
Abstract
Aim of this study was to investigate relationship between preoperative psychological factors and % total weight loss after gastric bypass. 76 adult patients scheduled for bariatric surgery were preoperatively asked to complete anxiety and depression Hamilton scales and Toronto Alexithymia Scale. At 3- and 6-month follow-up, body weight was assessed. At 6-month follow-up, alexithymic patients showed a poorer % total weight loss compared with non-alexithymic patients (p = .017), and moderately depressed patients showed a lower % total weight loss compared with non-depressed patients (p = .011). Focused pre- and postoperative psychological support could be useful in bariatric patients in order to improve surgical outcome.
Introduction
Bariatric surgery is currently the most effective treatment for morbid obesity (Courcoulas et al., 2013). However, recent papers highlight the need to improve methods for pre-surgical identification of patients at risk of both psychological and medical poor outcomes (Adamowicz et al., 2016; Janse Van Vuuren et al., 2018; Rouleau et al., 2016). Despite an improvement of quality of life (QoL) after bariatric surgery has been reported (Shen et al., 2015), the reasons why some patients experience suboptimal weight loss after bariatric surgery are not well understood, but probably involve both behavioral and physiologic processes (Won et al., 2014).
It has been stated that successful weight loss after bariatric surgery depends on the degree to which patients adhere to medical and dietary recommendations (Gorin and Raftopoulos, 2009; Robinson et al., 2014; Sarwer et al., 2012). However, most of the studies have investigated the influence of preoperative eating disorder or other common psychiatric disorders on weight loss after bariatric surgery (Gorin and Raftopoulos, 2009; Wimmelmann et al., 2014); whereas, the role of specific psychological characteristics associated with obesity, such as alexithymia (Noli et al., 2010; Pinna et al., 2011), has not been taken into account. Moreover, a recent review of literature concluded that relevant psychological predictors of weight loss after bariatric surgery have not been well identified (Wimmelmann et al., 2014), despite they could explain the wide difference in surgical outcome. Alexithymia, beside other more common psychological characteristics such as anxiety and depression, has been found able to affect adherence to the medical and dietary recommendations in other clinical conditions (Aceto et al., 2016; Calia et al., 2011a, 2011b, 2011c, 2015a, 2015b, 2015c; Lai et al., 2016). Therefore, the role of alexithymia could be crucial in affecting weight loss in bariatric patients.
Aim of this study was to investigate the influence of preoperative alexithymia, depression, and anxiety on postoperative % total weight loss (%TWL) at 3 and 6 months after laparoscopic Roux-en-Y gastric bypass (LRYGB).
The change in QoL after surgery was also evaluated and its relationship with weight loss.
Methods
Participants
This study was conducted at Department of Surgical Sciences of A. Gemelli University Hospital in Rome, in collaboration with the Department of Clinical and Dynamic Psychology of Sapienza University of Rome. After the Ethical Committee approval and informed consent, 76 Caucasic patients, aged 18–60 years, were enrolled. Exclusion criteria were lack of patient consent, preexisting chronic pain disorder, use of analgesic or psychotropic medications, and inability to complete the required psychological assessment in Italian language.
The patients were recruited on the first day of hospitalization for surgery through a face-to-face interview, at clinical ward of the Division of Metabolic and Endocrine Surgery of the Surgical Science Department.
Instruments
On the day before surgery, the following questionnaires were administered to the patients by a trained psychologist in order to assess their psychological status:
The Toronto Alexithymia Scale (TAS-20) is a self-administered questionnaire for the diagnosis of alexithymia that includes, in addition to a total score, three factors defined as “difficult to identify and discriminate emotions,” “difficulty in communicating emotions,” and “externally oriented thinking.” It consists of 20 items to which the subject must assign a score on a 5-point Likert scale whereby 1 = strongly disagree and 5 = strongly agree. The internal consistency of TAS-20 scores was good: Cronbach’s alpha of the total score was .88, of the F1 subscale was .86, of the F2 subscale was .80, and of the F3 subscale was .58 (Bagby et al., 2005).
The Hamilton Depression Scale (HAM-D) consists of 21 items used to assess the severity of depression in adult patients. The HAM-D (21 items) is used in order to evaluate the severity of depressive symptoms. Each item is scored on a 3- or 5-point scale. Internal consistency of the HAM-D was high (Cronbach’s alpha = from .91 to .94) (Reynolds and Kobak, 1995).
The Hamilton Anxiety Scale (HAM-A) consists of 14 items which are scored on a 5-point Likert scale. It is focused on psychic anxiety (mental agitation and psychological distress) and somatic anxiety (physical complaints related to anxiety). The HAM-A showed good internal consistency (Cronbach’s alpha = .89) (Shear et al., 2001).
The Short Form Health Survey (SF-36) includes 36 items divided into eight subscales that assess the following health concepts: physical functioning, physical role functioning, bodily pain, general health perceptions, vitality, social role functioning, emotional role functioning, and mental health. Each of the eight summed scores is linearly transformed into a scale from 0 (negative health) to 100 (positive health) to provide a score for each subscale (Ware and Sherbourne, 1992).
Procedures
After signed informed consent, on the day before surgery, patients were assessed by TAS-20, HAM-D, and HAM-A. QoL was assessed before surgery and 6 months after using SF-36.
Finally, weight loss was assessed in all the patients at 3-month (T1) and 6-month (T2) follow-up. %TWL was used as dependent variable (Jassil et al., 2015; Mack et al., 2016; Thomson et al., 2016).
Statistical analysis
Patients were classified on the basis of the cut-offs of each scale (TAS-20, HAM-A, and HAM-D) for each single independent variable (alexithymia, anxiety, and depression). Repeated-measure analyses of covariance (ANCOVAs) and planned post hoc comparisons were used in order to investigate if alexithymic, depressed, and anxious patients showed significant lower %TWL at studied intervals (T1 and T2). %TWL at T1 and T2 were calculated using the following formula: total body weight at follow-up − total body weight at T0/total body weight at T0 × 100. Body mass index (BMI) at T0 was inserted in these models as a covariate. Gender distribution was analyzed using chi-square test.
Multivariate analysis of variance (MANOVA) was also performed to compare QoL scores before and after surgical operation. Finally, Pearson’s correlations were computed in order to investigate relationship between SF-36 scores and %TWL at T1 and T2. p < .05 was considered statistically significant.
Statistical analyses were performed using Statistica Version 6.1 software (StatSoft, Tulsa, OK, USA, 1997).
Results
None of the patients were excluded from the study. A total of 76 patients (55 females and 21 males; mean age: 40.5 ± 10.3 years; mean BMI: 44 ± 5.6 kg/m2) with completed case report forms were included in the analysis.
Planned post hoc comparison revealed that alexithymic patients experienced a non-significant %TWL at 3-month follow-up (p = .401) and a significant lower %TWL at 6-month follow-up compared with non-alexithymic patients (p = .017) (see Table 1). Moreover, as shown in Table 2, planned post hoc comparison revealed that moderately depressed patients presented a significant lower %TWL at 6-month follow-up (p = .011), but not at 3-month (p = .703) follow-up, compared with non-depressed patients.
Repeated-measure ANCOVA (alexithymia per TIME) on %TWL at T1 and T2 in alexithymic, probably alexithymic, or non-alexithymic patients.
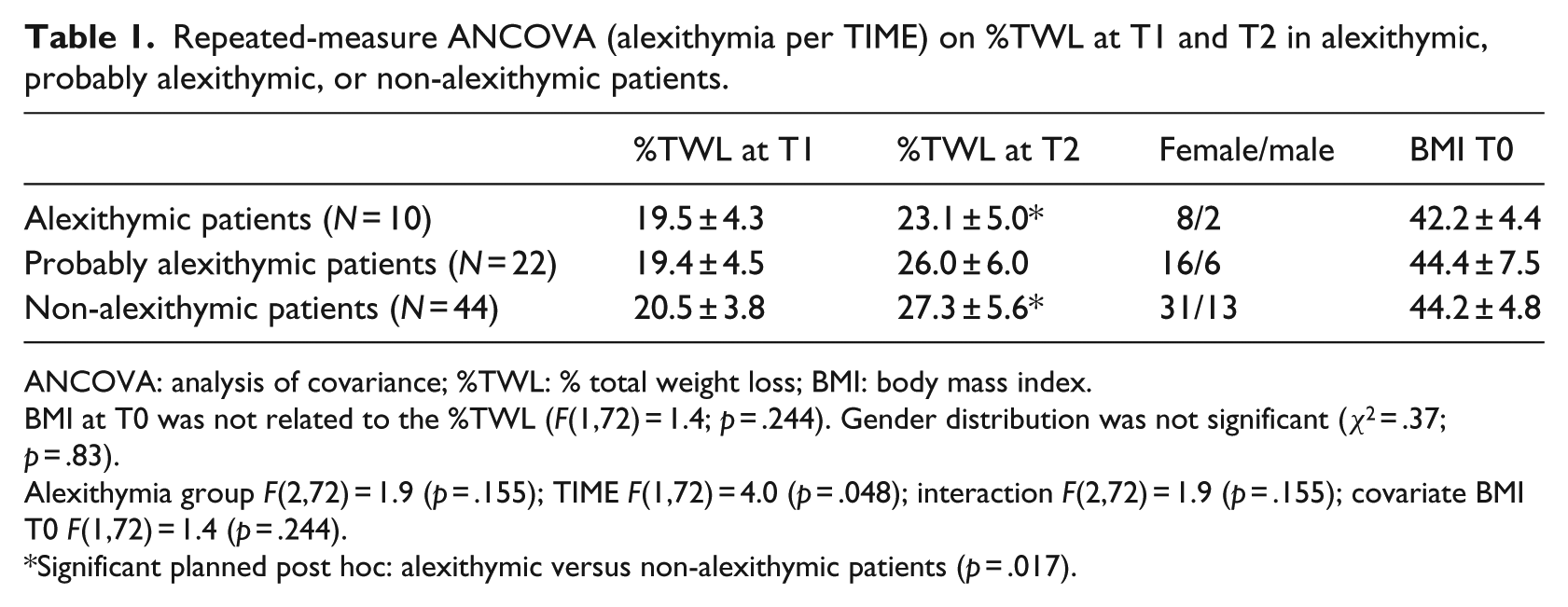
ANCOVA: analysis of covariance; %TWL: % total weight loss; BMI: body mass index.
BMI at T0 was not related to the %TWL (F(1,72) = 1.4; p = .244). Gender distribution was not significant (χ2 = .37; p = .83).
Alexithymia group F(2,72) = 1.9 (p = .155); TIME F(1,72) = 4.0 (p = .048); interaction F(2,72) = 1.9 (p = .155); covariate BMI T0 F(1,72) = 1.4 (p = .244).
Significant planned post hoc: alexithymic versus non-alexithymic patients (p = .017).
Repeated-measure ANCOVA (depression per TIME) on %TWL at T1 and T2 in moderately, mildly, and non-depressed patients.

ANCOVA: analysis of covariance; %TWL: % total weight loss; BMI: body mass index.
BMI at T0 was not related to the %TWL (F(1,72) = 1.9; p = .177). Gender distribution was not significant (χ2 = .54; p = .76).
Depression group F(2,72) = 1.9 (p = .15); TIME F(1,72) = 5.5 (p = .02); interaction F(2,73) = 3.0 (p = .053); covariate BMI T0 F(1,72) = 1.9 (p = .177).
Significant planned post hoc: moderately depressed versus non-depressed patients (p = .011).
Patients with higher values of anxiety did not show different %TWL at 3- and 6-month follow-up (Table 3).
Repeated-measure ANCOVA (anxiety per TIME) on %TWL at T1 and T2 in moderately, mildly, and non anxious patients.

ANCOVA: analysis of covariance; %TWL: % total weight loss; BMI: body mass index.
BMI at T0 was not related to the %TWL (F(1,72) = 1.3; p = .262). Gender distribution was not significant (χ2 = .34; p = .88).
Anxiety group F(2,72) = .9 (p = .390); TIME F(1,72) = 3.8 (p = .055); interaction F(2,72) = 1.9 (p = .161); covariate BMI T0 F(1,72) = 1.3 (p = .262).
BMI at T0 (covariate) was not related to the %TWL in the models. No differences were found regarding gender distribution among alexithymic, probably alexithymic, or non-alexithymic patients, moderately/mild/non-depressed patients, and moderately/mild/non-anxious patients (see Tables 1 to 3).
As shown in Figure 1, MANOVA showed a significant improvement for each scale of SF-36 in the obese patients after gastric bypass (Wilks F(8.67) = 34.5; p < .0001). A significant correlation between the improvement in general health perception and %TWL at T1 and T2 was also found (p < .05).

SF-36 scores before (T0) and 6 months (T2) after surgical intervention.
Discussion
The main finding of this study was that patients with preoperative high levels of alexithymia and depression showed lower %TWL only at 6 months after gastric bypass. Pre-existing anxiety was not able to affect %TWL at 3 and 6 months. Bariatric surgery had a significant impact on all aspects of QoL, and the extent of weight loss achieved by a patient at both 3- and 6-month follow-up was specifically correlated to improvement in patients’ general health perception.
Our findings are partially consistent with previous studies suggesting an association between level of psychological distress/depression and postoperative weight loss degree at 6-month follow-up (White et al., 2015). However, our findings partially seem to contradict a recent research demonstrating that patients with depression have equal weight loss after bariatric surgery compared to controls (Fuchs et al., 2016). However, the study by Fuchs et al. enrolled patients with severe controlled psychiatric disorders who have been excluded in our sample.
Pre- and postsurgical behavioral variables associated with successful weight loss outcomes, such as dietary adherence or observance of outpatient postoperative appointments, have been identified (Robinson et al., 2014), whereas the role of psychological characteristics is controversial. However, suboptimal weight loss in bariatric candidates has been reported in obese patients with psychiatric disorders compared with patients without mentally illness (Gorin and Raftopoulos, 2009; Lanyon and Maxwell, 2007; Legenbauer et al., 2011). Moreover, it has been demonstrated that bariatric candidates having more than one psychiatric disorder are less likely to achieve a successful weight loss (de Zwaan et al., 2011). The possible explanation is that bariatric patients with multiple psychiatric disorders have more difficulties adapting to the postoperative changes. The relationship between psychological characteristics and weight loss degree has been poorly investigated, but it could be the key for poor surgical outcome (Averbukh et al., 2003; Herpertz et al., 2015). The findings of this study highlight that the severity of alexithymia and depression may prevent successful weight loss.
Finally, in this study, anxiety did not affect weight loss in contrast with recent evidences (Aarts et al., 2015; de Zwaan et al., 2011). Further studies are required to clarify this incongruence.
The most peculiar result of our study is the effect of high levels of alexithymia on weight loss after bariatric surgery that has never been investigated. It is possible that the lower observed weight loss in alexithymic and moderately depressed patients should be due to their inability to adhere to postoperative behavioral adjustments. After surgery, these patients could require psychological support in order to cope with lifestyle modifications and to prevent the recurrence of past habits. Associations have been reported between weight loss and both support group attendance and adherence to lifestyle modifications (Livhits et al., 2010). The fact that, in our study, preoperative alexithymia and depression affect weight loss at 6-month follow-up and not at 3-month follow-up also highlights that psychological support is essential in the postoperative period, in order to help the patients to get used to the new lifestyle and to emotive, social, and behavioral changes.
Finally, the association between improvement of patients’ general heath perception and weight loss degree achieved after surgery found in this research, but not confirmed in a previous study (Major et al., 2015), merits further investigation. Improvement of the QoL has become one of the main aims of bariatric treatment (Herpertz et al., 2015; Major et al., 2015).
The main limitation of this study is that only 3- and 6-month follow-up were conducted. Previous research has suggested that results at these times are influenced by the so-called honeymoon period (Golomb et al., 2015). Therefore, the results of this study must be considered preliminary. It could be interesting to evaluate, at long-term follow-up, both preoperative psychological influence on weight loss and relationship between weight loss degree and QoL after bariatric surgery.
In conclusion, from this study it emerges that bariatric patients with preoperative high levels of alexithymia and depression may have more difficulties in achieving successful weight loss at 6-month follow-up. This is a preliminary report of an ongoing trial with long-term assessment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.