
Abstract
Mexican American women are disproportionately affected by overweight/obesity and the health complications accompanying them, but weight loss treatments are less successful in this ethnic group. High levels of familism, a value reflecting obligation to family that supersedes attention to oneself, interfere with weight loss for Mexican American women. This mixed methods study investigated overweight Mexican American women’s beliefs about how familism, and Mexican American culture, might hinder weight loss success, and how treatments might be culturally adapted. Results suggest a need to support women in their commitment to family while also helping them make changes. Recommendations for culturally adapted treatments are made.
Overweight and obesity pose significant health risks, including hypertension, type 2 diabetes, coronary heart disease, and stroke (National Institutes of Health, 1998). Mexican American women are significantly more likely than non-Hispanic White women to be overweight or obese (Hedley et al., 2004; Ogden and Carroll, 2010). Additionally, Mexican American women experience high rates of the metabolic syndrome, a cluster of symptoms associated with obesity that often precedes cardiovascular disease and diabetes (Beltrán-Sánchez et al., 2013). Mexican American women are 1.5 times more likely than non-Hispanic White women to meet criteria for the metabolic syndrome (Ervin, 2009). Given this information, knowledge about effective weight loss treatments for Mexican American women is crucial. 1
Empirical evidence has demonstrated that group behavioral weight loss treatments are effective in general (Wadden et al., 2012), yet weight loss interventions are typically less effective for Hispanic individuals (see review, Lindberg and Stevens, 2007). As a starting point, understanding the cultural meaning of food and weight may help clarify weight loss success that differs by ethnicity. For instance, higher weights in Mexican American culture can signify better health and the ability to provide for one’s family (Lindberg and Stevens, 2011). Furthermore, in Mexican American and other Hispanic cultures, eating can be a common method for coping with grief and trauma (Lindberg et al., 2013). For Mexican American women, providing food can be a sign of hospitality, and refusing food can be offensive (Shea et al., 2012). At the same time, Mexican American individuals endorse receptivity to weight loss information or group treatment (Diaz et al., 2007), and they believe weight loss to be important, particularly for diabetes prevention (Lindberg and Stevens, 2011).
Altogether, these factors suggest a need to study weight loss treatments for Mexican American women. One ongoing and active research area involves the cultural adaptation of such treatments for this population (Lindberg et al., 2013; Rivera and Burgos, 2012). However, culturally adapted weight loss treatments for Mexican American individuals have often resulted in minimal weight loss and significant treatment dropout (Avila and Hovell, 1994; Corsino et al., 2012; Cousins et al., 1992; Lindberg et al., 2012; Lindberg and Stevens, 2011; Poston et al., 2001, 2003). Thus, there is a need for continued investigation, particularly into adaptations of behavioral weight loss treatments known to be effective in other populations.
A review of treatment studies aimed at reducing body mass index (BMI; kg/m2) in predominantly Mexican American samples highlighted the cultural adaptations employed to date, such as involving family members in treatment, conducting treatment in Spanish, working with promotoras or community health workers, providing guidance on meal plans, creating early interventions for schoolchildren, and providing treatment in familiar community settings (Rivera and Burgos, 2012). Although a number of these adaptations appear promising, focused research is needed in order to systematically test which treatment modifications, if any, are essential. Furthermore, this review included many studies targeting children. Thus, research on which cultural adaptations work best in adults is still needed.
One potential key to adapting behavioral weight loss treatments is to focus first on understanding (and then ultimately addressing) culturally specific barriers to weight loss. One barrier identified in the literature is a high level of familism, a cultural value which reflects obligation to one’s family and to family relationships that supersedes attention to oneself (Austin et al., 2013). This value, found cross-culturally, is thought to be particularly relevant in Hispanic cultures (Steidel and Contreras, 2003). In a standard behavioral weight loss program (LEARN; Brownell and Center, 2004; Gardner et al., 2007), Mexican American women high in familism lost less weight, were less successful at meeting physical activity and calorie goals, and had higher attrition than those lower in familism (Austin et al., 2013). In line with this finding, Mexican American women in one qualitative study (Martinez et al., 2009) and Central or South American women in another (Greaney et al., 2012) reported that family responsibilities, such as childcare and family meal preparation, made it difficult to eat healthily and exercise. Interestingly, some evidence suggests that Mexican American individuals tend to lose weight in programs that involve families and focus on healthy lifestyle changes at home (Rivera and Burgos, 2012). These findings underscore the need to consider the role of familism in weight loss treatment for Mexican American women.
Given this, it seemed worthwhile to investigate how familism might affect Mexican American women’s success in behavioral weight loss treatment (Austin et al., 2013). Using focus groups, overweight Mexican American women were asked why they believed women high in familism lose less weight in treatment, and how being Mexican American may play a role. Study participants also were asked to make recommendations to improve treatments. Finally, quantitative questionnaires assessing acculturation and familism were administered in order to characterize the sample and provide a context for findings. The objective of this study was to identify ways to modify behavioral weight loss/healthy lifestyle programs so that they could be sensitive to the unique needs of Mexican American women. The effectiveness of these adapted programs would be tested at a later date.
Method
Participants
Study participants included 34 community women recruited from a greater metropolitan area in the southwestern United States. Inclusionary criteria were as follows: (1) female, (2) age 18–65 years, (3) BMI ⩾ 25 and ⩽40, and (4) self-identified heritage in current or former territories of Mexico (e.g. Mexican American, Mexican, Chicana). Exclusionary criteria were as follows: (1) pregnant or planning to become pregnant, (2) living or planning to move more than 50 mi from the study site, and (3) lack of proficiency in English. Participants received eligibility for a complementary weight loss workshop as an incentive. All participants completed the informed consent process as approved by the University of New Mexico IRB.
Measures
All measures were administered in English. Participants’ comfort with filling out the questionnaires in English and participating in an English-speaking focus group was queried during the phone screening, at which time the research assistant also informally assessed the interviewees’ English fluency.
Demographic questionnaire
This measure contained a checklist assessing ethnic background, languages spoken, educational background, current income, occupational status, and family composition.
Scale of Ethnic Experiences
This 32-item measure examines acculturation and ethnic identification using four subscales: ethnic identity (pride and identification with one’s ethnic group), perceived discrimination (one’s perception of discrimination toward one’s group), mainstream comfort (an individual’s perception of him or herself as a typical member of the dominant American culture), and social affiliation (one’s degree of emphasis on the importance of affiliating with one’s own ethnic group) (see Malcarne et al., 2006). Each item is rated on a 5-point rating scale (“strongly disagree” to “strongly agree”), with higher scores on each subscale indicating more experience with that factor. The Scale of Ethnic Experiences (SEE) demonstrated concurrent validity with other measures of acculturation and achieved adequate inter-item reliability with ethnically diverse samples (Malcarne et al., 2006). It was included in this study to characterize the sample’s acculturation to Anglo-American culture and relationship with Mexican American culture. In this sample, the inter-item reliability values for each subscale were as follows: ethnic identity, α = .71; perceived discrimination, α = .61; mainstream comfort, α = .59; and social affiliation, α = .84.
Attitudinal Familism Scale
This 18-item measure examines familism (Steidel and Contreras, 2003). Responses are on a 10-point Likert scale with scores ranging from 18 to 180, with higher total scores denoting higher familism. This measure also has four subscales: familial support, familial interconnectedness, familial honor, and subjugation of self for family. In a US Hispanic population, scores on this measure correlated negatively with acculturative status (Steidel and Contreras, 2003). For this study, only the total score was used (α = .86). The Attitudinal Familism Scale (AFS) was included in this study to provide a context for how relevant familism was to the participants themselves.
Procedure
Participants were recruited via flyers posted in community locations. The flyers sought overweight Mexican American and Chicana women who had weight concerns and were willing to participate in a focus group study about women’s weight loss. Interested women contacted the researcher and were screened for eligibility before attending the focus groups.
The study took place at a community health center located in a predominantly Hispanic neighborhood. Participants were informed about the study procedures in written and verbal formats, and questions were addressed before participants gave consent. Participants were weighed to ensure they met the BMI inclusion criteria, with information about weight loss treatment options available for those who did not meet the criteria.
A total of five separate focus groups were conducted. At the start of each group, participants agreed to protect the confidentiality of group members and consented to be audio-recorded. They were encouraged to express their opinions, and to respect and respond to the opinions of others (Ingram et al., 2009). Focus groups were structured around three open-ended questions emphasizing familism, ethnic identity, and weight loss (see section “Results” for the questions). The moderator only intervened to keep time, to allow multiple opinions to be expressed, and to remind the group about the target questions. Focus groups lasted approximately 2 hours.
Data analysis
Qualitative data analysis was based on processes used in other recent, similar focus group studies (Franko et al., 2012; Webb et al., 2013). Generally, this involved having multiple members of the research teams read focus group transcripts and develop initial conceptualizations of the themes in the data. Then, these lists of themes were refined through successive readings and team discussions.
For this study, all sessions were transcribed. First, the research team read the transcripts and developed a preliminary list of themes, with all discrete statements coded. One statement could receive multiple codes. Next, the research team split into three dyads. Dyads read transcripts from two focus groups for each of the three open-ended questions, and revised themes and definitions as necessary. The entire team met to review the themes, definitions, and examples, and to revise the codebook accordingly. Using the revised codebook, dyads coded the remaining three focus groups’ transcripts, noting problems in the process. The codebook was revised again by the entire team, and all transcripts were re-coded. Dyads met and reached consensus on their coding. Finally, the whole team met and finalized the codes via consensus.
Results
Demographics
Demographic information is presented in Table 1.
Demographics.

BMI: body mass index, SD: standard deviation; in all instances, $ refers to USD.
Acculturation and familism
SEE subscale scores are presented in Table 2, along with scores from a comparison sample of Mexican American adults, which were provided by the SEE’s developer (Vanessa Malcarne, 2015, personal communication). The mean total score on the AFS was 101.6 (standard deviation (SD) = 20.3; range: 66–154) out of a possible 180 points (see section “Discussion” for interpretation of quantitative results).
Scale of Ethnic Experience Scale scores.
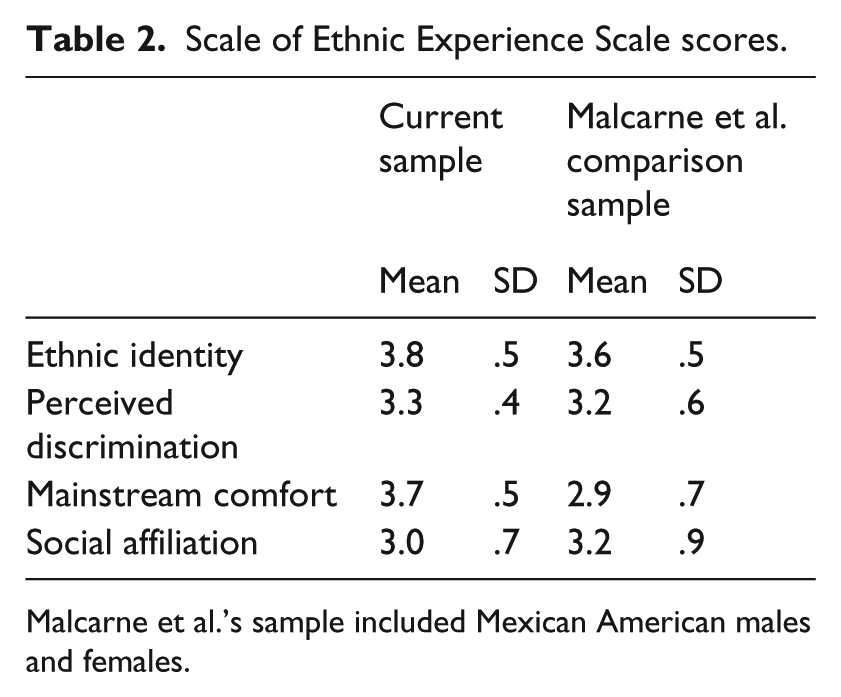
Malcarne et al.’s sample included Mexican American males and females.
Focus group themes
The most common themes across the focus groups are detailed below and are listed in Table 3. The least common themes (the bottom one-third in terms of frequency with which they were mentioned) are not described here. Definitions, quotes, and frequencies for these themes are available from the authors.
Focus group themes.
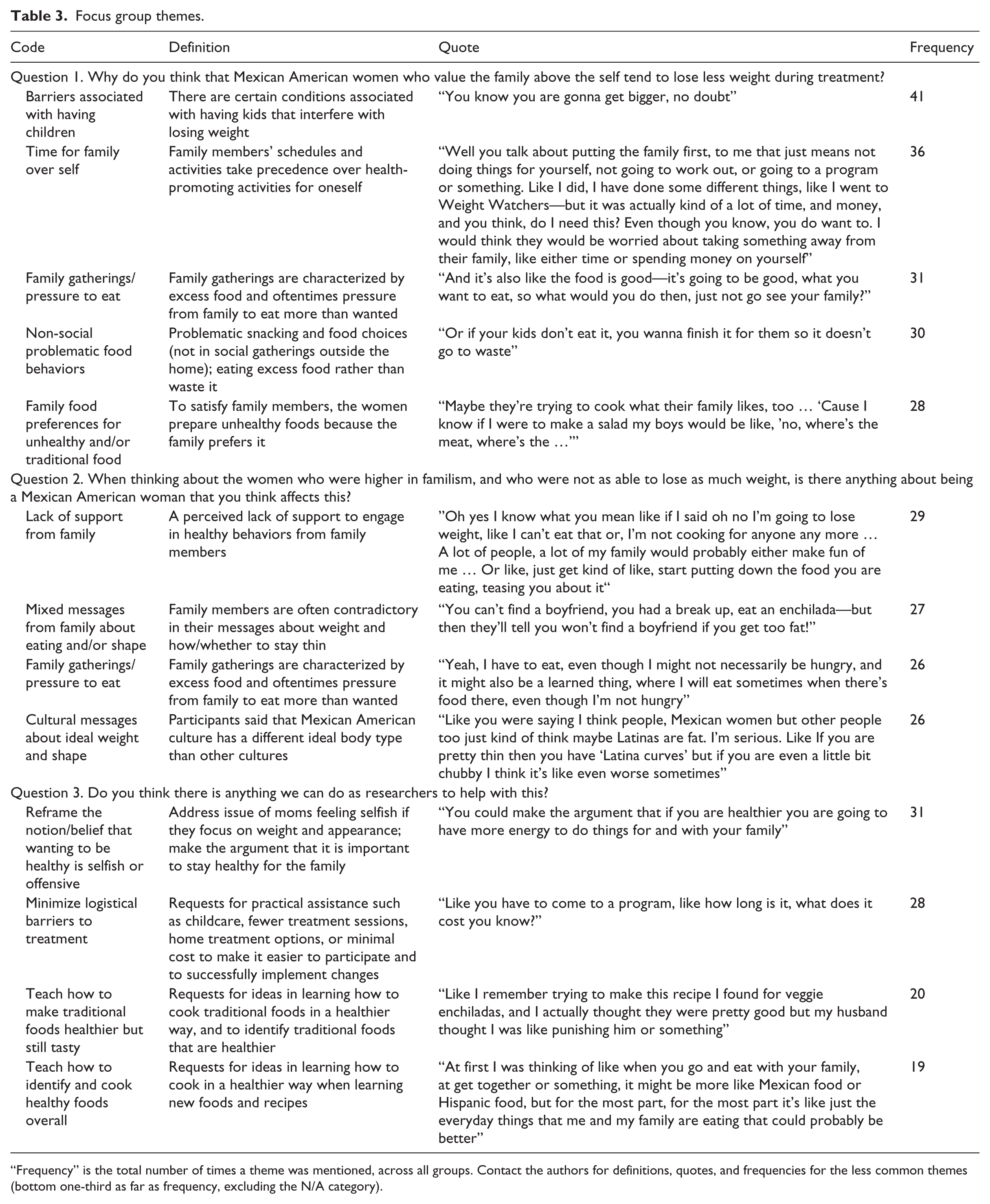
“Frequency” is the total number of times a theme was mentioned, across all groups. Contact the authors for definitions, quotes, and frequencies for the less common themes (bottom one-third as far as frequency, excluding the N/A category).
Question 1: the role of familism in weight loss treatment outcomes
The first prompt was A previous study found that Mexican American women who reported that they highly valued familism actually lost less weight than those who did not value familism as highly. Why do you think that Mexican American women who value the family above the self tend to lose less weight during treatment?
The most common themes for this question are below, starting with the highest frequency response.
Barriers associated with having children
Participants said that women high in familism are likely to have children and be highly invested in their children’s lives. One woman said, “Maybe women who are putting their family first are with their kids a lot more.” The women also believed that having children required having more food at home, because of children’s nutritional needs. They talked about having limited time to care for themselves, due to the time required for childcare. Women agreed that weight gain during pregnancy was inevitable, and that weight loss afterward was difficult.
Time for family over self
Participants explained that Mexican American women are expected to spend most of their time with family. Health-promoting or weight loss behaviors may take time away from family: When my kids were really young … I probably wouldn’t have taken time out to work out; Familismo means that you do things together and you’re going to do things for your family, so doing something on your own, like all, “I’m going to go be on a diet or start an exercise program,” it doesn’t make as much sense.
Family gatherings/pressure to eat
Participants described norms about eating at family gatherings, such as “I have a bigger family, and we do, we get together a few times a week and it’s like you’re always going to have more food.” Women generally felt that the food at Mexican American family gatherings was unhealthy, but also stated, “Your family might think that you’re acting picky if you are trying not to eat certain things.”
Non-social problematic food behaviors
Some women talked about food choices that were not necessarily in the context of social gatherings, such as excessive snacking, choosing unhealthy foods in general, eating while cooking, or eating leftover food rather than wasting it. One woman said, “The thing that my mom always did was, she’d say, ‘Oh, there’s just a little bit left, just finish it’—and that’s a bad habit, but I’m learning not to do that.”
Family food preferences for unhealthy and/or traditional food
Participants said that Mexican American families often prefer unhealthy foods: “I will go to my friends’ or family’s house and eat, and [it’s] not going to be really healthy food.” The women explained that they face conflict when deviating from their family’s usual foods, such as “I think it’s just wanting to eat with your family in general, the foods they want, … and not feeling like you can either do it on your own … or like make everyone change.”
The lower frequency themes were as follows: lack of support from family, cooking separate healthier meals for themselves, minimizing selfish and guilty feelings, money limitations, women’s value based on food taste and/or family competition, and not applicable (N/A).
Question 2: the role of Mexican American culture in weight loss treatment outcomes
Second, participants were asked, “When thinking about the women who were higher in familism, and who were not as able to lose as much weight, is there anything about being a Mexican American woman that you think affects this?” Again, the most common themes are below, beginning with the highest frequency response.
Lack of support from family
Some women said that their families did not approve of attempts to lose weight. One participant said, “If you are doing something to try to lose weight, they might tell you, on the one hand that it’s a little odd—you know like you’re fine the way you are.” Another said, “When you take time to do something else, or change the routine, then you might get a lot of pushback.”
Mixed messages from family about eating and/or shape
Women said that family members often made contradictory statements about weight. One woman explained, “You can’t get too fat, but then they will always feed you,” while another said, For me, even though I am bigger, I can still … get comments about making sure to fill up at meals because I don’t have enough meat on me. But then I also get comments telling me I am too fat, like even my husband will say both things.
Family gatherings/pressure to eat
This theme reflected similar experiences as the theme of the same name under Question 1 (above).
Cultural messages about ideal weight and shape
Some participants indicated that Mexican American culture has a different ideal body type than other cultures, including acceptance of heavier weights. Women said that their families believed, “Thick is good, thick is better,” and “Curvier the better.” One woman said, “It’s kind of like, maybe we would all like … to be thin and everything, but it’s also … like, not really.”
Lower frequency themes were as follows: time for family over self, family food preferences for unhealthy and/or traditional food, viewed weight gain as inevitable, cooking and food education, not raised to exercise/play sports, money limitations, and N/A.
Question 3: recommendations for researchers for culturally adapted treatments
Finally, participants were asked, “Thinking once again about the study in which Mexican American women who were high in familism lost less weight than those who were not, do you think there is anything we can do as researchers to help with this?” The most common themes are below, again beginning with the most frequent.
Reframe the notion/belief that wanting to be healthy is selfish or offensive
These statements addressed the norm that Mexican American women are made to feel “selfish,” “vain,” or “guilty” if attending to their health. Some offered alternate ideas to counteract this: “You stay healthy for your family” or “… not taking care of yourself is selfish because then you abandon your family [due to consequences of overweight].”
Minimize logistical barriers to treatment
Women offered a variety of practical requests to make treatment participation more feasible. Suggestions included childcare or children’s activities, fewer treatment sessions, home treatment options, and reduced treatment costs.
Teach how to make traditional foods healthier but still tasty
Women said that they wanted to retain traditional recipes, but make them healthier. One participant explained, … [On] websites about losing weight and everything, you look at the foods and the recipes and it’s like, ‘umm, am I really going to make that?’ And our [traditional] foods are not on there. To me it’s kind of depressing, because we know how to make some really good things, and it’s not like I am just never going to eat those foods again.
Teach how to identify and cook healthy foods overall
This theme included other requests for healthy cooking ideas, not in the context of traditional Mexican American food. Specifically, women indicated that they felt they lacked nutrition knowledge: “Maybe just breaking through those different oils, though, because it took me a long time to try olive oil,” and “It’s just the everyday things [rather than at parties/gatherings] that me and my family are eating that could probably be better.”
Lower frequency themes were as follows: teach how to eat in moderation, involve family in treatment, have group leader/visitors with similar experiences and who have successfully lost weight, teach how to modify family meals for dieting women, and N/A.
Discussion
This study provides novel information about the cultural context of Mexican American women’s weight loss efforts, specifically the role of familism. Although familism is a cultural strength, high levels have been shown to interfere with successful weight loss treatment for Mexican American women (Austin et al., 2013).
Acculturation and familism
Given the current sample’s higher score on the SEE’s mainstream comfort subscale than the score for a large recent sample of Mexican American adults (Vanessa Malcarne, 9 December 2015, personal communication), the current sample appears to be more highly acculturated when compared to Malcarne and colleagues’ sample. Comparable scores across the two samples on the other SEE scales suggest that participants in the current sample are otherwise representative of Mexican Americans in the United States overall. Participants were fairly highly identified with Mexican American culture, relatively highly affiliated with other Mexican American individuals, and fairly highly aware of experiences of discrimination.
Possible total scores on the AFS range from 18 to 180. The AFS total score in the current sample was 101.6, while in Austin et al. (2013) it was 119.1, and in an outpatient mental health treatment sample of Mexican American women it was 121.4 (Garza and Pettit, 2010). At times, an average rather than a total score is calculated. Hispanic samples which have not been predominantly Mexican American have obtained average scores of 7.35 (Steidel, 2005) and 7.99 (Baumann et al., 2010) on a 0–10 scale. In this study, the average score was 5.64. Scores reflected lower attitudinal familism than in similar samples, but given the range of possible scores, the familism scores in this sample do not appear unusually low. Thus, group members appeared to be able to provide reasonable insight on questions regarding familism.
Qualitative themes
Several themes were prominent in group discussions. It should be noted that in some cases, the researchers were uncertain as to whether a theme related to familism per se, or was more generally reflective of the experience of being a Mexican American woman. For instance, Mexican American cultural standards involving acceptance of higher weights (Diaz et al., 2007) and barriers such as time limitations and financial constraints (Martinez et al., 2009) are likely relevant across many Mexican American women samples. Similarly, some themes may be relevant for many overweight women, regardless of race/ethnicity, such as the sense that friends and family object to or undermine one’s attempt at weight loss (Whale et al., 2014), the idea that women’s families will refuse to change their diets to eat healthier foods, or the habit of finishing children’s leftovers (Chang et al., 2008). However, given that the focus group facilitator stressed that the discussion should address Mexican American women’s experience with high familism as a barrier to weight loss, we decided to report all the main themes that emerged regardless.
With this in mind, one of the most common themes was women reporting that they had minimal time for healthy self-care (e.g. making healthy meals, exercising) because of their responsibility to spend time with their families, particularly their children. This echoes findings from other studies (Greaney et al., 2012; Martinez et al., 2009). And again as in other studies, many women believed that their families would not support their weight loss efforts, because adding new habits and activities could interfere with family routines and preferences (Greaney et al., 2012; Shea et al., 2012). Participants also reported that family members might tease them or indirectly impede weight loss attempts, and group members said that constraining one’s eating at family gatherings was viewed as disrespectful and inappropriate, as noted in Greaney et al. (2012) and Shea et al. (2012) as well.
In a more novel theme, women said that they sometimes received mixed messages from family about whether they should attempt to lose weight. In this vein, one of the most common themes reflected the idea that Mexican American culture values higher weights for women, making weight loss efforts less acceptable. In Mexican culture, heavier women are considered to be healthy and nurturing, and being overweight signifies that a woman can provide for her family (Bojorquez-Chapela et al., 2014; Lindberg and Stevens, 2011). Given this, family members (and women themselves) may be ambivalent about the need for weight loss despite potential health consequences. Interestingly, a recent qualitative British study with women who were attempting to lose weight found the rather similar theme of family and friends being ambivalent about the women’s weight loss attempts (Whale et al., 2014).
The women in this study routinely suggested that weight loss programs should teach participants how to cook in a healthy manner, both traditional foods and new foods that their families might enjoy. Their concern about not wanting to give up traditional foods is one that arose in other focus group work on weight loss with Mexican American women (Lindberg and Stevens, 2011), and efforts to retain traditional recipes and foods have been a component of several previous weight loss treatments with Latino individuals (Corsino et al., 2012; Rivera and Burgos, 2012).
The possession of bad habits, such as snacking while cooking and eating leftovers when not hungry to avoid being wasteful, was another theme often raised by women in this study. Such habits were noted in another qualitative study about Latina weight loss (Greaney et al., 2012), and this repeated finding emphasizes the need to provide guidance for addressing these habits. Other related habits entailed consuming overly large portions and eating readily available food because the women were distracted while attending to family needs.
Recommendations
The following are preliminary recommendations (subject to scientific testing), based on the focus group discussions, for modifying weight loss programs so as to include cultural adaptations for Mexican American women:
Reframe the mistaken notion that wanting to lose weight is selfish. Providers should be keenly aware that women might be receiving minimal support, or even mixed messages, when attempting to lose weight. Clinicians should:
Discuss with overweight weight loss participants themselves how weight loss will allow them to be more present for their families, because improved health could allow them to spend more quality years with their loved ones.
Teach the women basic communication skills (and include role-plays) so they can talk with their families about the link between weight loss and improved health, and what this means for the family more generally.
Facilitate talking about the family context throughout treatment. Mexican American women might benefit from an ongoing discussion of the cultural context in which their weight loss efforts are occurring. For instance, since food may represent hospitality and support, helping women negotiate common situations in which they are offered unwanted food could be key (Shea et al., 2012). Clinicians should:
Set aside time each session to discuss the families’ reactions to the women’s weight loss efforts.
Teach a step-by-step behavioral problem-solving procedure (e.g. Smith and Meyers, 2004), and show how to apply it to new family problems that arise each week.
Teach “food refusal skills” for respectfully yet assertively turning down offers of unwanted food from family members.
Minimize logistical barriers to treatment. The matter of women not wishing to disrupt their families’ lives and habits with their own weight loss efforts has arisen in other qualitative work with Mexican American women (Lindberg and Stevens, 2011; Shea et al., 2012). Additionally, previous studies have found that missed sessions are common in weight loss treatment with Latino individuals (Austin et al., 2013; Corsino et al., 2012). Clinicians should:
Provide flexible session scheduling.
Offer additional sessions so that opportunities are readily available to make up missed sessions.
Offer remote or online treatment options to minimize childcare, travel burdens, and cost.
Provide instruction in healthy cooking. Many requests were made for basic cooking education and instruction, and there are multiple ways to approach this request. One culturally adapted treatment includes examining nutrition values in commercially available Mexican food and disseminating information about healthier versions of traditional foods (Lindberg et al., 2012). Clinicians should:
Provide instruction and practice in preparing uncomplicated, inexpensive healthy food recipes in general.
Demonstrate concrete ways to make traditional foods healthier while retaining taste.
Make assignments for participants to try out the new/modified food at home, and address problematic family reactions in the next session.
Offer specific plans for addressing common problematic eating behaviors. The women repeatedly requested assistance with some standard eating behaviors they viewed as problematic (e.g. excessive snacking, overeating leftovers, lack of portion control). Clinicians should:
Apply the problem-solving technique (see 2b) to various problematic eating behaviors (e.g. how to eat in moderation).
Query in subsequent sessions as to whether the behavioral plan worked or whether it needs to be modified. Get commitments to specific homework assignments.
Strengths and limitations
This study’s qualitative methodology allowed women to explain important perceived barriers to weight loss. This study also retained a narrow focus on familism, and produced information that will help tailor weight loss treatment for Mexican American women. Themes produced from the discussions in this study echoed results from similar studies (Greaney et al., 2012; Lindberg and Stevens, 2011; Shea et al., 2012), lending strength to the recommendations.
The study was limited by its restricted sample. Participants were overweight Mexican American women interested in receiving weight loss treatment, but they may not have been representative of women high in familism who were less successful in treatment. However, recruitment for this study was similar to recruitment for the study finding poorer outcomes for high-familism Mexican American women (Austin et al., 2013). It also may have been desirable to conduct focus groups in Spanish to capture a more varied sample of Mexican American women. Finally, the level of acculturation was fairly high in this sample, as was the average income and education level. Thus, it is unclear whether the findings would generalize to less acculturated women with different demographics.
Conclusion
Generally, treatments that allow overweight Mexican American women to prioritize their families and take care of their own health should be explored. The themes in this study suggest the need for a supportive and understanding approach to family dynamics during women’s weight loss treatment, in conjunction with a problem-oriented approach to behavior change.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Campos-Melady was supported on a Dissertation Fellowship through the University of New Mexico and Robert Wood Johnson Foundation Center for Health Policy during the data collection phase of this study.