
Abstract
This study examined the interactive role of perceived control and preference for control on adherence in a sample of patients with chronic kidney disease. As part of a randomized controlled trial assessing adherence to fluid-intake restrictions, 119 hemodialysis patients completed measures of these constructs; results indicated that patients with high perceived control and high preference for control demonstrated the most favorable adherence. This suggests that patients who believe health-related outcomes are a function of one’s own behaviors—and having the opportunity to exert control over aspects of treatment—may be most adherent to complex regimens in which self-management is key.
Keywords
Over 1.9 million patients worldwide with severe chronic kidney disease (CKD), a debilitating chronic illness often requiring life-sustaining renal replacement therapy, are treated with center-based hemodialysis (Fresenius Medical Care (FMC), 2011). Treatment requires adherence to a multifaceted behavioral regimen, including fluid and dietary restrictions in order to maximize the effectiveness of dialysis and limit burdensome complications. Perhaps the most challenging of these restrictions is the reduction in fluid consumption to approximately 1 L/day or less (see Denhaerynck et al., 2007). Research suggests that 30–60 percent of patients fail to adhere to fluid-intake recommendations (Bame et al., 1993; Christensen et al., 1997; Friend et al., 1997; Schneider et al., 1991), which is associated with uncomfortable and prolonged dialysis sessions as well as medical complications including bone demineralization, pulmonary edema, hypertension, congestive heart failure, and increased risk of mortality (see Christensen and Ehlers, 2002).
In general, non-adherence to chronic illness treatment is quite costly, both financially and in terms of patient burden (Howren, 2013), and may be attributable to any of several reasons, such as the degree of behavioral restriction, regimen complexity, social environment, treatment cost, and individual difference characteristics, among others (see Christensen, 2004). The latter has garnered considerable attention in psychology with numerous studies examining personality and individual difference characteristics as predictors of adherence (e.g. Adam and Folds, 2014; Axelsson et al., 2011; Bouchard et al., 2003; Christensen et al., 1999; DiMatteo et al., 2007; Hilliard et al., 2014; see Christensen and Smith, 1995; see Christensen, 2004; see Martin et al., 2005), including in this patient population (e.g. Cvengros et al., 2004; Moran et al., 1997; Wiebe and Christensen, 1997).
Perceived control, preference for control, and adherence
One individual difference characteristic in particular, health locus of control (HLC), has been extensively examined in the context of patient adherence (O’Hea et al., 2009; Wallston, 2005; Wallston and Smith, 1994). HLC captures the extent to which one believes that health-related outcomes are a function of one’s own behaviors (i.e. an internal orientation) versus some outside factor, such as chance or provider influence (i.e. an external orientation). Several studies have reported associations between HLC and adherence (e.g. McDonald-Miszczak et al., 2000; Morowatisharifabad et al., 2010; Omeje and Nebo, 2011; see O’Hea et al., 2005), while others notably have not (e.g. Bunting and Coates, 2000; Kneckt et al., 1999), but most have done so by examining the HLC constructs as main effects only. Fewer have studied the interaction among HLC constructs themselves and/or other variables (e.g. Christensen et al., 1991; O’Hea et al., 2009), despite evidence that such an interaction may be most important in predicting adherence and calls reiterating as much (O’Hea et al., 2005, 2009; Wallston, 2005; Wallston and Smith, 1994).
For example, O’Hea et al. (2009) examined the interaction among internal HLC, self-efficacy, and outcome expectancy in a sample of patients with type II diabetes. They reported a three-way interaction relative to the primary outcome, HbA1c, such that diabetics having both low self-efficacy and outcome expectancy, but high internal orientation, were more adherent. Conversely, patients were less adherent if having a high internal orientation, low self-efficacy, and high outcome expectancy. When analyzed as main effects, however, control beliefs and outcome expectations did not significantly relate to adherence.
Others have reported similar findings with respect to control-related variables (e.g. Christensen et al., 1991; Cvengros et al., 2004; Logan et al., 1991), including preference for control. For example, one study investigated the interaction between perceived control and desired control during a stressful dental procedure, finding that those with high preference for control, but low perceived control, had increased distress and avoidance (Logan et al., 1991). Cvengros and colleagues specifically examined the interaction between perceived restriction of control (using a rationally derived measure) and preference for control in the context of hemodialysis. They found that those patients who exhibited greater preference for control, but low perceived control, demonstrated increasingly poorer adherence which was severe enough to be deemed clinically non-adherent. When considered alone, neither variable was significantly associated with adherence. These results further underscore the need to consider variables capturing health-related control within an interactional framework.
The present study
This study sought to examine the joint role of perceived control, conceptualized as the extent to which patients were internally versus externally oriented on a measure of HLC, and preference for control in relation to medical regimen adherence in a sample of patients with CKD receiving treatment in a center-based dialysis setting. As noted above, CKD often requires adherence to a complex behavioral regimen, including fluid and dietary restrictions, with appropriate patient self-management directly related to various treatment outcomes, thus making it ideal to study aspects related to patient control. In light of research reviewed above, we hypothesized that those patients with both a high degree of perceived control and a strong preference for control would exhibit the greatest improvement in adherence to fluid-intake recommendations from baseline to post-treatment as measured by an objective marker often used in this patient population (see Clark et al., 2014).
Methods
Participants and protocol
As part of a behavioral self-regulation intervention trial comprising seven 1-hour weekly sessions designed to improve fluid-intake adherence, 119 non-adherent patients were recruited from hemodialysis centers across Eastern Iowa and Western Illinois. Eligible patients were (a) fluid non-adherent as defined by an interdialytic weight gain (IWG) > 2.5 kg over a 4-week period (see Christensen and Raichle, 2002), (b) > 18 years of age, (c) English-speaking with no severe cognitive impairment, (d) treated with center-based hemodialysis for >3 months, and (e) not living in a care facility in which meals were managed. Medical records were used to identify eligible patients who were then approached regarding potential participation by a research assistant during the patient’s routine hemodialysis treatment session. Upon consent, patients completed baseline measures of perceived control (i.e. HLC) and preference for control over their medical care.
For the purposes of this study, analyses are presented collapsed across trial arm (i.e. combing intervention and control patients). Justification for this is based on the fact that there was no significant difference between the intervention and control groups on the primary outcome, change in IWG. 1 A complete description of the intervention trial and primary results are reported elsewhere (Howren et al., 2015). All procedures were approved by the University of Iowa’s institutional review board (IRB).
Key measures
Perceived control (HLC)
Perceived control was measured using the six-item Internal subscale of the Multidimensional Health Locus of Control (I-MHLC) scale (Wallston et al., 1978). The I-MHLC was presented in six-point Likert format ranging from Strongly Disagree to Strongly Agree and measures the degree to which a patient attributes the cause of health-related outcomes to internal factors under one’s own control (i.e. a patient’s own actions). Sample items include the following: “If my condition takes a turn for the worse, it is because I have not been taking proper care of myself” and “If my condition worsens, it is my own behavior which determines how soon I will feel better again.” Coefficient alpha in this sample was .77.
Preference for control
Patient preferences for control in the healthcare setting were assessed using the Krantz Health Opinion Survey (KHOS; Krantz et al., 1980). The KHOS is a 16-item scale presented in agree/disagree format designed to capture patient tendencies to seek health-related information and prefer opportunities for active involvement in one’s medical care. In addition to a total score, two subscale scores—the Preference for Information (seven items) and Preference for Behavioral Involvement (nine items)—may be obtained. Sample items include the following: “I’d rather be given many choices about what’s best for my health than to have the physician make decisions for me” and “It is better to trust the physician or nurse in charge of a medical procedure than to question what he/she is doing.” For this study, the total KHOS score was used in all analyses; coefficient alpha was .75.
Dialysis adherence
Patient’s fluid-intake adherence was assessed by computing IWG. IWG is a valid representation of fluid intake between dialysis sessions often used in both clinical and research settings (see Clark et al., 2014). Patients with values greater than 2.5 kg are generally considered non-adherent (see Christensen and Raichle, 2002). Individual IWG values, abstracted from medical records, were averaged over 2 weeks (i.e. six dialysis sessions) at each assessment point. The baseline assessment (Time 0; T0) comprised the 2 weeks preceding intervention initiation, Time 1 (T1) comprised the 2 weeks immediately following the final intervention session, Time 2 (T2) comprised the 12th and 13th post-intervention weeks, and Time 3 (T3) comprised the 24th and 25th post-intervention weeks.
Data analysis
Hierarchical multiple regression analyses were used to evaluate the effect of the interaction between perceived control (as measured by I-MHLC) and preference for control (as measured by KHOS) on change in IWG from baseline (i.e. pretreatment; T0) to timepoints T1, T2, and T3, respectively, after adjustment for baseline IWG, diabetic status (yes/no), and time on dialysis (in months). I-MHLC and KHOS were treated as continuous variables in regression analyses. A priori variable entry was as follows: Block 1 = T0 IWG, diabetic status, time on dialysis; Block 2 = I-MHLC score, KHOS score; Block 3 = centered interaction term (Aiken and West, 1991). For all analyses, a p-value < .05 was considered statistically significant (see Note 1).
Results
Demographic and clinical characteristics are presented in Table 1. Patients were predominantly male (65.9%), Caucasian (65.7%), and on dialysis for an average of 54.5 months (standard deviation (SD) = 58.6). The average IWG value at baseline was 3.94 (SD = 1.20). Intercorrelations, means, and SDs between IWG at all timepoints, I-MHLC, and KHOS are reported in Table 2. As expected, there were no significant correlations between IWG and I-MHLC and KHOS, respectively, which is consistent with previous research in this patient population (Cvengros et al., 2004).
Patient characteristics (N = 119).
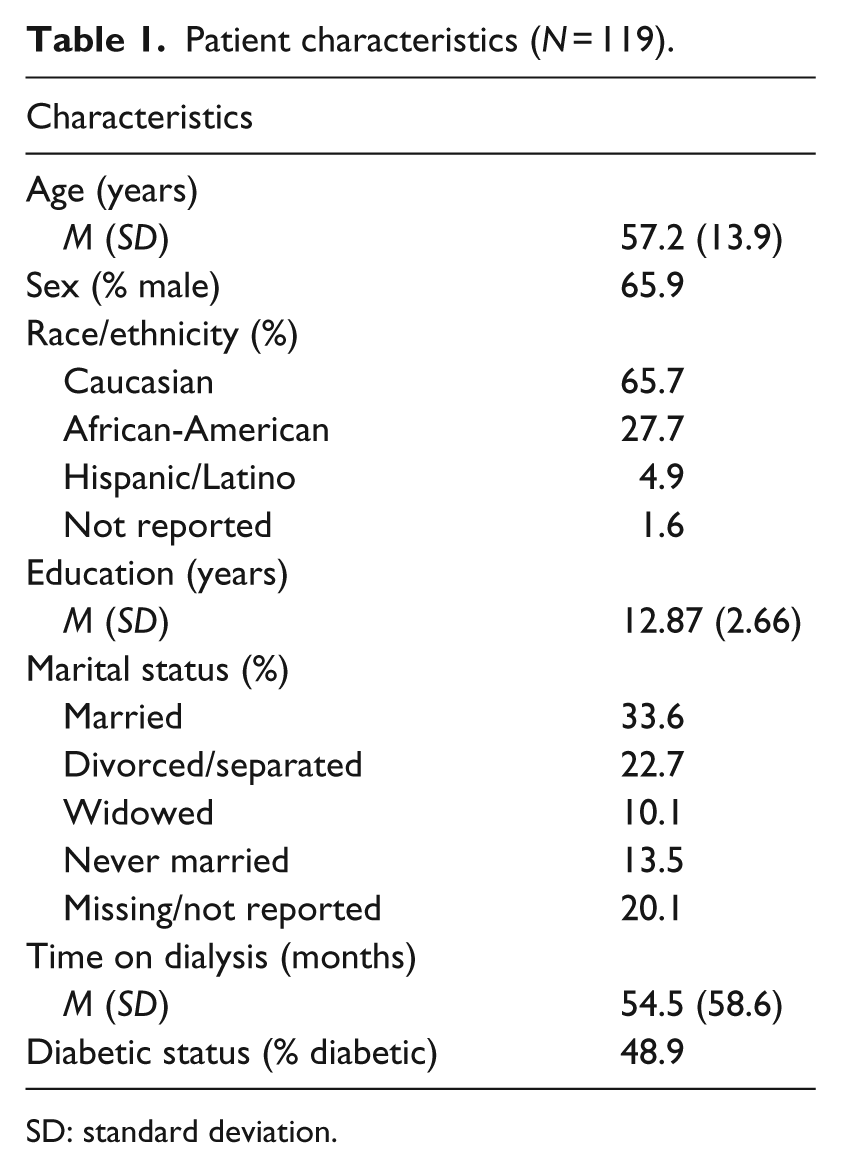
SD: standard deviation.
Intercorrelations, means, and SDs.
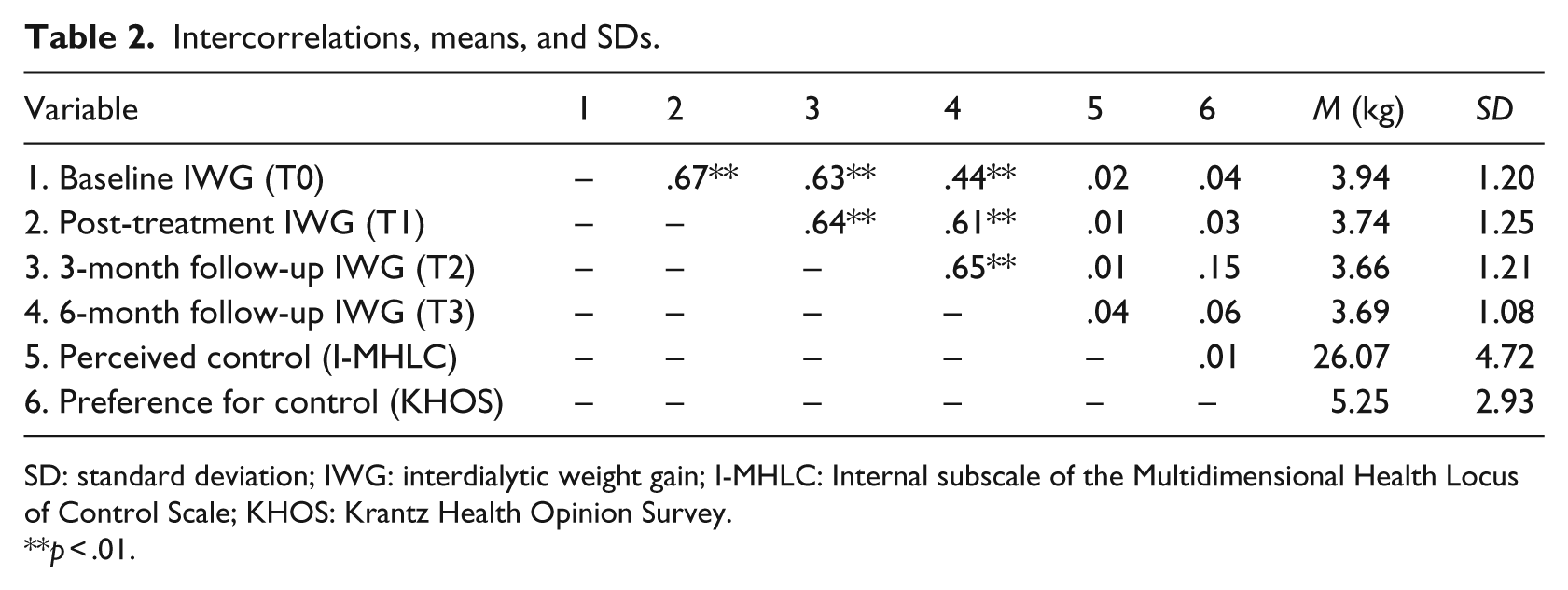
SD: standard deviation; IWG: interdialytic weight gain; I-MHLC: Internal subscale of the Multidimensional Health Locus of Control Scale; KHOS: Krantz Health Opinion Survey.
p < .01.
Hierarchical multiple regression analyses predicting change in IWG from T0 to T1—controlling for pretreatment IWG, diabetic status, and time on dialysis—indicated that although perceived control and preference for control alone did not significantly predict the outcome, the interaction between these variables explained a significant portion of variance in IWG from pre- to post-treatment (β = .222, p < .05, sr2 = .044; Table 3). Further analysis of the interaction results revealed that patients with strong perceptions of control (i.e. an internal HLC orientation) and also preferring much control and involvement showed, on average, over a 0.5-kg decrease in IWG from pre- to post-treatment (Figure 1). Conversely, those with an internal HLC orientation but preferring less control, or generally holding an external HLC orientation, showed little improvement from pre- to post-treatment.
Hierarchical multiple regression analyses predicting change in IWG from T0 to T1.
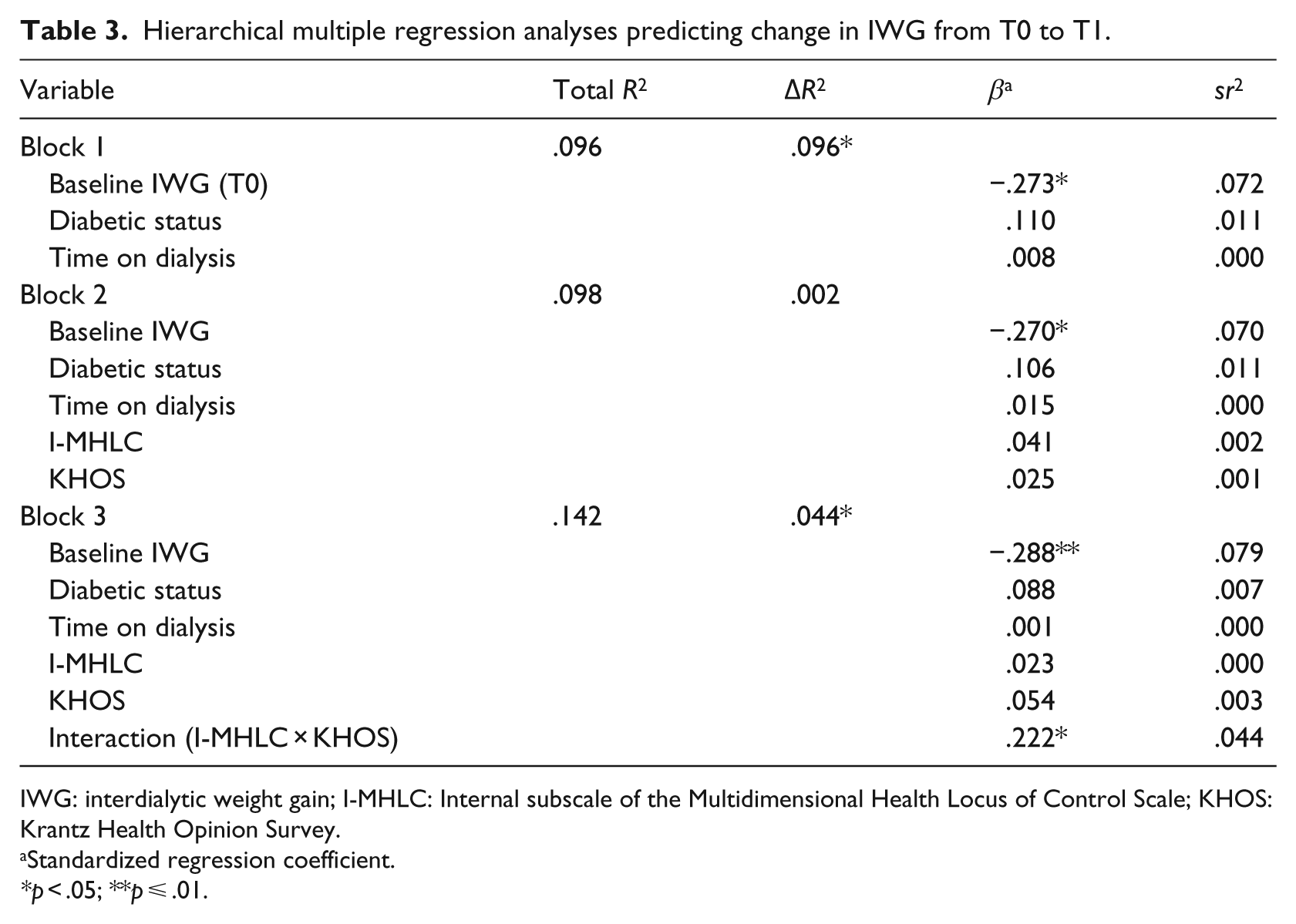
IWG: interdialytic weight gain; I-MHLC: Internal subscale of the Multidimensional Health Locus of Control Scale; KHOS: Krantz Health Opinion Survey.
Standardized regression coefficient.
*p < .05; **p ⩽ .01.

Average change in IWG from baseline to post-treatment.
Hierarchical multiple regression analyses predicting change in IWG from T0 to T2 showed similar results. Specifically, from T0 to T2, the interaction between perceived control and preference for control significantly predicted change in the outcome (β = .243, p < .05, sr2 = .052), but each behavioral variable alone did not (Table 4). From T0 to T3, neither the interaction term (β = .091, ns, sr2 = .007) nor the behavioral variables alone contributed significant variance to change in the outcome (Table 5).
Hierarchical multiple regression analyses predicting change in IWG from T0 to T2.
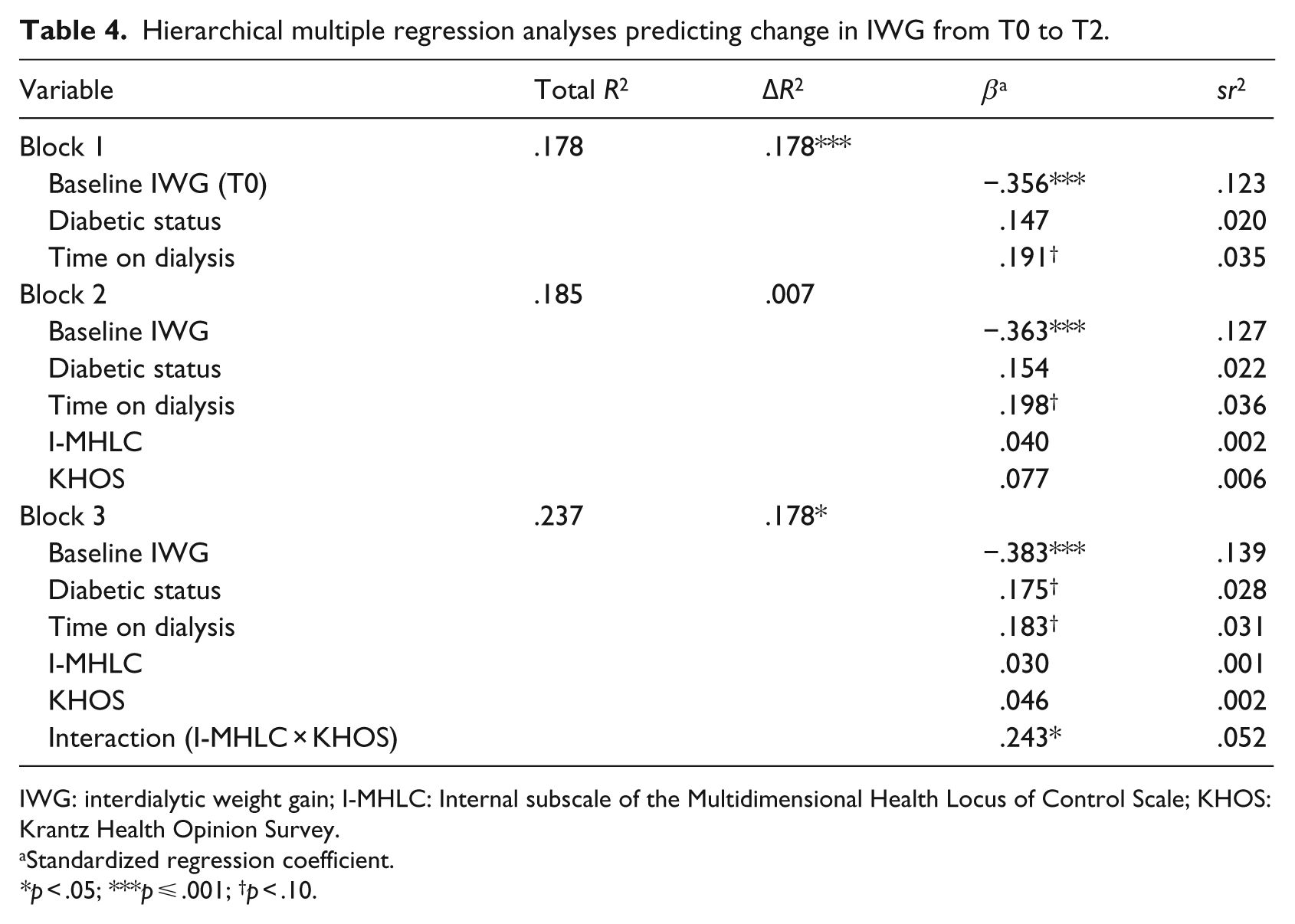
IWG: interdialytic weight gain; I-MHLC: Internal subscale of the Multidimensional Health Locus of Control Scale; KHOS: Krantz Health Opinion Survey.
Standardized regression coefficient.
*p < .05; ***p ⩽ .001; †p < .10.
Hierarchical multiple regression analyses predicting change in IWG from T0 to T3.
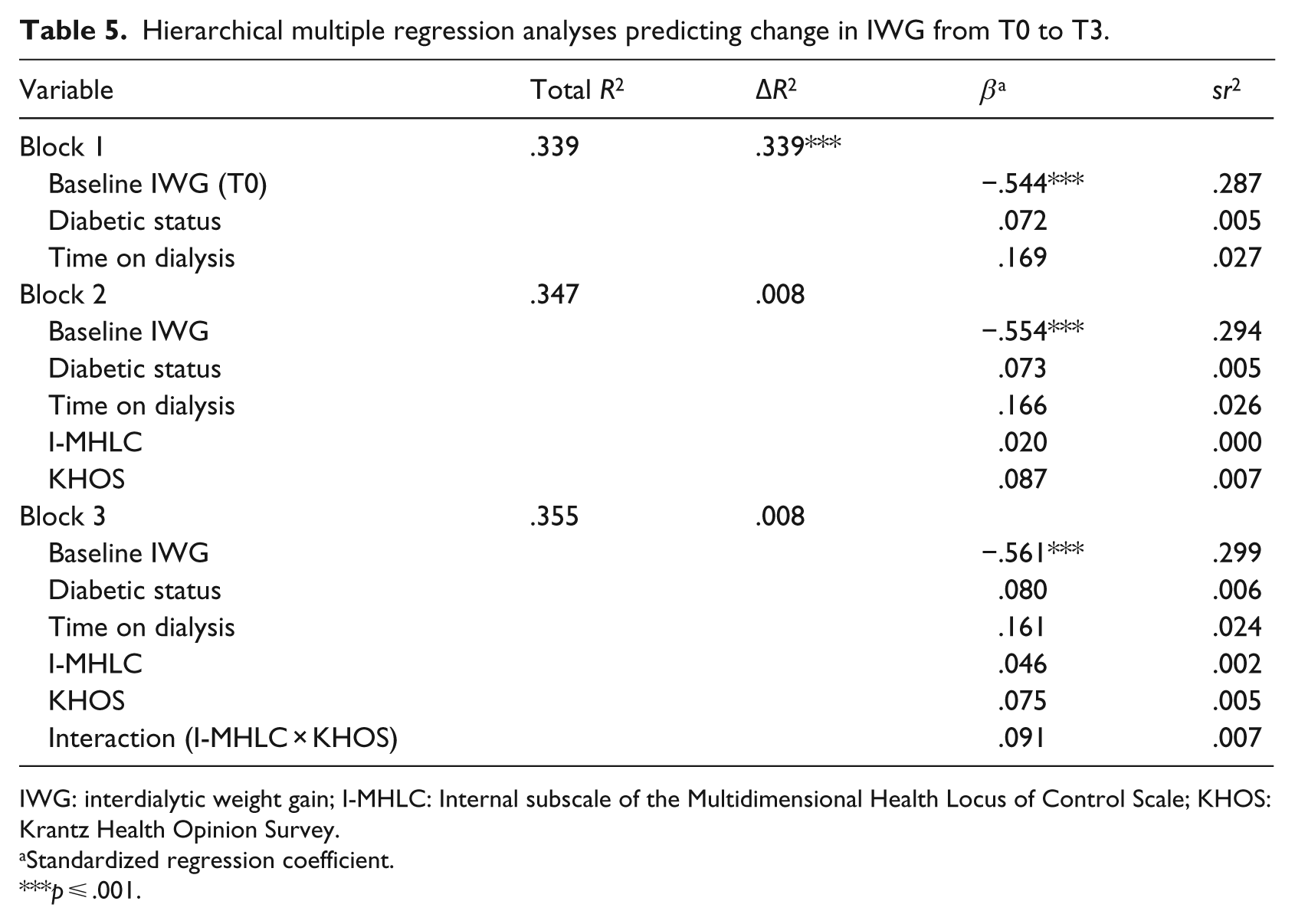
IWG: interdialytic weight gain; I-MHLC: Internal subscale of the Multidimensional Health Locus of Control Scale; KHOS: Krantz Health Opinion Survey.
Standardized regression coefficient.
p ⩽ .001.
Discussion
The present results are consistent with previous research suggesting that patient control beliefs are important for patient adherence and adaptation in the hemodialysis population (e.g. Cvengros et al., 2004). More specifically, it was not perceived control or preference for control alone that predicted improved adherence to fluid-intake restrictions, but rather the interaction between the two variables such that patients with a high internal HLC orientation coupled with a strong preference for control exhibited the most favorable reductions in IWG between dialysis sessions. The interactional nature follows previous research finding that such variables are inconsistently related to health outcomes when considered in a main effect fashion (see O’Hea et al., 2005).
These results suggest that those patients holding the belief that health-related outcomes are a function of one’s own behaviors—and having the opportunity to apply control over one or more aspects of treatment—may be most adherent to complex regimens in which patient self-management is key to optimal outcomes. Because HLC is fairly easy to capture, clinicians may consider increasing control for those preferring it, at least to the extent possible given each patient’s individual treatment regimen. For conditions like CKD, the multifaceted behavioral requirements described earlier may provide numerous opportunities to do so. More research is needed, however, to understand how these results may otherwise impact practice in this and other patient populations, what can be done for similar patients with conditions in which there is little option for control over treatment, and whether this information could be reliably included as part of a risk profile to help identify those at greatest risk of non-adherence.
It should be noted that we found high internal orientation and high preference for control to be most beneficial for change in IWG between timepoints T0 and T1 (i.e. baseline to immediately after the intervention) and T0 and T2 (i.e. baseline to 3-month follow-up), respectively, but not for change in IWG between timepoints T0 and T3 (baseline to 6-month follow-up). In the latter analysis, the only significant predictor was baseline IWG. The reasons are not clear, but this result underscores the importance of the patient’s level of adherence at enrollment in predicting outcomes over the course of treatment. This in no way reduces the implications of these findings, however, as this information may help clinicians facilitate meaningful improvement in adherence for this subset of patients holding these specific beliefs beyond that attributable to baseline levels of adherence.
Limitations and conclusion
Although it has several strengths (e.g. a relatively large sample of hemodialysis patients, frequently used measures of patient control beliefs, an objective clinical marker of adherence as the primary outcome), this study is not without limitations. Because patients were recruited from a concentrated geographic area, and because we excluded non-English-speaking patients, generalizability may be an issue. Of note, however, this sample compares favorably to national data reported for this patient population, including the number of minority participants (US Renal Data System (USRDS), 2014). In addition, although a 6-month follow-up period is fairly commonplace, we did not collect adherence data beyond this point, which is often noted as a limitation of many behavioral trials. We also did not have information regarding early termination of individual dialysis sessions, which presumably could impact IWG irrespective of the constructs studied here. Finally, we have no information on other constructs which may interact with patient control beliefs to impact adherence (e.g. perceived self-efficacy; O’Hea et al., 2009).
In conclusion, this study further supports the need to consider perceived control constructs—particularly those captured by the MHLC scales—within an interactional, as opposed to main effect, framework. Future research requires a more complex and nuanced approach if such moderators of treatment adherence are to be explained and resultant knowledge utilized in the practice setting. Doing so may help facilitate opportunities for behavioral medicine researchers and practitioners to improve adherence outcomes, perhaps even developing risk profiles which may be helpful for identifying non-adherent patients in this and other patient populations. As put forth by Wallston (2005), the action, indeed, seems to be in the interaction.
Footnotes
Acknowledgements
A portion of the information contained in this article was presented at the 34th Annual Meeting and Scientific Sessions of the Society of Behavioral Medicine in San Francisco, CA. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. ![]() Identifier: NCT01066949.
Identifier: NCT01066949.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported in part by NIDDK grant R01DK072325 awarded to Alan J. Christensen.