
Abstract
This study compares maladaptive coping, measured as substance use, behavioral disengagement, self-blame, and emotional eating, among adults (>18 years) who have experienced early parental loss (N = 1465 women, N = 331 men) with non-bereaved controls (N = 515 women, N = 115 men). We also compared bereaved adults who received grief counseling (N = 822 women, N = 190 men) with bereaved controls who had not (N = 233 women, N = 66 men). Bereaved adults reported significantly more substance use, behavioral disengagement, and emotional eating than non-bereaved adults. Counseling participants reported significantly more substance use and self-blame than non-participants. Our results suggest that early loss may negatively impact the development of adulthood coping.
The death of a parent in childhood is a painful experience, with potentially long-term consequences that may impact adult psychological health (Bowlby, 1980; Haine et al., 2008). Early parental loss has been linked to increased risks of depression, anxiety, and substance use in adulthood (e.g. Appel et al., 2013; Hamdan et al., 2013), indicating a lowered ability to cope with the stresses of life (Auerbach et al., 2010). However, to our knowledge, no study has investigated the long-term coping behavior of people who have lost a parent or who have received grief counseling.
“Coping” refers to the cognitive and behavioral strategies that individuals use to manage stress (Folkman and Moskowitz, 2004). It is mobilized by appraisal, a process whereby an external and/or internal demand is evaluated against a person’s resources (Lazarus and Folkman, 1984). Appraisal is influenced by multiple factors, including experiences across time (Lazarus, 1999). Within a life-course perspective, coping behaviors are seen as driven by developing systems, such as language and cognition, and shaped by person–environment interactions (Zimmer-Gembeck and Skinner, 2011).
Parents play an essential role for adaptive coping with stress (Gunnar and Cheatham, 2003). A secure parent–child attachment aids the development of emotional regulation (Waters et al., 2010), while consistent parental support increases the likelihood of successful coping experiences, fostering more flexible coping capabilities as the child matures (Zimmer-Gembeck and Skinner, 2011). The impact of losing a parent may depend upon the child’s age, which determines the cognitive capability to understand and cope with the death (Webb, 2010).
Grief counseling aims to facilitate the bereavement process, that is, to help the bereaved person adapt to the loss and resolve grief (Worden, 2009). While most children adapt without professional help (Akerman and Statham, 2011), some experience high levels of impairment warranting professional support (Worden, 2009). Two meta-analyses have summarized the limited studies on effects of grief counseling in bereaved children (age range, 5–18 years) (Currier et al., 2007; Rosner et al., 2010). The first meta-analysis, of 13 controlled studies, showed an overall average weighted effect size of Cohen’s d = 0.14 (p = 0.08), indicating no significant treatment effect. The second meta-analysis, of 13 controlled and 12 uncontrolled studies, showed overall effect sizes of Hedges’ g = 0.35 (p < 0.01) and 0.49 (p < 0.001), respectively, indicating small to moderate treatment effects. None of the studies considered adult outcomes. A single study, of the Family Bereavement Program (Sandler et al., 2003), included positive coping as an outcome and found effects for girls at the 11-month follow-up.
In this study, we compared maladaptive coping strategies (substance use, behavioral disengagement, self-blame, and emotional eating) in adulthood in relation to early parental loss and participation in grief counseling. First, we hypothesized that parental loss is associated with disruption of healthy coping development and that bereaved adults would report greater use of maladaptive coping strategies than non-bereaved adults. Second, we hypothesized that, by facilitating the bereavement process, receiving counseling would be associated with the development of adaptive coping, and that counseling participants would thus report less use of maladaptive strategies than non-participants. Additionally, we investigated whether child gender, which parent was lost, child’s age at the time of loss, and the perceived presence of family support played moderating roles in this association.
Method
Procedure
Data were drawn from a larger cross-sectional study of early parental loss and grief counseling, which combined register-based information with self-reported questionnaire responses (Appel et al., submitted). In Denmark, all residents have been recorded in the Central Population Register (CPR) since 1 April 1968 (Pedersen et al., 2006) with unique personal identification numbers, containing information on sex, date of birth, family linkage, migration, and death.
Three main nationwide organizations have offered free telephonic, group, and/or individual grief counseling to children and young adults. We identified participants who had received grief counseling at these centers between 1999 and 2009 and established a sample of 1811 participants who met the criteria of being over 18 years of age at 31 December 2010 and having lost one or both parents before the age of 30. We identified a second sample of 1803 bereaved participants from the CPR, who met the same conditions but were not on center files, and frequency matched them to the first group on gender, age, and time since parental death. A third sample of 1853 CPR-based non-bereaved controls were frequency matched on gender and age.
In all, 5467 participants (4045 females, 1422 males) were identified and invited to complete the questionnaire by mail. Informed consent is not required for questionnaire studies in Denmark; however, information on the project and the contact details of the primary researcher were provided. Non-responders were reminded after 3 weeks and again, by telephone, after a further 3 weeks. The study protocol was approved by the Danish Data Protection Agency (Record no. 2009-41-3506).
Study sample
A total of 2574 people completed the questionnaire (response rate, 47%). We excluded 12 bereaved respondents who had lost a parent after the age of 29 years, 67 whose self-reported parental loss was missing or incongruent with register information, and 36 participants from center files who self-reported no counseling, obtaining a group of confirmed recipients of grief counseling (Conf-GC). We found that 449 (60%) of bereaved participants in the CPR sample self-reported having received some kind of counseling (Self-GC), while 299 (40%) confirmed no counseling (No-GC). Finally, we excluded 69 respondents who did not complete the questionnaire and obtained a final study sample of 2390 participants, as shown in Figure 1.
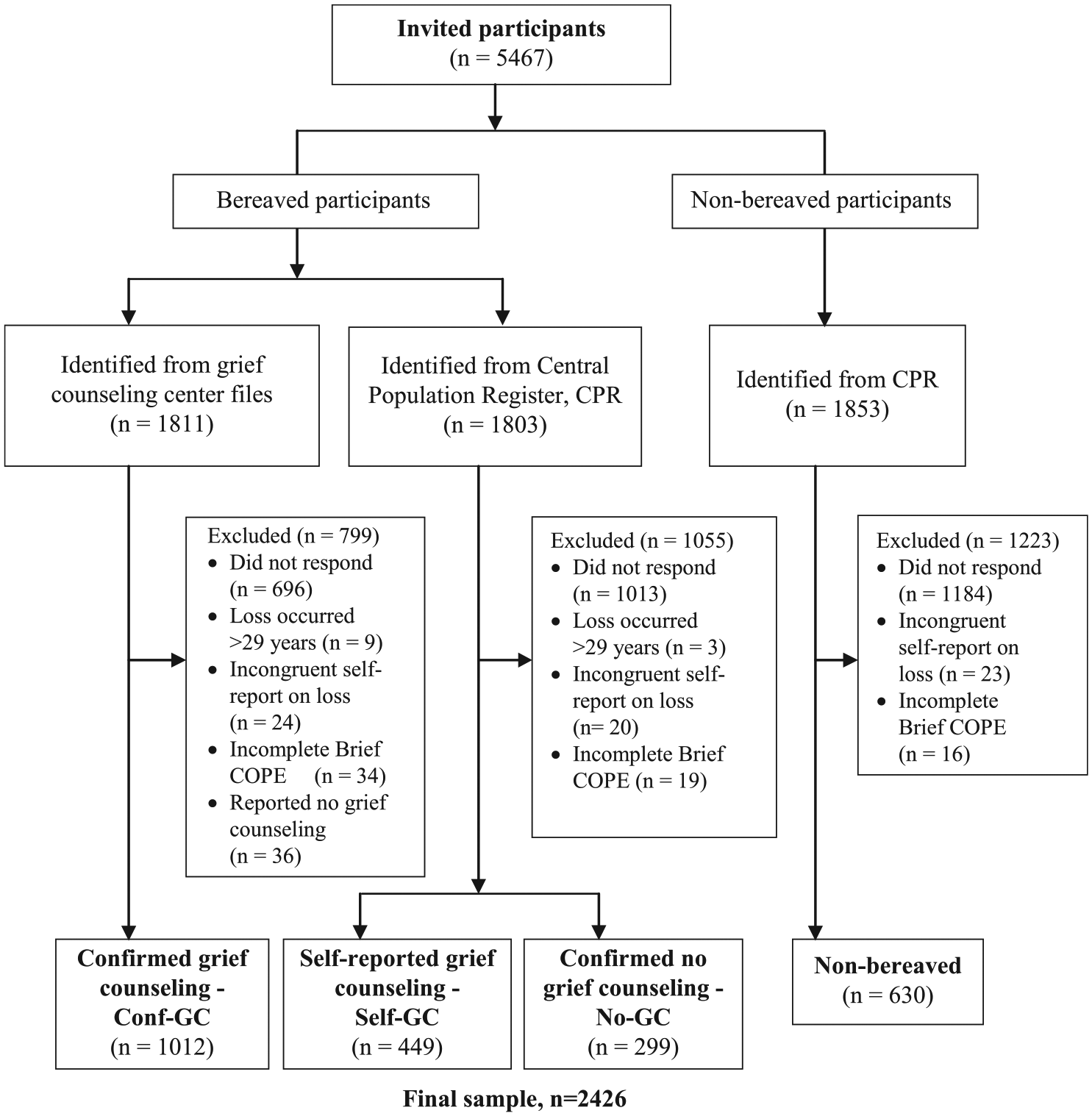
Flowchart of study participants.
Measures
Early parental loss (loss)
Loss was defined as losing one or both parents before the age of 30. We included individuals up to this age because previous studies suggest that loss during young adulthood continues to influence later psychological functioning (Appel et al., 2016; Nickerson et al., 2013). Loss was confirmed through the CPR and cross-checked with the questionnaire items, “Did your father/mother die before you were 30 years of age?”
Grief counseling (counseling)
Participation in counseling was determined from center files and checked from replies to the questionnaire item, “We would like to know if you participated in professional support at the time your parent died and if so, how many times did you participate?” Each support option (“psychologist,” “bereavement group,” “internet-based support,” “support by phone,” “general practitioner,” “priest,” “nurse,” or “other”) could have answers ranging from “Never” to “>40 sessions.” A response of “Never” for all the categories was considered self-reported No-GC, while all other responses were considered Self-GC.
Maladaptive coping
Coping was measured using the Brief COPE inventory (Carver, 1997), which was translated into Danish by two research psychologists and, subsequently, back-translated into English by a third bilingual psychologist. The back-translation corresponded semantically to the original version. It consists of 14 subscales of two items each that are answered on a 4-point Likert scale, ranging from 1 (“I haven’t been doing this at all”) to 4 (“I’ve been doing this a lot”). We focused on the subscales of substance use, behavioral disengagement, and self-blame. The range of scores for these subscales was 2–8. One additional item (“I have eaten for comfort”) was added in the questionnaire, giving a one-item emotional-eating subscale, with a score range of 1–4. The Brief COPE scales have good internal consistency, construct validity, and adequate test–retest reliability (Cooper et al., 2008), although the Danish version has yet to be validated.
Covariates
Participant’s gender, age at time of loss (0–5, 6–12, 13–18, ⩾19 years), education (basic school, high school or vocational, higher education, unknown), parent lost (father, mother, both), and perceived family support (yes, no) were identified as covariates. Gender and educational level have been related to coping styles (Christensen et al., 2006; Matud, 2004), and child’s educational level has been linked to parental educational level (Dubow et al., 2009), which is in turn associated with mortality rates (Montez et al., 2012). The parent lost, participant age at time of loss, and family support have been shown to affect bereavement outcomes (Raveis et al., 1999; Stroebe et al., 2006).
Participant gender, birth date, parent lost, and date of death were obtained by linkage with the CPR, while participants self-reported level of education and family support at the time of the death. Perceived family support was measured from answers to the item, “What level of support did you experience from the persons around you when your parent died?” Each person option (“parent,” “siblings,” “grandparents,” and “other family members”) could be answered with “high,” “moderate,” “low,” “none,” “don’t know,” or “have none.” Responses were dichotomized into a Yes/No perceived family support variable, where high and moderate reported levels of support were coded as “Yes” and the remaining responses as “No.”
Statistical analyses
Descriptive statistics
Descriptive comparisons of bereaved and non-bereaved participants were made according to gender, age, and educational level. Bereaved participants were further compared by the gender of the deceased parent, age at time of loss, and perceived family support according to counseling group (Conf-GC, Self-GC, and No-GC). Chi-squared tests were used for categorical variables and t tests for continuous variables.
Parental loss and coping
Multivariable linear regression models were used to examine the mean differences in substance use, behavioral disengagement, self-blame, and emotional eating according to bereavement status. As histograms indicated that scores on the maladaptive subscales peaked for the response that the behavior was not used, we also used logistic regression to estimate differences in behavior use (substance use, behavioral disengagement, self-blame >2; emotional eating >1) according to bereavement status and expressed as odds ratios. As log and linear models gave the same conclusions, linear regression was used for the remaining analyses to allow possible comparisons with the other scales that were more normally distributed. Analyses were carried out unadjusted as well as adjusted for age and educational level.
To investigate whether the differences between bereaved and non-bereaved participants were moderated by gender, parent lost, age at time of loss, and perceived family support, we added an interaction term between bereavement status and each of the four modifiers in separate models. The mean changes in coping scores were estimated, and effect modification was tested in F tests.
Grief counseling and coping
Multivariable linear regression models were used to compare differences in mean coping scores between grief counseling participants (Conf-GC and Self-GC) and No-GC. Analyses were unadjusted or adjusted for participant’s gender, parent lost, age at time of loss, educational level, and perceived family support, which may be associated with both receiving counseling and coping (Holahan and Moos, 1987; Vessey and Howard, 1993). All analyses were carried out using SAS Enterprise Guide 5.1.
Results
Study sample
Table 1 shows the characteristics of the full study sample. There were no significant differences by bereavement status, but there were significant differences by counseling status. Those in the Self-GC group tended to be younger, with correspondingly lower levels of attained education, and had experienced loss at a younger age than the Conf-GC and No-GC groups.
Characteristics of the full sample by bereavement status and of the bereaved sample by grief counseling status (group percentages in parentheses).
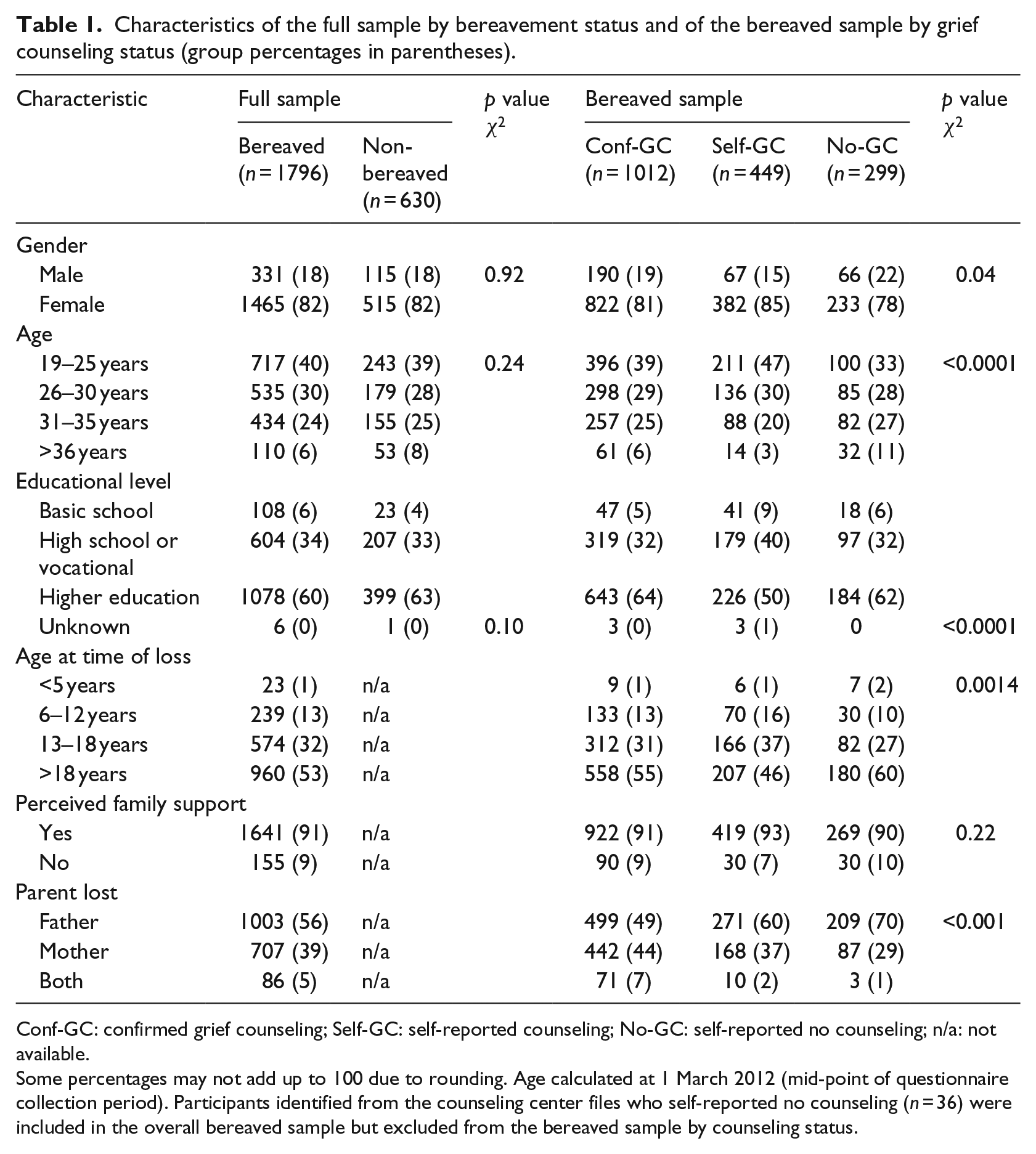
Conf-GC: confirmed grief counseling; Self-GC: self-reported counseling; No-GC: self-reported no counseling; n/a: not available.
Some percentages may not add up to 100 due to rounding. Age calculated at 1 March 2012 (mid-point of questionnaire collection period). Participants identified from the counseling center files who self-reported no counseling (n = 36) were included in the overall bereaved sample but excluded from the bereaved sample by counseling status.
Parental loss and coping
Bereaved participants scored significantly higher for substance use (adjusted mean difference (MD) = 0.21, 95% confidence interval (CI) [0.11, 0.30]), behavioral disengagement (MD = 0.13, 95% CI [0.02, 0.25]), and emotional eating (MD = 0.15, 95% CI [0.08, 0.23]) but not for self-blame (MD = 0.00, 95% CI [−0.13, 0.14]). The odds ratios with 95 percent CIs gave similar results (Table 2). Only perceived family support moderated the association between parental death and maladaptive coping on all four subscales (p < 0.0001 for all subscales), while parent lost and participant’s age at time of loss had a moderating effect only on substance use (p = 0.03 and p < 0.0001, respectively; results not shown).
Mean score, estimated mean differences, and odds ratio for use of coping behavior with 95 percent confidence intervals by bereavement status.
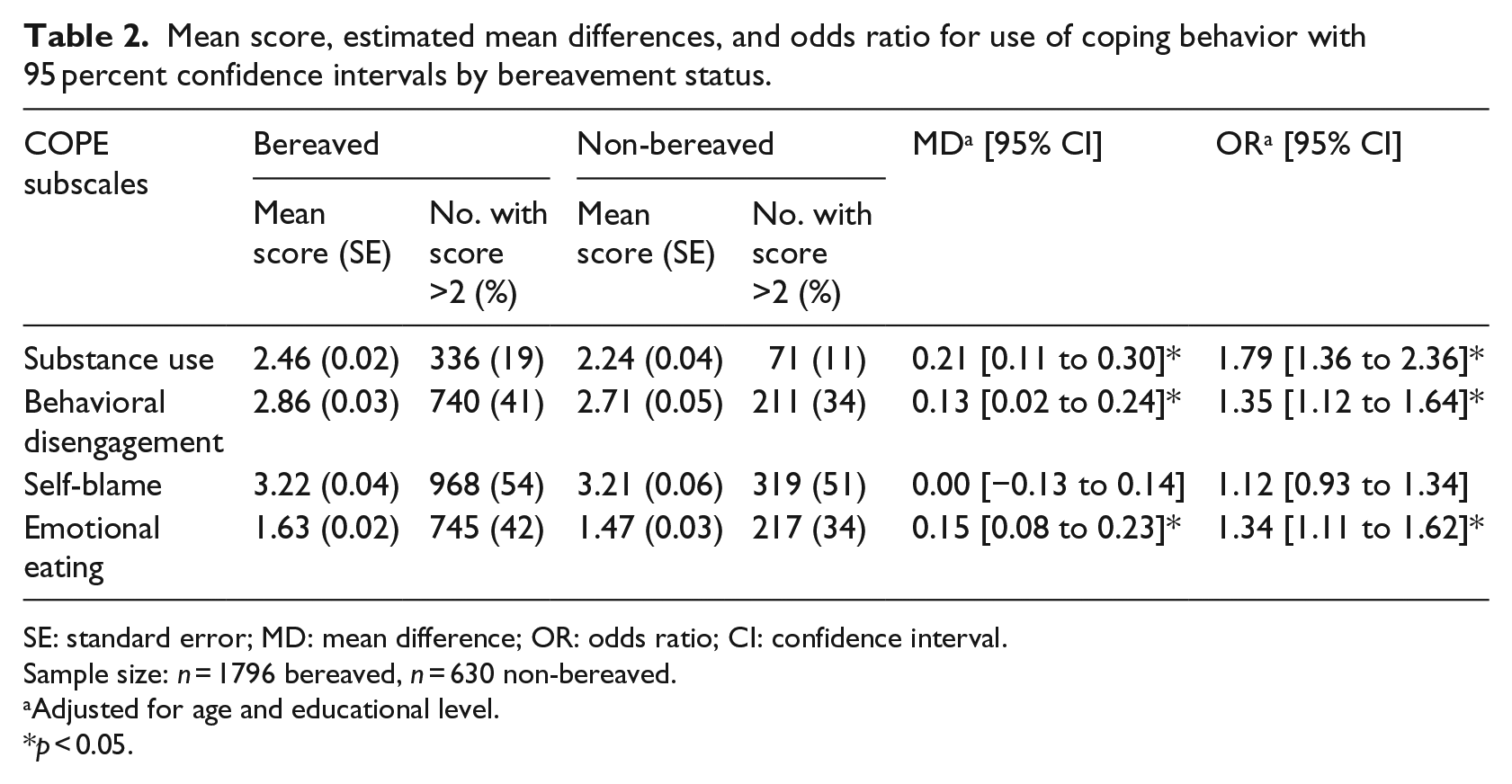
SE: standard error; MD: mean difference; OR: odds ratio; CI: confidence interval.
Sample size: n = 1796 bereaved, n = 630 non-bereaved.
Adjusted for age and educational level.
p < 0.05.
Grief counseling and coping
Grief counseling recipients and non-recipients did not differ significantly on the scales of behavioral disengagement and emotional eating; however, Conf-GC participants reported significantly more substance use (adjusted MD = 0.16, 95% CI [0.01, 0.30], p < 0.05) and self-blame (MD = 0.32, 95% CI [0.13, 0.52], p < 0.05) than No-GC participants. The unadjusted and adjusted results are shown in Table 3.
Mean score and estimated mean differences with 95 percent confidence intervals for maladaptive coping scales by counseling status: confirmed grief counseling (Conf-GC), self-reported counseling (Self-GC), or self-reported no counseling (No-GC).
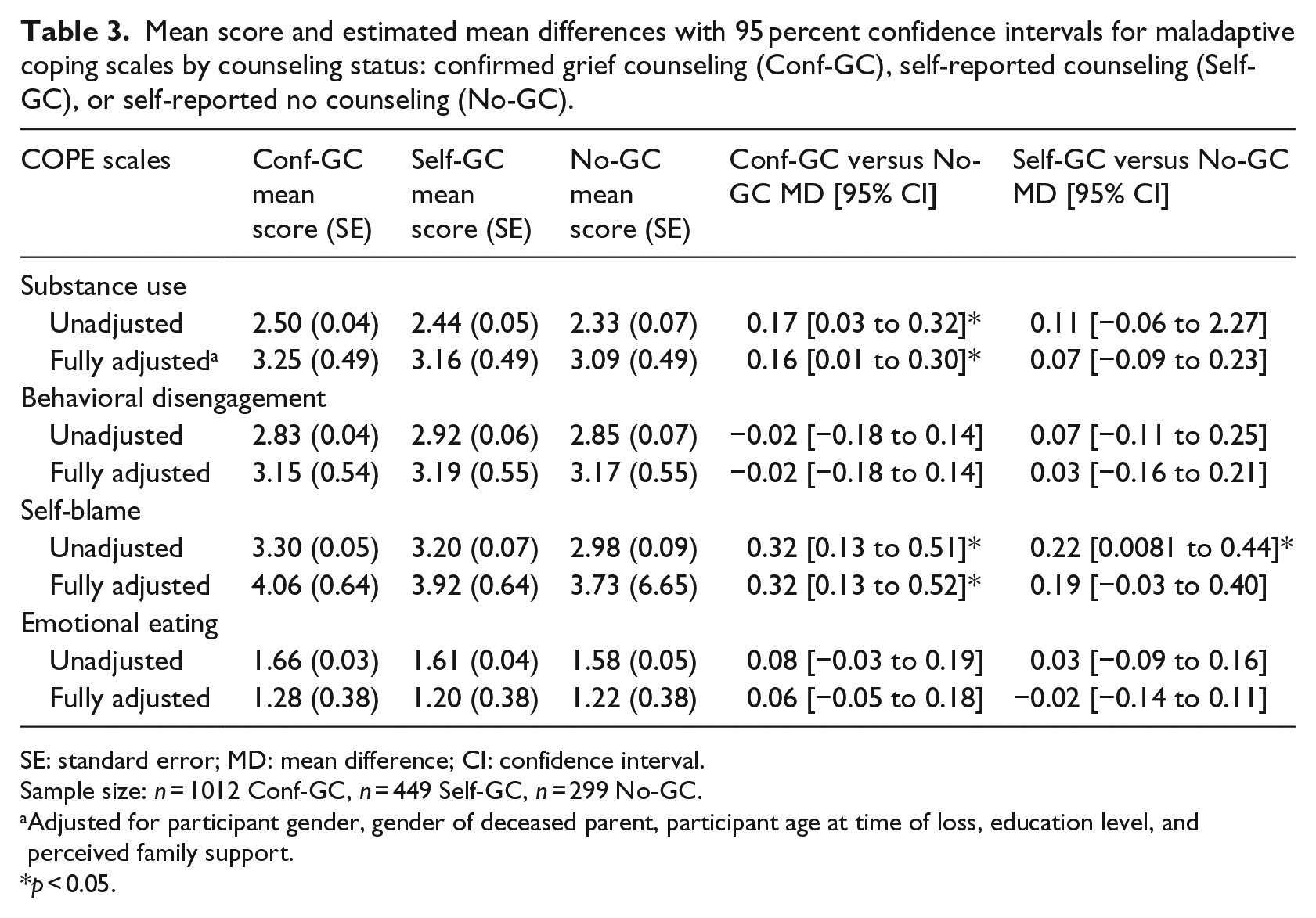
SE: standard error; MD: mean difference; CI: confidence interval.
Sample size: n = 1012 Conf-GC, n = 449 Self-GC, n = 299 No-GC.
Adjusted for participant gender, gender of deceased parent, participant age at time of loss, education level, and perceived family support.
p < 0.05.
Discussion
Our results underline the important role of parental loss in coping strategies. In accordance with our first hypothesis, bereaved adults reported significantly higher substance use, behavioral disengagement, and emotional eating than non-bereaved adults. The finding on substance use bears out several longitudinal studies that found higher levels of alcohol and substance abuse among both youth and adults after parental loss (Giordano et al., 2014; Hamdan et al., 2013). Those who lost both parents and those who experienced death between the ages of 6 and 18 years appeared most vulnerable to substance use as adults. For the other subscales, parent lost and child age at time of loss did not modify our results, indicating that parental death may have a long-term detrimental effect regardless of parent gender and child age.
A new contribution of our study is the finding that early parental loss is associated with behavioral disengagement and emotional eating as coping strategies in adulthood. Disengagement refers to giving up efforts to handle a stressor and has been linked with low self-efficacy, the lack of belief in one’s abilities (Bandura, 1977; Carver et al., 1989). The death of a parent is an experience of ultimate helplessness for a child and this vulnerability may interact with the surviving parent’s limited resources to model and foster subsequent mastery experiences needed for shaping high self-efficacy (Bandura, 1977; Fan and Williams, 2009). Our finding on emotional eating backs one previous study that found an association between parental bereavement and youth obesity (Weinberg et al., 2013). A possible explanation may be that eating patterns are influenced by family functioning and quality of parenting (Rhee, 2008), two factors potentially affected by parental loss. Interestingly, emotional eating may predict eating disorders (Stice et al., 2002), which in turn have been described as ways of coping with problems of personal control (Polivy and Herman, 2002). Future research may investigate the possibility that parental death influences maladaptive coping through pathways involving efficacy and control beliefs.
The only factor that modified the association between loss and all four maladaptive coping scales in our study was perceived family support. Significantly lower levels of maladaptive coping according to bereavement status were found in adults who reported higher family support. Emotional support has a positive effect on bereavement outcomes by lowering psychological distress (Raveis et al., 1999) and surviving parents, who are able to provide higher levels of emotional support to the grieving child, may also provide the stable attachment and security needed in the child’s environment post-loss. This highlights the need to target the family and “parenting capacity” of the surviving parent when intervening in bereaved children.
Contrary to our second hypothesis, we found no significant differences on behavioral disengagement and emotional eating between those who received counseling and those who did not. Furthermore, both groups of participants who received counseling (Conf-GC and Self-GC) reported significantly higher usage of substance use and self-blame than non-recipients, although the difference between Self-GC and non-recipients (No-GC) became insignificant in the fully adjusted model. These findings highlight a number of methodological and theoretical issues.
First and most important, it is highly probable that those who had sought and received grief counseling experienced higher distress levels compared to those who did not, resulting in a counseling group with a significantly higher baseline of maladaptive coping than the non-counseling group. Second, we had no detailed information about the structure or content of the grief counseling, and it is possible that the services offered were insufficient for participants suffering from more severe and complicated grief reactions. Third, the possibility for grief counseling to be harmful has been posited by Jordan and Neimeyer (2003), although the methodology used in that study has since proved questionable (Larson and Hoyt, 2007). However, since children have a “short sadness span” and a need to focus on non-grief related activities (Webb, 2010: 17), counseling may force the child to dwell unnecessarily on aspects of grief and interfere with the natural oscillation toward restoration-oriented tasks, as described in the dual-process model of grief (Stroebe and Schut, 1999). Screening may therefore be useful as there is evidence that interventions for symptomatic participants produce better outcomes than those with no selection criteria (Rosner et al., 2010).
This study has several strengths. This is the first study to examine the role of parental loss in adult coping. Also, our study is the largest on childhood bereavement and grief counseling. In the latest meta-analysis on childhood grief interventions, the largest study had 230 participants, while the numbers for the rest ranged from 17 to 87 (Rosner et al., 2010). The identification of a population-based non-bereaved control group is also unique, made possible by national registries that were established years before this study was hypothesized thereby avoiding information, recall, and selection bias. Also, grief counseling was available free of charge and our sample of counseling recipients were not recruited in an experimental setting, hence increasing the ecological validity of the results and decreasing sample selection bias (Steele et al., 2012). We also matched our groups on important confounders such as age, gender, age at time of parental death, and time since parental death.
However, the cross-sectional design limits the understanding of the causal nature of the association between early parental death, grief counseling, and coping in adulthood. Counseling participants were heterogeneous with regard to type and extent of counseling received, thus the current findings cannot be generalized to specific counseling practices. We were also unable to include other factors that influence a child’s development, such as family functioning, or adjust for other potentially confounding factors, such as substance use in the parent(s), which could be associated with both parental death and our outcome.
This study underlines the negative role of early parental loss on coping behaviors in adulthood. However, future studies with prospective design measuring coping behaviors over time before and after loss and counseling, respectively, are needed. Additional research in coping using a developmental perspective, and a further shift in focus to the areas of resilience and post-traumatic growth after parental death, may provide additional theoretical and clinical insights.
Footnotes
Acknowledgements
The authors thank the grief counseling organizations (The Danish Cancer Society, Children’s Welfare, and The Danish Counseling and Research Center for Grieving Children and Youth) for their contribution to this study. They also thank Visti B. Larsen for his invaluable assistance in data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Danish foundation TrygFonden (J.nr. 7134-08).