
Abstract
This cross-sectional study evaluated locus of control and its subscales in Parkinson’s disease. A total of 50 consecutive Parkinson’s disease participants and 50 healthy volunteers (control group) were enrolled. External locus of control was significantly higher in Parkinson’s disease participants, whereas internal locus of control had no significant differences. External locus of control and internal locus of control were correlated in control group, but not in Parkinson’s disease. In Parkinson’s disease participants, external locus of control was negatively associated with health-related quality of life as well as positively associated with emotional distress and disease severity (but not with disability). After adjusting to confound variables, the associations remained. On the other hand, internal locus of control was negatively associated with depression.
Locus of control (LOC) is a concept that specifically refers to personality psychology and more generally to medicine. Rotter (1966) introduced the concept, as an individual analysis of problems to be solved paralleled by a subjective evaluation of own resources (in a general sense). LOC is assumed to have two components: (1) the internal locus of control (LOC-int), that is, the individuals believe that they are able to control their own life, according to the Latin statement Faber est suae quisque fortunae, that is, everyone is the maker of his or her own fate and (2) the external locus of control (LOC-ext), that is, the individuals believe that their decisions and life are controlled by environmental factors which cannot be influenced. High LOC-int values mean that personal attributes or responses are controlled by the person’s resources. In Rotter’s theory, LOC-int has been associated with better coping and adjustment to chronic diseases. Indeed, those who are confident in their ability to control the destiny (1) are more sensitive to the elements of the surrounding environment, in leading their future behaviours; (2) seek to gradually enhance their surrounding environment; (3) better leverage the increase in their abilities while being more interested in their strengths as well as concerned about their weaknesses and (4) are more resilient to external influence. By contrast, high LOC-ext values mean that personal behaviour is driven by external and more powerful factors, such as chance, politics, genetic inheritance or other entities. For example, Chinese and Japanese people usually consider the fourth day of the month to be unlucky as the word shi means both the fourth and the death. Phillips et al. (2001) found that cardiac mortality in those populations peaked on the fourth day of the month. The peak was particularly large for deaths from chronic heart disease, whereas White controls showed no similar peak. This example is an extreme case of LOC-ext. However, LOC-int and LOC-ext have no dichotomous distribution, rather they range as a continuum.
LOC is also an important dimension to study chronic disorders, especially those, like Parkinson’s disease (PD), which cause a disabling condition requiring extensive coping in daily life. The LOC scale has been rarely applied in PD studies. The LOC-int achieved borderline significance in predicting health-related quality of life (HR-QoL) in a sample of 86 PD patients (Koplas et al., 1999). A relationship between LOC-int and disability was significant in 99 participants, even after adjustment for patient-reported disability and controlling for disease severity. In this study, a greater LOC-int was associated with a lower level of disability (Gruber-Baldini et al., 2009). A study by Zampieri and De Souza (2011) reported a positive correlation between LOC-ext orientation and depression and a positive correlation between LOC-ext and HR-QoL in 30 PD patients, whereas a negative correlation between LOC-int and depression was reported.
From the limited literature, a critical question remained unanswered, such as the extent at which PD patients felt they could control their own life, compared with lay-people. To address this issue, a group of PD patients was matched with a control group (CG) of healthy volunteers. Moreover, this study was also aimed at evaluating the influence of LOC on health-related variables, such as HR-QoL, emotional distress, activities of daily living (ADL), after accounting for sex, age, education and illness severity in PD.
The LOC Rotter’s model was worth studying because it might have been applied when PD patients were screened for rehabilitation in a day-hospital setting. The hypothesis was that those patients scoring high LOC-int had a better quality of life, less emotional distress and a better ADL, on the basis of a successful coping with disability. PD rehabilitation was a costly intervention considering the limited resources. Thus, it was recommended to enrol those patients with adequate personality traits. LOC was hypothesized to provide indication like that. New findings of our group suggested the possible role of personality traits in PD rehabilitation (Gison et al., 2015).
Method
Participants
A total of 60 consecutive patients with diagnosis of idiopathic PD were referred by general practitioners (GPs) of the health district in the period 2012–2013. Only patients with a confirmed diagnosis of idiopathic PD, five or more years of education and symptoms progression evaluated with Hoehn and Yahr’s (1967) clinical rating scale were included in the study. Individuals without a confirmed diagnosis of idiopathic PD, with mental impairment, refusing to sign the informed consent, using dopamine receptors blockers or affected by major comorbidity were excluded from the study. At the end of the screening procedures, which are described below, 10 patients did not meet the inclusion criteria and were not included. Thus, the study consisted of 50 participants (Table 1). They were at stages 2 or 3, based on Hoehn and Yahr (HY) scale (the HY stages range from 1 to 5). The mean duration of illness was 6.5 years (standard deviation (SD) = 2.1). The participants lived at home with their husband/wife or family. A total of 84 per cent of them were retired. Fifty healthy volunteers were randomly selected from the district GPs’ files and invited by letter. The mean age of CG was 67.3 years (SD = 6.1) and mean education was 11.8 years (4.2).
Spearman’s correlation analysis between socio-demographic, psychological and clinical characteristics in healthy controls and in Parkinson’s disease subjects.

LOC-ext: external locus of control; LOC-int: internal locus of control; UPDRS: Unified Parkinson’s Disease Rating Scale; WHO-5: Five-item World Health Organization; HADS: Hospital Anxiety and Depression Scale.
Statistical significant correlation: p < 0.05 (in bold).
The study was approved by the Ethical committee of the I.R.C.C.S. San Raffaele Pisana and a written consent was obtained by all participants.
Procedure
First of all the diagnosis of idiopathic PD was confirmed by movement disorder specialists in the subjects referred by their own GPs, according to the PD Brain Bank criteria (Hughes et al., 1992). All participants had magnetic resonance imaging which showed no alterations due to other brain diseases. The case history was aimed at excluding previous traumatic brain injuries and usage of dopamine receptors blockers. The case history and the clinical check were also aimed at excluding severe comorbidities, such as arthritis, cancer, arterial hypertension, small vessel and heart disease, as well as psychosis. Subsequently, participants were invited to fill in the tool without any time requirement. An investigator was always present (A.G.) to assist the participants without influencing on their own choice among the multiple responses. The same person tested all participants. The interview lasted about 3 hours.
Clinical assessment
The screening procedures used the following scales.
Cognitive function
We used the Italian version of the Mini-Mental State Examination (MMSE; Magni et al., 1996). MMSE consisted of questions on orientation, registration, attention and calculation, recall, language and copying. MMSE was considered to be a screening test for cognitive impairment. The maximum score was 30 points. Values below 22 indicated mental deterioration.
Disease severity
We applied the Movement Disorder Society – Unified Parkinson’s Disease Rating Scale (MDS-UPDRS; Goetz et al., 2007). The MDS-UPDRS had four parts: part I (non-motor experiences of daily living), part II (motor experiences of daily living), part III (motor examination) and part IV (motor complications). All items had five response options. The rank zero meant the absence of any alterations.
LOC
We applied a validated Italian version (Farma and Cortinovis, 2000) of the original Craig et al. (1984) scale. The 17-item Likert-type scale was independent on age, sex and location. The internal consistency was satisfactory (Cronbach’s alpha coefficient = 0.71; LOC-int = 0.67, LOC-ext = 0.71). The version had also satisfactory test–retest reliability after a 3-month interval (Pearson’s correlation coefficient: r = 0.69; LOC-int = 0.54, LOC-ext = 0.67). Seven items evaluated LOC-int and the other items evaluated LOC-ext. About factor analysis the construct validation depended upon all items loading on one common factor, namely, the personal control factor of the Rotter model.
HR-QoL
We used the Five-item World Health Organization Well-Being Index (WHO-5; Bech, 2004) in its validated Italian version (De Girolamo et al., 2000). The scale derived from a larger rating scale developed for a WHO project on HR-QoL. The original items were reduced to five items (WHO-5), which investigated positive mood (good spirits, relaxation), vitality (being active and waking up as fresh and rested) and other than general interests (being interested in things). The short form was more suitable for people with a reduced endurance. The scale was successfully applied to a PD population with Cronbach’s alpha = 0.83 (Schneider et al., 2010).
Emotional distress
We used the validated Italian translation of the scale Hospital Anxiety and Depression Scale (HADS; Costantini et al., 1999) derived from Zigmond and Snaith (1983). The HADS was a self-assessment scale to measure both anxiety and depression. Higher scores meant higher psychological distress. The cut-off scores were fixed at 5 for the partial scores and at 10 for the total score. Equivalent or higher scores classified subjects as psychologically distressed. The subscales were also valid measures of severity of the emotional disorder. In this research, the total score and the two subscales were chosen for statistical analysis.
Disability in ADL
We used the Barthel Index (Shah et al., 1989). The instrument was widely used to evaluate ADL. The scale consisted of 10 items that measured feeding, moving from wheelchair to bed and return, grooming, transferring to and from a toilet, bathing, walking on level surface, going up and down stairs, dressing, continence of bowels and bladder. The highest score was 100, that is, total independence. Since motor fluctuations were common in PD, the best score for each item in the last week was taken.
Comorbidity
We used the Cumulative Illness Rating Scale (CIRS; Linn et al., 1968). The CIRS scale identified 14 items, corresponding to different systems. Each system was scored as follows: 1 = none, no impairment to the specific organ/system; 2 = mild, impairment did not interfere with normal activity, treatment might or might not be required and prognosis was excellent; 3 = moderate, impairment interfered with normal activity, treatment was needed and prognosis was good; 4 = severe, impairment was disabling, treatment was urgently needed and prognosis was guarded; and 5 = extremely severe, impairment was life threatening, treatment was urgent or of no avail and prognosis was not good. Participants with scores over 3 in any item were not admitted in our study.
The MDS-UPDRS and the Barthel scale were compiled by the investigator along with the assistance of a caregiver. Healthy volunteers were invited to fill in only the LOC forms.
Data analysis
A general description of the study population was performed by summary statistics, comparing the PD with the CG through socio-demographic variables (i.e. sex, age and education) and LOC; the PD Group was also described by health-related and disease severe variables (i.e. WHO-5 Well-Being Index, HADS, UPDRS and Barthel Index). The Chi-square test was applied for categorical variables and the unpaired Student’s t test was used for continuous variables. In the PD group, Spearman’s correlation analysis was used to investigate the relationship between the LOC, UPDRS, WHO-5, HADS and Barthel Index scores. Correlation coefficients were expressed as percentage for an easier discussion. The effect of LOC on disability, emotional distress and on well-being was investigated by means of log-linear regression. Mean ratios adjusted for sex, age, education and MDS-UPDRS were estimated, with relative 95 per cent confidence intervals and p values. Threshold for statistical significance was set at p < 0.05. The statistical software we used was STATA/SE V12 (StataCorp., 2011, Stata Statistical Software: Release 12, College Station, TX: StataCorp LP).
Results
PD and CG participants did not differ by age (mean years: 67.1 ± 9.92 vs 67.34 ± 6.15, n.s.), gender (males: 62% vs 56%, n.s) and education (mean years: 10.38 ± 4.16 vs 11.78 ± 4.18, n.s.). The groups were also compared on LOC. LOC-int scores did not differ from the groups (mean scores: 23.46 ± 5.95 vs 24.30 ± 5.10, n.s.), while a statistical difference was found for LOC-ext scores (mean scores: 27.36 ± 8.45 vs 17.82 ± 9.06, p < 0.001). LOC-ext and LOC-int were correlated in CG. The value of R was −0.34 (p = 0.01), whereas in PD the value of R was 0.16 (n.s.). A statistically significant positive correlation was found among LOC-ext score, UPDRS (corr = 34%, p = 0.016) and HADS (total: corr = 35%, p = 0.014; particularly for depression: corr = 38%, p = 0.007), while a negative significant correlation emerged for LOC-int and HADS-depression only (corr = −33%, p = 0.021). The set of results is shown in Table 1.
The effect of LOC on the health variables of our study is shown in Table 2. After taking into account the confounding effect of age, gender and disease severity, only the association between LOC-ext and emotional distress showed significant results. Each increase in one point of the LOC-ext score corresponded to a +4 per cent (95% confidence interval (CI): +2% to +6%, p < 0.001) increase in total emotional distress. No other statistically significant effect was observed, although borderline significant associations were found between LOC-ext and quality of life (a unit increase in the LOC-ext score corresponded to a reduction in 2 per cent of the WHO-5 score (95% CI: −3% to 0%, p < 0.05). Borderline significant associations were also found between LOC-int and HADS, with a unit increase in LOC-int score corresponding to a 2 per cent reduction in anxiety and depression (95% CI: −5% to 0%, p < 0.06).
Effect of locus of control (LOC) on well-being (WHO-5: Quality of Life Questionnaire), anxiety and depression (HADS: Hospital Anxiety and Depression Scale) and disability (Barthel Index).
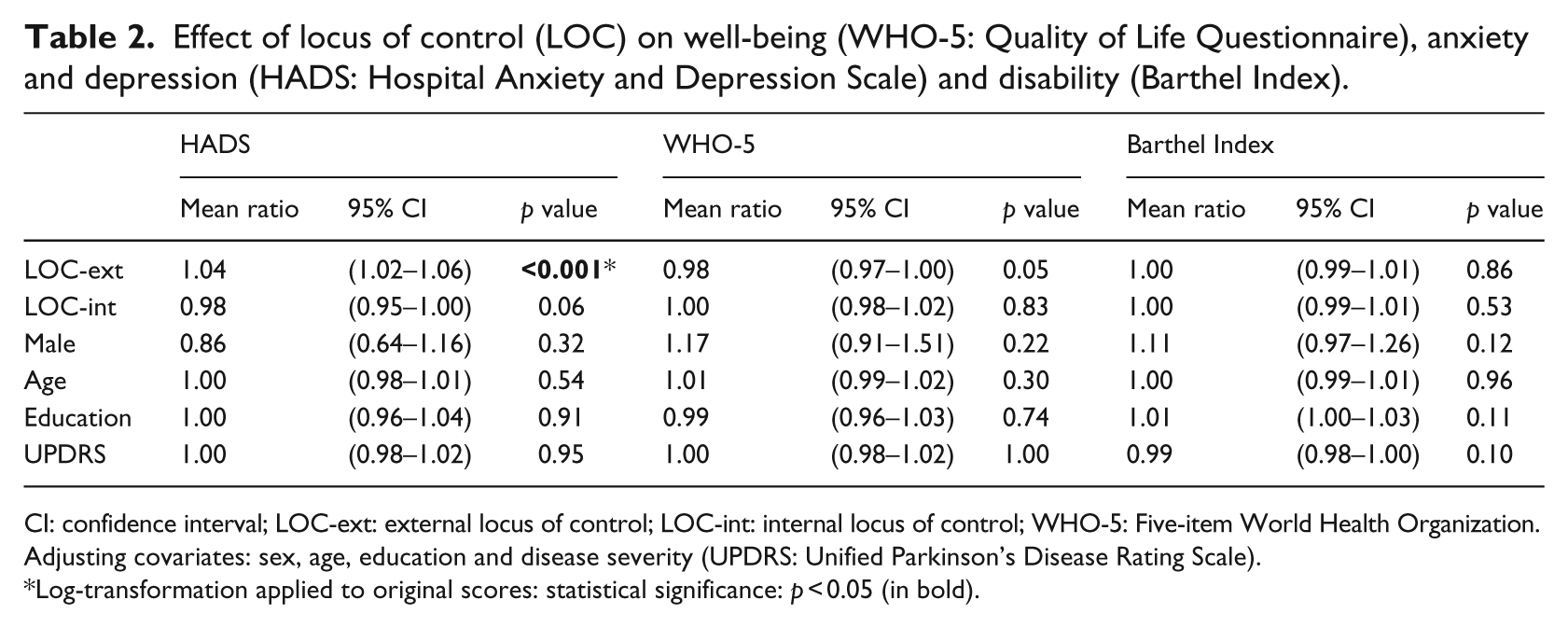
CI: confidence interval; LOC-ext: external locus of control; LOC-int: internal locus of control; WHO-5: Five-item World Health Organization.
Adjusting covariates: sex, age, education and disease severity (UPDRS: Unified Parkinson’s Disease Rating Scale).
Log-transformation applied to original scores: statistical significance: p < 0.05 (in bold).
Discussion
The most remarkable result of this study was the highly significant increase in LOC-ext in subjects suffering from PD. In Rotter’s LOC theory, life experiences are responsible for personal LOC orientation. Negative life events generate the condition known as external control, that is, the feeling of losing control of the life. Depression and disability are factors that can challenge the person’s ability to cope and adjust to different situations. Motor impairment caused by PD is responsible for disability in ADL and induces a feeling of dependency on the person. Early studies on the relation between LOC and depression found that LOC-ext was related to the presence of depression (Presson and Benassi, 1996). Gupta and Bhatia (2000) investigated the psychological factors closely associated with PD impact and found that feelings of dependency, feelings of being a burden and loss of control over their lives contributed to the occurrence of depression. Indeed, a chronic and progressive disease, such as PD, has a negative impact not only in a physical domain but also in cognitive, emotional, behavioural and social areas. Depression, especially in PD, is a combination of both physical and psychological factors (Gupta and Bhatia, 2000). Schrag et al. (2003) investigated the relationship between age of the patient when PD was diagnosed and the impact of the disease. They found that early-onset was frequently associated with difficult adaptation, reduced HR-QoL, loss of employment, a shattered family, greater perceived blame and depression. Moore and Seeney (2007) stated that not only the losses determined the presence of depression but also the way the patient faced them. Gross motor impairment, blaming self, avoidance symptom severity and recreational intimacy were the predictors of depression in a decreasing order of importance. These authors recommend the use of emotion-focused strategies, recreational intimacy and counselling. The evidence from the literature and the result of our study are consistent with the presence of higher LOC-ext in PD patients.
On the other hand, no statistical difference emerged in our study between PD and CG on LOC-int. This finding is in parallel with other observations on Dispositional Optimism (DO; Gison et al., 2014). In that research PD and CG were statistically similar and a decrease in Optimism in the controls was attributed to the political, economical and social difficulties of that period. In other words, PD participants were more concerned about their health, whereas CG participants were more concerned about social problems. We also found that in CG, LOC-ext and LOC-int were inversely correlated (p = 0.01) according to Rotter’s model, but the correlation was absent in PD. Thus, the disease changed some psychometric properties of the LOC. The model was no longer dichotomous. Rather, a continuum should have been conceived from LOC-int to LOC-ext. LOC-int appeared to be less reliable than LOC-ext, at least in our study. Indeed, Cvengros et al. (2005) found that studies in this field were not conclusive yet because there were conflicting findings, sometimes suggesting association between depression and internal orientation, sometimes suggesting the opposite. Our results are in line with those reported by Craig in young subjects with emotional distress, indicating a prevalent role of LOC-ext, but do not exactly overlap with previous findings in PD (Gruber-Baldini et al., 2009), where LOC-int was a better predictor of other health-related variables. A difference in the samples may probably explain the different results. In that research, outpatients visiting a PD centre were enrolled, whereas our participants were awaiting for rehabilitation. Indeed, these results from the literature and from our studies supported the hypothesis that the two tools were not exactly reflecting the same personality traits. The correlations of LOC-ext and LOC-int with other health-related variables were not symmetrical in our sample. LOC-int was negatively correlated with depression (−33%, p = 0.021), but LOC-ext was associated with UPDRS (p = 0.016), with emotional distress (HADS-total: 35%, p = 0.014; HADS-anxiety: 29%, p = 0.041; and HADS-depression: 38%, p = 0.007). LOC-ext was found to be positively correlated with adverse prognosis and disability in case of chronic kidney diseases (Cvengros et al., 2005), low back pain (Oliveira et al., 2008), higher anxiety levels in multiple sclerosis (Vuger-Kovacic et al., 2007) and depression and HR-QoL scores in PD (Zampieri and De Souza, 2011).
LOC-int and sense of coherence (SOC) shared similar features. In Antonovski’s (1979) theory, SOC was assumed to be a useful concept in the fields requiring person’s orientation and internal strengths. SOC was a theoretical model that was proposed to explain successful coping with stressful events of life. In such a way, SOC could be considered as a psychological factor that predicted good health and positive adjustment. SOC had a ‘salutogenetic orientation’ differently from the well-known concept of ‘pathogenetic orientation’, that is, the knowledge of the mechanism explaining the origin and the development of a disease. Compared to persons suffering from other non-neurological diseases, PD patients had a lower SOC score to indicate a less positive attitude in handling stress, but SOC correlated with mood, coping, well-being and HR-QoL (Pusswald et al., 2012). Other personality traits were also considered, like the previously mentioned DO in PD (Gison et al., 2014; Gruber-Baldini et al., 2009; The Global Parkinson’s Disease Survey GPDS Steering Committee, 2002). Dispositional factors, such as DO, and behavioural factors, such as LOC and SOC, influenced the pattern of a progressively disabling disease like PD.
These dimensions were worth studying because they correlated with several psychological factors, including HR-QoL. Personality changes were reported as well. PD patients were more suspicious and cautious than either healthy age-matched individuals or patients suffering from other chronic diseases. With relative uniformity, PD patients were described as stoic, serious, rigidly moral, non-flexible, non-impulsive and with less novelty-seeking behaviour (Eatough et al., 1990; Hubble et al., 1995; Menza et al., 1993; Poewe et al., 1983). Some of these latter personality traits were attributed to a dopaminergic reduction (Brüne et al., 2010; McNamara et al., 2007). The study of DO, LOC and SOC offered a new insight in the perspective of PD rehabilitation.
In our study, a negative significant correlation emerged for LOC-int and HADS-depression, even after adjusting for severity of the disease, while LOC-ext was associated with both components of HADS, that is, not only with depression but also with anxiety, and marginally with the HR-QoL. Interestingly, after taking into account the role of psychological status, disease severity and other major confounders, no association was found between LOC indexes and the degree of disability.
Participants in a global rehabilitation programme should have believed that their behaviour could be controlled before they could be changed. Increasing LOC-int might prompt motivation and help preventive strategies against stressors. The problem-solving coping improved HR-QoL. By contrast, the escape-avoidance coping had negative effects on emotional well-being, mood and social support (Bucks et al., 2011). Group psychotherapy positively was also successful in reducing depression, anxiety and improving HR-QoL (Sproesser et al., 2010).
The results of this study are affected by some limitations. (1) The study has a cross-sectional design, and the study variables were measured at one time-point. (2) The sample included participants in the early stages of PD. The lack of cases with severely disabling PD is explained by testing problems (e.g. some scales require handwriting). (3) The participants have generally a low income and the amount together with the quality of social support is unknown. However, in spite of the limitation discussed above, it is recommended to implement personality traits evaluation in current PD clinical models. PD patients are more than a defective motor device. Each patient is a person, therefore traits of personality are worth studying. LOC may indicate whether a patient can live alone, plan a trip and cope with stressors. Further research is warranted to find whether interventions that promote personal control and positive attitudes may assist in reducing disability and improving HR-QoL in PD participants under rehabilitation.
Footnotes
Acknowledgements
The authors would like to thank all study participants and the staff of the Day Hospital of I.R.C.C.S. San Raffaele Pisana, Rome.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.