants falling into the obese range (BMI ⩾ 30) and 82.9 percent into the extremely obese range (BMI ⩾ 40).
Procedure
We conducted a retrospective review of clinical records of bariatric surgery candidates who presented for evaluations from March 2010 to November 2012. The Human Subjects Institutional Review Board approved a waiver of consent for the use of these data, and all of the data used herein were abstracted from the charts of patients who underwent a comprehensive psychological evaluation designed to evaluate readiness for bariatric surgery. The evaluation included a battery of self-report questionnaires and the Psychological Interview for Bariatric Surgery (PIBS), a 75-minute face-to-face semi-structured clinical interview.
Assessment variables
Depressive symptomatology
Depressive symptomatology was measured by the Depression subscale of the MBMD (Millon et al., 2001), a 165-item questionnaire designed to evaluate patient characteristics associated with adjustment to treatment and treatment compliance. Items are rated as true or false, and responses were scored according to bariatric norms. This measure is known to have good validity and reliability (Millon et al., 2001). The depression subscale focuses on the mood state of patients, including loss of appetite, anhedonia, feelings of guilt, and social withdrawal. Greater scores suggest greater symptoms of depressive symptomatology, and scores 75 and above are considered to be within the clinical range.
Hopelessness
Hopelessness was assessed by the Dejection subscale of the MBMD. Higher scores on this subscale suggest patients are prone to disheartenment and unable to experience pleasure or joy, and higher scorers tend to have a hopeless orientation. Scores 75 and above are considered to be within the clinical range. This subscale will be referred to as the hopelessness subscale throughout the remainder of this article to decrease confusion surrounding terminology.
Suicidality
Suicidality was measured by the Suicidality Index included in the Psychological Interview for Bariatric Surgery (PIBS-SI). The PIBS-SI is a composite measure of three dichotomous (yes/no) questions concerning: (a) current suicidal ideation, (b) past suicidal ideations, and/or (c) past suicide attempts. Each of these items was scored as present (1) or absent (0), and the scores from all three of these items were summed to form a total suicidality score. Patients endorsing one or more of the three PIBS-SI items were classified as reporting “suicidality.”
Mood disorder diagnosis
Current mood disorders were evaluated with the MINI (Sheehan et al., 1998), a structured interview designed to assess Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnoses. Patients were classified as having a current mood disorder if they endorsed items on this measure consistent with DSM-IV criteria for one or more of the following: major depressive disorder, depressive disorder not otherwise specified, dysthymic disorder, or bipolar disorder. The MINI is considered to have good reliability and validity (Sheehan et al., 1998).
Results
Of the 203 participants, 32 (15.8%) endorsed one or more of the three SI items and were classified as meeting criteria for suicidality. Twenty-two participants (10.8%) were classified as having a current mood disorder, and one participant (.5%) met criteria for two current mood disorders. The breakdown of the different mood disorder diagnoses was as follows: major depressive disorder, 4.4 % depressivedisorder, 3.0 % dysthymic disorder, 2.5 % and bipolar disorder, 1.5 percent. Table 1 presents the percentage of participants above the clinical cut-offs on the Depression and Hopelessness subscales of the MBMD. Participants who endorsed suicidality were significantly more likely to score above the clinical cut-off for both the Depression and the Hopelessness subscales (Table 2). Table 3 shows the correlations among the major study variables. As predicted, endorsing suicidality was significantly and positively correlated with depression and hopelessness (p = .008 and .001, respectively). Participants reporting suicidality also endorsed higher (current) levels of depressive symptomatology and hopelessness than those without suicidality (t (39.31) = −2.34, p = .02, t (39.81) = −3.11, p = .003), respectively. Finally, participants reporting suicidality were more likely to meet criteria for a current mood disorder diagnosis than participants who did not report suicidality, χ2 (1, N = 203) = 13.97, p < .001.
Percentage of participants above clinical cut-offs on the MBMD subscales.

MBMD: Millon Behavioral Medicine Diagnostic.
Crosstabulation of endorsing suicidality and clinical cut-offs on the MBMD subscales.
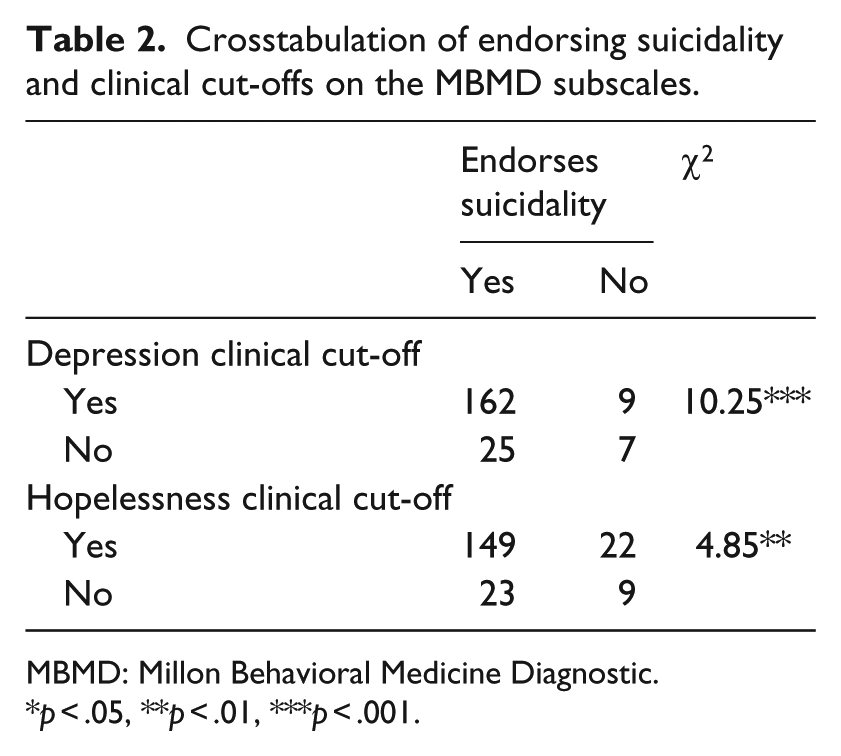
MBMD: Millon Behavioral Medicine Diagnostic.
p < .05, **p < .01, ***p < .001.
Descriptive characteristics and correlations among major study variables.

SD: standard deviation.
p < .05, **p < .01, ***p < .001.
To determine the unique predictive utility of depressive symptomatology, hopelessness, and current mood disorder for suicidality, we conducted a stepwise linear regression. The initial model with depression predicting suicidality was significant, F (1, 202) = 8.44, p = .004. Adding hopelessness into the model led to a significant increase in explained variance, Fchange = 5.60, p = .02. While the overall model remained significant with the addition of hopelessness, F (2, 202) = 7.11, p = .001 (beta = .22, p = .02), depressive symptomatology was no longer a significant unique predictor of suicidality (beta = .05, p =.63). Finally, the addition of mood disorder diagnosis into the model also led to a significant increase in explained variance, Fchange (1, 199) = 4.44, p = 04. The overall model with these three variables remained significant, F (3, 202) = 6.31, p < .001, as did the unique contributions of hopelessness (beta = .20, p = .04) and mood disorder diagnosis (beta = .15, p = .04); the unique contribution of depressive symptomatology remained non-significant (beta = .04, p = .69).
Finally, we examined the likelihood of endorsing suicidality based on the number of risk factors (diagnosis, depressive symptoms, hopelessness) reported. Primarily, a chi-square test for independence indicated that rates of suicidality differed significantly based on the number of risk factors endorsed, χ2 (3, N = 203) = 18.07, p < .001. As compared to not endorsing any risk factors, endorsing only one of the risk factors was not associated with a significant increase in likelihood of suicidality. However, endorsing at least two risk factors as compared to not endorsing any led to a significant increase in the likelihood of suicidality, odds ratio (OR) = 7.37, Z = 3.76, p < .001. Additionally, endorsing at least two risk factors as compared to endorsing only one risk factor also led to a significant increase in the likelihood of suicidality, OR = 5.5, Z = 2.37, p = .02.
Discussion
This study provided evidence that bariatric patients who are at risk for suicidality report increased levels of depressive symptomatology and hopelessness and may also be more likely to meet criteria for a current mood disorder than bariatric patients who are not at risk for suicidality. The strong relationships among these variables suggest that individuals with both current symptoms of depression and hopelessness and a current mood disorder may be at an increased risk for suicidal ideation or attempts following surgery.
Moreover, our regression analysis suggests that current elevated levels of depression significantly predict whether or not a patient was categorized as having high level of suicidality. In addition, both hopelessness and current mood disorder each uniquely predict suicidality above and beyond the predictive utility of depressive symptoms. Thus, while all of these psychological factors are interrelated (and are likely to be etiologically associated), it is also important to remember that they may contribute independently to the identification of patients who are at risk for suicidality post-surgery. Finally, information concerning symptoms of hopelessness and a diagnosis of mood disorder before pre-surgery are particularly important as they represent strong risk factors for negative outcomes post-surgery (De Zwaan et al., 2011; Legenbauer et al., 2011). This study underscores the importance of including a thorough assessment of these factors in pre-surgery psychological evaluations.
Limitations
While this study is ecologically valid and provides direct clinical implications for the assessment of risk factors in pre-bariatric surgery patients, it does have some limitations. First, only a relatively small number (15.8%) of patients report risk for suicidality and small numbers of participants always limit the variability present in analyses. While our prevalence rate of 15.8 percent is slightly higher than those of findings of previous studies, evaluating suicidality in a bariatric surgery seeking population (5.5%–11%; Chen et al., 2012; Sansone et al., 2008; Windover et al., 2010), these aforementioned estimates did not include individuals reporting suicidal ideation and only included individuals with a history of a suicide attempt. As such, we assume our estimate is a fairly accurate representation of the population individuals seeking surgery who have a past or current history of suicide attempt or suicidal ideation. Moreover, the risk of completing suicide after long-term follow-up from bariatric surgery is also a relatively small phenomenon. In fact, a recent systematic review of completed suicides following bariatric surgery estimates a suicide rate of 4.1 per 10,000 persons compared with 1.0/10,000 in the general population (Peterhänsel et al., 2013), suggesting that although the suicide rate is approximately four times higher in the population of individuals who have undergone surgery, the number of completed suicides is small. Notwithstanding, we believe this trend merits more comprehensive investigation.
Furthermore, the method used to classify a participant as being in the risk for suicidality group (namely, the PIBS-SI) may also be limited. It relies on a single method for assessing this complex problem, thereby limiting construct validity, and it does not have any reliability or validity data. Additionally, this study relied upon a cross-sectional design, which did not allow for determination of causality among study variables. Thus, future research is needed to further assess the causal relationships among hopelessness, symptoms of mood disorders, and suicidality in this patient population. Finally, while suicidality was only evaluated during the face-to-face interview, wherein patients may underreport thoughts of suicide out of fear they will not be cleared for surgery, this limitation is consistent with other studies on this population as research suggests that individuals presenting for bariatric surgery are likely to underreport symptoms of psychopathology during their pre-surgical psychological evaluation (Ambwani et al., 2013; Fabricatore et al., 2007).
Conclusion
In light of research suggesting a heightened risk of suicide after bariatric surgery, increased knowledge of the relationships among current depressive symptomatology, feelings of hopelessness, mood disorder diagnosis, and suicidality in this population may help improve treatment for patients seeking bariatric surgery and assist in the identification of high-risk patients. In particular, patients with both depressive symptoms and heightened levels of hopelessness may benefit from increased monitoring post-surgery.
Based on these data, we suggest that patients with a current mood disorder diagnosis who endorse both current elevated levels of depression and hopelessness be routinely assessed for depression and suicidality pre- and post-surgery using validated assessment tools (e.g. BDI-II, Beck et al., 1996; Columbia Suicide Severity Rating Scale, Posner et al., 2011). Additionally, all members of the patient’s healthcare team (surgeons, dieticians, nurses, primary care physicians, etc.) and the patient himself/herself should be aware of the increased risk. Finally, while the aforementioned assessment tools are validated in community samples and with individuals with depression, future studies are required to evaluate and produce an effective measure for determining suicide lethality in a bariatric population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.